
Abstract
Clinical studies suggest that athletes with a history of concussion may be at risk for additional mild traumatic brain injury (mTBI), and repetitive exposure to mTBI acutely increases risk for more significant and persistent symptoms and increases future risk for developing neurodegenerative diseases. Currently, symptoms of mTBI are managed with rest and pain medication; there are no drugs approved by the Food and Drug Administration (FDA) that target the biochemical pathology underlying mTBI to treat or prevent acute and long-term effects of repetitive mTBI. Memantine is an FDA-approved drug for treating Alzheimer's disease, and also was shown to be neuroprotective in rodents following a single, moderate to severe TBI. Therefore, we investigated the potential for memantine to mitigate negative outcomes from repetitive mild stretch injury in organotypical hippocampal slice cultures. Samples received two injuries 24 h apart; injury resulted in significant cell death, loss of long-term potentiation (LTP), and astrogliosis compared with naïve, uninjured samples. Delivery of 1.5 μM memantine 1 h following each stretch significantly reduced the effect of injury for all outcome measures, and did not alter those outcome measures that were unaffected by the injury. Therefore, memantine warrants further pre-clinical and clinical investigation for its therapeutic efficacy to prevent cognitive deficits and neuropathology from multiple mTBIs.
Introduction
D
Although there are therapeutics approved by the Food and Drug Administration (FDA) for treating the symptoms of neurodegenerative diseases, there are no cures for these pathologies. Currently, symptoms of mTBI are managed with rest and pain medication; there are no drugs approved by the FDA that target the biochemical pathology underlying mTBI to treat or prevent acute and long-term effects of repetitive mTBI. 3 An ideal therapeutic for mTBI would treat the injury, be effective when administered after the injury, and have no negative side effects. Additionally, drugs previously approved by the FDA, even for indications other than mTBI, may be especially amenable for expedited approval for additional indications, such as TBI or mTBI, given their known mechanism(s) of action and toxicology.
N-methyl-
Furthermore, memantine is an FDA-approved drug for the treatment of moderate to severe Alzheimer's disease and is also used clinically for the treatment of some patients with Parkinson's disease. 18 Memantine does not have the significant negative side effects, such as hallucinations and coma, of other NMDAR antagonists. 17,18,22 –24 In recent clinical trials of Alzheimer's disease, patients receiving memantine (20–40 mg/day) experienced side effects including rare dizziness and occasional restlessness or agitation, and were only reported for the highest doses. 17
In this study, we investigated the potential for delayed administration of memantine to improve outcome from repetitive mTBI using a well-characterized stretch injury model to expose organotypic hippocampal slice cultures (OHSCs) to biomechanics relevant to concussion. 25,26 Previously, we reported that repetitive mild stretch injury resulted in significant cell death, loss of long-term potentiation (LTP), astrogliosis, and dendritic damage, all of which were increased compared with a single mild mechanical stimulus. 26 Here, memantine, administered 1 h after each of two mild stretch injuries delivered 24 h apart, significantly reduced cell death, gliosis, and deficits in LTP. Memantine did not cause aberrant neuronal function or alter immunohistology not affected by repetitive injury. These findings suggest that memantine may mitigate pathologies that can result from multiple mTBIs, and with further pre-clinical and clinical testing, memantine may be a promising strategy for improving the quality of life for those who have sustained multiple mTBIs.
Methods
Organotypical hippocampal slice cultures
All animal procedures were approved by the Columbia University Institutional Animal Care and Use Committee (IACUC). Methods for generating and maintaining OHSCs have been published previously.
24
Sprague–Dawley rat pups ages P8–10 were decapitated, the brain and hippocampi were excised, hippocampi were sectioned into 400 μm thick slices, and slices were plated onto the silicone membrane of a custom well (Specialty Manufacturing, Saginaw, MI). Wells were coated with poly-L-lysine (0.32 mg/mL; Invitrogen, Carlsbad, CA) and laminin (0.08 mg/mL; Invitrogen) prior to culture. Cultures were initially fed with Neurobasal medium (Neurobasal-A supplemented with 1 mM GlutaMAX, 1X B27 supplement, 10 mM HEPES, 25 mM
Stretch injury
The stretch injury device and injury mechanism have been published and characterized in detail. 25 For each well of cultures receiving the injury, an equi-biaxial stretch injury was achieved with controlled strain and strain rate by displacing the well and silicone substrate over a hollow, cylindrical indenter. 25 Both substrate and tissue strains were verified via image analysis of high-speed video of the injury using custom MatLab code (Natick, MA). Stretch injury was equi-biaxial with an average equi-biaxial stain of 12.9% and an average strain rate of 5.1 sec−1. The injury device was maintained at 37°C during experimentation. Following injury, all samples were returned to fresh, pre-warmed full-serum medium, incubated, and rocked.
Memantine
For all injured samples, one hour following stretch, all culture medium was removed from each well and replaced with full-serum medium containing either 1.5 μM memantine (Sigma) or the vehicle (phosphate- buffered saline solution [PBS]; Sigma) (Fig. 1). One hour after the first injury, the medium was exchanged with either drug- or vehicle-containing medium, which incubated with samples for 23 h until the second injury time point. Immediately prior to the second injury, the medium was removed, the injury was performed, and fresh full-serum medium was added to each well. One hour following the second injury, the medium was replaced with drug- or vehicle-containing medium that incubated with samples until the time point indicated. Samples were returned to the rocker and incubated without further media changes for 72 h until cell death was evaluated and electrophysiological recordings were begun. Two sets of naïve samples were collected to both evaluate the health of uninjured OHSCs and to determine if additional medium changes to administer the vehicle/memantine had an effect on outcome measures. One set of naïve samples was imaged on Day 0 (Fig. 1), returned to fresh full-serum medium, fed 24 h later, and left undisturbed until Day 4 when propidium iodide (PI) images were taken and electrophysiological recordings began. One set of naïve samples was imaged on Day 0, was returned to fresh full-serum medium, and received a full medium change 1 h later in lieu of vehicle/memantine administration; these samples received a full media change to fresh full-serum medium 24 h later and again 1 h later in lieu of vehicle/memantine administration.
