
Abstract
Traumatic brain injury (TBI) is associated with an elevated frequency of mood disorders that may, in part, be explained by changes in white-matter microstructure. This study is the first to examine the relationship between mood disorders and white-matter pathology in a sample of patients with mild to severe TBI using a standardized psychiatric interview. This study reports on a sub-sample of 29 individuals recruited from a large prospective study that examined the evolution of psychiatric disorders following complicated, mild to severe TBI. Individuals with TBI were also compared with 23 healthy control participants. Individuals were invited to complete the Structured Clinical Interview for DSM-IV Disorders (SCID) to diagnose psychiatric disorders. Participants who developed a mood disorder within the first 3 years were categorized into a TBI-Mood group. Diffusion tensor tractography assessed white matter microstructure using atlas-based tract-averaged and along-tract approaches. Fractional anisotropy (FA) was used as the measure of white-matter microstructure. TBI participants with and without a mood disorder did not differ in regard to injury severity and other background factors. Nevertheless, TBI participants diagnosed with a mood disorder displayed significantly lower tract-averaged FA values for the right arcuate fasciculus (p = 0.011), right inferior longitudinal fasciculus (p = 0.009), and anterior segments I (p = 0.0004) and II (p = 0.007) of the corpus callosum, as well as the left (p = 0.014) and right (p = 0.015) fronto-occipital longitudinal fasciculi. The pattern of white matter disruption identified in the current study provides further support for a neurobiological basis of post-TBI mood disorders. Greater understanding of individuals' underlying neuropathology may enable better characterization and prediction of mood disorders. Integration of neuropathology may also inform the potential efficacy of pharmacological and psychological interventions.
Introduction
M
Despite this high prevalence, the causes and risk factors of mood disorders following TBI are poorly understood. Pre-morbid and injury-related factors generally display inconsistent relationships with mood disorders following TBI. 2,6 These factors include age, gender, and injury severity. Pre-morbid psychiatric history, however, more consistently predicts the development of mood disorders. 2,7,8 Environmental stressors and degree of disability account for a proportion of mood disorders following TBI. That is, experiencing a significant life stressor, loss of physical and cognitive functions, and restricted community participation play a role in the development of mood disorders. Nevertheless, there is a growing body of literature suggesting that neuropathological changes specific to TBI also contribute to the development of mood disorders. For example, Jorge and colleagues 2 found that depressive disorders were more frequent among patients with TBI compared with trauma patients who did not sustain a brain injury.
Indeed, mood disorders are considered to be multi-dimensional systems-level disturbances affecting functionally integrated brain pathways. 9 From a neurobiological perspective, the development of emotional, cognitive, and somatic features of mood disorders is currently best captured within the limbic-cortical dysregulation model. 9 –11 Converging findings suggest that mood disorders arise when certain brain circuits fail to maintain homeostatic emotional control during periods of increased cognitive or somatic stress. 11 –13 This model proposes three distinct, but interrelated compartments. The dorsal compartment modulates attentional and cognitive features of mood, comprising neocortical regions—such as the dorsolateral prefrontal cortex—as well as regions of the cingulate. The ventral compartment is related to the vegetative and somatic features of depression, comprising the orbito-frontal cortex, as well as deeper limbic, subcortical, and brainstem regions. The third compartment, the rostral cingulate, is hypothesized to regulate interactions between these two distinct compartments due to the presence of reciprocal connections between dorsal and ventral regions. Disordered mood, therefore, is not a dysfunction of a single component but the failure of the coordinated interactions between the compartments. 9
Given the significance of frontal and limbic areas in the development of mood disorders, it is unsurprising that elevated rates of mood disorders are present following TBI. 2,7,14,15 In TBI, which can include focal lesions and diffuse axonal injuries (DAI), fronto-temporal pathology is especially common. 16 There is substantial evidence linking pathology in brain regions and circuits injured due to TBI with mood disorders. 2,17 Most studies have examined the association between mood disorders, location of brain lesion, and regional assessments of brain structure and function. 17 –30 Findings from these studies largely align with the limbic-cortical model, whereby pathology is detected in prefrontal, striatal, basal ganglia, and limbic regions in association with post-TBI mood disorders.
