
Abstract
Cardiovascular disease is one of the leading causes of morbidity and mortality in the spinal cord injury (SCI) population. SCI may disrupt autonomic cardiovascular homeostasis, which can lead to persistent hypotension, irregular diurnal rhythmicity, and the development of autonomic dysreflexia (AD). There is currently no software available to perform automated detection and evaluation of cardiovascular autonomic dysfunction(s) such as those generated from 24 h ambulatory blood pressure monitoring (ABPM) recordings in the clinical setting. The objective of this study is to compare the efficacy of a novel 24 h ABPM Autonomic Dysfunction Detection Software against manual detection and to use the software to demonstrate the relationships between level of injury and the degree of autonomic cardiovascular impairment in a large cohort of individuals with SCI. A total of 46 individuals with cervical (group 1, n = 37) or high thoracic (group 2, n = 9) SCI participated in the study. Outcome measures included the frequency and severity of AD, frequency of hypotensive events, and diurnal variations in blood pressure and heart rate. There was good agreement between the software and manual detection of AD events (Bland–Altman limits of agreement = ±1.458 events). Cervical SCI presented with more frequent (p = 0.0043) and severe AD (p = 0.0343) than did high thoracic SCI. Cervical SCI exhibited higher systolic and diastolic blood pressure during the night and lower heart rate during the day than high thoracic SCI. In conclusion, our ABPM AD Detection Software was equally as effective in detecting the frequency and severity of AD and hypotensive events as manual detection, suggesting that this software can be used in the clinical setting to expedite ABPM analyses.
Introduction
S
Impaired autonomic BP control may subsequently lead to irregular diurnal BP variations, chronic hypotension, orthostatic hypotension (OH), and autonomic dysreflexia (AD). 3,4 AD is a potentially life-threatening condition characterized by extreme hypertensive events in which systolic BP (SBP) can rise as high as 300 mm Hg. 5 AD is caused by noxious and non-noxious visceral or somatic stimuli such as bladder and bowel distension. 6 Loss of descending tonic inhibitory drive to the sympathetic preganglionic neurons is one of the major mechanisms responsible for the development of AD. If left untreated, episodes of AD may result in seizures, 7 myocardial infarction, 8 stroke, 9,10 and even death. 11
Changes in diurnal variations in BP post-SCI have been characterized by the presence or absence of a nocturnal dip, whereby there is little to no change in BP between day and night in individuals with cervical SCI. 12 Diminished or absence of a nocturnal dip is considered one of the most sensitive predictors of stroke, congestive heart failure, and cardiovascular morbidity in able-bodied subjects. 13 –15 Further to altered diurnal rhythmicity, injury above T6 may result in reduced sympathetic activity in the splanchnic vascular bed and lower limb blood vessels, which hat may culminate in decreased systemic vascular tone, 16,17 chronic hypotension, 18 and OH. 19 OH is characterized by a decrease in systolic BP by 20 mm Hg or a decrease in diastolic BP by10 mm Hg. 20 Symptoms of OH include blurred vision, fatigue or weakness, light headedness, and dizziness. 21
We and others have developed novel algorithms and software to characterize spontaneous AD from continuous arterial BP in rats using telemetry. 22,23 There are, however, no clinically validated algorithms that can be applied to 24 h ambulatory BP monitoring (ABPM) data. Presently, these data are analyzed in a highly laborious fashion, and none of the available approaches are able to accurately detect concomitant changes in both BP and heart rate (HR), which is critical given that AD is defined by changes in both BP and HR. 6 The development of automated BP and HR analysis software would allow for the expedited detection of spontaneous occurring AD, hypotensive events, and assessment of diurnal rhythmicity without subjective error. Such software, if employed universally, would also allow for easier comparisons across laboratories and would assist in amalgamating data sets to circumvent the inherent limitation of small sample sizes in SCI research. Moreover, with the advent of personalized medicine, the ability to rapidly assess such indices on an individualized basis is likely to become ever more important.
