
Abstract
Traumatic brain injury and hemorrhagic shock is associated with blood–brain barrier (BBB) breakdown and edema formation. Recent animal studies have shown that fresh frozen plasma (FFP) resuscitation reduces brain swelling and improves endothelial function compared to isotonic NaCl (NS). The aim of this study was to investigate whether pooled and pathogen-reduced plasma (OctaplasLG® [OCTA]; Octapharma, Stockholm, Sweden) was comparable to FFP with regard to effects on brain water content, BBB permeability, and plasma biomarkers of endothelial glycocalyx shedding and cell damage. After fluid percussion brain injury, hemorrhage (20 mL/kg), and 90-min shock, 48 male Sprague-Dawley rats were randomized to resuscitation with OCTA, FFP, or NS (n = 16/group). Brain water content (wet/dry weight) and BBB permeability (transfer constant for 51Cr-EDTA) were measured at 24 h. Plasma osmolality, oncotic pressure, and biomarkers of systemic glycocalyx shedding (syndecan-1) and cell damage (histone-complexed DNA) were measured at 0 and 23 h. At 24 h, brain water content was 80.44 ± 0.39%, 80.82 ± 0.82%, and 81.15 ± 0.86% in the OCTA, FFP, and NS groups (lower in OCTA vs. NS; p = 0.026), with no difference in BBB permeability. Plasma osmolality and oncotic pressures were highest in FFP and OCTA resuscitated, and osmolality was further highest in OCTA versus FFP (p = 0.027). In addition, syndecan-1 was highest in FFP and OCTA resuscitated (p = 0.010). These results suggest that pooled solvent-detergent (SD)-treated plasma attenuates the post-traumatic increase in brain water content, and that this effect may, in part, be explained by a high crystalloid and colloid osmotic pressure in SD-treated plasma.
Introduction
T
The aim of the present study was to investigate the effects of SD-treated plasma (OctaplasLG® [OCTA]; Octapharma, Stockholm, Sweden), FFP, and 0.9% NaCl in a rat model of fluid percussion brain injury (FPI) and HS. Primary outcome was brain water content at 24 h post-trauma, and secondary outcomes were BBB permeability to 51-chromium-labeled ethylenediamine tetra-acetic acid (51Cr-EDTA), plasma colloid osmotic pressure, plasma osmolality, and plasma biomarkers of glycocalyx shedding (syndecan-1) and cellular damage (histone-complexed DNA [hcDNA] fragments) measured at 23-24 h post-trauma.
Resuscitation volumes were chosen with the objective to result in similar plasma volume expansion to separate volume-expanding effects from other pharmacodynamic properties of the respective fluids. 3,18,19
Methods
Study design
An overview of the experiment is presented in Figures 1 and 2. The study was approved by the Ethics Committee for Animal Research of Lund University (M61-12; Lund, Sweden). Male Sprague-Dawley rats (Taconic Biosciences, Inc., Ejby, Denmark), treated in accord with the Guide for the Care and Use of Laboratory Animals of the National Academy of Science (AAALAC International, Frederick, MD), were used. Surgical preparation was performed as described previously. 3 Briefly, anesthesia was induced with injection of sodium pentobarbital (60 mg/kg) intraperitoneally (Apoteket AB, Stockholm, Sweden) and maintained with isoflurane (0.6–1.5%) through a nose mask (Schering-Plough, Farum, Denmark). Rectal temperature was kept constant at 37°C. The right internal jugular vein was cannulated for transfusion and the left femoral artery for measurement of mean arterial pressure (MAP) and blood sampling. MAP was expressed as the mean of 5 min before and after each measurement point. The cranium was fixed in a stereotactic frame to conduct a 5-mm left-sided parietal craniotomy, which was connected to a plastic luer-lock device with Histoacryl (Braun, Tuttingen, Germany) and further with dental cement (Dentalon Plus; Heraeus Kulzer GmbH, Hanau, Germany) and a screw in the frontal bone to the cranium. After 90 min of preparation, animals received a standardized fluid percussion brain injury (FPI) of approximately 2.3 atmospheres (atm) (time point indicated as 0 h) and were bled 20 mL/kg and left in shock for 90 min. After shock, animals were resuscitated with either OCTA or FFP at a dose of 1.25 times or NS at 4.5 times the shed blood volume with the objective to result in equal plasma volume expansion. 3,18,19

Experimental protocol. Time point “0h” indicates the time of fluid percussion brain injury (FPI). Post-FPI, animals were left to rest for up to 10 min before bleeding. ABG, arterial blood gas; FPI, fluid percussion brain injury; PV, plasma volume; hcDNA, histone-complexed DNA; BWC, brain water content, Ki, BBB permeability to 51-chromium-labeled ethylenediamine tetra-acetic acid.