Diffusion tensor imaging (DTI) is a magnetic resonance imaging (MRI) technique that quantifies the orientation of white-matter bundles. 31,32 This neuroimaging method is of particular importance following TBI due to its ability to quantify DAI, even in milder forms of TBI. 33,34 DAI is hypothesized to play a role in many of the residual neurocognitive and neurobehavioral impairments following injury. Fractional anisotropy (FA) and mean diffusivity (MD) are two of the most frequently used diffusion parameters, which assess the directionality and magnitude of water diffusion along white-matter bundles, respectively. Generally, lower FA and higher MD values following TBI are associated with a range of cognitive, behavioral, and motor deficits. 35 –38
Because of its sensitivity to disrupted white-matter circuitry, DTI has potential to identify novel biomarkers for post-TBI mood disorders. Of the four studies that have used DTI, three have been limited to mild TBI. 26,39 –41 In addition, there has been a reliance on self-rated questionnaires to assess symptoms of depression. Nevertheless, studies incorporating only mild TBI participants report associations between disturbed mood and changes in white-matter microstructure in fronto-temporal regions, the basal ganglia, and brainstem. In a sample of participants with mild and moderate TBI assessed on average 9 years post-injury, Han and associates 40 used resting state network analysis to detect increased amygdala connectivity with other limbic and prefrontal regions in the mood TBI group, as well as areas specific to the limbic-cortical mood-regulating circuit, including left prefrontal regions and the right thalamus.
Despite the vast literature highlighting the utility of MRI in delineating injury severity as well as neuronal damage underpinning cognitive, behavioral, and emotional impairments, patients still do not systematically have MRI scans following TBI. 42 In many trauma centers, however, computed tomography (CT) is standard following moderate to severe TBI. This may reflect high costs of scans and concerns regarding contraindications, although MRI is generally more sensitive to neuronal damage than more conventional imaging modalities. 42 Demonstrating that novel MRI techniques are sensitive to biomarkers of functional impairments might further justify use of MRI scanning as a clinical tool following TBI.
The present study used DTI tractography to examine the relationship between mood disorders and white-matter pathology in a sample of patients with mild to severe TBI, diagnosed with a mood disorder using a structured psychiatric interview. In addition, this study was the first to use “along-tract” analysis of reconstructed tracts to isolate disturbances within individual tracts following TBI. We hypothesized that participants who developed mood disorders following TBI would display white-matter pathology in tracts coursing through temporal and frontal regions, in line with the cortical-limbic model of emotional dysregulation.
Methods
Participants
Ethical approval was obtained from the Epworth HealthCare and Monash University Human Research Ethics Committees. This study reports on a sub-sample of individuals recruited from a larger prospective study examining the evolution of psychiatric disorders following mild to severe TBI. As part of the large prospective study, individuals were invited to complete the Structured Clinical Interview for DSM-IV Disorders (SCID) to diagnose DSM-IV-TR Axis I psychiatric disorders. 43 Participants were followed up over eight time-points up to 5 years following their injury. Refer to Gould and colleagues 7 and Alway and co-workers 5 for a more detailed account of the study methodology. For each participant, an initial SCID-I interview was conducted soon after resolution of post-traumatic amnesia (PTA) to obtain a lifetime pre-morbid history of psychiatric disorders as well as those present since the injury. Interviews were repeated to obtain diagnoses occurring within the intervening period at each follow-up time-point.
From the total sample of 203 recruited into the larger prospective study, a sub-sample of 29 individuals consented to, and underwent, an MRI scan. MRI scanning was conducted once for each participant up to 3 years following the TBI. Of this sub-sample, 8 individuals met criteria on the DSM-IV-TR for a diagnosis of a mood disorder, at least once, within the first 3 years following injury (for detailed information see online Supplementary Table 1 at
This cohort comprised 161 participants who completed baseline assessment and a year of more of follow-up as part of the prospective psychiatric study. For further information about this cohort refer to Alway et al. 5
For the full cohort age is the age at accident.
CT, computed tomography; d, days; GCS, Glasgow Coma Scale; m, months; MRI, magnetic resonance imaging; PTA, post-traumatic amnesia; SD, standard deviation; TBI, traumatic brain injury; y, year.
