
Abstract
Traumatic spinal cord injury (SCI) represents a significant burden of illness, but it is relatively uncommon and heterogeneous, making it challenging to achieve sufficient subject enrollment in clinical trials of therapeutic interventions for acute SCI. The Rick Hansen Spinal Cord Injury Registry (RHSCIR) is a national SCI Registry that enters patients with SCI from acute-care centers across Canada. To predict the feasibility of conducting clinical trials of acute SCI within Canada, we have applied the inclusion/exclusion criteria of six previously conducted SCI trials to the RHSCIR data set and generated estimates of how many Canadian persons would have been eligible theoretically for enrollment in these studies. Data for SCI cases were prospectively collected for RHSCIR at 18 acute and 13 rehabilitation sites across Canada. RHSCIR patients enrolled between 2009–2013 who met the following key criteria were included: non-penetrating traumatic SCI; received acute care at a RHSCIR site; age more than 18, less than 75 years, and had complete admission single neurological level of injury data. Inclusion and exclusion criteria for the Minocycline in Acute Spinal Cord injury (Minocycline), Riluzole, Surgical Timing in Acute Spinal Cord Injury Study (STASCIS), Cethrin, Nogo antibody study (NOGO), and Sygen studies were applied retrospectively to this data set. The numbers of patients eligible for each clinical trial were determined. There were 2166 of the initial 2714 patients (79.8%) who met the key criteria and were included in the data set. Projected annual numbers of eligible patients for each trial were: Minocycline, 117; Riluzole, 62; STASCIS, 109; Cethrin, 101; NOGO, 82; and Sygen, 70. An additional 8.0% of the sample had a major head injury (Glasgow Coma Scale [GCS] score ≤12) and would have been excluded from the trials. RHSCIR provides a comprehensive national data set that may serve as a useful tool in the planning of multicenter clinical SCI trials.
Introduction
T
The challenges of conducting trials of acute SCI are well recognized. Because many potential treatments are neuroprotective, their administration is time-sensitive and requires that patients be expeditiously assessed and enrolled at acute-care facilities. The number of patients who can potentially participate in such clinical trials can be reduced based on the time it takes for them to be transferred to the acute care hospital, particularly at centers with large geographic catchments. Patients with multi-trauma patients often have concomitant traumatic brain injury (TBI), 3 which may preclude outcome measure assessment and enrollment in trials. Older patients, who may be more susceptible to SCI after relatively minor trauma because of pre-existing spinal stenosis, are more likely to have co-morbidities that may also exclude them from participating in trials.
Detecting treatment effects can also be difficult. Patients with incomplete injuries typically achieve some level of spontaneous recovery after injury, and variability in this recovery makes it difficult to elucidate whether a person's recovery is attributable to treatment rather than natural recovery; as such, large numbers of patients may be required to detect a realistic therapeutic effect. 4 Selecting patients with specific severity and neurologic levels of injury can reduce heterogeneity, but this reduces the pool of potential study participants significantly. Although there are more than 1700 new cases of SCI in Canada per year, 1 the incidence is relatively low in comparison with other diseases, so that even multi-center studies can experience recruitment challenges. 5
SCI trials are costly and time-consuming. 6 Optimal trial design is crucial for success, and it is important to understand study feasibility a priori. Lee and associates 4 reported on the proportion of patients with SCI who might be eligible for acute SCI trials using prospective registry data from a single center. Within Canada, however, geographic, demographic, and trauma system variability suggest that this proportion may differ significantly between SCI centers. The Canadian Health Care System, with its universal coverage and single payer system, in concert with the Rick Hansen Spinal Cord Injury Registry (RHSCIR), a national registry of traumatic SCI cases, would theoretically create an ideal opportunity for performing acute care clinical SCI trials. Understanding the available patient population for acute intervention studies would facilitate power calculations, determination of study feasibility, and could influence study design so as to best direct resources to achieve most effective and efficient recruitment.