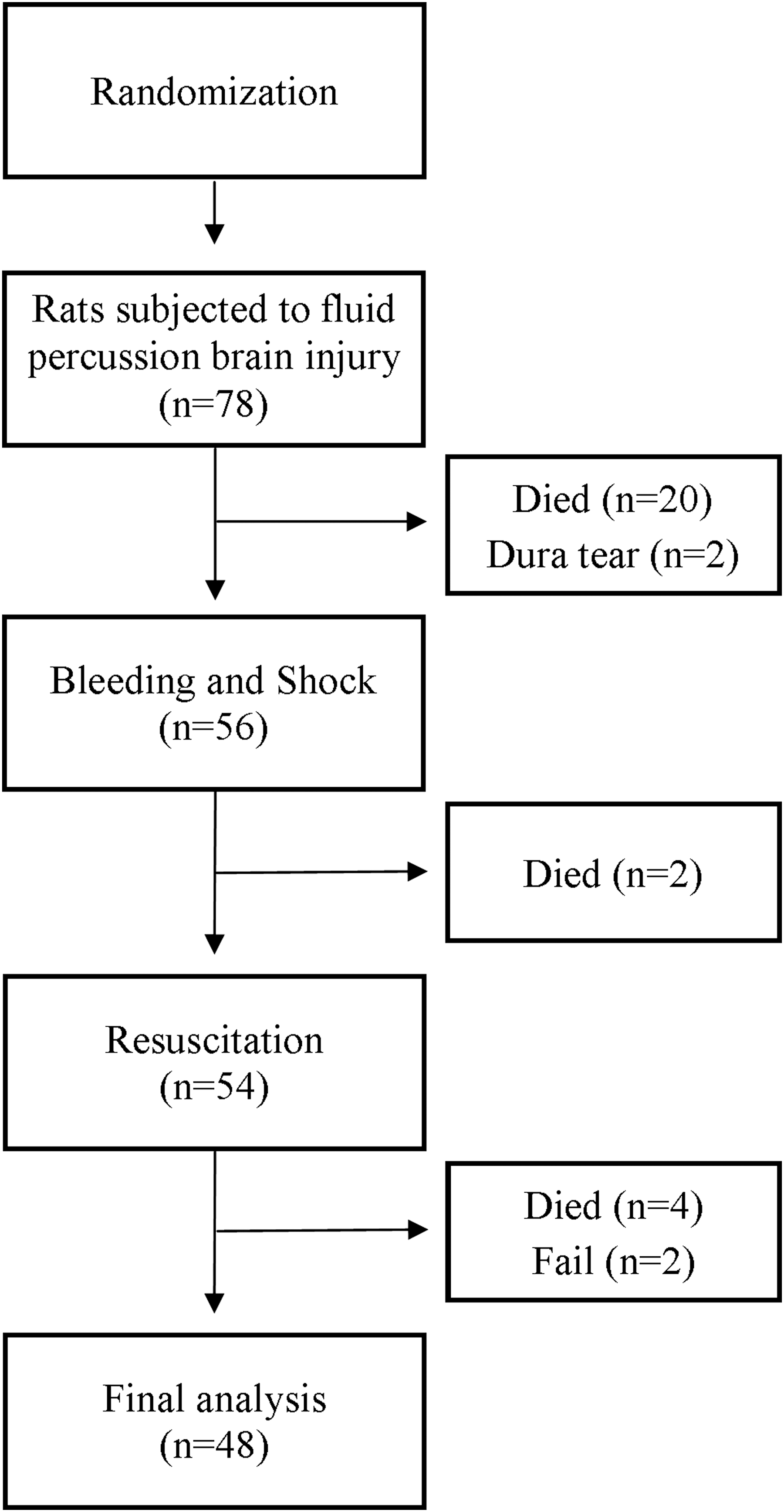
Consort-scheme of animals included in the study. Fail = no edema measurement because of technical problems.
