
Abstract
Traumatic brain injury (TBI) contributes to the increased rates of suicide and post-traumatic stress disorder in military personnel and veterans, and it is also associated with the risk for neurodegenerative and psychiatric disorders. A cross-phenotype high-resolution polygenic risk score (PRS) analysis of persistent post-concussive symptoms (PCS) was conducted in 845 U.S. Army soldiers who sustained TBI during their deployment. We used a prospective longitudinal survey of three brigade combat teams to assess deployment-acquired TBI and persistent physical, cognitive, and emotional PCS. PRS was derived from summary statistics of large genome-wide association studies of Alzheimer's disease, Parkinson's disease, schizophrenia, bipolar disorder, and major depressive disorder (MDD); and for years of schooling, college completion, childhood intelligence, infant head circumference (IHC), and adult intracranial volume. Although our study had more than 95% of statistical power to detect moderate-to-large effect sizes, no association was observed with neurodegenerative and psychiatric disorders, suggesting that persistent PCS does not share genetic components with these traits to a moderate-to-large degree. We observed a significant finding: subjects with high IHC PRS recovered better from cognitive/emotional persistent PCS than the other individuals (R2 = 1.11%; p = 3.37 × 10−3). Enrichment analysis identified two significant Gene Ontology (GO) terms related to this result: GO:0050839∼Cell adhesion molecule binding (p = 8.9 × 10−6) and GO:0050905∼Neuromuscular process (p = 9.8 × 10−5). In summary, our study indicated that the genetic predisposition to persistent PCS after TBI does not have substantial overlap with neurodegenerative and psychiatric diseases, but mechanisms related to early brain growth may be involved.
Introduction
T
Molecular investigations have shown that biochemical changes induced by concussive trauma can lead to ionic disturbance, excitatory amino acid neurotoxicity, initial mitochondrial dysfunction, reactive oxygen species-mediated damage, energy metabolism depression, altered gene expression, and ultimately, neuronal dysfunction. 12 Most individuals recover from these TBI-induced molecular changes after a short time, but some vulnerable subjects develop persistent neurological and psychological symptoms that can culminate in neurodegenerative and psychiatric disorders. A likely scenario is that this vulnerability to long-term consequences of TBI is linked to individual genetic susceptibility: TBI might interact with genetic predisposition to neurodegenerative and psychiatric disorders in determining persistent neurological and psychological PCS. Although this hypothesis requires a high shared heritability between persistent PCS and neurodegenerative or psychiatric diseases, very few genetic studies have been conducted on persistent PCS. Those that have been completed investigated the APOE e4 allele and serotonin receptor alleles, with inconsistent results. 13 –15 Genome-wide investigations have demonstrated that the genetic predisposition to complex traits is highly polygenic (i.e., many variants with small effects). 16 Risk alleles identified by genome-wide association studies (GWAS) can be investigated in cross-phenotype investigations. 17 High-resolution polygenic risk scores (PRS) derived from large GWAS were able to predict the same trait in independent cohorts, and additionally, other phenotypes with shared genetic vulnerability. 18 –21 Accordingly, if the hypothesis of shared genetic vulnerability is correct, PRS derived from neurological and psychiatric GWAS may be able to predict persistent PCS in subjects who sustained TBI.
In the present study, genetic and epidemiological data from the Army STARRS Initiative were used to investigate the role of genetic vulnerability to persistent PCS in U.S. Army soldiers with deployment-acquired TBI. Specifically, we conducted a high-resolution cross-phenotype PRS analysis to investigate the shared genetic components between persistent PCS and multiple traits including neurodegenerative diseases, psychiatry disorders, and other brain-related phenotypes. To our knowledge, this is the first genome-wide investigation of persistent PCS. Our results provide novel insights regarding mechanisms related to their pathophysiology that can guide future molecular investigations.