Magnetic resonance imaging acquisition
Neuroimaging was performed on a Siemens Magnetom Verio 3 Tesla MRI scanner (Siemens Medical Imaging, Erlangen, Germany). The DTI included the following parameters: repetition time [TR] = 5500, echo time [TE] = 110; 20 diffusion gradient directions; number of excitations = 2; slice thickness = 4 mm; field of view = 240 mm; matrix = 122 × 122, in-plane = 1.97 × 1.97 mm; b value = 1000 sec/mm2, one acquisition for each run with b = 0 sec/mm2. In addition, a three-dimensional (3D) T1-weighted sequence was acquired in the sagittal orientation with the following parameters: inversion time = 1100 msec; TR = 1930 msec; TE = 2.48 msec; resolution = 256 × 256 × 160; flip angle = 12 degrees; field of view = 256 mm; slice thickness = 1.00 mm, 160 slices.
Diffusion tensor imaging pre-processing
ExploreDTI version 4.8.5, a DTI toolbox, was used for all pre-processing, tractography, and along-tract procedures (Fig. 1, Panel 1). 44 Images were pre-processed in accordance with procedures outlined in Deprez and colleagues 45 Data quality assessments were conducted, including global assessments of gross image distortions prior to tensor estimation, as well as qualitative and quantitative assessments of the diffusion tensor residuals following tensor estimation. Images were corrected for participant motion and eddy currents. 46 Echo-planar imaging (EPI) distortions were corrected by elastically registering each participant's DTI images to their corresponding T1-weighted image. Prior to EPI correction, T1-weighted images were resampled to 2 × 2 × 2 mm. The diffusion tensor was estimated using the Robust Estimation of Tensors by Outlier Rejection (RESTORE). 47 This process iteratively reweighted the least-squares regression for outlier identification to remove artefacts associated with physiology and participant motion. Following pre-processing, whole-brain tractography was conducted for each dataset using constrained spherical deconvolution (CSD) 48,49 with the following parameters: step size = 1 mm; fiber orientation distribution (FOD) threshold = 0.1; angle threshold = 30 degrees; length range = 50–500 mm; seed resolution = 2 × 2 × 2 mm; L max = 4.
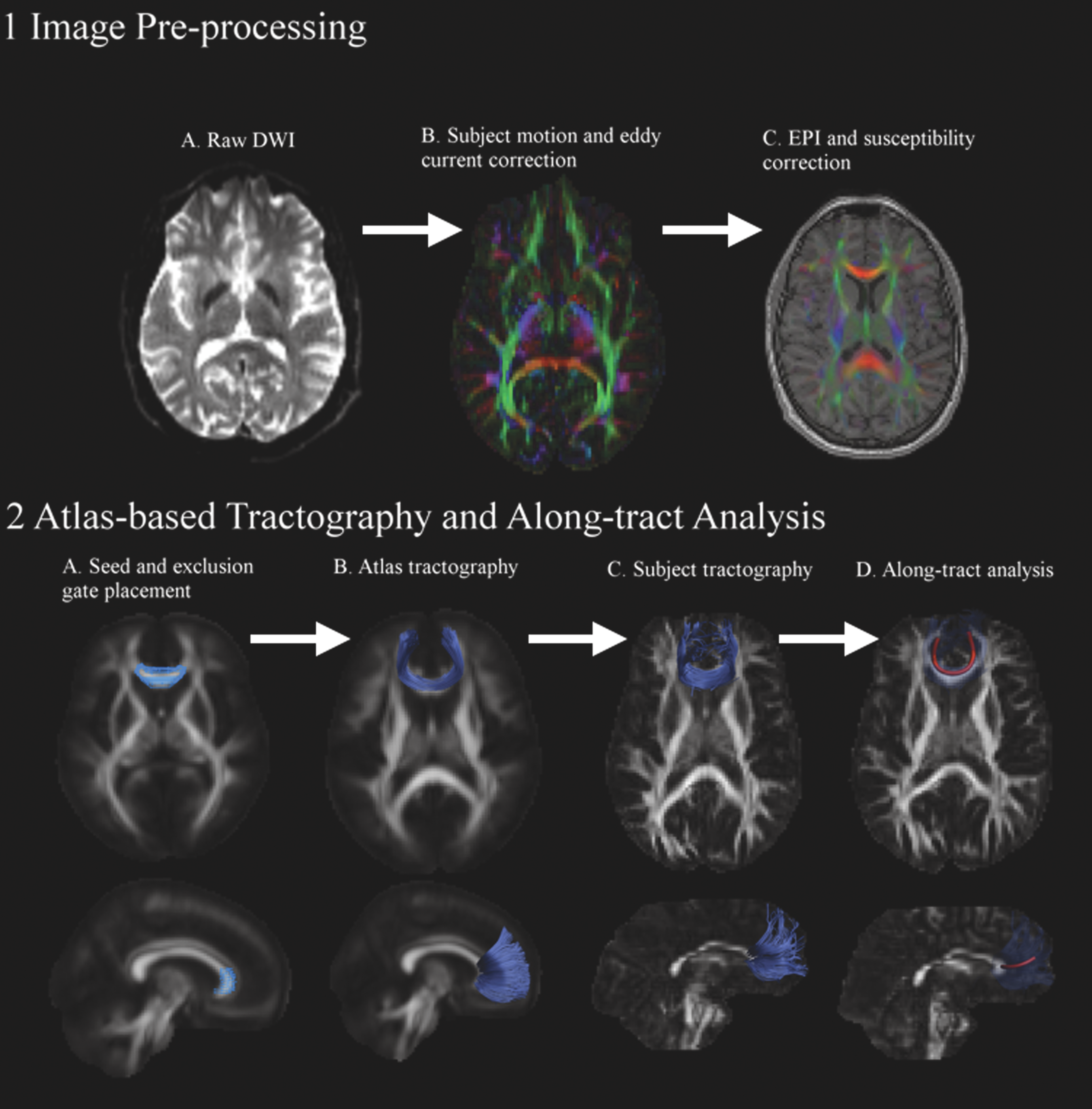
Summary of the study neuroimaging protocol. Stage 1 presents the image pre-processing steps. Raw diffusion-weighted images (DWI) were converted to diffusion tensor volumes (DTI) using Robust Diffusion Tensor estimation, which excluded outliers prior to estimation. Corrections were made for participant motion and eddy current distortions
Atlas-based tractography