The purpose of this article was to use the published inclusion/exclusion criteria for six SCI trials and apply these criteria to the patient population identified across Canada through RHSCIR. By comparing specific eligibility criteria with actual patient characteristics, we will examine the potential for recruitment to SCI trials at centers across Canada and provide some insights into the feasibility of performing multi-center trials in the Canadian environment.
Methods
RHSCIR
RHSCIR was initiated in 2004 and was developed to collect data on persons who sustain SCIs and link clinicians, researchers, and healthcare administrators. RHSCIR was expanded in the years after inception, thereafter to achieve consistent, national enrollment in 2009. A broad objective of such a registry is to improve both research and clinical practice for persons with SCI by facilitating the translation of research into clinical practice and promoting evidence-based practices. The RHSCIR sites include 18 acute and 13 rehabilitation facilities representing all the major regions of Canada and all specialized SCI treatment facilities. All RHSCIR sites are required to obtain local Research Ethics Board (REB) approval before enrolling participants into the registry.
Any person over the age of majority who is treated at a RHSCIR site for a new traumatic SCI is eligible for inclusion in the registry. Participants who provide informed consent have an expanded data set collected including information regarding acute treatment (surgical procedure vs. no surgical procedure and the time from injury to operation). Participants who do not provide informed consent or are unable to be approached during their initial hospitalization (e.g., those found by local case finding) are included in RHSCIR with a core data set recorded as per local REB approvals, thus capturing all newly injured persons admitted to the site.
A detailed neurological assessment according to the International Standards for the Neurological Classification of Spinal Cord Injury 7 is conducted by trained clinicians at the registry sites as a part of standard of care and is recorded in both the core and expanded data sets. Details of the RHSCIR data set have been described previously. 8 Note that participation in any studies or trials does not exclude participation in RHSCIR.
Retrospective identification of potentially eligible trial participants
Participants with a complete RHSCIR record (data complete up to discharge to the community) were considered as potentially eligible for SCI clinical trials if they had a non-penetrating traumatic SCI, received acute care at a RHSCIR site, and were over the age of 18 and under the age of 75 (in consideration of common age restrictions in clinical trials). To ensure completeness of annual data and regular recruitment from all sites cases, because site participation was staggered over earlier years, patients enrolled in RHSCIR between 2009–2013 were used to generate average enrollment projections. Those with the recorded presence of co-morbidities that frequently exclude potential participants from clinical trials were then excluded from the potential trial population. Minor co-morbidities (Table 1) unlikely to exclude persons from trial participation were recorded but were not used to exclude registry participants from the potential trial population.
Presence of one or more of the serious complications excluded participants for the purposes of this study.
Example SCI clinical trials
Major inclusion criteria from several recent/ongoing acute SCI clinical trials were then applied to the sample. Criteria from five previously conducted drug trials were applied: Minocycline in Acute Spinal Cord Injury (Minocycline), 9 Riluzole in Spinal Cord Injury Study, 10 Cethrin, 11 Nogo antibody study (NOGO; personal communication with NOGO Investigator A. Curt, March 2015), and Sygen in Acute Spinal Cord Injury. 12 A large-scale surgical SCI study was also included: Surgical Timing in Acute Spinal Cord Injury Study (STASCIS), 13 a multi-center, international, prospective cohort study evaluating the relative effectiveness of early (<24 ho after injury) versus late (≥24 h after injury) decompressive surgical procedure after traumatic cervical SCI.
Criteria for inclusion into these clinical trials that were applied to the RHSCIR potential trial population included time from injury to first acute admission to a RHSCIR site, the SNL (single neurological level) and American Spinal Injury Association Impairment Scale (AIS) at admission to the acute RHSCIR site, and whether and operation was performed within 7 days. Study-specific criteria applied were as follows:
Minocycline
SNL C0–C8; time from injury to acute RHSCIR site ≤11 h (to allow for treatment within 12 h of injury).
Riluzole
SNL C4–C8; AIS A, B, C; time from injury to acute RHSCIR site ≤11 h (to allow for treatment within 12 h of injury).
STASCIS
SNL C0–C8; time from injury to acute RHSCIR site ≤16 h (chosen as cutoff to have surgical procedure within 24 h); acute surgical procedure was performed within 7 days of injury.