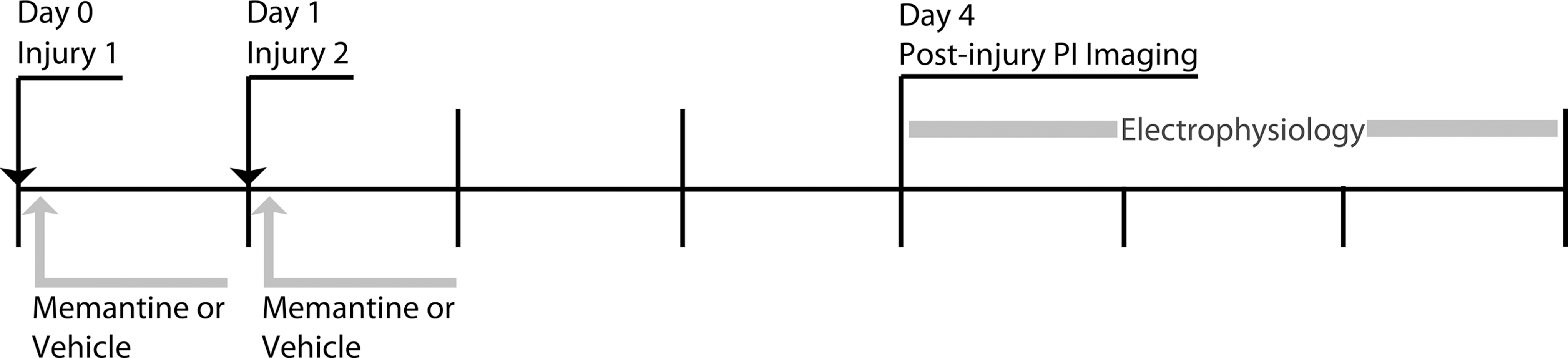
Experimental injury and drug delivery paradigm. Samples were stretched twice, 24 h apart. Medium containing the memantine or the vehicle was added to samples 1 h following the first injury, and remained on the samples until the time of the second injury. Following the second injury, samples received fresh full-serum media, which was changed to memantine- or vehicle-containing media 1 h following the injury. Additional naïve samples received medium changes at the time points for injury and memantine/vehicle administration or no additional media changes. Cell death was evaluated with propidium iodide (PI) on Day 0 and Day 4, and electrophysiological function was subsequently evaluated through Day 6.
Cell death quantification
PI, a fluorescent indicator of dead cells, was used to quantify cell death present in OHSCs immediately prior to the first injury and 72 h following the second injury time point.
27
For staining, OHSCs were incubated in 1.5 μM PI in serum-free medium (75% Minimum Essential Medium, 25% Hank's Balanced Salt Solution, 2 μM GlutaMAX, 25 mM
Electrophysiological recordings
Methods for recording and quantifying electrophysiological have been previously published. 27,29 Electrophysiological recordings were performed 72–120 h following the second stretch injury. Neuron activity was recorded with 60 channel microelectrode arrays (8 × 8 electrode grid, 30 μm electrode diameter, 200 μm electrode spacing; multi-electrode array [MEA], Multi-Channel Systems, Reutlingen, Germany). Before a recording, each sample was carefully inverted onto an MEA. The sample was held in place with a nylon mesh harp slice grid (ALA Scientific Instruments, Farmingdale, NY) and gently perfused with artificial cerebral spinal fluid (aCSF) (125 mM NaCl, 3.5 mM KCl, 26 mM NaHCO3, 1.2 mM KH2PO4, 2.4 mM CaCl2, 1.3 mM MgCl2, 10 mM HEPES, and 10 mM glucose; pH 7.4) that was warmed and bubbled with 5% CO2 and 95% O2. 29 For all recordings within a slice, the same two electrodes located in the Schaffer collaterals (SC) were stimulated.
Stimulus-response (S-R) curves were generated as previously described.
27,29
A constant current, bipolar, biphasic stimulus (100 μs positive phase followed by a 100 μs negative phase) was applied to the stimulating electrodes. Stimulus magnitude was gradually increased 0–200 μA in 10 μA increments, and evoked responses were recorded from all nonstimulating electrodes. The range of peak-to-peak responses for each electrode was fit to a sigmoidal curve with the following equation:
30
As described previously, Rmax represents the maximum peak-to-peak amplitude of the evoked response, I50 represents the current necessary to generate a half of Rmax , and the term m is proportional to the slope of the linear portion of the sigmoidal fit. 27,29 These three parameters were calculated for each electrode. Images of each sample on the MEA were used to identify the location of each electrode (DG, CA3, CA1). Subsequently, an average of each parameter was calculated for each ROI and slice.
Short-term plasticity was evaluated by calculating paired-pulse ratios (PPRs), as previously described. 27,29 Samples were stimulated twice at the I50 , and the interstimulus interval (ISI) was varied from 20 to 2000 ms. PPRs were calculated as the ratio of the peak-to-peak response elicited by the second stimulus as compared with that of the first stimulus in a pair. ISIs were assigned to bins—short term ISI (20 ms), early-mid ISIs (35–100 ms), late-mid ISIs (140–500 ms), and long-term ISIs (> 500 ms), and an average PPR for each ROI, slice, and bin was calculated.
LTP was evaluated utilizing methods previously published. 27,29 Peak-to-peak response to I50 stimulation was recorded for 30 min, stimulating every 60 sec. Immediately after this baseline recording, LTP was induced by stimulating at the I50 with three successive, 1 sec long, 100 Hz trains with 10 sec breaks between trains. The post-induction response was recorded for 60 min, stimulating at the I50 , stimulating every 60 sec. Percent potentiation was calculated as the percent increase in peak-to-peak response of the post-induction recording normalized to the pre-induction recording. The average response of the last 10 min of pre- and post-induction recordings was used for calculations. Potentiation was calculated for electrodes within the CA1 in response to SC stimulation only.
