
Abstract
The aim of this study was to review the literature about the effects of activity-based therapy (ABT) interventions on mobility, functional independence, and quality of life for people with a spinal cord injury (SCI). A systematic review with meta-analysis of randomized and non-randomized trials was performed, including adults with a non-progressive SCI at any level. The intervention of interest was ABT, defined as any intervention that sought to improve muscle activation or sensory function below the level of injury in the spinal cord and does not rely on compensatory mechanisms for improving function. The comparison was either no intervention or conventional physical interventions targeted to regions above the level of injury. The outcome measures were quality-of-life questionnaires, mobility assessments, and functional independence scales. Nineteen trials were included in this systematic review. Three compared ABT to no intervention and 16 to conventional physical rehabilitation. The methodological quality of the trials was assessed using the PEDro scale as moderate. Six studies investigated the effects of ABT interventions for the upper limbs, 11 investigated gait-related interventions, and two applied multi-modal interventions. Compared with no intervention, the meta-analysis found that ABT was not more effective for improving independence or lower limb mobility, but conferred a large positive effect on upper limb function. Compared with conventional physical interventions, there was no significant effect of ABT on lower limb mobility, independence, or quality of life; however, it had positive effects on upper limbs. In conclusion, there is evidence that ABT can improve independence and functional ability when applied to the upper limbs in people with SCI. However, it is not superior to conventional physical interventions when applied to the lower limbs.
Introduction
E
Animal studies have demonstrated that a high degree of functional recovery can be achieved after SCI. 4 The degree of motor recovery is defined largely by the type and intensity of motor training and sensory stimulation following the injury. 5,6 Training and exercise have profound effects on cellular and molecular function involved in spinal plasticity. It appears that the spinal cord in animals has the ability to change through the repeated activation of sensory circuits. 7,8 This plasticity can be due to the activation of the circuitry contained within the spinal cord that is responsible for the organization of complex movements, using central pattern generators and reflexes local to the spinal cord. 9,10
In humans, some late neural recovery can occur after the acute phase of injury 11 ; however, the magnitude of recovery is small and diminishes over time, leading to residual disability. Hence, physical interventions, such as exercises and physical therapy, play an important role in enhancing performance and functional outcomes, promoting independence.
There is evidence that in a similar way to animals, the human nervous system is responsive to input and can adapt even after injury. 10,11 The training experience afforded to the nervous system is critical to promote recovery. 12 Intense activity in the form of repeated active movements, often combined with augmented sensory stimulation, may lead to neural or functional improvements, or both, in humans at any level of injury or any degree of completeness. 13,14 This is the basis of activity-based therapy (ABT) interventions.
By definition, ABT is “a group of multimodal interventions that seek to minimize compensatory mechanism of functional recovery and provide activation of the neuromuscular system below the level of injury with the goal of retraining the nervous system in order to facilitate the recovery of a specific motor task.” 15 The majority of ABT interventions are focused on the recovery of motor and sensory function in the lower limbs with the aim of walking; therefore, locomotor training strategies have been the main focus of research to date. It has been demonstrated that recovery of walking and balance function can occur after injury. 16 –18 However, the quality of the studies is questionable. A Cochrane systematic review conducted in 2012 included only five randomized controlled trials involving 309 participants across all trials. Their findings were inconclusive, with no significant superior effect of any locomotor training approach on walking function after SCI, compared with any other kind of physical rehabilitation. 19
Fewer studies have investigated the application of ABT to improve the ability to reach and manipulate objects. Massed practice and functional electrical stimulation have been the most investigated ABT interventions for upper limbs. 20,21 Backus and colleagues 14 conducted a systematic review to investigate the efficacy of ABT interventions for improving neural activity and function in adults and children with SCI. They included 21 experimental, quasi-experimental, and descriptive trials. Only three of them targeted upper limb interventions. Their review supports the use of ABT interventions to improve function in incomplete SCI. However, only trials published between 1998 and 2008 were included.
Despite having the goal of improving functional recovery of areas below the level of injury, ABT interventions may help optimize the function above the injury due to the nature of the tasks performed. ABT interventions are highly repetitive and involve low load tasks, which can improve strength of innervated or partially innervated muscles. 21 –30 Moreover, exercises are performed in different body positions, out of the wheelchair, and usually associated with load bearing through the lower limbs, which can contribute to increased muscle strength, control, and greater physical capacity. Further, the high number of repetitions may lead to cortical plasticity and motor learning. 31 The combination of those factors may lead to improved general mobility and increased independence, promoting better quality of life.
Therefore, the aim of this systematic review was to examine the effectiveness of ABT interventions for improving general mobility, functional independence, and quality of life for people sustaining a SCI. This review included only randomized or controlled trials, including crossover clinical studies. The review was registered at PROSPERO (CRD42015017917).
Methods
Literature search
Searches were conducted on MEDLINE, CINAHL, EMBASE, AMED, SCOPUS, SPORTDiscuss, Web of Science, Cochrane Library, and PEDro databases for relevant studies without date or language restrictions. The search was run from the earliest record to February 2016 in each of the databases. Search terms included words and phrases related to spinal cord injuries or quadriplegia or tetraplegia and mobility, or activities of daily living or recovery of function, and words related to activity-based interventions (such as exercise, exercise therapy, and physical training). See Appendix 1 for the full search strategy.
Selection of trials
Articles titles and abstracts were screened by two reviewers (CQDO and GMD) to identify relevant studies. Full article copies of peer-reviewed relevant articles were retrieved and their reference lists screened to identify further studies of relevance. Conference proceedings and dissertations were not included in this review. The methodology of the retrieved articles was extracted and reviewed independently by two reviewers using predetermined criteria (Table 1). Results for each citation were also extracted by two reviewers (CQDO and LDJ). Disagreement or ambiguities were resolved by consensus after discussion with a third reviewer (GMD).
At the end of the screening process, all abstracts that had originally been considered for exclusion had their full text of the publication assessed in order to avoid inappropriate exclusion as there might be incomplete information about the research protocol in the abstract.
Assessment of characteristics of trials
Quality
The quality of included trials was assessed by extracting PEDro scores from the Physiotherapy Evidence Database. 32 The PEDro scale is an 11-item scale designed for rating the methodological quality (internal validity and statistical information) of randomized trials. Each item, except for item 1, contributes one point to the total PEDro score (range: 0 to 10 points), with greater scores representing higher quality. Conventionally, total scores lower than 3 are considered of low quality, total scores between 4 and 6 are considered of moderate quality, and total scores above 7 are considered high quality. 33 Trials that were not included in the PEDro database and those that were, were scored independently by two reviewers (CQDO and LDJ). Disagreement or ambiguities were resolved by consensus with a third independent reviewer (GMD).