Methods
Army STARRS cohort
The subjects investigated were selected from U.S. Army soldiers who participated in the Army STARRS Initiative. All participants gave written informed consent to participate. These procedures were approved by the Human Subjects Committees of all collaborating organizations. We considered U.S. soldiers from three brigade combat teams deployed in Afghanistan during the first quarter of 2012. These subjects were assessed through the Pre/Post Deployment Survey (PPDS) that is a multi-wave panel survey based on self-administered questionnaires (SAQs) that collected prospective data at four time points: T0 (within approximately 6 weeks of their deployment), T1 (within one month of their return), T2 (approximately 3 months from their return), and T3 (approximately 9 months from their return). The T0 SAQ was an extensive survey focused on socio-demographic characteristics, lifetime and past-30-day mental disorders, and other potential risk and resilience factors. The T1 follow-up SAQ included an assessment of deployment experiences including deployment stressors and TBI. The T2 and T3 SAQs included questions about PCS. In the present investigation, we included 845 subjects with European ancestry that met criteria for mild-to-moderate TBI at the T1 follow-up SAQ. Further details regarding the Army STARRS initiative, U.S. Army cohorts, PPDS, and deployment-acquired TBI criteria are available in previous publications. 4,22
Post-concussive symptom measures
Consistent with the National Institute of Mental Health's Research Domain Criteria (RDoC) initiative, 23 we conducted our PRS analysis considering dimensional measures of PCS derived from symptom scales based on self-reported information. Further details concerning the methods for PCS severity calculation and categorization are available in our previous publication. 4
Longitudinal analysis of persistent PCS was conducted at the T2 and T3 follow-up assessments. Both T2 and T3 SAQs included eight items that reflect the array of PCS: 1) balance problems or dizziness; 2) sensitivity to noise; 3) sensitivity to light; 4) memory problems; 5) headaches; 6) difficulty concentrating; 7) irritability; and 8) feeling tired out or being easily fatigued. Respondents rated each symptom on a 5-point frequency scale that ranged from “None of the time (0)” through “All or almost all of the time (4).” Further details regarding PCS assessments are available in our previous publication. 4 Summing these ratings yielded a global PCS score (PCS-8) ranging from 0 to 32. Because persistent PCS affect multiple neurobehavioral domains (i.e., vestibular, somatic/sensory, cognitive, and emotional), 2 we also calculated two alternative PCS measures: a “physical” PCS score and a “cognitive/emotional” PCS score. The physical PCS score (PCS-5; range = 0–20) included vestibular and somatic/sensory PCS items: balance problems or dizziness, sensitivity to noise, sensitivity to light, memory problems, and headaches. The cognitive/emotional PCS score (PCS-3; range = 0–12) included cognitive and emotional PCS items: irritability, difficulty concentrating, and feeling tired or easily fatigued. For all PCS scores (i.e., PCS-8, PCS-5, and PCS-3), we considered the highest PCS score at either T2 or T3 (PCS Max) to reflect persistent PCS and the PCS change between T3 and T2 (PCS Δ) to evaluate the course of persistent PCS after the deployment-acquired TBI.