Histology and immunohistology
Histology and immunohistology methods have been previously published. 27 A subset of samples from each experimental group were fixed with neutral buffered 10% formalin (Sigma) for 30 min, dehydrated in a gradient of alcohols and xylene, embedded in paraffin, and cut into 6 μm thick sections. For histology, sections were stained with hematoxylin and eosin (H&E) (Gill's Hematoxylin 3 and Eosin Y, Thermo Fisher Scientific, Waltham, MA), dehydrated with a gradient of alcohols, and mounted on slides for routine pathological analysis. For immunohistology, separate sections were stained with an antibody for microtubule associated protein 2 (MAP-2) (anti-MAP2 AB5622, Millipore; 1:100), an antibody for phosphorylated neurofilament heavy (pNF-H) (SMI-31, BioLegend, San Diego, CA; 1:500), an antibody for glial fibrillary acidic protein (GFAP) (anti-GFAP Ab7260, Abcam, Cambridge, MA; 1:2000), and an antibody for ionized calcium-binding adapter molecule 1 (IBA1) (anti-IBA1, Wako Pure Chemical Industries, Richmond, VA; 1:400). Negative controls received identical handling but were not incubated with the primary, for each stain respectively.
Samples were analyzed semiquantitatively by an individual blinded to the sample group using a rubric previously published. 27 Staining was graded on a continuous scale (0–3), using specific indicators of pathology for each stain, as previously described. 27 H&E was used to assess integrity of the principal cell layers, and stained sections were evaluated for shrunken neurons, vacuolization, neuronal loss, and dark neurons (0, none; 1, rare; 2, occasional; 3, frequent). For MAP-2 and SMI-31, intensity and consistency of each stain's immunoreactivity was assessed (0, uniform staining; 1, patchy loss of staining; 2, extensive loss of staining; 3, complete loss of staining). Relative presence of GFAP-positive cells was assessed (0, no GFAP expression; 1, minimal number of GFAP-positive astrocytes; 2, moderate number of GFAP-positive astrocytes; 3, large number of GFAP-positive astrocytes). Presence and morphology of cells positive for IBA1 was assessed (0, no IBA1 expression; 1, minimal number of IBA1- positive cells; 2, moderate number of IBA1-positive cells with varying presence of activated microglia [amoeboid shape] and macrophages; 3, high number of IBA1-positive cells with large numbers of activated microglia and macrophages).
Statistical analysis
To evaluate efficacy of memantine to change any outcome measure (cell death, S-R, PPR, LTP, GFAP, IBA1, SMI-31, or MAP2), a one way ANOVA was used to determine statistically significant changes in that measure (SPSS v. 19, IBM, Armonk, NY). For cell death, S-R measures, and PPR ISI bins, statistical analysis was performed on data for each ROI separately. A Bonferroni post-hoc analysis was performed for data sets with significance in the ANOVA. For semiquantitative measures, a Dunnett post-hoc analysis was performed for data sets with significance in the ANOVA. Significance was set to *p < 0.05 for all analyses.
Results
Cell death from repetitive mild stretch injury was mitigated by memantine treatment
Cell death was >8% in each ROI (DG, CA3, CA1) for samples receiving repetitive injury and the vehicle (Fig. 2). Cell death was significantly reduced in all ROI in OHSCs that received the repetitive injury and memantine. There was no significant difference in cell death between samples receiving memantine and naïve samples. Cell death from the two naïve groups was not significantly different and was combined into one “naïve” data set that was used for statistical comparison to vehicle and memantine groups.
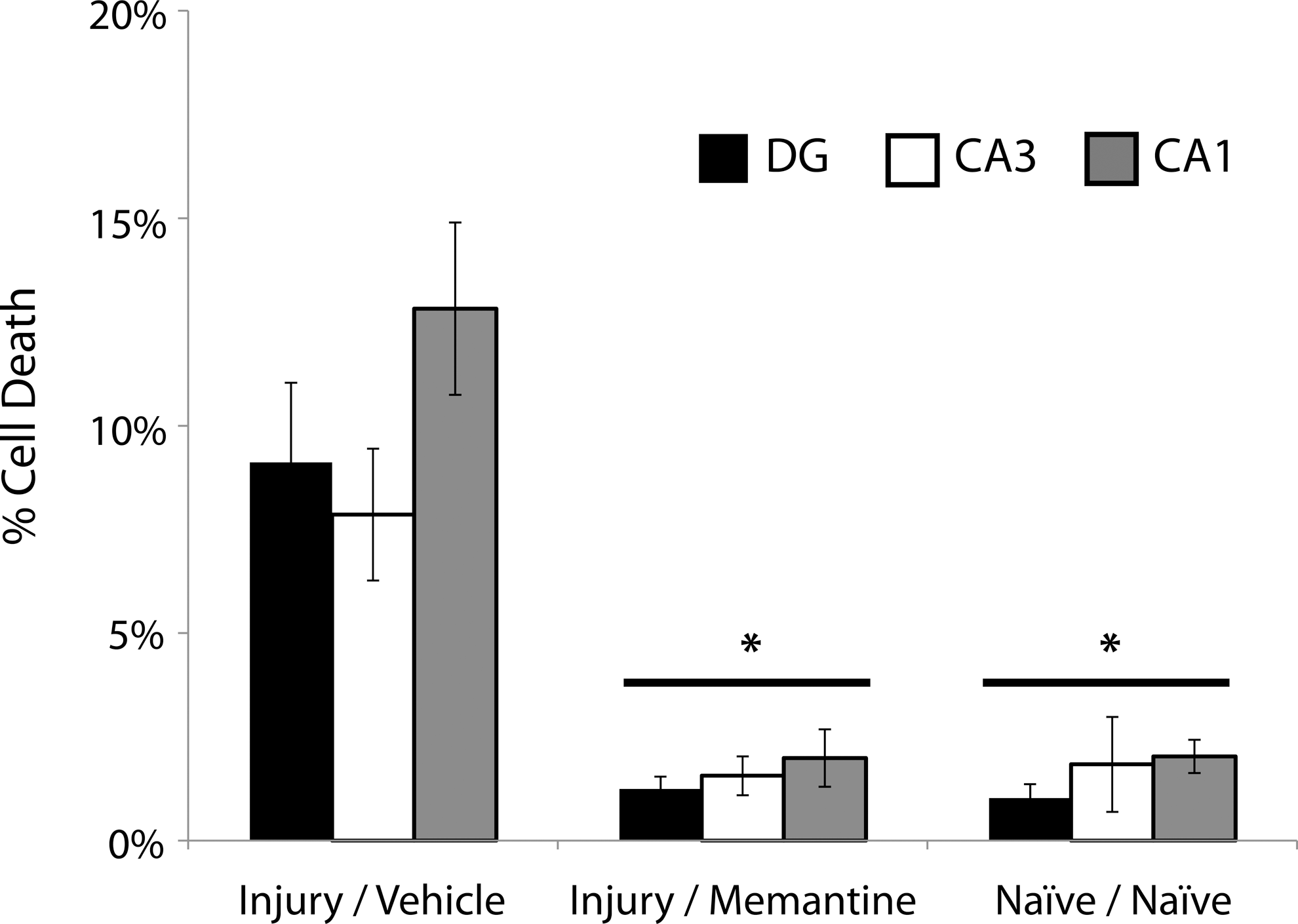
Cell death was reduced by delayed memantine delivery. Cell death was significantly increased in all regions of organotypic hippocampal slice cultures (OHSCs) (dentate gyrus [DG], cornu ammonis [CA]1, CA3) by repetitive mild stretch injury compared with in naïve samples, and memantine significantly reduced cell loss from repetitive injury (n ≥ 20, ± SEM, *p < 0.05, as compared with vehicle for each region of interest [ROI], respectively). There was no significant difference in cell death between the injured samples receiving memantine and naïve samples for all ROI.