Participants
Eligible studies included adults at any time after sustaining a traumatic spinal cord injury. Studies comprising traumatic and non-traumatic injuries were included if at least 50% or more of the sample comprised of traumatic injuries and if the etiology was non-progressive. Individuals with all levels of injury and American Spinal Injury Association Impairment Scale (AIS) classification 34 were included. The number of participants, age, gender, level of injury, AIS classification (grades A-D), and time since injury were recorded to assess the similarity of the studies.
Intervention
To be included, the experimental intervention was an activity-based therapy as defined by Backus and colleagues, 14 namely “any intervention that specifically uses tools and interventions to improve muscle activation or sensory function below the level of injury in the spinal cord, and does not rely on compensatory mechanisms for improving function after SCI. Such approach includes interventions that combine intensive active movement with one or more of the following: facilitation techniques (use of tactile or vibratory stimulation); electrical stimulation for muscles or nerves (surface or indwelling); body weight–supported locomotor training (manual or robotic); upper extremity robotics; massed practice training.” Interventions including the use of electrical stimulation or robotic devices (e.g., neuroprosthesis) or sensory stimulation in isolation from movement were not considered as ABT interventions. Since the phrase activity-based therapy is an umbrella term, the literature search was conducted using the keyword “exercise” and other related words. The reviewers (CQDO and GMD) judged if the intervention was activity-based therapy according the definition of Backus and colleagues. 14
The comparison condition could be no intervention at all or any conventional rehabilitation physical intervention targeted to regions above the level of injury and aiming to compensate for loss of function through muscle strengthening, task-specific training, training of activities of daily living, and aerobic exercise training. This approach relies substantially on providing compensatory strategies focused on the use of the preserved muscles above the level of injury, using leverage and momentum to move weak or paralyzed body parts and the use of orthotic devices to enhance function. Frequency, duration, and number of sessions were recorded in order to assess the similarity of the studies and to guide the development of “best practice” ABT in the context of this review.
Measures
There were three outcomes of interest: mobility, independence, and quality of life. Measures of general mobility that assessed the ability of an individual to perform transfers, change positions, balance, ambulate, reach, and manipulate objects were included, such as the Jebsen-Taylor Hand Function Test (JTHFT), 35 Berg Balance Scale (BBS), 36 and Walking Index for Spinal Cord Injuries (WISCI). 37 Discrete measure of walking ability, such as gait speed, distance, cadence, and step length, were outside the scope of this review. A Cochrane review conducted by Mehrholz and colleagues 19 already has investigated the effects of locomotor training, which is the main ABT intervention for lower extremities, on discrete gait parameters and walking capacity.
Level of independence was appraised using outcome measures that sought to assess how much assistance was required by the individual to carry out activities of daily living. Assessment tools included the Functional Independence Measure (FIM), 38 the Spinal Cord Independence Measure (SCIM), 39 and the Canadian Occupational Measure, 40 among others.
Studies that assessed quality of life via questionnaires, such as the 36-item Short Form Survey (SF-36), 41 the Quality of Life Index for SCI, 42 and the Satisfaction With Life Scale (SWLS) 43 also were included.
The timing of the outcomes measurements and the procedure used to measure the different outcomes were recorded in order to assess the appropriateness of combining studies in a meta-analysis.
For the meta-analysis, in cases where studies reported more than one measure for a single outcome, the reviewers selected the one that was validated for spinal cord injuries or was reported as the primary outcome of the study, or the one used in the majority of studies. For trials that reported more than one outcome of mobility, the one that included more comprehensive aspects of mobility such as bed mobility, postural changes, balance and locomotion in the same tool was selected.
Statistical analysis
Information about the methods (i.e., design, participants, intervention, measures) and results (i.e., number of participants, mean and standard deviation of outcomes of interest) from each article were extracted by two reviewers (CQDO and LDJ), and checked among reviewers. Where information was not available in the published trial, details were requested from the corresponding author. When trials reported medians and interquartile ranges, the conversion formulae described by Wang and colleagues 44 was utilized to estimate mean and standard deviation. When trials provided standard errors, standard deviations were calculated by multiplying the standard errors by the square root of sample size.
In some trials, two groups of interest performed different forms of ABT interventions and were compared with conventional rehabilitation. In this case, either the most common intervention among the included trials or the intervention that best described the definition of ABT by Backus and colleagues 14 was selected. When both groups received similar modalities of ABT, they were combined into one group, using the formulae provided in the Cochrane Handbook for Systematic Reviews 45 in order to obtain the combined mean and standard deviation for meta-analysis.
The post-intervention scores were used to obtain the pooled estimate of the effect of intervention. For crossover trials, the post-intervention scores for the first intervention period were obtained and considered in the meta-analysis.
A random effects analysis was used to measure the effect size of the combined trials. The analyses were performed using The MIX–Meta–Analysis Made Easy program Version 1.7. 46 For all outcome measures, the significance was set at a level of 0.05 (two-tailed). The pooled data for each outcome were reported as the standardized mean difference—Cohen's d (95% confidence interval [CI]). Where data were not available to be included in the pooled analysis, the between groups difference was reported. Statistical heterogeneity (I2) was also calculated.
Results
Flow of trials through the review
The electronic search strategy identified 22,484 articles (excluding duplicates). After screening titles, abstracts and reference lists, 43 potentially relevant full articles were retrieved. After screening full text of irrelevant abstracts, one more article was considerate relevant. Twenty-six articles failed to meet the inclusion criteria (Table 2 and Appendix 2). Finally, 18 trials were included in this systematic review initially; however, after submission for journal review, one trial that fit the inclusion criteria was published and added to this systematic review, leading to a total of 18 trials included. (Fig. 1). Six trials investigated ABT interventions for recovery of function in the upper limbs, whereas 11 investigated interventions to improve function in the lower limbs. Two trials investigated multi-modal interventions.