The goal of the study, therefore, is to validate a novel ABPM Autonomic Dysfunction Detection Software that we have developed. A secondary goal was to use the software to characterize spontaneous AD, hypotensive events, and diurnal BP rhythms based on the neurological level of injury in individuals with SCI at or above the sixth thoracic spinal cord segment.
Methods
Subject demographics and SCI assessment
Eligible individuals were recruited from both inpatient and outpatient programs in Vancouver, British Columbia, Canada. Inclusion criteria include a SCI higher than and including the sixth thoracic segment with American Spinal Injury Association (ASIA) Impairment Scale (AIS) of A to B. Forty-six individuals with SCI (7 females, 39 males; mean age of 43 ± 12; level of SCI = C3-T6; SCI duration = 1 month to 30 years; AIS = A-B; 5 inpatients and 41 outpatients; 9 paraplegics and 37 tetraplegics) participated in the study. The neurological level and severity of SCI was determined using the International Standards of Neurological Classification of SCI. 24 Exclusion criteria included age of <18 years, history and symptoms of cardiovascular or pulmonary obstructive disease, unstable psychiatric condition or substance abuse disorder, or any cognitive dysfunction. Four of the included participants were regularly taking BP medication (midodrine). All procedures were granted ethics approval by the University of British Columbia, and all eligible individuals gave informed, written consent prior to participation.
Study protocol
This study has two parts: 1) To assess the validity of a novel 24 h ABPM Autonomic Dysfunction Detection Software developed in-house, and 2) to use ABPM Autonomic Dysfunction Detection Software to assess how the neurological level of injury relates to the frequency and severity of AD, the frequency of hypotensive events, and diurnal rhythmicity post-SCI.
In the first part of the study, we validated the ABPM Autonomic Dysfunction Detection Software's capacity to detect the frequency and severity of AD and hypotensive events and diurnal rhythms from 24 h ABPM profiles by comparing it to an unautomated (i.e., human visual) approach. We assessed agreement between the automated and unautomated methods with respect to the number of AD and hypotensive events from all 46 ABPM profiles. The unautomated analysis was performed by a cardiovascular physiologist with knowledge and expertise in BP assessments post-SCI (C.R.W.), whereas the automated analysis using the ABPM AD Detection Software was performed by an additional, blinded investigator (D.W.P.).
The second part of this study assessed the severity and frequency of AD events, frequency of hypotensive events, and diurnal BP rhythms between cervical and high thoracic SCI individuals using the ABPM Autonomic Dysfunction Detection Software described. We separated participants into two groups: cervical SCI (above and including the eighth cervical spinal cord segment, n = 37) and high thoracic SCI (above and including the sixth thoracic spinal cord segment, n = 9).
ABPM monitoring
Twenty-four hour ABPM was performed using the Meditech Card(X)plore device (Meditech, Budapest, Hungary). An appropriate cuff size was secured to the nondominant arm, and measurements of SBP, diastolic BP (DBP) and HR were recorded automatically every 15 min from 0800 to 1900 h, and every hour between 1900 and 0800 h. Participants with a scheduled bowel routine within the 24 h monitoring period took self-initiated measurements at 5 min intervals before, during, and after their bowel routine. Patients were also asked to take self-measurements if they experienced symptoms or completed any activity that could trigger a hypertensive or hypotensive event. Notes about their BP related symptoms, activities, and sleep schedules were recorded in a diary. Patients were given oral and written instructions to ensure that ABPM devices were worn correctly to maintain accurate hemodynamic measurements. No individuals reported any sleep disturbances caused by the ABPM device. Data were stored on a secure digital (SD) memory card and were extracted for data analyses. To validate our software, data were visualized using CardioVisions 1.13.0 software (MediTech) and extracted to an Excel file (.xlsx file) which was subsequently analyzed using our ABPM Autonomic Dysfunction Detection Software (see next section).