LTP deficits from repetitive mild stretch injury were mitigated by memantine treatment
Percent potentiation of samples that received the repetitive injury and the vehicle was 15% (Fig. 3), and percent potentiation of samples that received repetitive injury with memantine was 50%. Percent potentiation of samples receiving memantine was significantly higher than that of samples receiving the vehicle, and was not significantly lower than that of naïve samples, which was >60%. LTP from the two naïve groups was not significantly different and was combined into one “naïve” data set that was used for statistical comparison to vehicle and memantine groups for Figure 3.
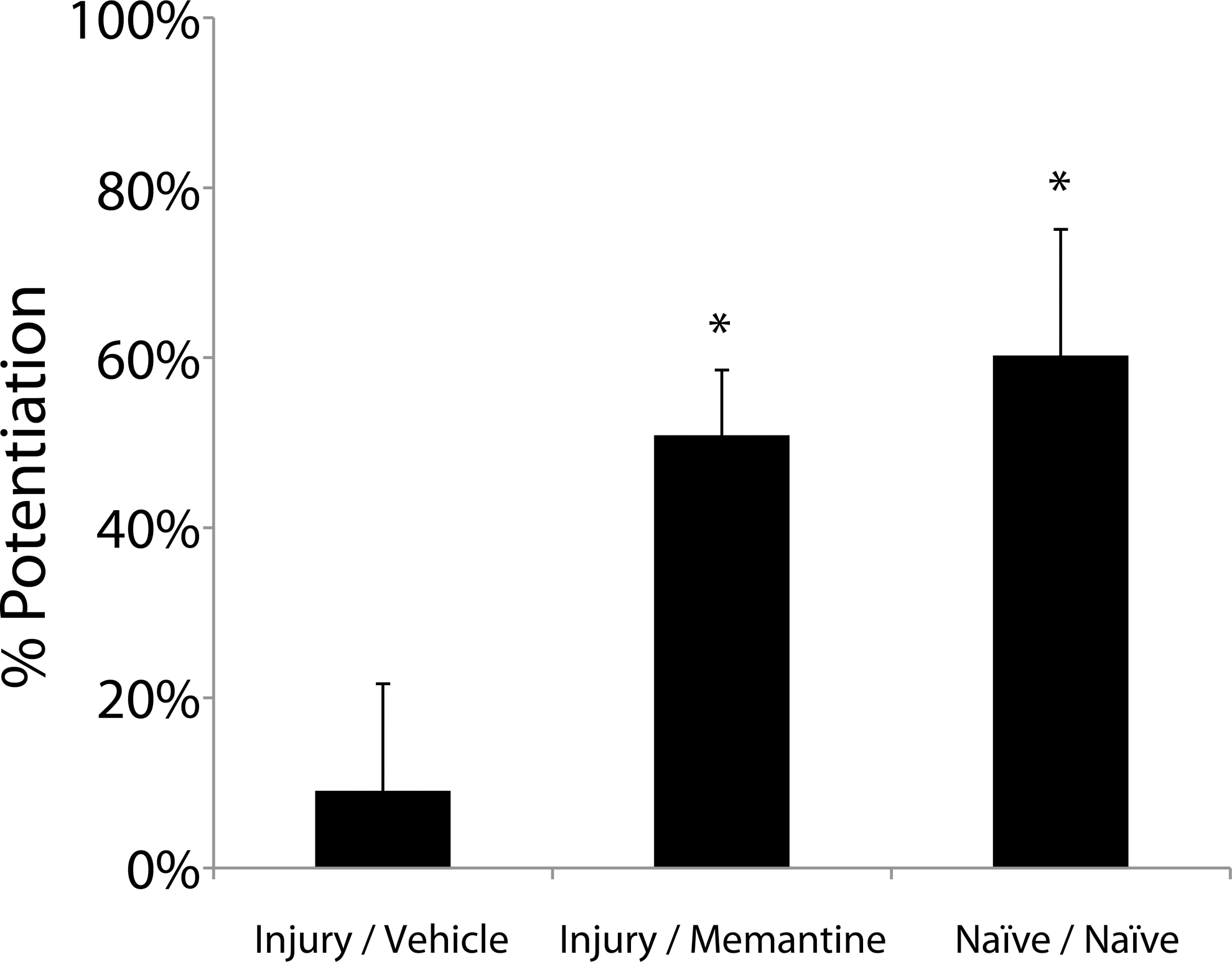
Long-term potentiation was improved by delayed administration of memantine. Percent potentiation was significantly reduced by repetitive mild stretch injury compared with naïve samples, and memantine significantly increased long-term potentiation (LTP) following repetitive mild stretch injury (n ≥ 6, ± SEM, *p < 0.05). There was no significant difference between injured, memantine-treated samples and naïve samples.