GWAS summary statistics
We derived PRS from previous large GWAS conducted on multiple brain-related phenotypic traits: Alzheimer's disease, Parkinson's disease, schizophrenia, bipolar disorder, major depressive disorder (MDD), years of schooling, college completion, childhood intelligence, infant head circumference (IHC), and adult intracranial volume. For Alzheimer's disease, we used stage 1 summary statistics from the GWAS conducted by the International Genomics of Alzheimer's Project on 17,008 Alzheimer's disease case patients and 37,154 controls. 24 For Parkinson's disease, we used summary statistics from the GWAS conducted on 13,708 case patients and 95,282 controls available at the PDGene database. 25,26 Parkinson's disease PRS analysis was conducted considering only two association p-value thresholds (p-value = 0.001, 0.05) for SNP (single nucleotide polymorphism) inclusion because the GWAS summary statistics included only detailed information regarding the top 10,000 variants. For psychiatric disorders (schizophrenia, bipolar disorder, and MDD), we used summary statistics from GWAS conducted by the Psychiatric Genomics Consortium. 27 –29 For years of schooling and college completion, we used summary statistics from GWAS performed by the Social Science Genetic Association Consortium. 30 For childhood intelligence, we used summary statistics from the GWAS performed by the Childhood Intelligence Consortium. 31 For IHC, we used summary statistics from the GWAS conducted by the Early Growth Genetics Consortium. 32 For adult intracranial volume, we used summary statistics from the GWAS conducted by the Enhancing Neuro Imaging Genetics through Meta-Analysis Consortium. 33
Statistical analysis
We conducted cross-phenotype PRS analyses using PRSice software. 34 PPDS subjects were genotyped using the Illumina OmniExpress + Exome array with additional custom content (967,000 genetic markers). After pre-imputation quality control, a total of 664,457 SNPs entered the subsequent analysis. The genotype imputation was conducted using SHAPEIT 35 for pre-phasing, IMPUTE2 36 for imputation, and 1000 Genomes Project Phase 1 37 as the reference panel. Further details regarding genotyping and imputation procedures are available in our previous publication. 38
We used imputed genotypes to maximize a consistent SNP panel between the training and testing sets and performed linkage disequilibrium (LD) clumping by excluding SNPs that had R2 ≥0.3 with another SNP with a lower association p-value in a 500 kb window. We used four association p-value thresholds (p-value = 0.001, 0.05, 0.3, 0.5) for SNP inclusion in the high-resolution PRS except as noted above. Because the GWAS used were conducted on subjects with European ancestry, we restricted our analysis to Army STARRS participants with European ancestry. To confirm subjects’ ancestry, we performed a principal component (PC) analysis combining the Army STARRS samples with the HapMap3 39 reference subjects. Then, a PC analysis was conducted within each ancestry group using only the study samples to obtain the top 10 PCs for population stratification adjustment. Further details regarding the methods of PC analysis are available in our previous publication. 38
We used summary statistics from the large GWAS selected as the training dataset and fitted in regression models with adjustments for age, sex, and the top 10 PCs to calculate Nagelkerke's R2 as the figure of merit for prediction ability. Before being entered in the regression model, PCS score (Max and Δ) were normalized using appropriate Box-Cox power transformations. Because we performed multiple tests, we considered a PRS-wise significant threshold (p < 0.005; Bonferroni correction for the 10 PRS) in accordance with what was recently proposed for phenome analysis of previously identified alleles.
40
To estimate the statistical power of the PRS analysis conducted in our sample, we performed a power analysis in R (
Finally, we conducted an enrichment analysis for the significant PRS, analyzing the association of the SNPs included in the PRS with the PCS phenotype. SNPs with nominal concordant direction with PRS-PCS association were mapped to the corresponding genes using DEPICT v1 41 and then the loci were entered in Gene Ontology (GO) enrichment analysis conducted using DAVID v6.7. 42
Results
Table 1 reports the characteristics of the study population investigated in the cross-phenotype PRS analysis. The sample is mainly constituted by young male subjects (50% <24 years of age and 80% male). All participants reported experiencing a deployment-acquired TBI during the index deployment; 94% of them met our criteria for mild TBI. Forty-nine percent of them reported no pre-deployment TBI. Maximum PCS scores (PCS-8 Max, PCS-5 Max, and PCS-3 Max) indicated that the sample investigated included both subjects with persistent PCS and subjects with no PCS after TBI. The prospective analysis of PCS (i.e., PCS Δ values) indicated that more than 50% of the subjects improved their PCS status in T3 follow-up assessment compared with T2, considering both global, physical, and cognitive/emotional PCS scores (PCS-8 Δ, PCS-5 Δ, and PCS-3 Δ, respectively).
PCS, post-concussive symptoms; TBI, traumatic brain injury.
We conducted a power analysis to evaluate the likelihood to detect different effect sizes in the sample investigated (Fig. 1). With 845 subjects, we had more than 95% statistical power to detect moderate-to-large effects (R2 >5%). For a small effect size (R2 = 1%), we had 41% statistical power to detect a small effect at nominal significance (p = 0.05) and 14% at a PRS-wise significance (p = 0.005).