ABPM AD Detection Software
A novel ABPM AD Detection Software (JAVA platform) was developed and utilized to assess hemodynamic variations in ambulatory BP data in the clinical setting. The software is able to assess the frequency of AD and hypotensive events, in addition to characterizing diurnal rhythms in SBP, DBP, and HR. Using the software, one can modify restrictions associated with the detection of AD events, including modifying the threshold associated with detecting the spike in SBP/DBP, as well as the “bounds” associated with the HR response to the AD event. The software also automatically separates AD events based on whether the spikes in SBP are accompanied by bradycardia, tachycardia, or no HR response. Finally, the software also characterizes the number of times SBP and DBP fall below a customized cutoff. A visual representation of the 24 h ABPM profile is presented by the software (Fig. 1), and the detected AD and hypotensive events are also highlighted. Lastly, the software extracts hour-by-hour averages of hemodynamic data (i.e., SBP, DBP, and HR). The presently available software of the commercial device (i.e., the unautomated method) that was used in our study has the capacity to build a diagram of the BP and HR changes during the 24 h ABPM monitoring period. This method, however, is unable to detect AD events, which is how the presently described automated software is advantageous. Without the automated software, the medical professional would be required to review the recording visually and examine a corresponding Excel spreadsheet of all hemodynamic indices to detect AD and hypotensive events.

Example of 24 h ambulatory blood pressure monitoring (ABPM) software profile output from
Data analysis
Three baseline SBP, DBP, and HR measurements were collected and averaged from Meditech Card(X)plore ABPM devices when participants were in a seated position, and a further three were collected and averaged when participants were in a supine position. The supine average was used for nighttime analyses (2300–0559) and the seated average for the daytime analyses (0600–2259). AD events were defined as an increase in SBP ≥20 mm Hg above baseline SBP. AD events with bradycardia had a corresponding drop in HR ≥10 bpm below baseline. Hypotensive events were defined as a drop in SBP ≥20 mm Hg and/or DBP ≥10 mm Hg below their respective baseline BPs.
Statistical analysis
For the first part of the study, the level of agreement between the ABPM Autonomic Dysfunction Detection Software and manual method was performed using the Bland–Altman method on GraphPad v5.0 (GraphPad Software, San Deigo, CA). For the second part of the study, data were tested for normality using the Kolmogrov and Smirnov assumptions. Further, independent samples t tests with equal variances were performed using STATA v12.0 (StataCorp LP, College Station, TX) to assess lesion level differences between the frequency and severity of detected AD events and the frequency of hypotensive events. Two way analyses of variance (ANOVA) with Bonferroni corrected post-hoc comparisons were used to assess the effect of lesion level on diurnal rhythmicity of SBP, DBP, and HR.
Results
Validation of ABPM AD detection software
Little bias was found between both methods for AD and hypotensive event detection (0 and 0.0412, respectively; Fig. 2). The 95% limits of agreement between the two methods for AD event detection are −1.458 and 1.458. The limits of agreement between the two methods for hypotensive event detection are −1.168 and 1.252.