Automated atlas-based tractography involved defining a set of regions-of-interest (ROI) on the ICBM 2 mm DTI atlas (Fig. 1, Panel 2A).
50
These ROIs were then registered to each participant's DTI image to automatically reconstruct all tracts of interest (Fig. 1, Panel 2B). A broad range of tracts was examined in the current study to ensure comprehensive coverage throughout the brain (see online Supplementary Fig. 1 at
White-matter pathways were initially identified by placing ROIs on axial slices of the ICBM template as outlined by the Catani and colleagues 51 DTI tractography atlas. This atlas was used to reconstruct the following pathways: arcuate fasiciculus, cingulum, inferior longitudinal fasciculus, uncinate fasciculus, inferior fronto-occipital fasciculus, corpus callosum, fornix, and the internal capsule/corona radiata. The corpus callosum was further partitioned into five segments, as instructed by Hofer and Frahm. 52 Different segments have been found to project into specific cortical areas, which may have implications for association with psychiatric disorders. A set of “OR” gates were placed for each tract and reconstructed on the ICBM template to ensure appropriate correspondence with tracts displayed in the Catani and colleagues 51 atlas. In addition, a unique set of “NOT” gates was also placed for each tract to exclude fibers not belonging to the tract of interest. All tracts reconstructed for each participant were visually inspected to ensure appropriate registration was achieved from standard space, and that reconstruction was not compromised due to brain lesions. Tract-averaged FA was extracted for each white-matter pathway.
Along-tract analysis
Along tract analysis was conducted to provide additional within-tract information to better localize white-matter disruption. 53 To conduct such an analysis each participant's reconstructed tracts, obtained through the preceding atlas-based tractography, was processed in a number of steps. For each tract, a) streamlines were reoriented according to a common origin, b) were reparametrized with cubic B-splines, c) resampled so that each streamline had the same number of points—or vertices—along its length, d) resampled the underlying voxel volume to obtain, for this study, FA values at each of these points, and e) collapsed these values across the streamlines for each point along the tract to obtain average values. For each white-matter pathway, the number of points was determined by dividing the mean tract length by the voxel size, which in this study was 2 × 2 × 2 mm. For example, 88 mm/2 mm = 44 points.