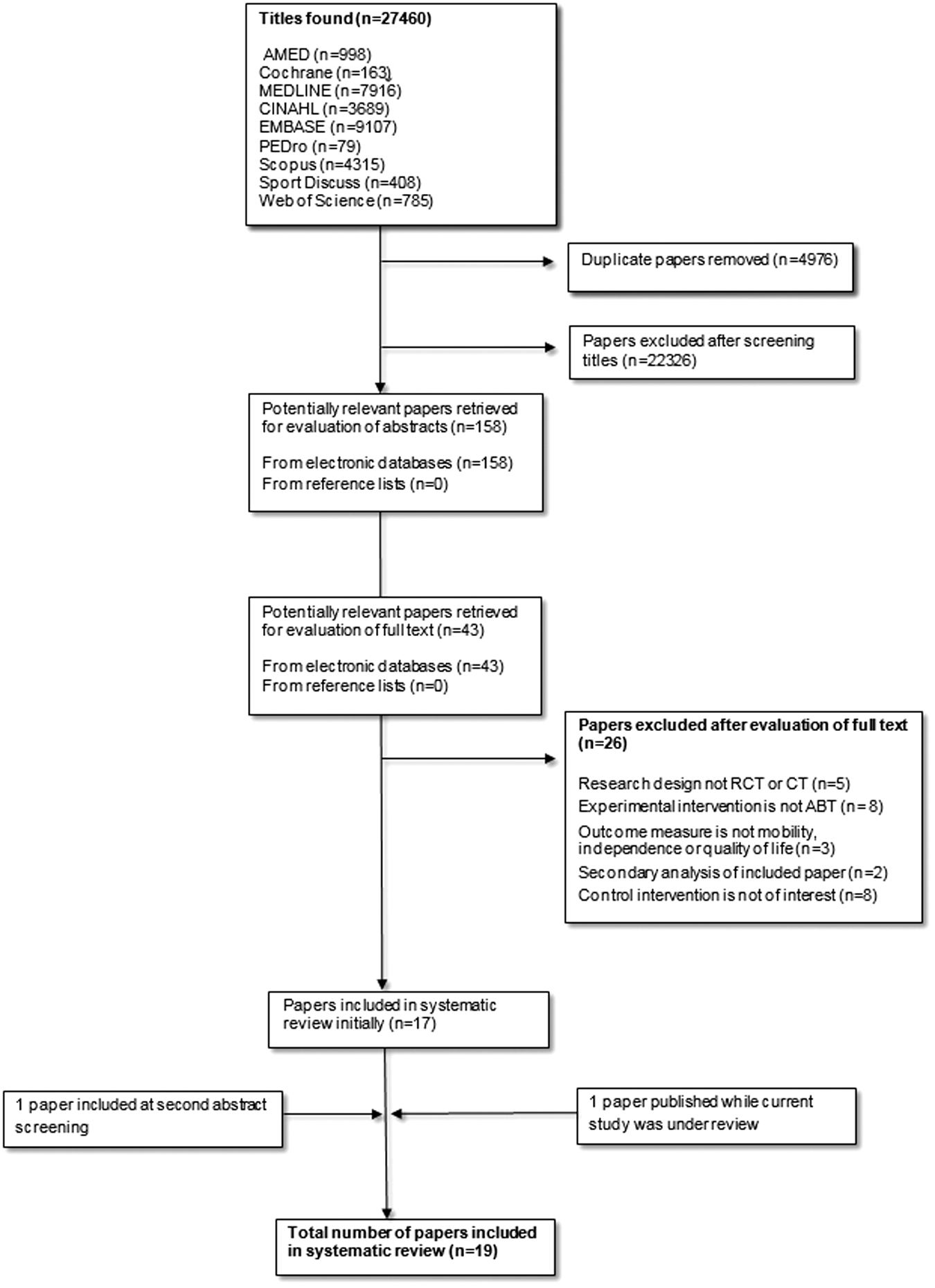
Flow of studies through the review. RCT, randomized clinical trial; CT, controlled trial; ABT, activity-based therapy.
#Groups and outcome measures listed are those that were analyzed in this systematic review. Ages and time since injury means (standard deviation).
RCT, randomized clinical trial; CT, controlled trial; AIS, American Spinal Cord Injury Association Impairment Scale; Exp. experimental group; Con, control group; BWSTT, body weight support treadmill training; BWST, body weight support training; BWS, body weight support; FIM, Functional Independence Measure; QoL, quality of life; WISCI II, Walking Index for Spinal Cord Injuries, version II; BBS, Berg Balance Scale; CHART, Craig Handicap Assessment Report Technique; ADL, activities of daily living; SCIM, Spinal Cord Injury Independence Measure; TUG, Timed Up and Go test; SCI-FAP, Spinal Cord Injury—Functional Ambulation Profile.
Characteristics of included trials
The 19 trials included 639 participants and investigated the efficacy of ABT interventions on mobility, independence, and quality of life outcomes for people with SCI. (Tables 2 and 3). Three trials compared ABT interventions with no intervention, whereas 16 trials compared ABT interventions with conventional physical rehabilitation interventions.
#Groups and outcome measures listed are those that were analyzed in this systematic review; there may have been other groups or measures or assessment time-points in the paper. Ages and time since injury means (standard deviation).
RCT, randomized clinical trial; CT, controlled trial; AIS, American Spinal Cord Injury Association Impairment Scale; Exp, experimental group; Con, control group; FES, Functional Electrical Stimulation; FIM, Functional Independence Measure; TRIHFT, Toronto Rehabilitation Institute Hand Function Test; JTHFT, Jebsen- Taylor Hand Function Test; RELHFT, Rehabilitation Engineering Laboratory Hand Function Test,
Quality
The mean PEDro score of the trials was 5.3 (range 2 to 8; Table 4). The majority of trials (84%) randomly allocated participants and 89% reported between-group differences. Almost all trials (95%) reported point estimate and variability. However, only 26% of the trials conducted intention-to-treat analysis. Not all trials reported concealed allocation nor had blinded assessors (42% and 53%, respectively). The majority of trials (74%) had fewer than 15% drop outs, and had similar groups at baseline (63%). No trials blinded participants or therapists, which is difficult or impossible for complex physical interventions.
Y, yes; N, no.
Participants
The mean age of participants ranged from 28.6 to 59.0 years across the studies. The mean time since injury ranged from 4.5 weeks to 9.5 years. The majority of trials (63%) comprised participants in the chronic phase of injury (i.e., more than 6 months, ranging from 1.8 to 9.5 years after injury). The time since injury in the trials that comprised participants in the acute and sub-acute phase varied from 3.2 to 17.0 weeks after injury. The majority of trials (84%) included only participants with upper motor neuron injuries. Only 26% of the studies included participants with complete injuries (AIS grade A), and 58% included only participants with motor incomplete injuries (AIS grades C and D). The majority of trials (68%) had samples comprising participants with tetraplegia and paraplegia. The percentage of participants with tetraplegia across these trials varied from 29% to 90%, whereas the percentage of people with paraplegia varied from 10% to 71%. Only 32% of the trials had samples composed only of persons with tetraplegia. None of the studies had a sample composed only of persons with paraplegia.
Intervention
Six trials applied ABT interventions to the upper limbs, 21,47 –51 whereas 11 trials 22 –24,52 –59 applied gait-related interventions. Two trials 60,61 investigated multi-modal interventions (whole–body activities); however, since the primary outcomes related to improving function in the lower limbs, these two trials were analyzed and discussed with the trials that applied gait-related interventions.
In all trials that applied gait-related ABT interventions, the experimental intervention was body weight–supported gait training. Four trials 23,24,52,59 applied body weight–supported gait training with manual assistance, whereas two trials 54,55 applied body weight–supported gait training associated with electrical stimulation to the lower limb musculature. Five trials 22,53,56 –58 performed robotic body weight–supported gait training.