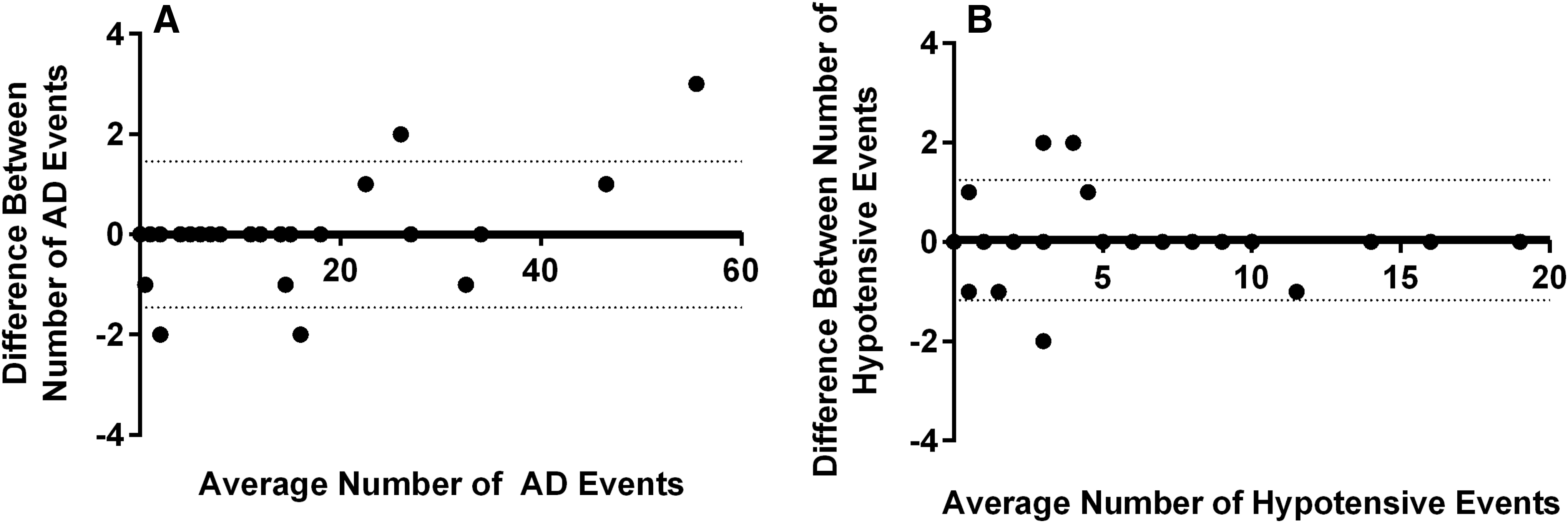
Bland–Altman plots demonstrating good agreement between the ambulatory blood pressure monitoring (ABPM) Autonomic Dysfunction Detection Software and unautomated analysis of ABPM profiles for autonomic dysreflexia (AD)
Effect of level of SCI on AD and hypotensive events
The cervical SCI group experienced an increased frequency of spontaneous AD events with (p = 0.0264) or without (p = 0.0043) accompanying bradycardia compared with the high thoracic SCI group (Fig. 3). Additionally, cervical SCI individuals exhibited AD events with a greater maximum pressor response (i.e., ΔSBP relative to baseline) (p = 0.0343) and maximum SBP compared with high thoracic SCI individuals (p = 0.0343). The HR drop associated with an AD event in the cervical SCI group was higher than in the high thoracic SCI group (p = 0.0468). Further, the minimum HR during the detected AD events were lower in the cervical SCI group than in the high thoracic SCI group (p = 0.0203). There were no significant differences in the frequency of hypotensive events detected in the cervical and high thoracic SCI groups (Fig. 4).