Cethrin
Cethrin (thoracolumbar): SNL T2–T12; AIS A; administered at the time of decompressive operation, within 7 days of injury. Cethrin (cervical): SNL C4–T1; AIS A; administered at the time of decompressive operation within 7 days of injury.
NOGO
SNL C5–T11; AIS A; treatment within 4–28 days post-injury (i.e.. time from injury to acute RHSCIR site ≤28 days of injury).
Sygen
SNL C1–T9; one/both lower extremity motor scores (LEMS) at admission ≤15/25; time from injury to admission to acute RHSCIR site ≤7 h from injury (chosen as cutoff to have methylprednisolone administered within 8 h of injury).
Trial numbers and imputation of missing data
The trial numbers in Figure 1 and Figure 2 were obtained in a stepwise fashion. In other words, the number of participants who fulfilled a certain trial criterion were the total number of participants available for the next criterion, from which a new number of fulfilled, excluded, and missing were derived. The trial numbers in Table 2 were obtained by applying the same percentages by year from available data to the new total numbers from each trial after imputation on missing data.
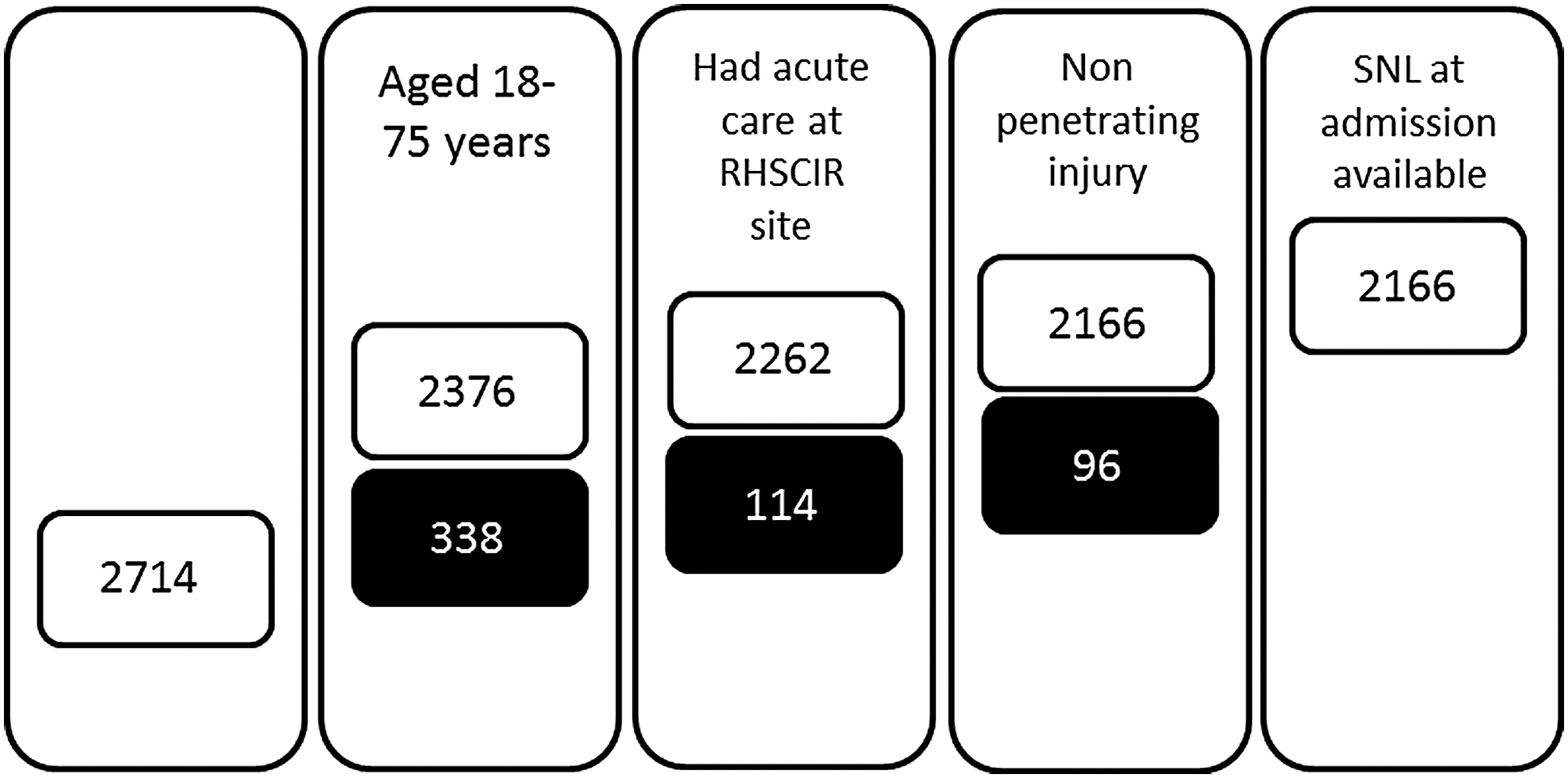
Number of Rick Hansen Spinal Cord Injury Registry (RHSCIR) patients when key exclusion criteria are applied to the entire cohort (n = 2714). Black boxes represent the number of patients not meeting the given criteria. SNL, single neurological level.
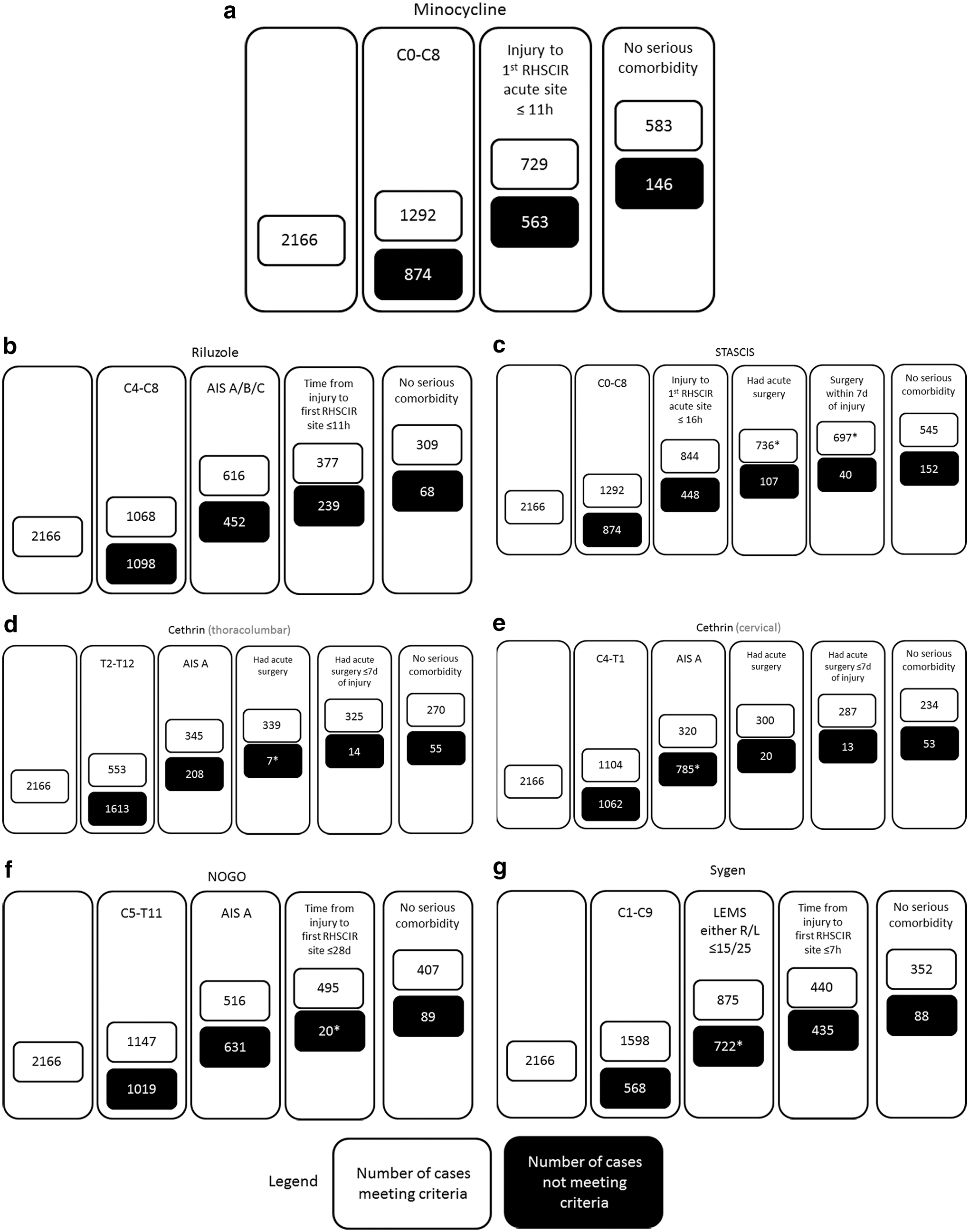
Rick Hansen Spinal Cord Injury Registry (RHSCIR) cases remaining after study-specific inclusion criteria and co-morbidity exclusion criteria were applied for the example trials: (