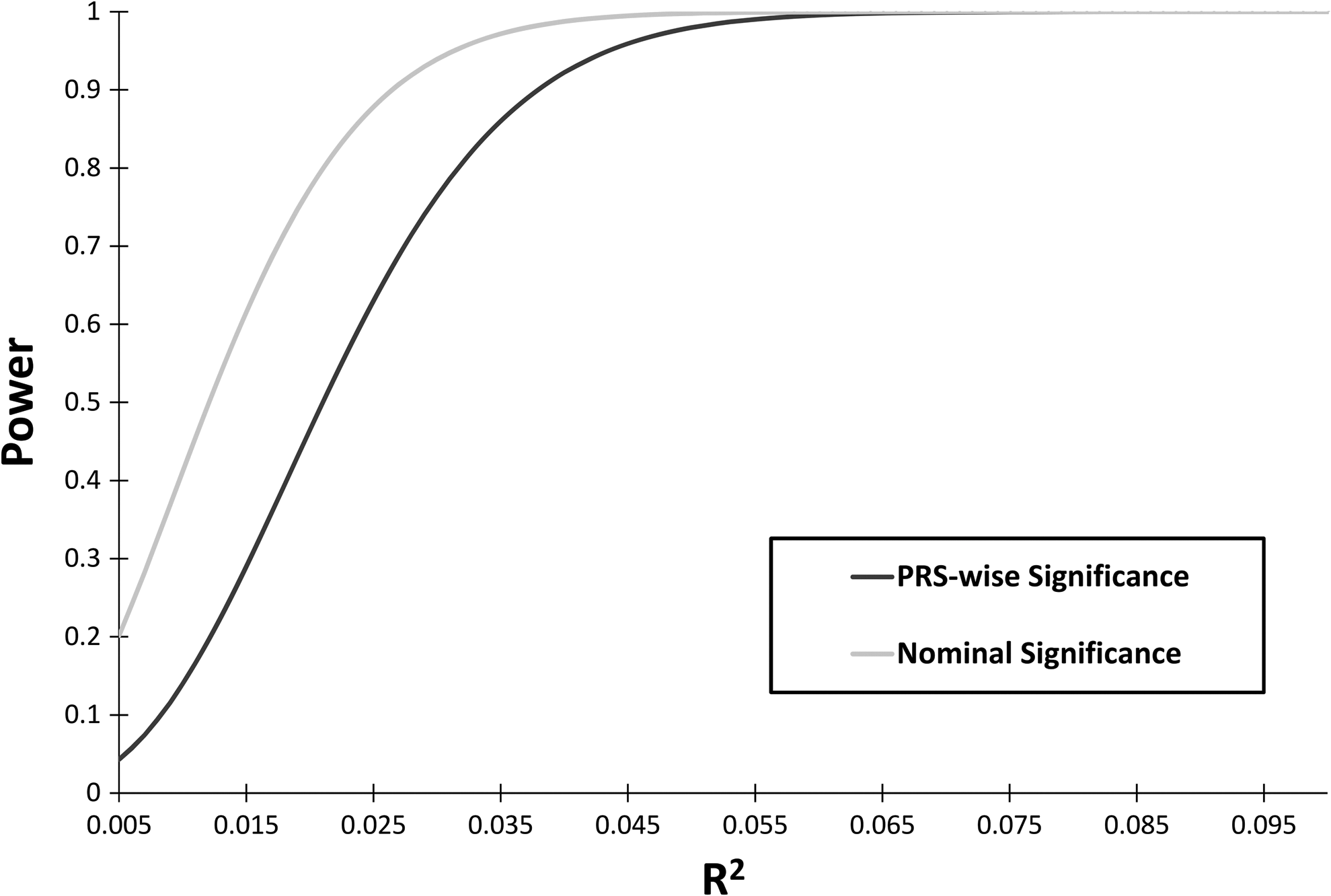
Statistical power to detect significant effects considering PRS-wise and nominal thresholds. PRS, polygenic risk score.