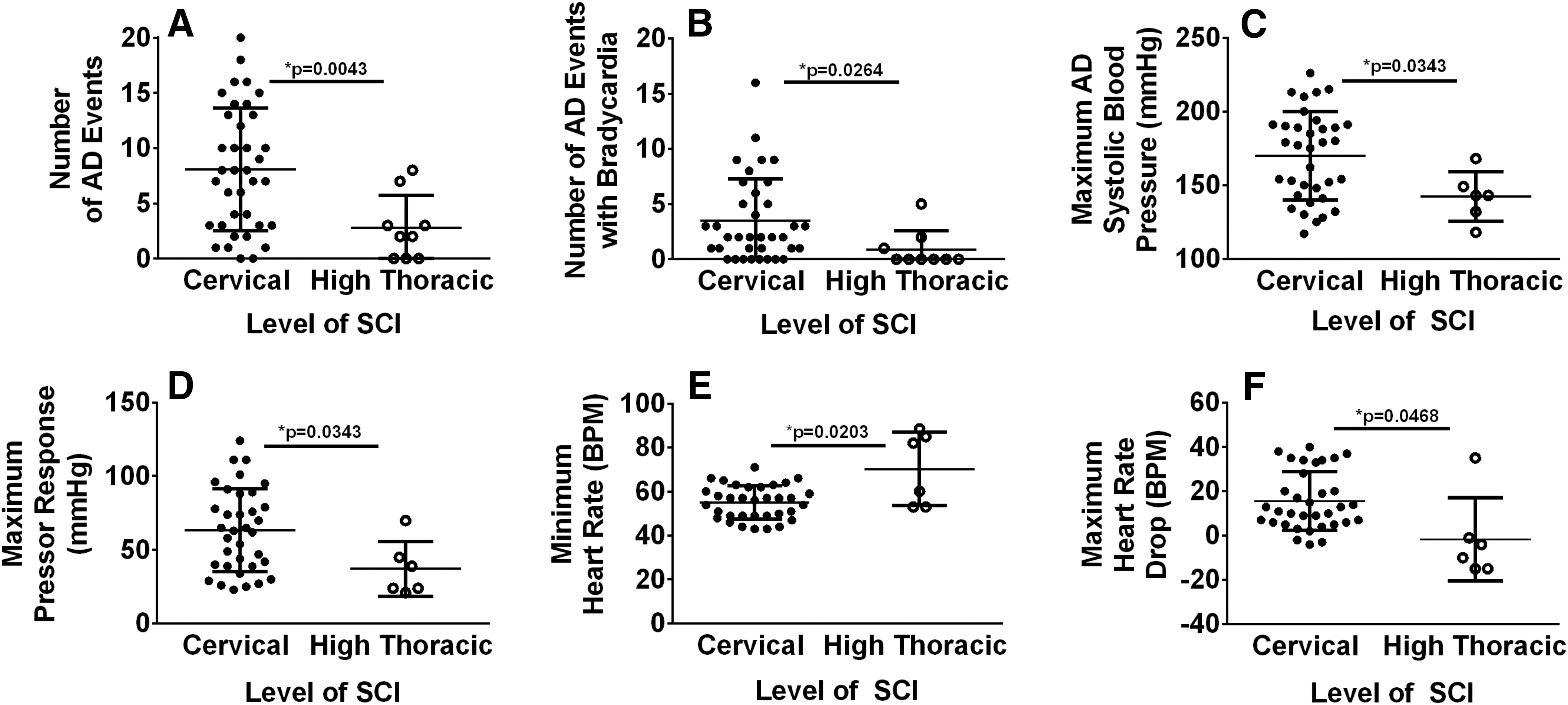
Cervical spinal cord injury (SCI) individuals exhibit more frequent and severe autonomic dysreflexia (AD) than high thoracic SCI individuals. Group mean ± SD of indices derived from ambulatory blood pressure monitoring (ABPM) during AD. Cervical SCI individuals exhibit more frequent AD with or without accompanying bradycardia than high thoracic SCI individuals (
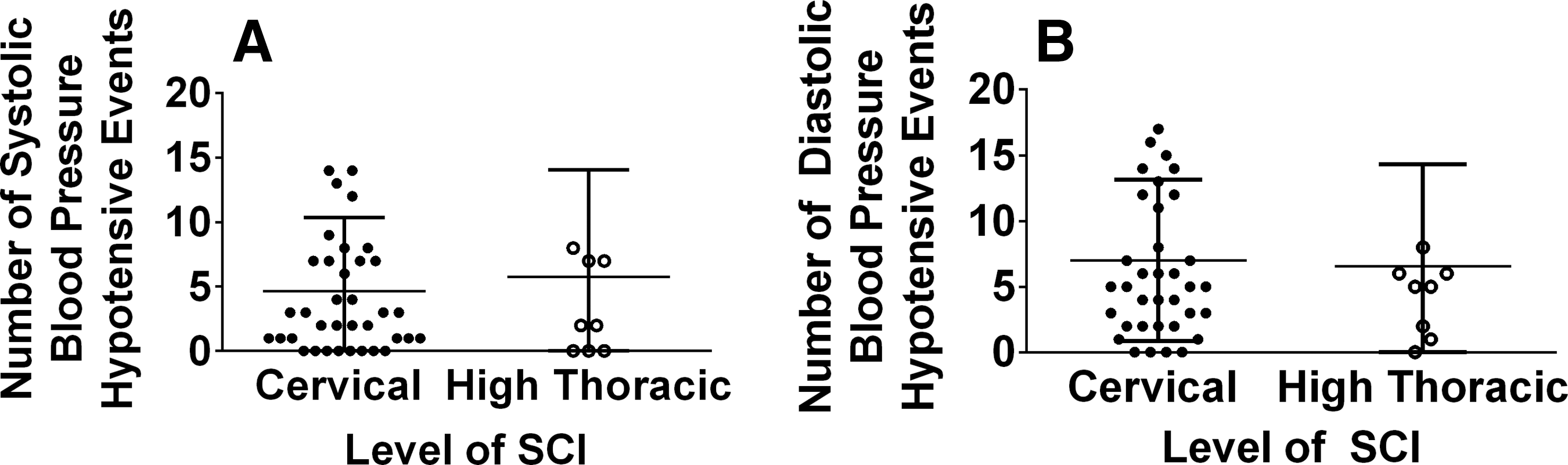
There are no significant differences in the number of hypotensive events detected in the cervical and high thoracic SCI groups. Group mean ± SD of hypotensive events detected using systolic blood pressure
Most common reported causes of AD
Approximately 59% of detected AD events were not reported, meaning that the study participant did not make any comments at the time of the BP measurement. The most frequently reported comment during the monitoring period that was associated with an AD event was related to bladder management (voiding, catheterization, or kink in catheter; 11% of AD events, with an average maximum pressor response of 49 mm Hg and average maximum SBP of 152 mm Hg) and bowel routine (11% of AD events with average maximum pressor response of 52 mm Hg and average maximum SBP of 163 mm Hg). This is followed by AD events reported during transfer or repositioning (9% of AD events with average maximum pressor response of 46 mm Hg and average maximum SBP of 156 mm Hg) and AD events associated with a spasm (5% of AD events with