STASCIS, Surgical Timing in Acute Spinal Cord Injury Study; NOGO, Nogo antibody study.
To report the number of potential trial participants more fairly, missing data were imputed for single neurological level, surgery (y/n and time from injury to operation), AIS, and co-morbidity. Specifically, the same percent of exclusions from available data were applied to the missing data, and new estimated numbers of included and excluded participants were obtained. The imputation for single neurological level was performed on actual missing data from available data, while imputation for surgical procedure (y/n and time from injury to operation), AIS, and co-morbidity data was performed on the estimated missing data.
Co-morbidities
Co-morbidities collected for RHSCIR are based on the Charlson Comorbidity Index 14 ; these are listed in Table 1, including their seriousness, with those deemed as serious being considered as an exclusion criterion for most clinical trials. Co-morbidity data are part of the expanded RHSCIR data set and are not collected in those in the core data set. Among those who had co-morbidity data from the expanded RHSCIR data set, the percentage of persons with a serious co-morbidity was determined; missing co-morbidity data were imputed as above.
Estimated exclusions based on Glasgow Coma Scale (GCS) score and consent status
A GCS score of 12 or less 15 is considered to indicate a moderate/major head injury that would likely preclude participation in a clinical trial for discussion purposes. GCS data are provided to RHSCIR from administrative hospital data, and many values are missing in provided extracts. To calculate the most accurate count of potential trial participants, rather than limiting the analysis cohort on the basis of incomplete data, we estimated the proportion of participants with a GCS of 12 or less based on available data.
The analysis cohort was also not limited by whether or not the patients consented to the expanded RHSCIR data set, because it would not be appropriate to assume consent to the RHSCIR would be equivalent to consent to an acute therapeutic study. These consent rates will be reported and discussed, however.
Results
Potential trial population
There were 2714 patients with completed admission data recruited into RHSCIR over a period of five years between 2009 and 2013; 338 were excluded for age <18 or >75 (Fig. 1). Of the remaining 2376 patients, 114 had not received their care at an acute RHSCIR site, leaving 2262 potential patients. There were 96 of 2262 (4.2%) patients who had penetrating injuries, leaving 2166 potential patients.
Consent rates
An expanded data set requiring consent was obtained for 1213 (56.0%) of the 2166 cases; 1504 were asked to provide consent (Fig. 3). Reasons for being unable to approach for consent included: being discharged too quickly or it being medically inappropriate to consent (27.5%), and language or cognitive barriers (4.2%). Of those who were asked to provide consent (1504/2166), 234 (15.6%) declined consent and 55 (3.7%) withdrew after enrollment; consent status was missing for two patients.

Expanded dataset availability and consent status.