The cross-phenotype PRS analysis performed considering 10 PRS and 6 PCS phenotypes did not identify any significant moderate-to-large effect. Full results are available in the Supplementary Table 1 (see online supplementary material at
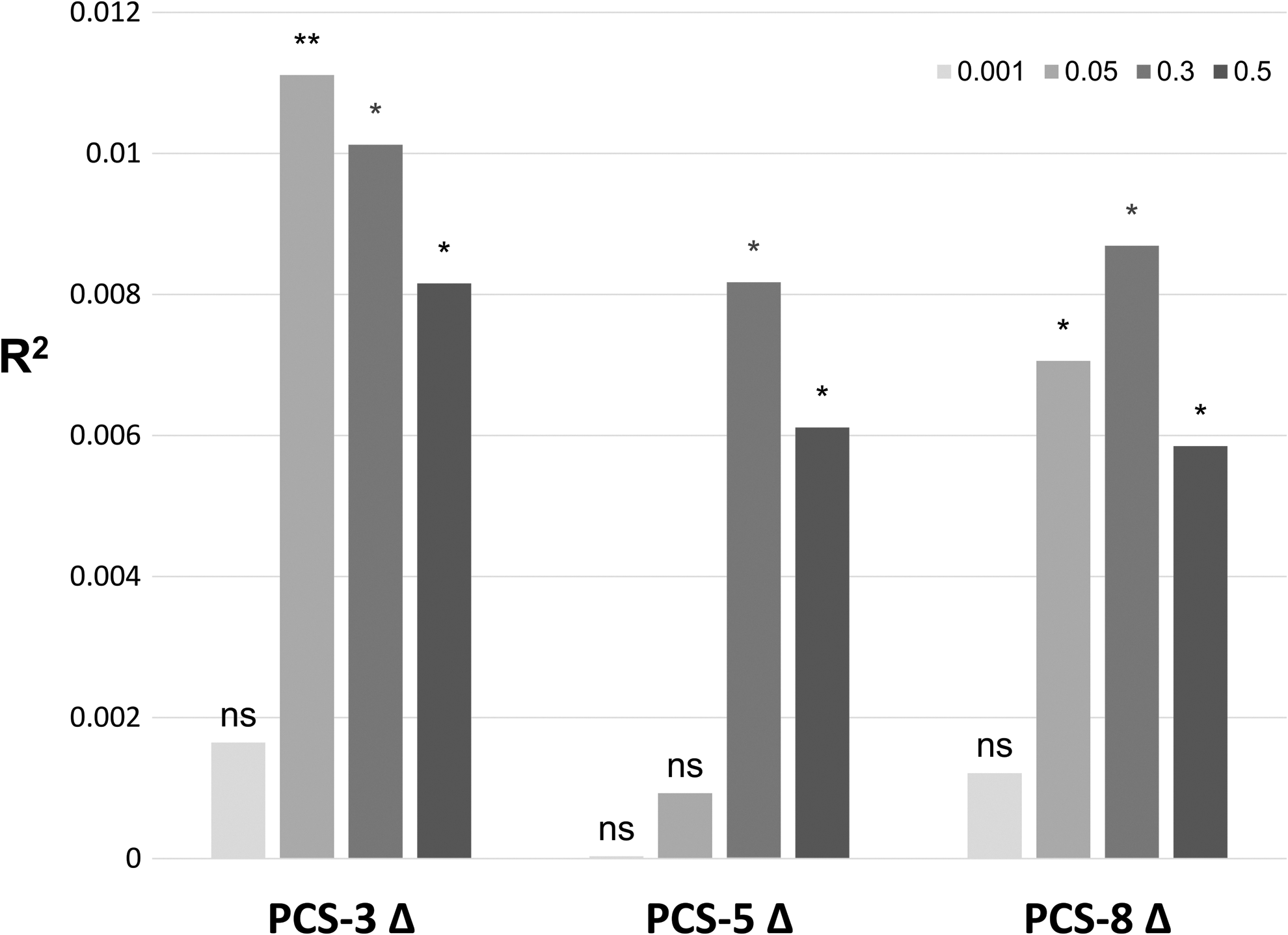
Results at broad p-value thresholds for infant head circumference PRS predicting the courses of total, physical, and cognitive/emotional PCS Δ (PCS-8 Δ, PCS-5 Δ, and PCS-3 Δ, respectively). NS (not significant; p > 0.05); *nominal significance (p < 0.05); **PRS-wise significance (p < 0.005). PCS, post-concussive symptoms; PRS, polygenic risk score.