All trials that performed body weight–supported gait training utilized a treadmill, except for one trial 22 that had one group walking on a treadmill and one group overground walking. The multi-modal ABT interventions applied by Harness and colleagues 60 and Jones 61 consisted of whole–body activities, which included active-assisted lower limb exercises, whole–body resistance training, load-bearing activities, gait training with and without body weight support, and functional electrical stimulation to muscles below the level of injury.
In three trials, the experimental intervention was delivered to the upper limb, 47,49,50 with the application of functional electrical stimulation to muscles below the level of injury. Two trials 21,48 investigated the effects of massed practice associated with sensory stimulation. One trial delivered intensive task-specific hand training though an instrumented exercise workstation in conjunction with functional electrical stimulation. 51
Overall, participants received ABT training for between 12 to 112 sessions, with a duration of 30 to 180 min, three to five times per week. In three trials, 21,57,61 the comparison group received no intervention. In all the other trials, the comparison group received conventional physical interventions, including: standing passively on a tilt-table 52 ; conventional physiotherapy, 22,24,53 –56,58 including joint mobilization, strengthening of the supralesional musculature and remaining motor function; practice of self-care skills; gait training exercises on parallel bars or with assistive devices 59 ; self-regulated exercises 60,61 ; and conventional occupational therapy. 47 –51 The latter included muscle facilitation exercises, task-specific training, strengthening, electrical stimulation, and motor control activities targeting supralesional areas, stretches, practice of activities of daily living, and caregiver training.
Outcome measures
Independence
The majority of included trials, except for Beekhuizen and Field-Fote, 21 Harness and colleagues, 60 Niu and colleagues, 57 Nasser and colleagues, 48 and Yang and colleagues 59 reported at least one measure of independence before and after the intervention. Five trials 22 –24,52,53 used the FIM reporting scores as a total or for separate domains to assess independence. Four trials 51,56,58,61 used SCIM. Four trials 47,49,50,55 used both FIM and SCIM. In that case, since FIM was the most frequently used outcome among the included trials, it was selected as the outcome measure of choice for the meta-analysis. One trial 54 used the SCIM and the Lawton Instrumental Activity of Daily Living Scale (LIADL) to measure independence; however, they did not report the immediate post intervention values, hence data from LIADL was used in the meta-analysis.
Mobility
The majority of trials, except for Adams and Hicks, 52 reported at least one measure of mobility pre- and post-intervention. Six trials 22,23,53,56,58,59 measured walking mobility using the WISCI II. Other measures of walking mobility were: Spinal Cord Injury Functional Ambulation Index, 61 Functional Ambulation Category (FAC), 58 Spinal Cord Injury-Functional Ambulation Profile, 59 and Walking Mobility Scale. 55 Seven studies 23,24,55 –57,59,61 measured mobility using balance scales. The scales used were the Tinneti Scale, 24 BBS, 23,56 Timed Up and Go Test, 55,57,61 and Activities-specific Balance Confidence scale. 59 Two trials measured general mobility using the Craig Handicap Assessment and Reporting Technique. 54,60
Six trials 21,47 –51 assessed mobility related to upper limb function. The outcome measures used were the Toronto Rehabilitation Institute Hand Function Test, 47,50 the Wolf Motor Function Test, 21,48 JTHFT, 21,48 the Rehabilitation Engineering Laboratory Hand Function Test, 49 and the Action Research Arm Test. 51
Where trials reported more than one measure for mobility, 21,23,48,54 –56,58,59,61 the reviewers selected the tool that assessed either more aspects of mobility (not only walking), had been validated for SCI population, was frequently used in other trials, or was the primary outcome of the trial.
Quality of life
Only four trials assessed quality of life. The outcome measures used were: Assessment of Quality of Life 8 (AQoL-8), 51 Quality of life Index version III, 52 SF-36, 24 and SWLS. 54
Activity-based therapy interventions compared with no intervention
Three trials 21,57,61 compared the effects of ABT interventions with no intervention.
Effectiveness on independence
Only one trial compared the efficacy of ABT interventions with no intervention for improving independence. Jones 61 demonstrated that a multi-modal ABT program did not improve independence more than no intervention in 20 people with chronic motor incomplete SCI. The between-group difference on the SCIM was −0.7 points (95% CI: −13.71 to 12.31). The PEDro score was 5, indicating moderate scientific quality.
Effectiveness on mobility related to upper limb function
Only one study compared the efficacy of ABT interventions with no intervention with the aim of improving upper limb function. Beekhuizen and Field-Fote 21 demonstrated that massed practice associated with median nerve stimulation improved hand function in people with chronic incomplete tetraplegia. The between-groups difference on the JTHFT in response to intervention was 44.6 seconds (95% CI: 16.07 to 105.21), with a large effect size (d = 0.95). The PEDro score was 4, indicating moderate quality; however, the sample size was small (n per group = 6).
Effectiveness on lower limb mobility
Two studies 57,61 reported the efficacy of ABT interventions for improving lower limb mobility, compared with no intervention, for people with chronic incomplete SCI. The effect was examined by pooling post-intervention data of the two trials involving 79 participants. There was no statistical heterogeneity (I2 = 0). ABT interventions had a small positive effect on lower limb mobility with no statistical significance. (d = 0.2, 95% CI: −0.2 to 0.7; Fig. 2; see Fig. 1 in Appendix 3 for the detailed forest plot). Both trials received a PEDRo score of 5, indicating moderate quality.

Activity-based therapy interventions versus no intervention for independence (n = 79). Standardized mean difference (SMD; Cohen's d and 95% confidence interval [CI]).