After 30-min observation, animals were allowed to wake up with free access to food and water. At 22 h, animals were reanesthetized with isoflurane in a closed chamber followed by tracheostomy and mechanical ventilation (Ugo Basile Animal Ventilators, Comerio, Italy) to an end-tidal CO2 between 4.5 and 6.5 kPa, using VC-mode and PEEP of 3 mm of H2O and decapitated at 24 h after the final measurements.
Measurement of brain water content and blood–brain barrier permeability
Brain water content and BBB permeability was investigated as described previously.
3
Briefly, animals were decapitated at 24 h and a 4-mm-thick coronal section of the injured and uninjured hemisphere was rapidly collected on a chilled support (Fig. 3). Tissue samples were weighed (CP 225D; Sartorius AG, Göttingen, Germany), and water content was calculated after drying the samples at 100°C for 24 h: brain water content = [(wet weight – dry weight) / wet weight] * 100. BBB permeability was investigated by measuring the blood-to-brain transfer constant (Ki) for 51Cr-EDTA (Nycomed Amersham, Stockholm, Sweden) using an intravenous bolus and constant infusion 40 min before decapitation. Blood samples were obtained at 5-min intervals to determine the plasma activity of 51Cr-EDTA and measured together with brain tissue activity in a gamma counter (1480 Wizard; Wallace Sweden AB, Sollentuna, Sweden). Cortical uptake of 51Cr-EDTA was then calculated as brain tissue activity minus tissue plasma activity using a standardized intracerebral plasma volume of 0.01 mL/g.
20
Ki for 51Cr-EDTA was then calculated according to the following formula:
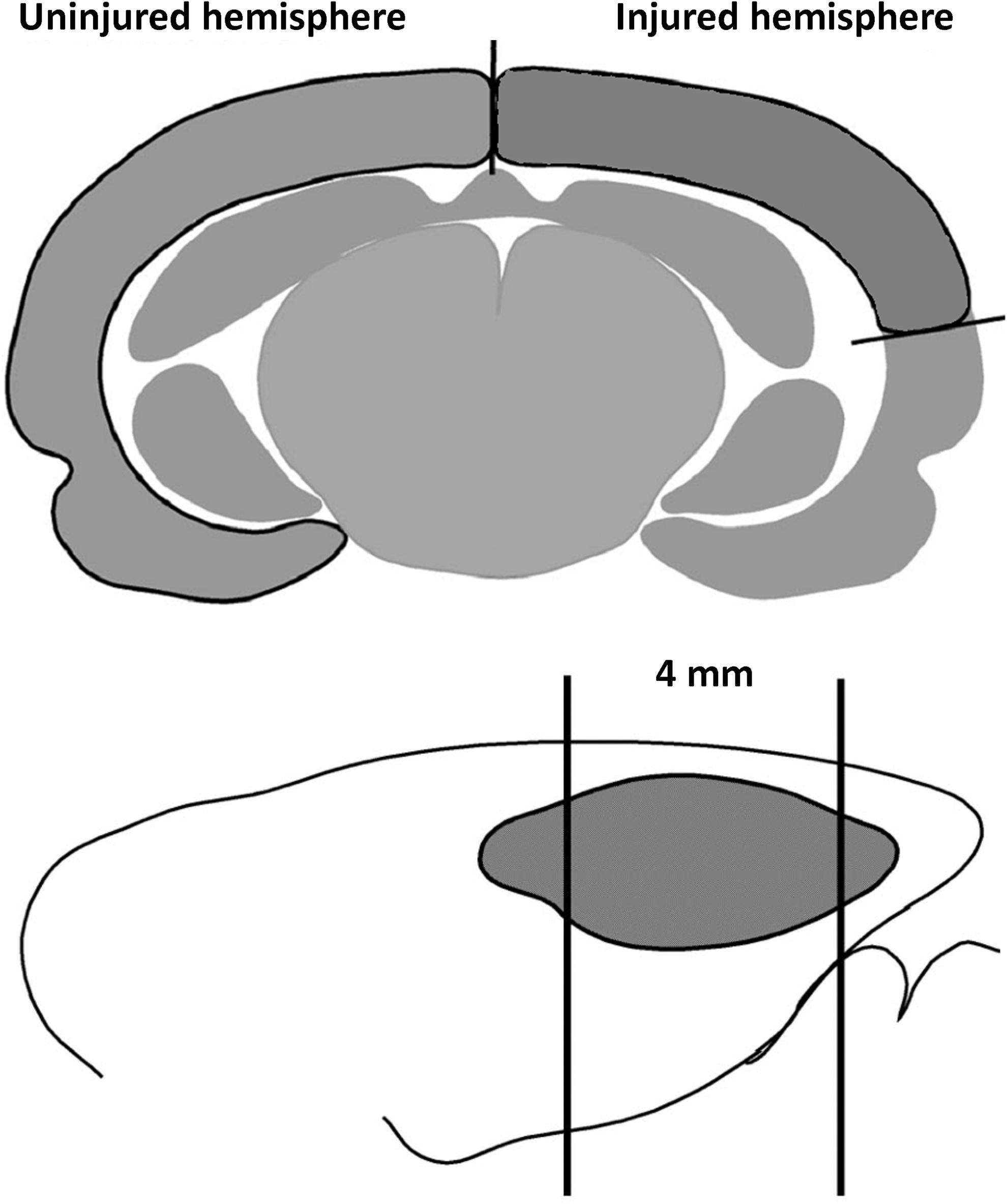
Coronal (top) and sagittal (bottom) view of the brain parts used for brain water content and blood–brain barrier permeability measurements.
where B is the amount of tracer in the tissue, Ca is the concentration of the tracer in arterial plasma as a function of time, and T is the duration of the experiment. Tracer uptake has been found to be independent of plasma flow during this experimental condition. 4
Oncotic pressure, osmolality, and plasma volume
Oncotic pressure, osmolality, and plasma volume were measured at 0 h and 23 h. Oncotic pressure was analyzed with a 10-kDa cut-off membrane (Osmomat 050; Gonotec, Berlin, Germany) and osmolality with the freeze-point method (Micro-Osmometer Model 210; Fiske Associates, Norwood, MA). Plasma volume was determined by measuring the plasma concentration of 125I-albumin (Department of Radiation Physics, Skåne University Hospital, Lund, Sweden) after injection of a known amount of the tracer. 3 Before injection, the tracer was purified from free iodine by centrifugal filtration (Microcon 30 filters; Millipore, Bedford, MA), and percentages of free iodine were found to be 1.31 ± 0.15% with no intergroup difference.
Arterial blood gas and glucose analysis
Arterial blood gas (ABG) analysis (i-STAT; Abbot Scandinavia AB, Stockholm, Sweden: Hct, lactate, Na+, Base Excess, K+, HCO3 −, pCO2, and pO2) was conducted at 0 h, end of shock period, completion of resuscitation and at 23 h, together with glucose measurements (Glucosure; HaeMedic AB, ka-Ljungby, Sweden).