Enrollment criteria for SCI trials
The minocycline clinical trial (Minocycline) requires randomization and intravenous administration of minocycline to patients with acute cervical SCI within 12 h of injury. There were 1292/2166 (59.6%) patients meeting Minocycline's SNL criteria of C0–C8 (Fig. 2) with a baseline AIS of A, B, C, or D, and 729 (56.4%) of those arrived at the RHSCIR facility within 11 h of injury. Of those 729 patients, 146 (20.0%) had a serious co-morbidity, leaving 583 potential subjects over the 5-year period from 2009–2013.
With respect to the Riluzole study, 1068 met the SNL criteria (C4–C8), and 616 had a baseline AIS of A, B, or C). There were 377 (61.2%) patients who arrived at the RHSCIR facility within 11 h. There were 68 (20.4%) patients excluded for serious co-morbidity, leaving 309 potential subjects.
STASCIS was a prospective observational study to evaluate the timing of decompressive operation in cervical SCI between “early” (<24 h) and “late” (>24 h but <7 days). When the criteria for STASCIS were applied to the 2166 patients, 1292 fit the SNL criteria (C0–C8); 844/1292 patients presented to an acute RHSCIR center within 16 h of injury. Among those 844 patients, 736 had a surgical procedure. Among those who had an operation, 697/736 had the procedure within seven days of injury. Of those 697 patients, 152 (21.8%) had at least one serious co-morbidity, leaving 545 potential STASCIS patients.
The original Cethrin study required the extradural application of the recombinant protein in AIS A cervical and thoracic patients with SCI at the time of surgical decompression, within seven days of injury. Cethrin (thoracolumbar) included thoracic (T2–T12) motor complete (AIS A) patients who had a surgical procedure within seven days of injury; 553/2166 fit the SNL criteria (T2–T12), and 345 of these fit the AIS A criteria. There were 339/345 patients who had an acute surgical procedure; of those, 325/339 had acute operation within seven days of injury. There were 55/325 patients who had one or more serious co-morbidities, leaving 270 potential Cethrin (thoracolumbar) patients. Cethrin (cervical) included cervical (C4–T1) motor complete (AIS A) patients with acute SCI who had a surgical procedure within seven days of injury; 1104/2166 patients fit the SNL criteria (C4–T1), and 320/1104 fit the AIS A criteria. There were 300/320 who had an acute operation, and 287/300 who had a surgical procedure within seven days of injury. Of those 287 patients, 53 had at least one serious co-morbidity, leaving 234 potential Cethrin (cervical) patients.
The NOGO trial involved the intrathecal administration of the anti-Nogo antibody within 30 days of injury in AIS A cervical and thoracic SCI. When the NOGO study criteria were applied, 1147 patients had a SNL between C5 and T11, and 516 of those were AIS A. There were 495/516 who arrived at the acute RHSCIR site within 28 days of injury; 89 of those 495 patients had a serious co-morbidity, leaving 407 potential patients.
Last, the Sygen trial involved the intravenous administration of Sygen to patients with acute cervical and thoracic SCI within 72 h of admission (but only after the patients had been administered methylprednisolone). There were 1598 who met the SNL criteria for Sygen (C1–T9). The LEMS in one or both legs was ≤15 in 875/1598 patients. There were 440/875 patients who arrived at the RHSCIR acute site within 7 h of injury. At least one serious co-morbidity was present in 88 of the remaining patients, leaving 352.
Annual enrollment projections were generated for Minocycline, Riluzole, STASCIS, Cethrin, NOGO, and Sygen (117, 62, 109, 101 [54 in thoracolumbar, 47 in cervical], 82, and 70 respectively) (Table 2). Minocycline was projected to have the highest and Riluzole the lowest enrollment rates of 117 and 62 potential cases per year, respectively.
Estimated exclusion based on GCS score and consent status
GCS data were available for 1012 of the 2166 patients. Of these, 81 (8.0%) of patients had a GCS score of 12 or less at the RHSCIR facility.