Activity-based therapy interventions compared with conventional physical interventions
Effectiveness of ABT interventions for lower limbs for improving independence
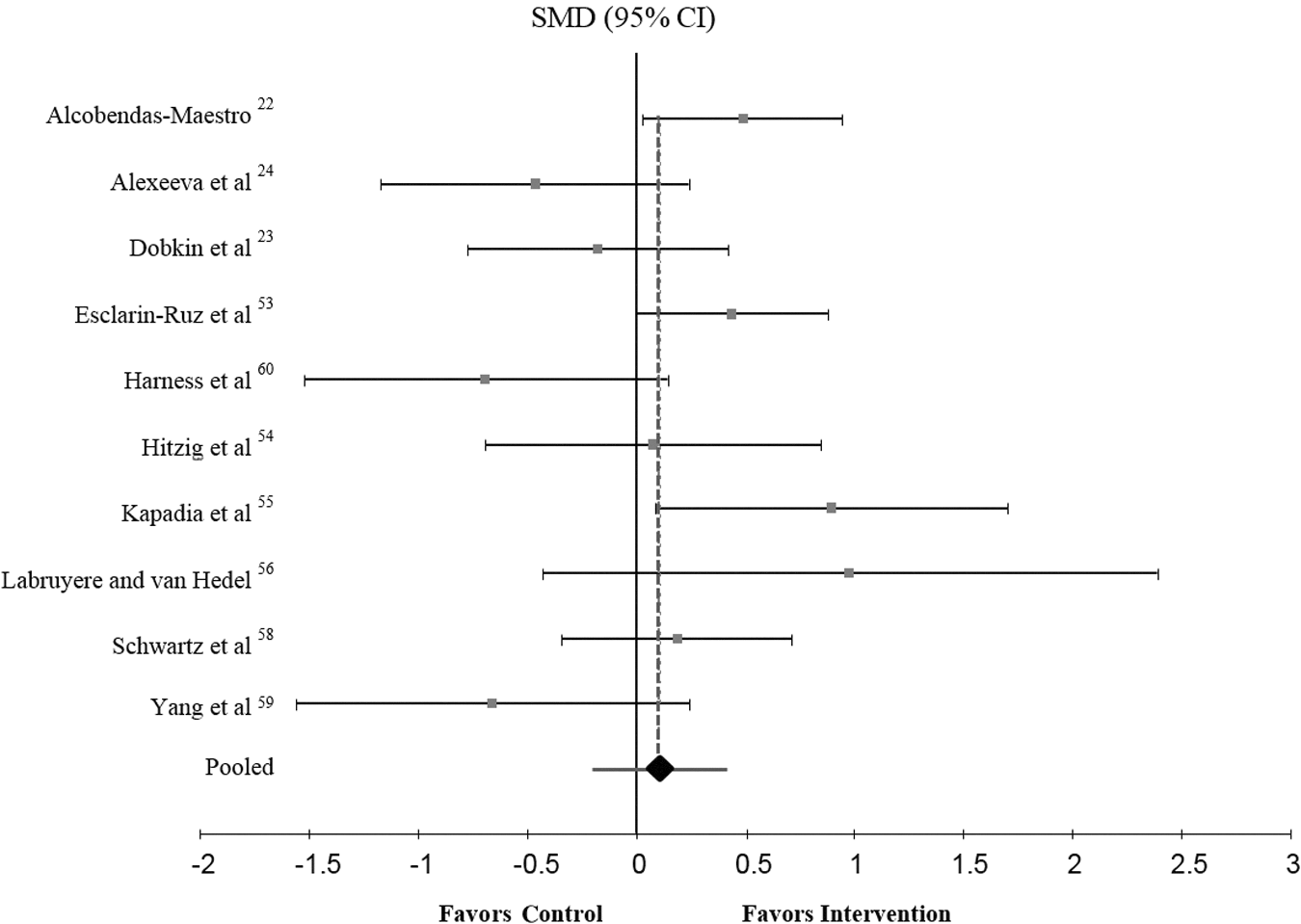
The effect of ABT interventions for the lower limbs on independence was examined by pooling post-intervention data from nine trials involving 364 participants. There was low statistical heterogeneity (I2 = 31%). The statistical analysis revealed no greater effectiveness of ABT interventions than of conventional interventions on independence (d = 0.13, 95% CI: −0.14 to 0.39; Fig. 3; see Fig. 2 in Appendix 3 for the detailed forest plot). The mean PEDro score was 6, indicating moderate to high quality.
Activity-based therapy interventions for lower limbs versus conventional physical interventions for independence (n = 364). Standardized mean difference (SMD; Cohen's d and 95% confidence interval [CI]).