Finally, we performed a GO enrichment analysis based on SNPs included in the IHC PRS (p = 0.05) that have nominal association with PCS-3 Δ with a direction concordant with IHC PRS-PCS-3 Δ association (Table 2). In the tested SNP set, two GO terms were significantly enriched after Bonferroni multiple-testing correction: Cell adhesion molecule binding (GO:0050839; p = 8.9 × 10−6) and Neuromuscular process (GO:0050905; p = 9.8 × 10−5).
Fisher's exact test p-values are reported.
Discussion
To our knowledge, this is the first genome-wide investigation of persistent PCS. Because large sample sizes are required to conduct powerful complex trait GWAS, we conducted this genome-wide evaluation by means of a high-resolution cross-phenotype PRS analysis to detect shared genetic components between persistent PCS and multiple brain-related phenotypes. This strategy, although it lacks the ability to identify novel risk variants in a hypothesis-free way, is supported by epidemiological evidence that links TBI and persistent PCS to neurodegenerative and psychiatric diseases. 11 Indeed, the genetic predisposition to neurodegenerative and psychiatric diseases may identify those subjects who are vulnerable to develop persistent PCS after TBI. Under this hypothesis, we expected to detect consistent effects of GWAS-derived PRS on persistent PCS and its recovery course.
We investigated 845 U.S. soldiers who sustained TBI during their deployment; power analysis demonstrated that we had >95% of statistical power to detect moderate-to-large effects in the PRS analysis. However, we did not observe any moderate-to-large effect of the PRS investigated on persistent global, physical, or cognitive/emotional PCS score (Max and Δ) that survived PRS-wise correction. This outcome was unexpected. Persistent emotional PCS (i.e., irritability, difficulty concentrating, and feeling tired or easily fatigued) includes symptoms commonly associated with depressive disorders and therefore a genetic overlap was anticipated with MDD and a significant result was predicted between PCS-3 and MDD PRS. Because, as stated, our study design had >95% statistical power to detect moderate-to-large effects, the negative result observed indicates that the genetic vulnerability of subjects who sustained TBI to develop persistent PCS (and possibly to have an increased risk for neurodegenerative and psychiatric disorders as TBI consequence) may not overlap with the genetics of neurodegenerative and psychiatric disorders in the general population. This provided novel information regarding the pathogenesis of TBI consequences, and on the basis of this information, we surmise that molecular mechanisms independent from those highlighted by GWAS of neuropsychiatric traits are mainly responsible for persistent PCS and other TBI consequences.
Recent studies hypothesized that TBI may affect neuronal morphology and synaptic connectivity through transcriptomic and epigenetic changes activating pathogenic pathways responsible for the manifestation of persistent neurological dysfunction.
43,44
Consistent with this possible scenario, the only significant finding (with small effect) observed was between IHC PRS and PCS-3 Δ (i.e., variation of persistent cognitive/emotional PCS after TBI): individuals with high IHC PRS had better recovery than subjects with low IHC PRS. Nominally significant associations were also observed between IHC PRS and PCS-5 Δ and PCS-8 Δ. Thus, mechanisms involved in early brain growth (such as regulatory functions relevant to neuronal morphology and synaptic connectivity)
45
could be involved in the resilience to TBI consequences rather than the pathogenic pathways we tested. Indeed, although there is some suggestive local genetic overlap between IHC and neuropsychiatric diseases,
32
Bonferroni-significant global genetic overlap has been observed between IHC and other development-related phenotypes (i.e., birth length and weight).