S-R parameters were not significantly modified by repetitive stretch injury or memantine treatment
There was no significant difference in any S-R parameter (I50, Rmax, m) among samples receiving repetitive injury and the vehicle or memantine as well as uninjured, naïve samples (Fig. 4). S-R parameters from the two naïve groups were not significantly different and were combined into one “naïve” data set that was used for statistical comparison to vehicle and memantine groups for Figure 4.
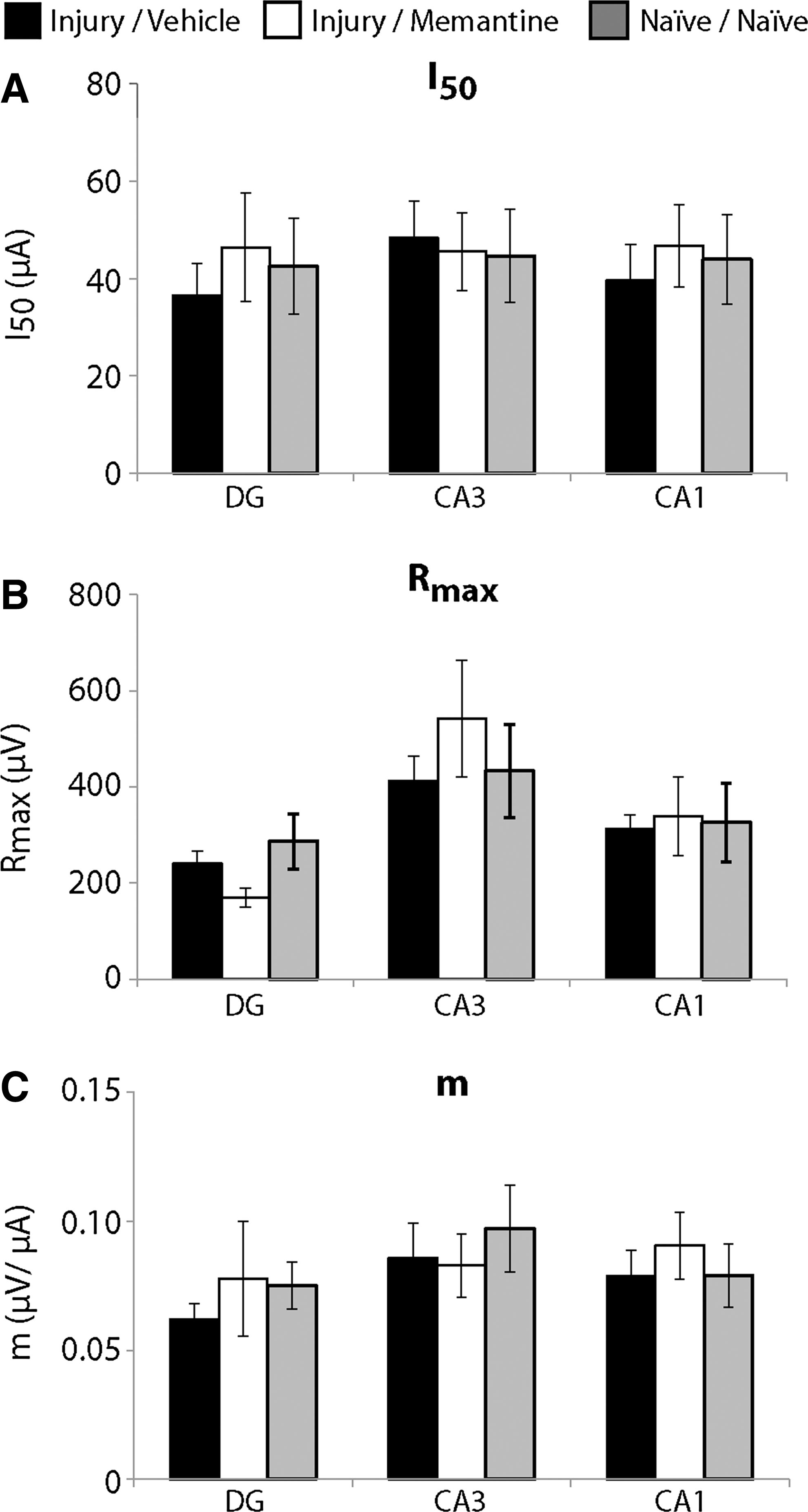
Stimulus-response parameters were not modified by repetitive injury or memantine administration.
PPRs were mostly unaltered by repetitive stretch injury or memantine treatment
There was no significant difference in PPR for any ISI bin (short-term, early-mid, late-mid, late-term) among samples receiving repetitive injury and the vehicle or memantine and naïve samples (Fig. 5) with one exception. In the CA1 for the early-mid ISIs, PPRs for injured, memantine-treated samples was significantly higher than for injured, vehicle samples (Fig. 5B); the average PPR for the memantine-treated group was not significantly different than that for naïve samples. PPRs from the two naïve groups were not significantly different and were combined into one “naïve” data set that was used for statistical comparison to vehicle and memantine groups for Figure 5.