Effectiveness of ABT interventions for upper limbs for improving independence
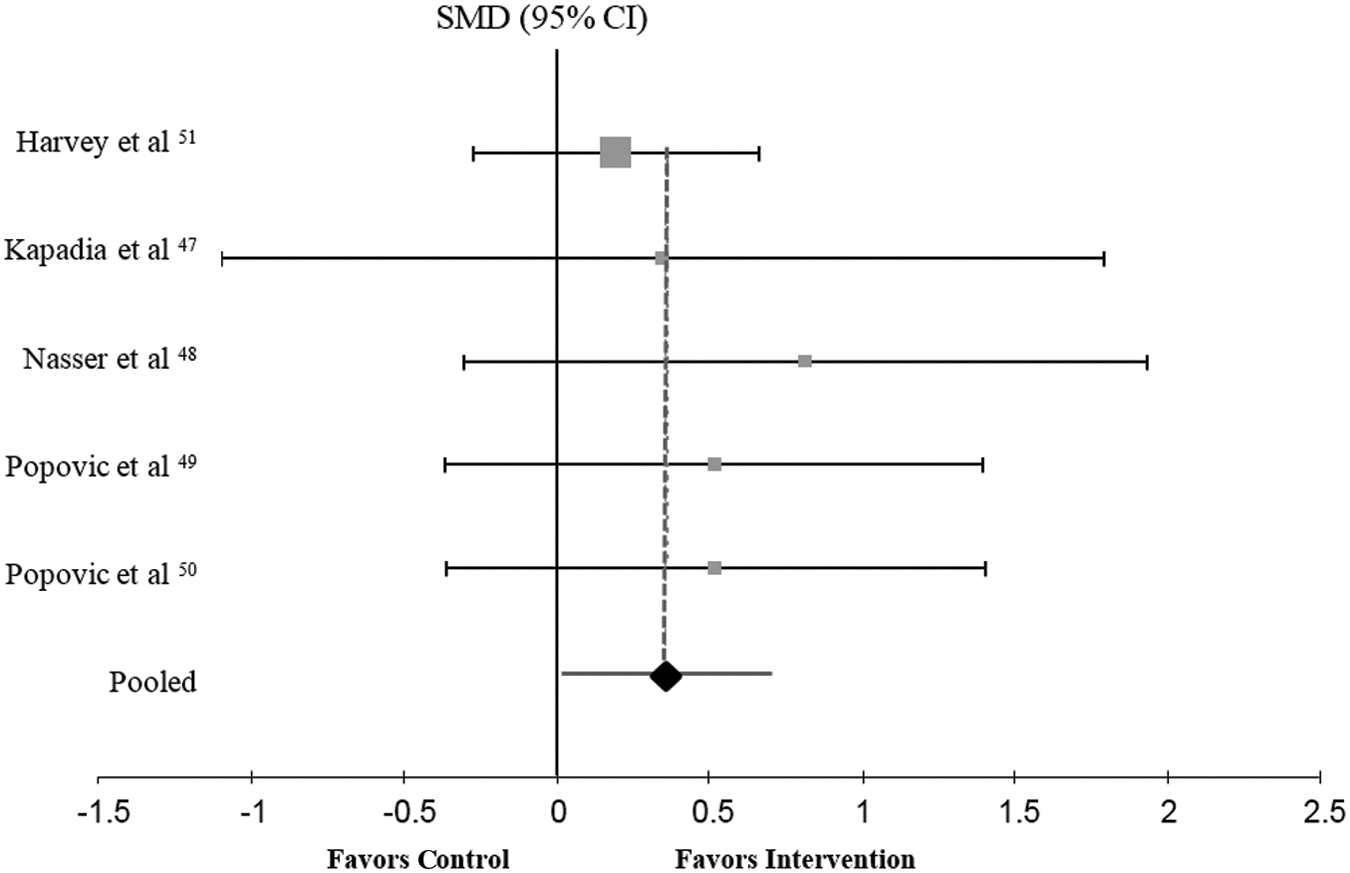
The effect of ABT interventions for the upper limbs on independence was examined by pooling post-intervention data from four trials involving 120 participants. There was no statistical heterogeneity (I2 = 0). There was a positive effect on independence of ABT interventions targeting the upper limbs. There was a moderate effect size (d = 0.51, 95% CI: 0.15 to 0.88) in favor of ABT interventions (Fig. 4; see Fig. 3 in Appendix 3 for the detailed forest
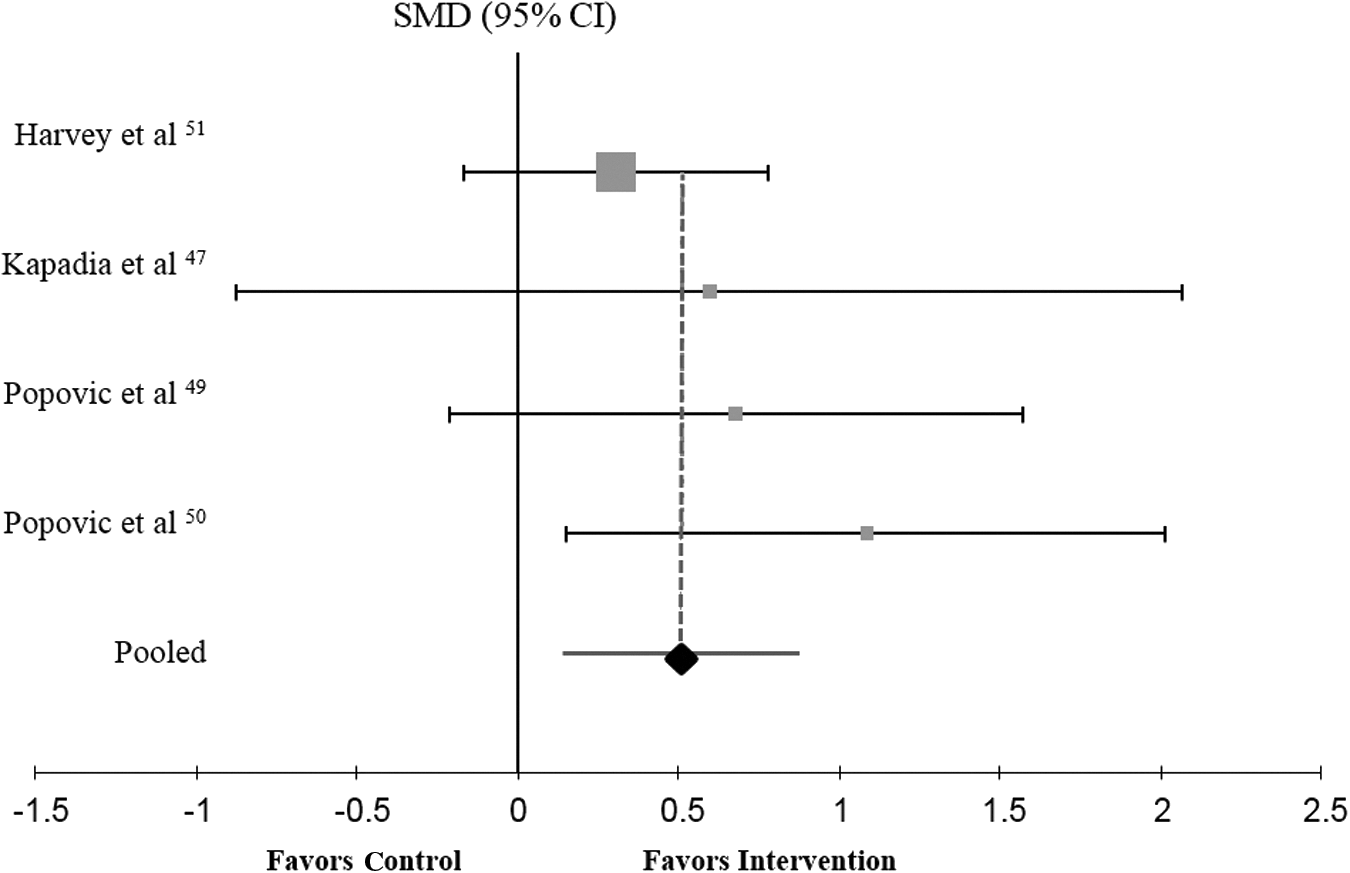
Activity-based therapy interventions for upper limbs versus conventional physical interventions for independence (n = 120). Standardized mean difference (SMD; Cohen's d and 95% confidence interval [CI]).