an average maximum pressor response of 53 mm Hg and an average maximum SBP of 162 mm Hg). Intermittent catheterization was the most common method (54%) of bladder management in our study, followed by Foley or suprapubic catheterization (26%), and condom catheterization (20%).
Effect of level of SCI on diurnal variations
There was a significant drop in SBP and DBP in the high thoracic SCI group at every hour from 0100 to 0500 h compared with the cervical SCI group (all p < 0.05) (Fig. 5). There was also a significant increase in HR at 0100–1300 h, 1300–1600 h, and 1900 h for the high thoracic SCI group (p < 0.05).

Individuals with cervical SCI exhibit impaired diurnal rhythmicity compared with high thoracic SCI individuals. Diurnal variations in systolic blood pressure
Discussion
We have developed a novel automated ABPM Autonomic Dysfunction Detection Software that is able to characterize the severity of cardiovascular autonomic dysfunction post SCI (i.e., hemodynamic diurnal rhythmicity, frequency and severity of AD, and hypotensive events) as effectively as unautomated characterization. Using our newly validated software, we have also illustrated that individuals with cervical SCI had an increased propensity for spontaneous AD with a substantially more pronounced pressor response and HR drop compared with individuals with high thoracic SCI. We also observed that the cervical and high thoracic SCI groups showed no significant differences in the number of hypotensive events.