46
Positive nominally significant genetic correlations of IHC have been observed for years of schooling, college completion, and childhood intelligence (data available at
Our GO enrichment analysis of the IHC PRS-PCS-3 Δ association provided further data regarding the molecular pathways potentially shared by persistent PCS and IHC. As expected for brain-related phenotypes, we observed a significant GO term related to the functions of the nervous and muscular systems (GO:0050905∼Neuromuscular process). The second significant GO term provided more details about the potential mechanisms: GO:0050839∼Cell adhesion molecule binding. Indeed, adhesive extracellular matrix constituent, cell adhesion molecule activity, and cell adhesion receptor activity are all functions that may play an important role in determining the vulnerability/resilience to TBI consequences. 48 GO:0050839∼Cell adhesion molecule binding also suggests associations related to neuroinflammation and immune and neuroendocrine systems because they are all strictly linked in the injury and repair processes related to TBI. 49,50
In summary, we applied an advanced genome-wide approach to longitudinal prospective data from the Army STARRS Initiative to investigate the molecular processes related to persistent PCS after deployment-acquired TBI. Our results indicated that the neurodegenerative and psychiatric diseases do not share large genetic components with persistent physical, cognitive, and emotional PCS. Because our sample was powered to detect moderate-to-large effects, we cannot exclude small-scale genetic overlap. Nevertheless, we identified a significant association for IHC PRS. This could indicate that genetic mechanisms related to early brain growth play a more relevant role in TBI consequences than genetic susceptibility to neuropsychiatric disorders. In particular, in the context of TBI, the enrichment for cell adhesion molecule activity suggests other closely related molecular processes, including neuroinflammation and neuroendocrine–immune functions, as components of the genetics of persistent PCS. Additional large-scale genome-wide investigations are needed to dissect the genetic architecture of persistent PCS. Increased knowledge regarding genetics of TBI consequences can provide a basis to develop effective preventive treatments, especially for high-risk categories such as military personnel.
Footnotes
Acknowledgments
The Army STARRS Team consists of Co-Principal Investigators: Robert J. Ursano, MD (Uniformed Services University of the Health Sciences) and Murray B. Stein, MD, MPH (University of California, San Diego and VA San Diego Healthcare System); Site Principal Investigators: Steven Heeringa, PhD (University of Michigan) and Ronald C. Kessler, PhD (Harvard Medical School); National Institute of Mental Health (NIMH) Collaborating Scientists: Lisa J. Colpe, PhD, MPH and Michael Schoenbaum, PhD; Army Liaisons/Consultants: Col. Steven Cersovsky, MD, MPH (USAPHC) and Kenneth Cox, MD, MPH (USAPHC); Other Team Members: Pablo A. Aliaga, MA (Uniformed Services University of the Health Sciences); Col. David M. Benedek, MD (Uniformed Services University of the Health Sciences); K. Nikki Benevides, MA (Uniformed Services University of the Health Sciences); Paul D. Bliese, PhD (University of South Carolina); Susan Borja, PhD (NIMH); Evelyn J. Bromet, PhD (Stony Brook University School of Medicine); Gregory G. Brown, PhD (University of California, San Diego); Laura Campbell-Sills, PhD (University of California, San Diego); Catherine L. Dempsey, PhD, MPH (Uniformed Services University of the Health Sciences); Carol S. Fullerton, PhD (Uniformed Services University of the Health Sciences); Nancy Gebler, MA (University of Michigan); Robert K. Gifford, PhD (Uniformed Services University of the Health Sciences); Stephen E. Gilman, ScD (Harvard School of Public Health); Marjan G. Holloway, PhD (Uniformed Services University of the Health Sciences); Paul E. Hurwitz, MPH (Uniformed Services University of the Health Sciences); Sonia Jain, PhD (University of California, San Diego); Tzu-Cheg