Effectiveness of ABT interventions for lower limbs for improving mobility
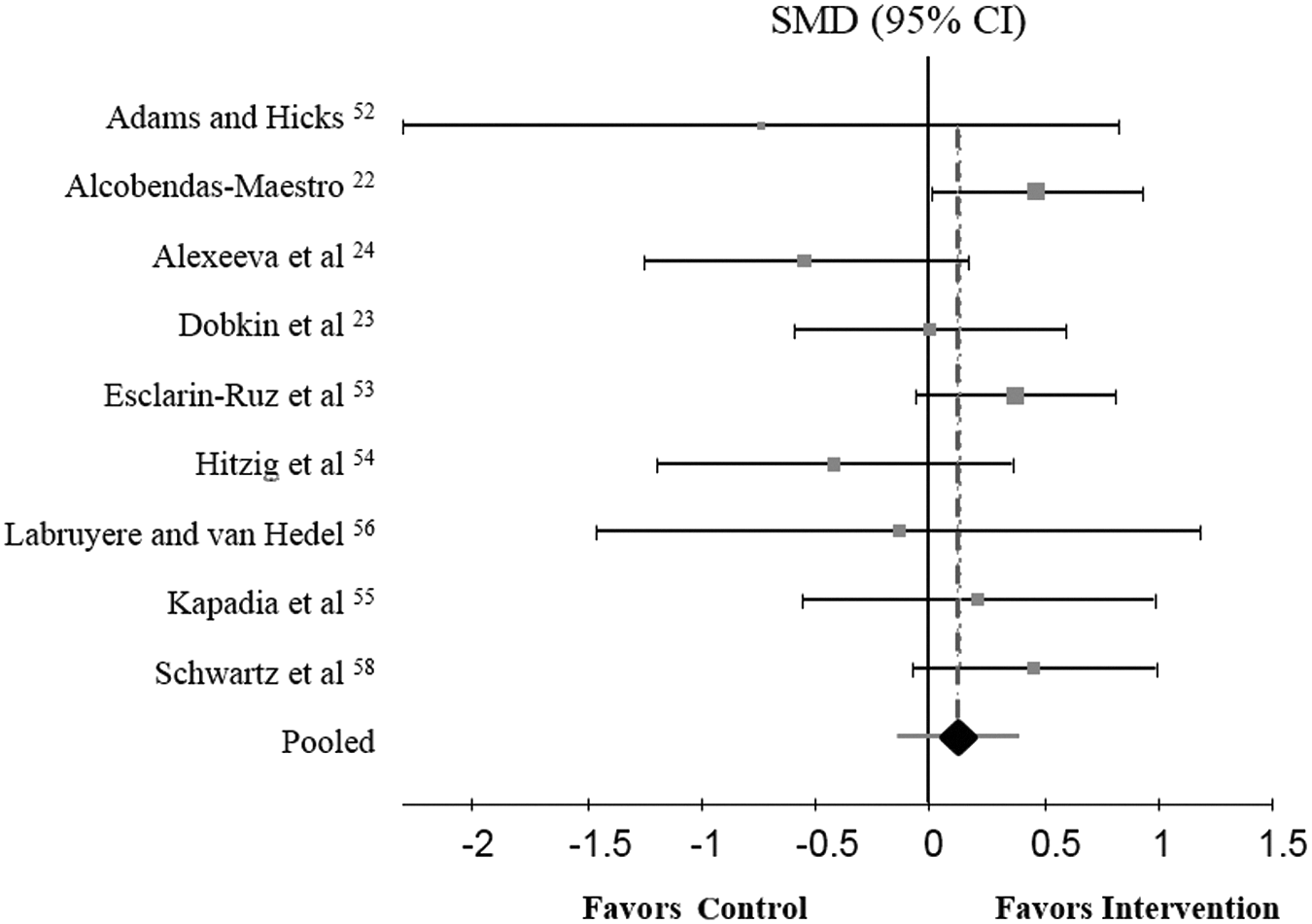
The effect of ABT interventions on lower limb mobility was examined by pooling data from 10 trials including 406 participants. There was moderate statistical heterogeneity (I2 = 54%) that seems to be due to methodological differences among trials, such as variable sample sizes (ranging from 9 to 83), length of interventions (ranging from 30 to 120 min), and time since injury (ranging from <2 to 114 months). The effect size was close to zero (d = 0.11, 95% CI: −0.21 to 0.42) in favor of ABT interventions with no statistical significance (Fig. 5; see Fig. 4 in Appendix 3 for the detailed forest plot). The mean PEDro score was 6, indicating moderate to high quality.
Activity-based therapy interventions for lower limbs versus conventional physical interventions for mobility (n = 406). Standardized mean difference (SMD; Cohen's d and 95% confidence interval [CI]).
Effectiveness of ABT interventions for upper limbs for improving mobility related to upper limb function
The effect of ABT interventions on upper limb function was examined by pooling data from five trials including 135 participants. There was no statistical heterogeneity (I2 = 0). There was a positive effect on upper limb function, compared with conventional interventions. There was a small to moderate effect size (d = 0.4, 95% CI: 0.02 to 0.71) in favor of ABT interventions (Fig. 6; see Fig. 5 in Appendix 3 for the detailed forest plot). The mean PEDro score was 4.2 representing moderate quality.
Activity-based therapy interventions for upper limbs versus conventional physical interventions for mobility related to upper limb function (n = 135). Standardized mean difference (SMD; Cohen's d and 95% confidence interval [CI]).
Effectiveness of ABT interventions for improving quality of life
The effect of ABT interventions on quality of life was examined by pooling data from four studies including 139 participants. There was no statistical heterogeneity (I2 = 0). There was no difference between ABT interventions and conventional interventions on quality of life (d = 0.11, 95% CI: −0.23 to 0.45; Fig. 7; see Fig. 6 in Appendix 3 for the detailed forest plot). The mean PEDro score was 6, indicating moderate to high quality.

Activity-based therapy interventions versus conventional physical interventions for quality of life (n = 139). Standardized mean difference (SMD; Cohen's d and 95% confidence interval [CI]).
Forest plots, as presented herein, provide a graphical display of the extracted results from studies included in meta-analysis. They were used in this systematic review and meta-analysis to demonstrate the measure of effect (standardized mean difference, Cohen's d). Each square represented a single study, with its area characterizing the study's weight in the meta-analysis. The dashed vertical line and the diamond represent the overall effect size, and the lateral points denote confidence intervals. A vertical line representing no effect also has been shown.
Discussion
This systematic review and meta-analysis provided evidence that ABT interventions that aimed at improving lower limb function had no effect on independence or mobility when compared with no intervention and conventional physical interventions. In contrast, our findings revealed that ABT interventions that aimed towards improving upper limb function promoted significant and marked changes in upper limb function and independence, compared with no intervention or conventional physical interventions. Overall, ABT interventions had no effect on quality of life compared, with no intervention or conventional physical interventions.
A large number of trials were found in the initial search of titles. This was attributed to the search strategy conducted using the keyword “exercise” instead of “activity-based therapy.” ABT is an idiom that has emerged only in the past 10 to 15 years and some researchers still avoid its use, believing the phrase to be inaccurate or an umbrella term. Hence, in order not to miss any relevant trials that used an exercise intervention targeted to the areas below the site affected by spinal cord injury without using “activity-based therapy” as a search phrase, the word “exercise” was included. This led to a much larger number of citations being discovered when compared with previous reviews involving ABT. For the same reason, the authors re-assessed the full text articles for the abstracts that had been excluded at the initial screening. As result, another article was added, 59 which employed the term “endurance training,” referring to body weight–supported treadmill training, but leading to its exclusion at the abstract stage of selection for subsequent full text review.
The most frequently investigated ABT modality was body weight–supported treadmill training. Several non-controlled trials found beneficial functional outcomes on the ability to stand, balance and walk, especially in individuals with incomplete impairments. 17,28,62 –67 However, the data pooled from the included trials, both randomized and non-randomized, demonstrated little or no effect when compared with either no intervention or to conventional interventions in the domains of independence, general mobility and quality of life. This finding is in accord with a systematic review conducted by Mehrholz and colleagues 19 that investigated the effects of body weight–supported treadmill training on locomotor function. The authors included five RCTs and found that gait-related ABT interventions had no significant effects on speed of walking or walking capacity.