Statistical analysis
Statistical analysis was conducted using Stata, version 14.1. 54 A linear regression was conducted for each white-matter pathway to examine differences in tract-averaged FA between controls, TBI-No Mood, and TBI-Mood groups. Age at MRI, gender, and years of education were controlled in all regression models due to apparent differences between the groups. Corrections for multiple comparisons were conducted following the tract-averaged regressions by controlling the false discovery rate (FDR) at p < 0.05. 55 In the current study, we were specifically interested in comparing the TBI-Mood group with the control and TBI-No Mood groups. The FDR procedure, therefore, corrected for multiple comparisons in regard to the following post hoc comparisons: TBI-Mood versus healthy controls and TBI-Mood versus TBI-No Mood.
Tracts that differentiated the TBI-Mood and TBI-No Mood groups following FDR correction were considered for the following along-tract analysis. A linear regression was conducted for each point along the tract controlling for age at MRI, gender, and years of education. Due to the high number of comparisons, an FDR correction was applied at p < 0.05. Similar to the tract-average analysis, for each tract only the post hoc comparisons of TBI-Mood versus healthy controls and TBI-Mood versus TBI-No Mood were considered for the FDR procedure.
Results
Sample characteristics
Individuals included in this study did not differ on important demographic and injury-related variables compared with participants in the prospective psychiatric study who were not imaged. These two samples did not differ on age at injury (t (201) = 0.70, p = 0.48), years of education (t (201) = 0.43, p = 0.67), or duration of PTA (t (200) = 0.69, p = 0.49). The distribution for gender (χ2 (2, N = 203) = 0.005, p = 0.94) and worst Glasgow Coma Scale (GCS) categories (χ2 (2, N = 193) = 0.90, p = 0.64) did not differ between the samples. The samples did not differ on proportion of pre-morbid mood (χ2 (2, N = 203) = 0.31, p = 0.58), anxiety (χ2 (2, N = 203) = 0.02, p = 0.89), psychotic (χ2 (2, N = 203) = 0.00, p = 1.00), or substance use disorders (χ2 (2, N = 203) = 0.05, p = 0.82). In addition, the samples did not differ in proportion of individuals reporting mood (χ2 (2, N = 203) = 3.17, p = 0.08), anxiety (χ2 (2, N = 203) = 0.33, p = 0.56), psychotic (χ2 (2, N = 203) = 0.02, p = 0.88), or substance use (χ2 (2, N = 203) = 0.16, p = 0.69) disorders at any time-point up to 3 years following their injury.
Statistically significant differences were found between the imaged healthy controls and the TBI groups (Table 1). Healthy controls did not differ on age at MRI scan compared with the TBI-Mood group (p = 0.64), but were younger than the TBI-No Mood group (p = 0.02). Controls were more highly educated, compared with both the TBI-Mood (p < 0.001) and TBI-No Mood groups (p = 0.002), and had a lower proportion of males compared with the TBI-Mood (p = 0.03) and TBI-No Mood groups (p = 0.03). Importantly, the TBI-Mood and TBI-No Mood groups did not differ from one another on age at MRI (p = 0.28), time between injury and MRI (p = 0.52), years of education (p = 0.29), duration of PTA (0.68), or the proportion of males (0.45) and worst GCS categories (0.93). In terms of functional outcomes, individuals in the TBI-Mood group were less likely to return to employment or study within the first 3 years following injury, compared with individuals in the TBI-No Mood group (see online Supplementary Table 2 at
Atlas-based whole-tract analyses
The primary analysis of interest was the comparison of the TBI-No Mood and TBI-Mood groups to examine the effect of mood disorders (See Fig. 2). It was evident, however, from Figure 2 that the TBI-Mood group also differed from healthy controls. After applying the correction for multiple comparisons, the TBI-Mood group displayed significantly lower tract-averaged FA values, compared with the TBI-No Mood group, for the right arcuate fasciculus, right inferior longitudinal fasciculus, first and second segments of the corpus callosum, as well as the left and right fronto-occipital longitudinal fasciculi.