Kao, PhD (Uniformed Services University of the Health Sciences); Karestan C. Koenen, PhD (Columbia University); Lisa Lewandowski-Romps, PhD (University of Michigan); Holly Herberman Mash, PhD (Uniformed Services University of the Health Sciences); James E. McCarroll, PhD, MPH (Uniformed Services University of the Health Sciences); James A. Naifeh, PhD (Uniformed Services University of the Health Sciences); Tsz Hin Hinz Ng, MPH (Uniformed Services University of the Health Sciences); Matthew K. Nock, PhD (Harvard University); Rema Raman, PhD (University of California, San Diego); Holly J. Ramsawh, PhD (Uniformed Services University of the Health Sciences); Anthony Joseph Rosellini, PhD (Harvard Medical School); Nancy A. Sampson, BA (Harvard Medical School); LCDR Patcho Santiago, MD, MPH (Uniformed Services University of the Health Sciences); Michaelle Scanlon, MBA (NIMH); Jordan W. Smoller, MD, ScD (Harvard Medical School); Amy Street, PhD (Boston University School of Medicine); Michael L. Thomas, PhD (University of California, San Diego); Leming Wang, MS (Uniformed Services University of the Health Sciences); Christina L. Wassel, PhD (University of Pittsburgh); Simon Wessely, FMedSci (King's College London); Christina L. Wryter, BA (Uniformed Services University of the Health Sciences); Hongyan Wu, MPH (Uniformed Services University of the Health Sciences); Ltc. Gary H. Wynn, MD (Uniformed Services University of the Health Sciences); and Alan M. Zaslavsky, PhD (Harvard Medical School). Kerry Ressler MD, PhD (Emory University) chaired the Scientific Advisory Board.
We thank the GWAS consortia IGAP (International Genomics of Alzheimer's Project), PDGene, PGC (Psychiatric Genomics Consortium), SSGAC (Social Science Genetic Association Consortium), CHIC (Childhood Intelligence Consortium), EGG (Early Growth Genetics), and ENIGMA (Enhancing Neuro Imaging Genetics through Meta-Analysis) and their funding agencies for providing summary results data for these analyses. The investigators who contributed to the design and implementation of these previous GWAS did not participate in analysis or writing of this report. IGAP and its participants were supported by the French National Foundation on Alzheimer's Disease and Related Disorders, LABEX (Laboratory Of Excellence Program Investment for the Future) DISTALZ grant, Medical Research Council (Grant no. 503480), Alzheimer's Research UK (Grant no. 503176), Wellcome Trust (Grant no. 082604/2/07/Z), German Federal Ministry of Education and Research (BMBF) Competence Network Dementia (CND) (Grant no. 01GI0102, 01GI0711, 01GI0420), NIH/NIA Grants (R01 AG033193, AG081220, U01 AG032984, U24 AG021886, U01 AG016976) and AGES contract N01–AG–12100, NHLBI Grant R01 HL105756, Icelandic Heart Association, Erasmus Medical Center and Erasmus University, and Alzheimer's Association Grant ADGC–10–196728.
Army STARRS was sponsored by the Department of the Army and funded under cooperative agreement number U01MH087981 with the U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Mental Health (NIH/NIMH). Additional support was provided by the grant R21 AA024404 from the National Institutes of Health, National Institute of Alcoholism and Alcohol Abuse (NIH/NIAAA). The contents are solely the responsibility of the authors and do not necessarily represent the views of the Department of Health and Human Services, NIMH, Veterans Administration, Department of the Army, or Department of Defense.
Author Disclosure Statement
Dr. Stein has in the last 3 years been a consultant for Healthcare Management Technologies, Janssen, Pfizer, Resilience Therapeutics, and Oxeia Biopharmaceuticals. In the past 3 years, Dr. Kessler has been a consultant for Hoffman-La Roche, Inc., Johnson & Johnson Wellness and Prevention, and Sonofi-Aventis Groupe. Dr. Kessler has served on advisory boards for Mensante Corporation, Plus One Health Management, Lake Nona Institute, and U.S. Preventive Medicine. Dr. Kessler owns a 25% share in DataStat, Inc. The remaining authors report they have nothing to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.