ABT interventions that sought to improve lower limb function did not result in greater independence, compared with no intervention or conventional physical interventions. For functional mobility, a small effect size in favor of ABT interventions was detected, compared with none or to conventional physical therapy interventions, although with no statistical significance. (d = 0.2 and d = 0.11, respectively). These findings are inconsistent with a previous systematic review conducted by Backus and colleagues 14 that reported positive effects on functional outcomes and walking ability; however, non-controlled trials were included in their review and no meta-analysis was conducted. The results of the current systematic review provided stronger evidence about the lack of proven efficacy for commonly used ABT interventions for the lower limbs; thus, the conclusions reached were based on a meta-analysis of 10 trials of reasonable quality. Our findings are important to guide clinicians in appropriate clinical decision-making regarding interventions to improve independence or general mobility for people after SCI. As part of evidence-based practice, it is important for clinicians to considerate the patient's preferences. However, ABT interventions for lower limbs, especially body weight–supported treadmill training, are costly, requires expensive equipment, and are more staff intensive than conventional physical therapies; therefore, the cost-benefit may not be advantageous.
Nonetheless, ABT interventions that sought to improve upper limb function have clearly demonstrated superiority over no intervention and conventional rehabilitation with regard to mobility and independence in areas of self-care and ability to reach and manipulate objects. A medium effect size (d = 0.51) in favor of ABT interventions was detected for independence when compared with conventional therapies. In addition, a small to medium effect size (d = 0.4) for upper limb function was found. This finding corroborated a recent systematic review conducted by Lu and colleagues, 68 which investigated the effects of training upper limb function in people with cervical SCI. Of the 16 articles included, five applied ABT interventions. Their results demonstrated that exercise therapy could improve arm and hand function after SCI. In addition, Backus and colleagues 14 found improved neurologic and upper extremity functional outcomes following ABT interventions that were task-specific, regardless of the level of injury.
In the present review, the methodological quality of the trials investigating interventions focused on the upper limbs was inferior (mean PEDro score = 4.2) to those trials investigating lower limb interventions (mean PEDro score = 6), potentially providing a source of bias. Moreover, three 47,49,50 of the six trials that investigated upper limb function were performed by the same group of researchers, which may have contributed to the low statistical heterogeneity and similar results among these trials.
Another possible hypothesis for the positives effects on upper limb functional capacity in comparison to the minimal effects on lower limbs could be due to the nature of tasks performed by the upper limbs that would require lower loads than tasks performed by the legs. Even small increments in arm and hand function may have a profound impact on a person's independence in self-care and activities of daily living.
Loss of arm and hand function is one of the most devastating impairments after a cervical SCI and it is a priority for recovery in people with tetraplegia. 68,69 The current review provides evidence that ABT interventions for the upper limbs are a sound strategy for clinicians to improve functional independence and mobility related to upper limb function. Further, the ABT interventions for upper limbs are not as costly or demanding on staff resources as those targeted to the lower limbs, and hence are easier to implement.
Despite the devastation of SCI and its profound impact on quality of life, the present review was the first to investigate the efficacy of ABT interventions on quality of life. Only four included trials reported quality of life outcomes with no positive effects. The quality of the included trials was moderate to high; however, sample sizes were quite small in most of them, except for Harvey and colleagues 51 This finding differs from the results of non-controlled trials that have shown important improvements in quality of life and life satisfaction after ABT interventions. 70 –73
This review has both limitations and strengths. The mean PEDro score of 5.3 for the 19 trials included in this review represents moderate scientific quality overall. A source of bias in included herein trials was lack of blinding of therapist and patients, but it is rarely feasible to blind therapists and participants during ABT interventions. Other sources of bias were lack of blinded assessors and not reporting concealed allocation or whether an intention-to-treat analysis was undertaken. The majority of trials included in this review had relatively small sample sizes, with only five trials 22,23,51,53,59 reporting sample size power calculations. Moreover, the trials included varied on levels of function of participants, time since injury, training methods, and outcome measures, which resulted in methodological heterogeneity; however, the statistical heterogeneity was low. For this reason, subanalyses of upper and lower limb outcomes by duration since injury, type of training modality/methodology or functional status of participants was deemed inappropriate. Further, publication bias inherent to systematic reviews was avoided by including studies published in languages other than English to the search, but no articles in other languages met the criteria to be included in this review.
In conclusion, this systematic review provided evidence that ABT interventions can improve independence and function when applied to the upper limbs in people with SCI. However, they are not superior to conventional physical interventions when applied to the lower limbs. There were no effects on quality of life. Considering the costs involved and labor intensity required to deliver ABT interventions to the lower limbs, it is recommended that clinicians be judicious when delivering ABT interventions.
Footnotes
Acknowledgments
The authors acknowledge Spinal Cord Injuries Australia. This review was registered at PROSPERO (CRD42015017917).
Author Disclosure Statement
No competing financial interests exist.
Appendix 1: Search Strategy for Systematic Review: Effects of Activity-Based Therapy Interventions on Mobility,Independence,and Quality of Life for People With Spinal Cord Injuries
Appendix 2
| Reasons for exclusion | |||||
|---|---|---|---|---|---|
| Studies | 1 | 2 | 3 | 4 | 5 |
| Beekhuizen and Field-Fote (2005) | ✓ | ||||
| Boswell-Ruys et al (2010) | ✓ | ||||
| Ditor et al. (2003) | ✓ | ||||
| Dobkin et al. (2007) | ✓ | ||||
| Field-Fote (2001) | ✓ | ||||
| Field-Fote et al (2005) | ✓ | ||||
| Field-Fote and Roach (2011) | ✓ | ||||
| Freivogel et al (2009) | ✓ | ||||
| Fritz et al. (2011) | ✓ | ||||
| Harvey et al (2010) | ✓ | ||||
| Harvey et al (2011) | ✓ | ||||
| Hicks et al. (2003) | ✓ | ||||
| Hoffman and Field-Fote (2010) | ✓ | ||||
| Jayamaran et al. (2013) | ✓ | ||||
| Jones (2014) | ✓ | ||||
| Kim et al. (2010) | ✓ | ||||
| Klose et al. (1990) | ✓ | ||||
| Kowalczewski et al. (2011) | ✓ | ||||
| Lucarelli et al. (2011) | ✓ | ||||
| Nooijen et al. (2009) | ✓ | ||||
| Pillastrini et al. (2007) | ✓ | ||||
| Ponstans et al. (2004) | ✓ | ||||
| Spooren et al. (2011) | ✓ | ||||
| Wernig et al. (1995) | ✓ | ||||
| Wriz et al. (2011) | ✓ | ||||
| Wu et al. (2012) | ✓ | ||||
1 = Research design not randomized clinical trials or controlled trials; 2 = Experimental intervention is not activity-based; 3 = Outcome measure is not mobility, independence, or quality of life; 4 = Secondary analysis of included paper; 5 = Control intervention is not of interest.