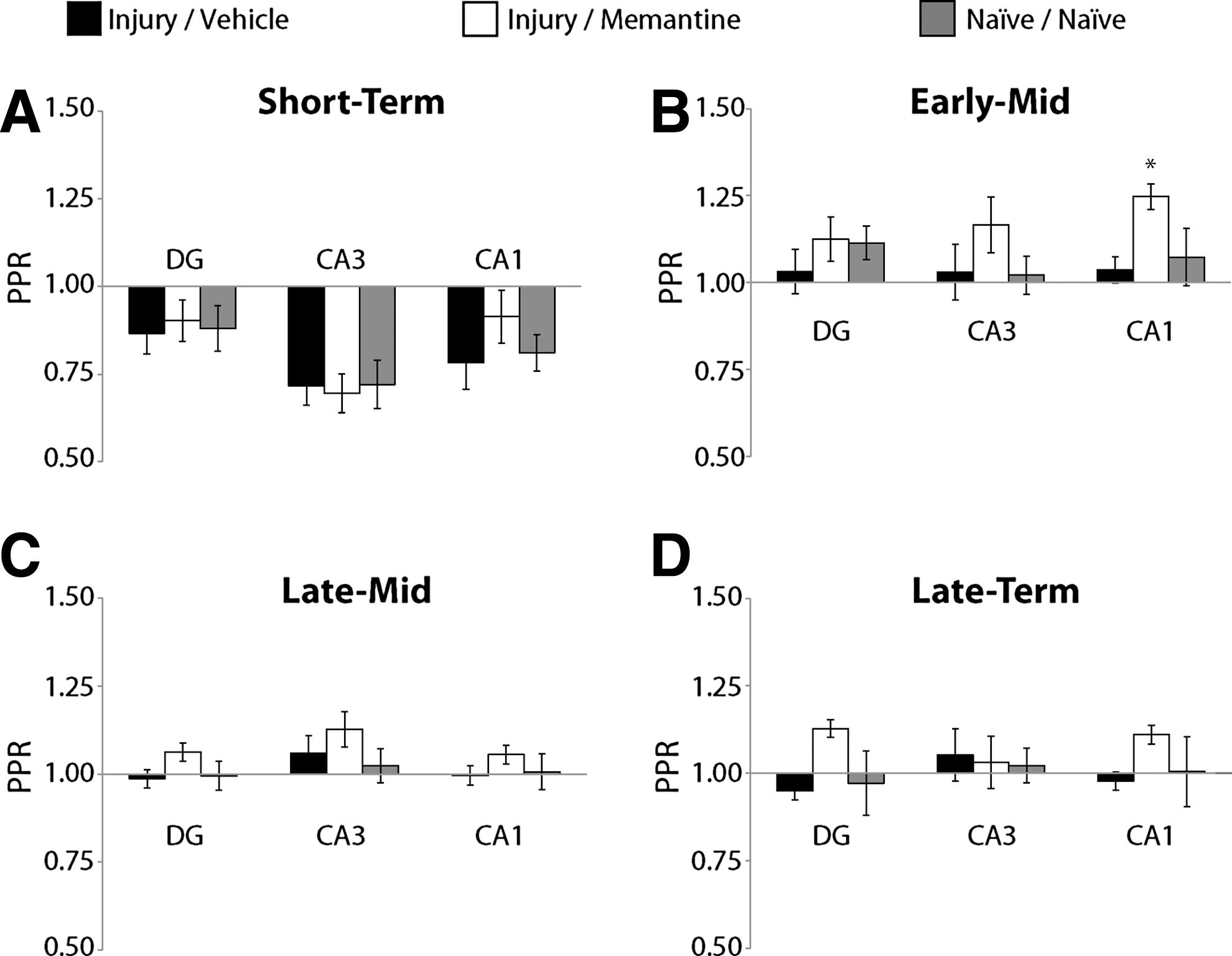
Short-term plasticity was mostly not altered by repetitive injury or memantine administration.
Cell loss and astrogliosis were prevented by memantine treatment
Semiquantitative H&E grade was significantly lower, corresponding to improved outcome, for samples that were injured and received memantine compared with that of samples that were injured and received the vehicle (Fig. 6A). Similarly, H&E grade for naïve samples was significantly lower than that of the injured samples that received the vehicle. Cell loss from repetitive injury was isolated to the principal cell layers and was observed predominantly in the CA1 region of OHSCs (Fig. 6B and C), whereas the principal cell layers appeared continuous and healthy in injured samples that received memantine (Fig. 6D and E).
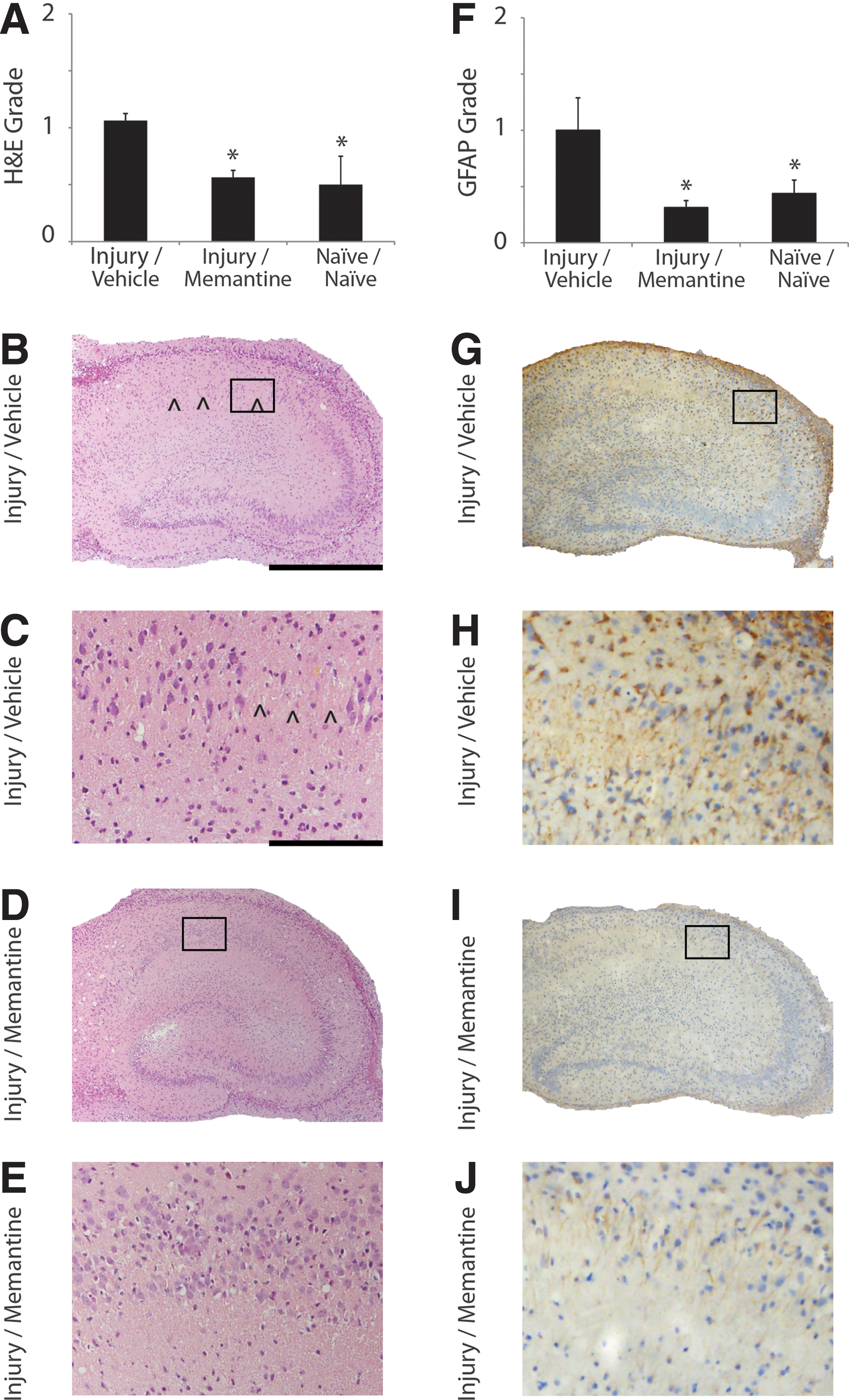
Histology and immunohistology.