Discussion
SCI is a devastating injury that contributes a significant burden of illness to individual patients and society. There is an imperative to identify therapeutic interventions that improve neurological recovery as well as those that may hinder it. To do so requires well-designed clinical trials; however, recruiting sufficient patients for these clinical trials can be challenging because of the low incidence of SCI, the frequent associated injuries and co-morbidities, and difficulties in accessing and enrolling acutely injured patients within narrow time intervals from the moment of injury. Multi-center initiatives provide an opportunity to enroll sufficient numbers of subjects for such trials and may provide a more representative and generalizable population for study, 16 lending robustness and greater validity to the study results.
Assessing the feasibility of recruiting an adequate sample size are critical elements of planning a successful clinical trial and have been ranked sixth and seventh, respectively, of 28 possible priority areas for clinical trial methodological research. 17 Nearly two-thirds of clinical trials do not meet their enrollment targets within their planned timeline. 18 Having fewer eligible participants than anticipated was understandably identified as the top reason for early participant recruitment problems. 18
Databases have been increasingly recognized in their usefulness for clinical trial planning. Studies using electronic medical record data, for instance, have shown that in half of the trials, they were able to predict whether the trial would have a low enrollment because of fewer than expected eligible patients before the start of the trial. 19 Maas and colleagues 20 have suggested that innovative study design planning and modeling can reduce the size of a trial by up to 50%.
Planning to execute acute SCI trials can be particularly challenging, because of the urgency with which enrollment must occur and the heterogeneity of injury severity and anatomical level of injury. 21 Because the pool of persons affected with SCI is relatively small and the infrastructure required to enroll subjects into time-sensitive clinical trials is not necessarily available at every center, there is a concern that enrollment in one study could negatively affect enrollment in other studies. 22 Detailed data and statistical modeling can facilitate efficient trial design during this planning phase.
We have applied the inclusion/exclusion criteria of six previously conducted SCI clinical trials to a prospectively collected Registry data set to examine the feasibility of running similar clinical trials in Canada. Significant variability was observed in the projected eligible population for the trials; for instance, Minocycline, with its broader study criteria (encompassing 27.0% of the RHSCIR cohort), was projected to encounter eligible subjects at nearly twice the rate of the Riluzole study, which has much narrower criteria (14.3%).
Per annum national study eligibility estimates for the trials based on RHSCIR data ranged from a mean of 62 participants per year (for Riluzole) to 117 participants per year (Minocycline). Thus, reaching the recruitment targets of 351 (for Riluzole) and 248 (Minocycline) would take 5.7 and 2.1 years, respectively, with recruitment in the RHSCIR network. These numbers, of course, assume that every RHSCIR facility across Canada would have the necessary personnel available to enroll patients with acute SCI on their arrival, that there would be no further exclusions, and all patients would consent to participate in these trials.
The number of eligible participants, however, is only one factor affecting successful trial completion. As a general rule, studies with broader criteria may require higher enrollment targets to detect clinically relevant effects because of variability in spontaneous neurologic recovery. To plan for this heterogeneity among patients with SCI, participants should be stratified in trials by both level of injury and motor score 21 ; RHSCIR can be used as a tool to achieve this. Because of its scope, RHSCIR could be used by future trials to perform a priori sample size calculations based on estimated effect sizes (extrapolated, to some extent, from previous interventional trials). The RHSCIR data set contains many of the data elements that would be required for these calculations, including detailed neurological information, timeline data, and co-morbidity data.
There are factors that are not or cannot be collected by the RHSCIR but that could impact enrollment, such as the cognitive status of the patient at the time of arrival, which may be impaired by drug intoxication or pharmacologic sedation and preclude a valid baseline neurological assessment. Blood alcohol levels are recorded by RHSCIR; however, there is substantial variability among sites with respect to testing rates as well as in the time elapsed before testing. In this study, we were not able to determine whether an individual patient might be unable to consent within the time frame of a particular study.