Results of linear regression analyses modeling fractional anisotropy (FA), controlling for age, years of education, and gender. The plots present the mean FA for each group (thick horizontal line), standard deviation error bars, and the each individual's adjusted FA. Only comparisons between the two traumatic brain injury (TBI) groups were considered for post hoc significance testing. Tracts presented are only those for which a significant difference was observed between TBI individuals with and without a mood disorder, controlling for multiple comparisons using the Simes false discovery rate (FDR). Significant tracts were the right arcuate fasciculus, the right inferior longitudinal fasciculus, the first and second sections of the corpus callosum, as well as the left and right fronto-occipital fasciculi. Color image is available online at
Along-tract analyses
Along-tract results for the significant tract-average white matter pathways after controlling for multiple comparisons using an FDR of p < 0.05are presented in Figure 3. No significant along-tract differences in FA were found between the TBI-No Mood and TBI-Mood group for the right arcuate fasciculus. Lower FA in anterior, medial, and posterior portions of the right inferior longitudinal fasciculus were found for the TBI-Mood group, compared with TBI-No Mood participants. The TBI-Mood group displayed lower FA values along the entire first segment of the corpus callosum, except for the left most points. The TBI-Mood group displayed lower FA values only for the medial portion of the second segment of the corpus callosum and the left fronto-occpital white matter pathways, compared with the TBI-No Mood group. Lower FA in anterior points, however, differentiated the TBI-Mood and TBI-No Mood groups of the right fronto-occpital fasciculus.
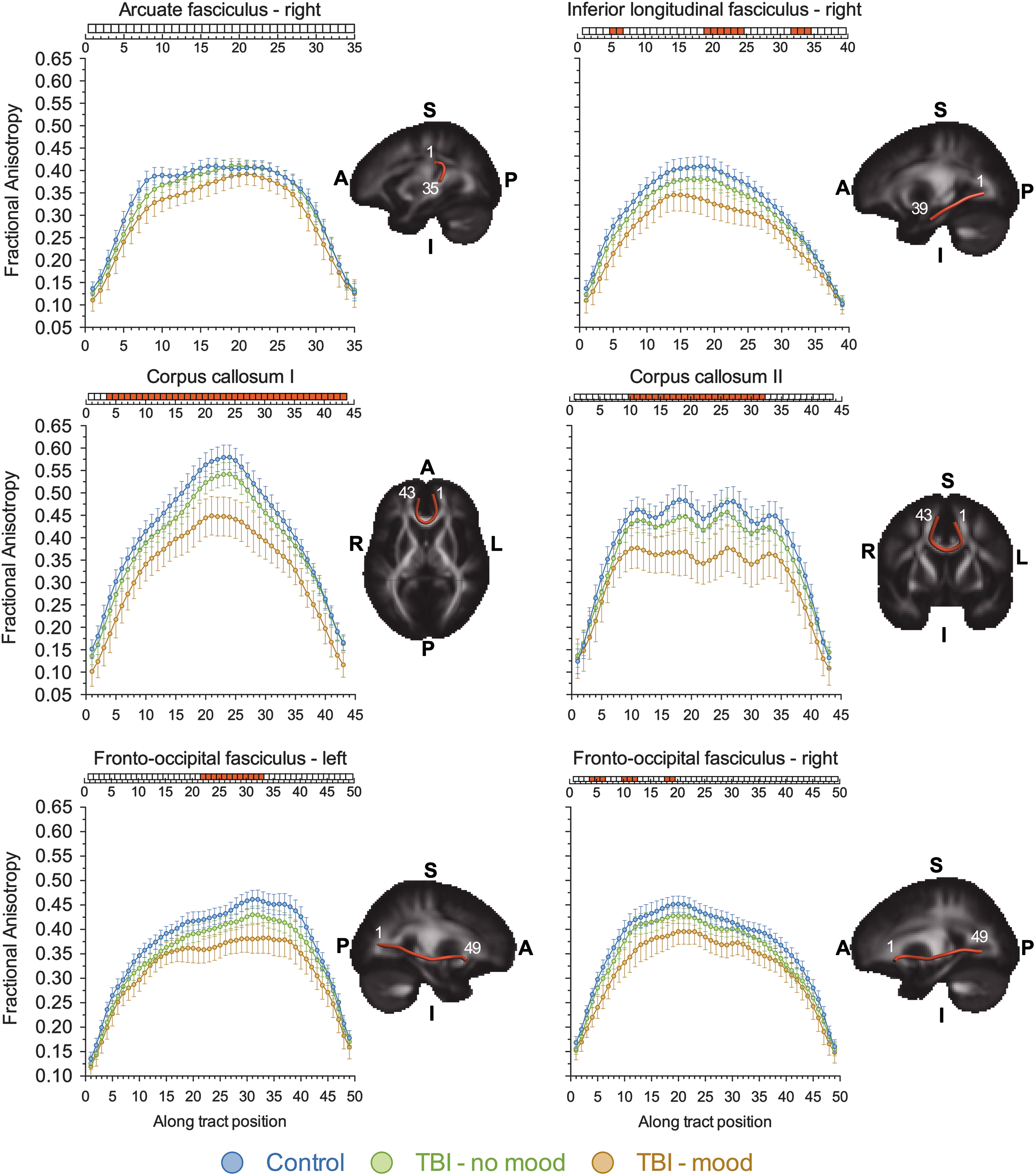
Results of the along-tract analysis for tracts that previously differentiated traumatic brain injury (TBI) individuals with and without a diagnosed mood disorder for the tract-averaged analysis. Mean fractional anisotropy (FA) is presented along each tract section for the right arcuate fasciculus, the right inferior longitudinal fasciculus, the first and second sections of the corpus callosum, as well as the left and right fronto-occipital fasciculi. A significance bar is presented above each tract highlighting tract sections that significantly differentiated TBI individuals with and without a diagnosed mood disorder. Significant comparisons, after correction, are presented in red. Correction for multiple comparisons was conducted using the Simes procedure for controlling the false discovery rate (FDR). Along-tract reconstructions are presented for each brain tract, superimposed on the ICBM template. The numbers in white provide a reference guide to interpret the corresponding brain location for each along-tract position. A, anterior; P, posterior; S, superior; I, inferior; L, left; R, right. Color image is available online at
Discussion