Validation of ABPM AD Detection Analysis Software
We have developed a software with no significant bias relative to unautomated (manual) assessment that may be used in the clinical setting to detect the onset and severity of spontaneous AD and hypotensive events in an expedited fashion. In addition, the software assesses diurnal rhythmicity in hemodynamics, which in turn can be used to assess the presence or absence of a nocturnal dip. For the present study, the cutoff used for AD detection was transposed vertically 20 mm Hg above baseline, as per the clinical definition; 6 however, users of the software may modify the bounds associated with the detection of the AD pressor response to suit their specific needs. This is the first software to our knowledge that also measures simultaneous HR responses. In the present study, we used this function to confirm the change in HR (i.e., bradycardia) upon the onset of AD. The software provides the user full functionality to modify the criteria associated with the detection of spontaneous AD by creating bounds for the associated HR change during AD. For the present study, we presented AD data both with and without bradycardia, because some previous studies have shown the absence of bradycardia upon onset of AD. 6,25,26
There is currently no other software available to detect spontaneous AD events from 24 h ABPM profiles. There is software available that may be used to assess hypertensive and hypotensive events relative to a baseline, but none of the software currently available is able to concurrently assess the unique baroreceptor mediated HR response to these reflexive spikes in SBP associated with AD. The baroreceptor mediated HR drop upon onset of the pressor response of spontaneous AD is unique to cardiovascular autonomic dysfunction post-cervical/high thoracic/ SCI. Nevertheless, our software may be applied to other conditions associated with autonomic dysregulation of hemodynamics such as non-SCI OH and postural orthostatic tachycardia syndrome, which is characterized by an increase in HR and increase in BP upon assumption of the upright posture caused by sympathetic overactivity. 27 The software may be also applied to other disease states in which the symptoms associated with the diagnosis are accompanied with a characteristic HR and BP response that is a hallmark of the condition. For example, ventricular tachycardia and renal failure are associated with onset of tachycardia and HR arrhythmia, which is found in combination with hypotension. This software may also be applied to a variety of cardiovascular autonomic neuropathies (most commonly diabetes) such as that brought on by damage to the autonomic innervation of the heart and blood vessels resulting in impaired heart rate rhythms and vascular dynamics. 28 Diabetic patients with cardiovascular autonomic neuropathies are prone to postural hypotension and silent ischemia. 29
Cervical SCI individuals experience an increased frequency and severity of spontaneous AD events compared with high thoracic SCI individuals
Using our ABPM AD Detection Software, we report, in a large cohort of individuals with SCI, that cervical SCI exhibited an increased propensity for spontaneous AD events compared with high thoracic SCI. This corroborates previous findings from our laboratory that tetraplegic individuals are prone to more frequent AD then paraplegic individuals. 26 We are also the first to show increased severity of AD and a greater baroreceptor mediated HR drop in cervical SCI individuals in comparison with high thoracic SCI individuals. The increased frequency and severity of spontaneous AD with a more cranial level of injury may be the result of the greater loss of supraspinal input from cardiovascular control centers to spinal sympathetic circuitry. 4 These differences may, however, also be the result of the specific level of injury-dependent changes in sympathetic preganglionic neurons and interneurons, along with aberrant sprouting of dorsal root afferent fibers, 30 –32 and/or differential changes in the sensitivity of α-adrenergic receptors. 33,34
The most common underlying causes of AD in the study were bladder management program and bowel routine, which is in agreement with previous studies that have investigated underlying causes of AD. 6,16 The most severe AD events occurred during the bowel routine, when SBP reached a maximum of 195 mm Hg and a corresponding pressor response of 88 mm Hg. Of the four individuals who were taking midodrine, one individual did not exhibit any AD events and the other three individuals exhibited a similar number of AD events to those not taking midodrine. Importantly, however, the pressor response during AD and the maximum SBP was elevated in those taking midodrine compared with those not taking midodrine. A comparison of AD severity between individuals who are taking midodrine and those who are not would be an interesting future area of study. Clinically, midodrine is often prescribed to help maintain basal arterial BP and mitigate OH; however, a potential consequence is that the maximum pressor response during AD is elevated. For this reason, individuals with SCI are recommended not to take midodrine prior to or during a bowel routine.