Semiquantitative GFAP grade was significantly lower, corresponding to improved outcome and reduced astrogliosis, for injured samples that received memantine compared with that of injured samples that received the vehicle (Fig. 6F). GFAP grade was significantly lower for the naïve samples compared with the injured samples that received the vehicle. Density of GFAP-positive cells was increased in all ROIs in samples that received repetitive injury and the vehicle (Fig. 6G and H) compared with that of injured samples that received memantine (Fig. 6I and J).
There was no observed difference in IBA1, SMI-31, or MAP-2 immunoreactivity among all samples (images not shown). Semiquantitative analysis of all samples stained with IBA1, SMI-31, or MAP-2 antibodies did not reveal any significant difference among experimental groups (data not shown).
Semiquantitative grades for H&E, GFAP, IBA1, SMI-31, and MAP-2 for the two naïve groups were not significantly different and were combined into one “naïve” data set that was ultimately used for statistical comparisons.
Discussion
In this study, memantine effectively treated electrophysiological and pathological changes resulting from repetitive mild stretch injury. Memantine improved several outcome measures modified by repetitive mild stretch injury and did not alter those outcome measures that were unaffected by the injuries. Additionally, memantine was effective when administration was delayed 1 h following the injuries. Currently, there are no FDA-approved therapies that prevent changes in brain function and pathology that can result from repetitive mTBI. Given that memantine is FDA-approved for Alzheimer's disease, it may have a more expeditious approval for other indications such as mTBI, making it potentially a successful therapeutic candidate for mTBI treatment.
Using the same stretch injury model and injury biomechanics used in this study, we previously reported that repetitive mild stretch injuries delivered 24 h apart without therapeutic intervention resulted in a significant increase in cell death, loss of LTP, astrogliosis, and dendritic damage. 26 Other studies of repetitive mTBI in vivo and in vitro suggest that repetitive mTBI can result in cell loss, LTP deficits, and gliosis. 26,31 –34 Here, we reproduced our findings from the previous work for the 24 h inter-injury interval, and we reported that memantine treatment rescued LTP. 26 In this study, repetitive mild stretch injury did not significantly change PPR or S-R parameters from those of the naïve OHSCs, and these measures were not affected by memantine treatment. We reported similar findings in our previous work on repetitive mild stretch injury, suggesting that repetitive mild stretch injury does not alter basal function electrical activity in response to external electrical stimulation. 26 This finding is also significant because an ideal therapeutic drug would rescue only those outcome measures modified by the injury with minimal off-target effects. Therefore, repetitive mild stretch injury may initiate injury mechanisms that preferentially affect LTP. Additionally, in a mouse model of cerebral ischemia, memantine delivered pre-injury reduced neuronal injury, neuronal apoptosis, and astrogliosis. 35 Incubation in 1 μM memantine, which is the memantine concentration in the cerebral CSF of dementia patients treated with this drug, rescued LTP deficits of hippocampal slices induced by reduced Mg2+ exposure leading to overactivation of NMDARs. 36 We similarly reported in this study and in our previous work that repetitive mild stretch injury resulted in astrogliosis, and here, memantine prevented astrogliosis from repetitive mTBI. 26
Given that memantine preferentially targets NR2B-containing NMDARs, electrophysiological and pathological effects of repetitive mTBI may be mediated by overactivation of these receptors. 19,24 Previous studies have suggested that NR2B-containing NMDARs that are largely extrasynaptic, are mechanosensitive, responding to stretch injury, and that activation of these receptors can initiate a cytotoxic response. 19 Additionally, in another study of in vitro cultured neurons exposed to high-intensity stretch injury, stretch increased activity via calcium-permeable AMPA (CP-AMPA) receptors, GluN2B NMDAR-mediated whole cell currents, and extrasynaptic GluN2B-containing NMDAR-mediated currents, but did not alter synaptic NMDAR-mediated currents. Administration of 10 μM memantine, which is a higher concentration than we used that blocked synaptic and extrasynaptic NMDARs, or treatment with Ro 25-6981, which blocked extrasynaptic NR2B-containing NMDARs only, immediately following injury reduced CP-AMPA receptor transmission. 37 Therefore, extrasynaptic NR2B-containing NMDARs may be preferentially overactivated by injury. 37 Further studies are necessary to determine the role of NR2B-containing NMDARs in mediating the brain's response to repetitive mTBI. However, our findings suggest that NR2B-containing NMDARs may be activated by repetitive stretch leading to injury and that memantine, and potentially other therapeutics that target extrasynaptic NMDARs, may be effective therapeutics for treating injury from repetitive mTBI.