Fluid compositions
SD-treated plasma (OctaplasLG; Octapharma) was produced from human European AB plasma, pooled with other 630 apheresis units or 1520 recovered units, totaling 380 liters of pooled plasma treated with the solvent detergent method and a chromatographic step for binding of prion proteins (PrPSc) and stored at −80°C in 200-mL bags. 17 Glycine was further added (C2H5NO2, molecular weight of 75.07 g/mol) as a stabilizer that gives a high osmolality. FFP was isolated from human Danish AB RhD negative donors and frozen within 6 h of collection at −80°C in 270-mL bags. Two batches of OCTA and FFP bags were initially thawed and separated into 20-mL plastic tubes and kept at −20°C before use. On the day of use, OCTA and FFP plastic tubes were thawed in a heated water bath at 37°C and subsequently kept at room temperature for up to 20 min before administration. NS (0.9% NaCl; B. Braun Medical A/S, Frederiksberg, Denmark; osmolality measured at our laboratory to be 283.3 ± 5.4 mOsm/kg) was stored at room temperature and administered at room temperature. Analysis of plasma chemistry was done at the Department of Biochemistry at Rigshospitalet (Copenhagen, Denmark).
Biomarker analysis (enzyme-linked immunosorbent assay)
Blood sampling for biomarker analysis was sampled in EDTA anticoagulation tubes at 0 and 23 h, double spun at 1000g for 12 min, and stored at −80°C. Analyses of biomarkers were performed with commercially available immunoassays; syndecan-1 (SEB966Ra; USCN Life Sciences Inc., Wuhan, China) and hcDNA fragments (Cell Death Detection ELISA PLUS; Roche, Hvidovre, Denmark). Syndecan-1 is one of the major proteoglycans of the endothelial glycocalyx. Plasma hcDNA fragments (kit contains antibodies specific for histones H1, H2A, H2B, H3, and H4 and single- and double-stranded DNA) are released from death and injured cells. Syndecan-1 is reported as ng/mL and hcDNA as %, calculated by dividing a fixed amount of control material with the samples.