The current study examined the relationship between diagnosed mood disorders and white matter pathology following TBI. As expected, individuals with TBI displayed widespread disruption within white matter tracts, compared with healthy control participants. Individuals who developed a mood disorder following TBI displayed greater white matter disruption compared with participants who did not have a mood disorder. The pattern of white matter disruption, identified using diffusion tensor tractography, provides additional support for a neurobiological role for post-TBI mood disorders, in accordance with the cortical-limbic dysregulation model. 9,11,13
Tract-averaged reductions in FA for individuals with post-TBI mood disorder were identified within the right arcuate fasciculus, right inferior longitudinal fasciculus, as well as the fronto-occipital fasciculus bilaterally. The arcuate fasciculus provides connectivity between the frontal and temporal lobes, the inferior longitudinal fasciculus connects visual areas to the amygdala and hippocampus, whereas the fronto-occipital fasciculi connect the occipital lobe to the orbitofrontal cortex. 51 Reduced connectivity to the temporal lobes likely interacts with emotion regulation circuits within limbic and basal ganglia regions, given these lie within the temporal lobes. 9 The orbitofrontal cortex is also a critical region for mood regulation. 13 Disrupted connectivity affecting the hippocampus, ventral frontal, and amygdala regions, for instance, is hypothesized to cause mood dysregulation by inducing a pathological increase in activation of these regions. 9,56
Reduced FA was identified in the two most anterior regions of the corpus callosum, which displayed strong associations with post-TBI mood disorders. Subregion I comprises the superior and inferior genu, as well as the rostrum of the corpus callosum, projecting fibers to the prefrontal cortex. Subregion II of the corpus callosum comprises the posterior genu and anterior midbody, with fibers projecting to pre-motor and supplementary motor cortical areas. Subregion I of the corpus callosum displayed the strongest association with mood disorders in the current study. This supports much of the literature within the TBI field, which has most frequently implicated frontal pathology—including presence of lesions and reduced regional volume—in post-injury mood disorders. 2,19 These two most anterior subdivisions of the corpus callosum were also found to differentiate between depressed and non-depressed mild TBI patients in a recent study using DTI. 41 Interestingly, encircling these two anterior subregions of the corpus callosum is the cingulate cortex, which comprises subregions arguably most vital for emotion regulation. 9,11,13,57 This includes the dorsal, rostral, and ventral cingulate. The dorsal compartment is hypothesized to modulate the attentional and cognitive aspects of mood, whereas ventral regions relate to the vegetative and somatic aspects. The rostral cingulate is critical for maintaining homeostasis between these two compartments.