Other considerations that may affect enrollment that are not captured in RHSCIR include pregnancy, the likelihood that the patient would participate in follow-up, and actual willingness to participate in the study (although based on previous survey studies of individuals with SCI, their eagerness to participate in studies is generally high). 23 In the Sygen study, for instance, these elements accounted for 4.6% of screen failures. 24 Refusal to participate may be less of a factor in SCI trials than that observed in trials for other conditions, because there are such limited treatment options available outside of clinical trials, increasing the likelihood that patients will consent to a study. 18
Time from injury to acute care is often an important consideration for SCI trials, and although RHSCIR captures the time of arrival at the RHSCIR facility, the logistical capacity to screen, enroll, and administer drug/treatment under narrow time constraints (often within 12 h of injury) can vary significantly from site to site. In addition, while estimates of the proportion of individuals with a TBI were used in this study, patients on presentation to an emergency department frequently are also sedated/obtunded because of pharmacologic sedation and/or drug intoxication. Persons who are intubated in the trauma setting for airway control may also be difficult to examine and enroll into studies. These factors were not taken into account in this current analysis.
Further, internal factors such as staffing issues can also be a significant cause of delay in achieving enrollment targets. 18 It should be emphasized that the ability to enroll patients into an acute clinical trial requires a personnel infrastructure (e.g., study coordinators, research nurses, 24 h pharmacy access) that are not necessarily available at all centers.
There are also limitations within the existing data set. For instance, RHSCIR's co-morbidity data are comprehensive but not exhaustive. Trial exclusion criteria are often broader (i.e., significant pre-injury neurological deficits) while the co-morbidity data are more specific, and there may be a small subset of cases within our sample with co-morbidities substantive enough to exclude them from trials but not captured by the RHSCIR data set.
GCS data were missing for 53.3% of participants; 8.0% of those with GCS data would be excluded for major head injury as defined by GCS score. This number, however, was based on the entire analysis cohort, so it is possible that the prevalence of head injury was different among those who met the individual study criteria. Consent status was also not applied to each study criteria, because it is inappropriate to consider that consent rates for registry participation would be equivalent to consent for study purposes.
Centers may undergo the expense of taking on a trial, investing in appropriate training, staffing levels, and infrastructure, to then only enroll a small handful of patients. This reflects the reality of what occurs when attempting to enroll patients with specific inclusion/exclusion criteria. Clinical centers across Canada are diverse both geographically and demographically. A center located in a demographically older area may be better able to recruit for a trial for central cord syndrome, which disproportionately affects the elderly. A center with a smaller geographic catchment area with high population density may have a larger proportion of its patients who arrive within a few hours of injury. Selecting the most appropriate centers for a given trial may be facilitated using the Registry and may provide a unique opportunity to objectively assess a center's ability to participate and thus to optimize which centers are involved in which study.
Clinical trials are expensive undertakings that require tremendous effort from all involved. RHSCIR contains national, extensive data for SCI cases in Canada. This study suggests that a multi-center Canadian trial would be feasible and that national RHSCIR data may be helpful in a priori planning of such a trial.
Footnotes
Acknowledgments
The authors thank the Rick Hansen Spinal Cord Injury Registry Network and all of the participating sites: G.F. Strong Rehabilitation Centre, Vancouver General Hospital, Foothills Medical Centre, Glenrose Rehabilitation Hospital, Royal Alexandra Hospital, University of Alberta Hospital, Royal University Hospital, Saskatoon City Hospital, Winnipeg Health Sciences Centre, Toronto Western Hospital, Toronto Rehabilitation Institute, St. Michael's Hospital, Sunnybrook Health Sciences Centre, Hamilton General Hospital, Hamilton Health Sciences – Regional Rehabilitation Centre, Victoria Hospital, University Hospital, Parkwood Institute, The Ottawa Hospital Rehabilitation Centre, The Ottawa Hospital – Civic Campus, Hôpital de l'Enfant Jésus, Institut de réadaptation en déficience physique de Québec, Centré de réadaptation Lucie-Bruneau, Institut de réadaptation Gingras-Lindsay-de-Montréal, Hôpital du Sacré-Coeur de Montréal, Nova Scotia Rehabilitation Centre, QEII Health Sciences Centre, Saint John Regional Hospital, Stan Cassidy Centre for Rehabilitation, St. John's Health Sciences Centre, and Dr. Leonard A. Miller Rehabilitation Centre.
Author Disclosure Statement
No competing financial interests exist.