In our study, 1.5 μM memantine delivered 1 h following each of two mild stretch injuries was effective. We chose this concentration because previous preclinical studies suggested that 1–10 μM was effective at mitigating TBI or injuries secondary to TBI such as hypoxia, ischemia, or excitotoxic injury, with minimal off-target effects in vitro. 18 In a previous study, we found that 1 μM memantine administered immediately post-stretch was the lowest concentration that significantly reduced cell death. 20 An in vivo study reported that injection of 20 mg/kg of memantine intraperitoneally 5 min post-injury, which within 30–60 min of injection resulted in 0.8–1.2 μM memantine in the CSF, significantly reduced cell death after TBI. 21 Additionally, in vivo studies suggest that the free concentration of memantine in the brain after 30–60 min following a clinically relevant dose was 0.5–10 μM, which is also the approximate CSF concentration in Parkinson's disease patients receiving chronic memantine treatment. 18,38 Another study reported that CSF concentration in dementia patients chronically treated with memantine was 1 μM, and 1 μM memantine rescued LTP loss in rodent-derived hippocampal slices from overactivation of NMDARs. 36 In vitro studies suggest that memantine >11 μM may inhibit LTP. 18 Therefore, we chose to evaluate 1.5 μM because it may be a low, yet effective, dose that is relevant for evaluating the benefit of clinically tolerable concentrations of memantine.
Each stretch injury was ∼12.9% strain and 5.3 sec−1 strain rate. Based on the cell death and functional tolerance criteria that our laboratory has defined for OHSCs and this stretch injury model, a single mild stretch of this severity should result in no overt cell death or change in basal evoked function (i.e., no change in S-R parameters or PPRs), and preliminary work in our laboratory has confirmed these results. 25,26,28,39 Previous pre-clinical studies suggest that a single mild closed head injury results in minimal pathology but may initiate a window of heightened tissue vulnerability during which additional injury can have a significant negative effect on brain samples. 40 These studies suggest that this window of heightened vulnerability may last from 24 h to ≥15 days following an initial mild injury. 9,26,41 –43 In our previous work, we reported that heightened vulnerability of OHSCs to repetitive mild stretch injury lasted as long as 72 h, but was over by 144 h following the initial injury, depending on the outcome measure used to assess injury; therefore, we chose a 24 h inter-injury interval in this study. 26
For most injuries, there can be a delay between onset of the injury and administration of a therapeutic drug, necessitated by transportation to a clinical facility and evaluation by a clinical professional before a therapy can be administered. Therefore, ideal drugs that are practical for clinical use are effective at delayed administration time points. Memantine was delivered 1 h following the first injury and allowed to incubate with the samples for 23 h prior to the second injury, and memantine was delivered again 1 h following the second injury. Memantine has been neuroprotective at delayed administration time points. In an in vitro study, 12 μM memantine prevented cell death in neonatal rat retinal ganglion cells even when administered up to 4 h following excitotoxicity exposure. 44 In a study previously performed by our laboratory, we reported that a combination of 100 pM 17β estradiol (E2) and 10 μM memantine was effective when administered 1 h following injury, but was no longer effective when administered 2 h following injury. 20 Therefore, we evaluated the effect of delayed administration 1 h following stretch injury. Administration of memantine following the first injury may be considered prophylactic treatment for the second injury. Prophylactic administration of a therapeutic drug for the first injury is not realistic given the potentially random occurrence of injury and may lead to overmedication of patients. However, for athletes who are at higher risk for brain injuries, administration of memantine prior to play could be beneficial as a prophylactic treatment to prevent significant pathology that could result from additional future brain injury. In humans, the half-life of memantine is 60–80 h; therefore, memantine administered once following an initial mTBI may remain active in the body for >3 days, potentially protecting the injured athlete from additional brain injury during this period. 45 However, further pre-clinical and clinical testing may be necessary for memantine to be approved by the FDA for this indication and to identify therapeutic windows appropriate for concussion.
It is difficult to draw conclusions about clinical efficacy from in vitro results alone. The injured athlete may experience varying injury severities, number of injuries, and intervals between exposures. The time course for pathology development in vitro may be more rapid than that for the human. Further pre-clinical and clinical translational studies are necessary before we can determine the potential for memantine to improve outcomes for the injured athlete, and determine dosing and an ideal therapeutic window for humans. We were not able to evaluate the potential effect of the vasculature, the blood–brain barrier, or a systemic response on injury outcomes with or without memantine. Additionally, further studies are necessary to validate the biochemical mechanism whereby memantine rescues LTP, reduces cell death, and improves pathology from repetitive mTBI
The biomechanics of this injury were chosen specifically to represent the intracranial deformation of brain experienced during real-world mTBI. 26 The current standard of care for mTBI is rest from work and activity while symptoms recover. As such, any therapeutic drug that can target the pathology, prevent symptoms, and allow the patient to maintain quality of life would be an improvement on the current standard of care. The socioeconomic cost associated with mTBI in the United States is estimated to be nearly $17 billion annually. 2 Given the high incidence of mTBI, the increased likelihood of additional injury for patients who have sustained an mTBI, and the potential for repetitive mTBI to lead to more significant cognitive deficits and neurodegenerative disease, there is a need for therapeutic drugs that can treat and prevent injury from multiple mTBIs to improve quality of life for these patients and reduce the economic burden associated with the short- and long-term care of patients with mTBI. Based on the results of this study and the well-studied mechanism of action and defined toxicology of memantine, memantine may warrant further investigation in translational studies to determine its potential for improving outcomes of mTBI.
Footnotes
Acknowledgments
The authors acknowledge the technical assistance of Elise Gill, Kimberly A. Lynch, and Shruthi Nammalwar. This research was funded in part by Grant 1 R49 CE002096 from the National Center for Injury Prevention and Control of the Centers for Disease Control and Prevention to the Center for Injury Epidemiology and Prevention at Columbia University Medical Center, and a multi-disciplinary university research initiative from the Army Research Office (W911NF-10-1-05026). The contents of this manuscript are the sole responsibility of the authors and do not necessarily reflect the official views of the funding agencies.
Author Disclosure Statement
No competing financial interests exist.