Going beyond track-averaged FA and examining along-tract differences provided further insight into mood-related pathology. We expected that differences between the TBI-Mood and TBI No-Mood groups would be greatest as tracts coursed toward temporal and frontal regions. Some evidence for this was present in the left and right fronto-occipital fasciculi, as differences between groups were skewed, such that differences were greatest at anterior positions along the tracts. This pattern was not evident for the inferior longitudinal fasciculus, however, where differences were evident in posterior, mid, and anterior regions, as well as the corpus callosum subregions, which displayed the greatest differences mid-tract. Despite some mixed findings regarding the along-tract analysis, presenting finer-grained analysis of tracts in addition to tract-average results is recommended to aid interpretation of findings.
The study findings provide further support for a neurobiological basis for mood disorders following TBI. The Mood and No-Mood TBI groups had similar rates of pre-morbid mood and anxiety disorders as well as similar levels of injury severity. These results should not detract from models and other studies that emphasise the role of pre-morbid, personal, and environmental factors in the development and maintenance of mood disorders. 8,58,59 Instead, the underlying neuropathology should be incorporated into biopsychosocial models for more accurate classification of mood subtypes as well as for the delivery of more effective treatments. Establishing differences between individuals regarding the underlying brain pathology may assist in explaining why two individuals respond differently to similar injuries. In addition, distinct profiles of brain pathology following TBI could explain why treatments for mood disorders fail for certain individuals. Unlike idiopathic mood disorders, where brain circuitry may be preserved, damage to brain circuitry following TBI potentially restricts the likelihood of achieving homeostasis of emotional regulation.
Future studies should examine these specific issues relevant to psychiatric disturbance following TBI. Studies should be conducted that recruit larger samples of TBI participants with mood disorders to examine potential subgroups in relation to mood diagnosis criteria; that is, whether individuals can be categoriszd into primarily cognitive, somatic, or emotional subtypes. In turn, mood subtypes may have a common neuropathological profile that is consistent with the cortico-limbic model. Additionally, treatment studies for depression, anxiety, and other psychiatric disorders should examine differences in the underlying brain circuits for responders and non-responders. Individuals who respond to treatment may have relatively more preserved emotion regulation circuitry compared with treatment-resistant patients.
Strengths and limitations
The present study used a neuroimaging analysis pipeline that minimized bias introduced by conducting tractography on each participant's native DTI image. Instead, tracts were reconstructed by using an atlas-based approach that warped seed, inclusion, and exclusion gates delineated on standard templates to each participant's native-space images. In addition, tracts were resampled to obtain more detailed information of pathology at multiple positions along the tract. To our knowledge, this tract resampling technique has not been applied before within the TBI field. Mood disorders were diagnosed in the current study using the SCID-I for DSM-IV-TR, which is a semi-structured clinical interview and considered the gold-standard approach. Other studies have relied on self-report rating scales, such as the Beck Depression Inventory (BDI), that may not reliably capture clinical significant mood disturbance, nor distinguish mood from injury-related symptoms.
The current study examined mood in a relatively small sample of individuals with TBI. Despite an unbiased tractography pipeline and controlling for Type I errors by considering the FDR, the results need to be replicated. The TBI sample did not differ from the larger psychiatric study from which this subgroup stems, however, and the results align well with the literature. Caution, is required, however, given that the TBI-Mood group in the current study had a greater frequency of pre-morbid substance-use disorders compared with TBI-No Mood participants. Reduced regional gray matter volume has been demonstrated in individuals with TBI who had alcohol abuse or dependence. 43 Future studies are needed to disentangle the effect of premorbid substance use, brain pathology, and mood disorder diagnosis.
The study results further support the Mayberg model by showing that structural changes in white matter circuitry may play a role in the development of mood disorders. However, the study is limited in its ability to demonstrate hypo- and hyper-activation of certain brain regions or compartments within this model. Combining functional with structural neuroimaging in future studies will enable research to examine whether specific features of depression, for example cognitive or somatic symptoms, are associated with regions displaying over- or under-activation.
Conclusions
Mood disorders following TBI are associated with reduced white matter integrity in multiple tracts connecting to temporal and frontal brain regions. There is a need to integrate TBI-related neuropathology in conceptual models of mood disorders following TBI. Doing so has the potential to improve the management of mood disorders by tailoring treatment approaches to underlying neuropathology.
Footnotes
Acknowledgments
Dr. Spitz and Professor Ponsford had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author contributions: data collection: Spitz, Gould, Alway; analysis: Spitz; writing and editing: Spitz, Gould, Alway, Ponsford.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.