There are no differences between cervical and high thoracic SCI individuals in the frequency of hypotensive events
That we found no differences in the number of hypotensive events between high thoracic and cervical SCI is likely a consequence of the sympathetic innervation provided by the T1-T6 sympathetic preganglionic neurons. These neurons provide sympathetic modulation of vascular tone to the upper body. Conversely, the T6-L2 sympathetic preganglionic neurons mediate sympathetic innervation of the major vasculature beds within the splanchnic circulation and the lower extremities. The splanchnic circulation is considered one of the foremost important influences in cardiovascular control, because it stores approximately one fourth of the total blood volume and is considered the primary capacitance bed in the human body. Therefore, high thoracic and cervical SCI may result in a similar degree of hypotension, as both exhibit the loss of vascular tone in resistance vasculature within the splanchnic bed. 16
Cervical SCI individuals present with impaired hemodynamic diurnal rhythmicity compared with high thoracic SCI individuals
Cervical SCI individuals presented with impaired hemodynamic diurnal rhythmicity compared with high thoracic SCI individuals. Specifically, high thoracic SCI individuals had significantly lower SBP during the nighttime compared with cervical SCI individuals, which implies that high thoracic SCI presents with a nocturnal dip and that cervical SCI does not. This finding corroborates previous findings that tetraplegic individuals lose retention of their nocturnal dip compared with high thoracic SCI (T2-T5) individuals. 12 Complete lesions of the cervical spinal cord have an absence of nighttime melatonin, which demonstrates that the neural pathway for the endogenous production of melatonin passes through the cervical spinal cord segment. 35 Exogenous production of melatonin can shorten sleep onset, improve sleep maintenance, and increase rapid eye movement sleep. 36 –38 Disruption of endogenous melatonin production may play an imperative role in the disruption of normal sleep patterns and subsequently circadian rhythms in BP and HR in cervical SCI individuals. In addition, the lower HR during the day for the cervical SCI group could be attributed to loss of sympathetic innervation to the heart from the T1-T5 spinal cord segments. The lack of sympathetic mediated HR increase throughout the day for the cervical SCI group corroborates previous studies that have shown loss of circadian HR rhythms in tetraplegic individuals. 39,40
Considerations
We believe that our newly developed ABPM Autonomic Dysfunction Detection Software that automatically assesses hemodynamic function from 24 h ABPM is more advantageous than the unautomated analysis approach because of the expedited, less time laborious nature of the software. We also believe that our program is more advantageous than other programs because in addition to detecting AD and hypotensive events, we can also assess the baroreceptor-mediated HR responses to detected fluctuations in BP. We suggest, therefore, that our program should be used in the routine autonomic/cardiovascular assessment when 24 h hemodynamic monitoring is indicated. By using our new software alongside established clinical questionnaires such as the Autonomic Dysfunction Following Spinal Cord Injury (ADFSCI) questionnaire, the clinician/researcher is able to more fully and quantitatively assess AD and OH pathology development. 26
Conclusion
Twenty-four hour ABPM in conjunction with our novel ABPM Autonomic Dysfunction Detection Analysis Software may have applications in the diagnosis and treatment of autonomic cardiovascular dysfunction post-SCI. Cervical SCI individuals have an increased propensity for more frequent and severe spontaneous AD than high thoracic SCI individuals. There were no significant differences in the number of hypotensive events detected between cervical and high thoracic SCI individuals. Further, we show that cervical SCI individuals present with impaired hemodynamic diurnal rhythmicity when compared with high thoracic SCI individuals.
Footnotes
Acknowledgments
This work was supported by the Canadian Institutes of Health Research.
Author Disclosure Statement
No competing financial interests exist.