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows (version 22.0; IBM Corp., Armonk, NY), and data are presented as means ± standard deviation with p values <0.05 considered significant. Sample-size calculations based on brain water content were based on a standard deviation of 1.0. 3 To detect a 1.0% difference, with a power of 80% and α of 0.05, it was calculated that 16 animals were required per group. Differences between groups were compared using the one-way analysis of variance with Bonferroni correction. Differences within groups between 0 and 23 h were compared using a paired t-test. Differences in plasma chemistry were investigated using an unpaired t-test. Mortality in the different groups was compared using Fisher's exact test.
Results
Mean arterial blood pressure
MAP was equal between the groups despite the completion of resuscitation, where MAP was highest in the NS group (p < 0.05) with no difference at 23 h (Fig. 4).
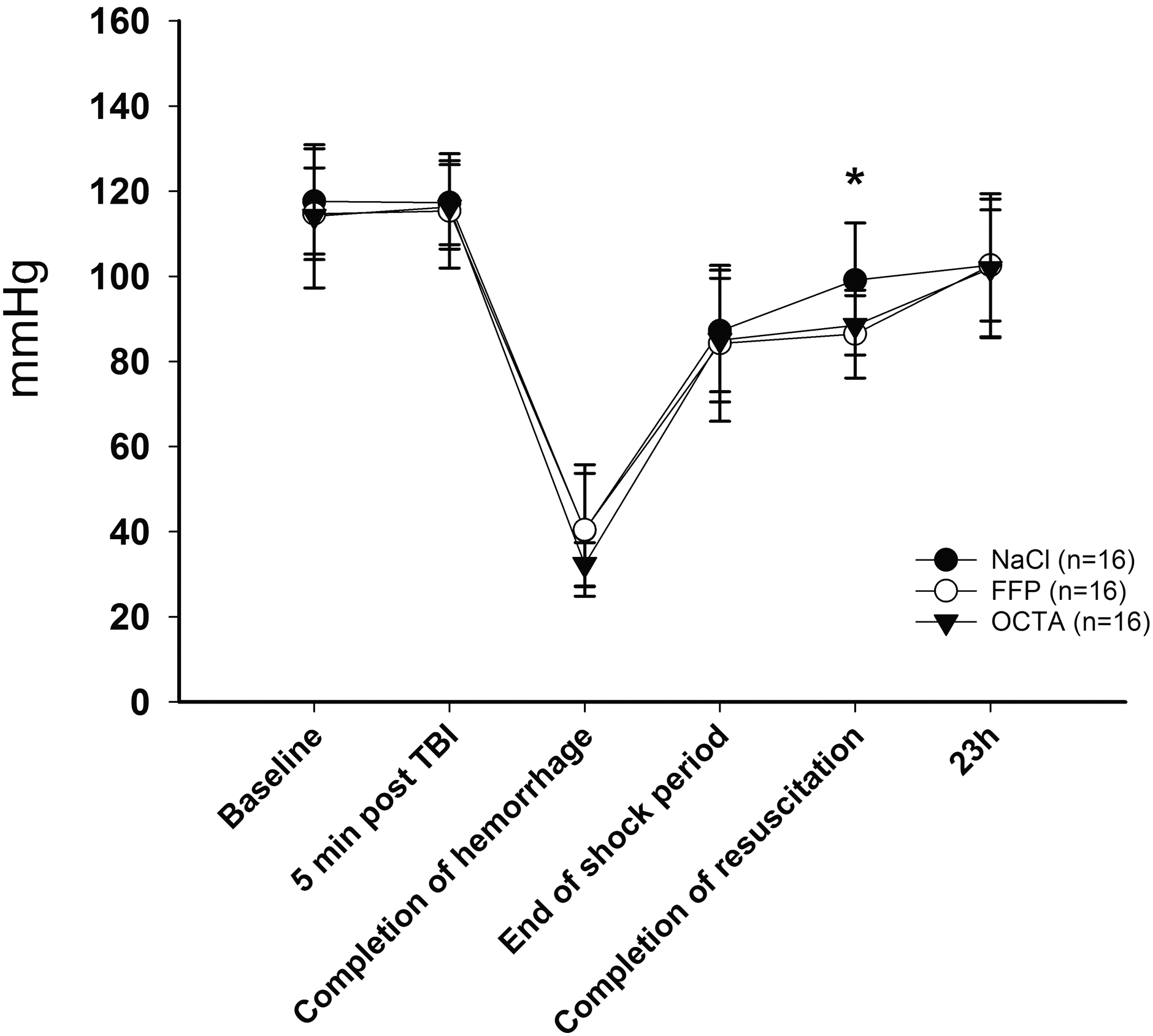
Mean arterial blood pressures at baseline, 5 min post-TBI, completion of hemorrhage, end of shock period, completion of resuscitation, and at 23 h.
Brain water content and blood–brain barrier permeability
At 24 h, brain water content was increased in the injured hemisphere, compared to the uninjured, in all groups (p < 0.001), and it was further increased in the NS group compared to OCTA (81.15 ± 0.86% vs. 80.44 ± 0.29%; p = 0.026; Fig. 5). Brain water content in the injured hemisphere in the FFP group (80.82 ± 0.82%) did not differ from the NS or OCTA groups. BBB permeability (Ki) for 51Cr-EDTA was increased in the injured hemisphere (0.59 ± 0.17 μL/g/min; mean for all), compared to the uninjured (0.27 ± 0.10 17 μL/g/min; mean for all), at 24 h (p < 0.001, for all), with no differences between the groups.

Brain water content (
Oncotic pressure, osmolality, plasma volume, and weight
Oncotic pressure increased in all, with the highest increase in the FFP and OCTA groups at 23 h (p < 0.001; Fig. 6). In the NS group, plasma osmolality decreased immediately after resuscitation to 23 h, which was in contrast to the FFP and OCTA groups. At 23 h, osmolality was further higher in the OCTA versus FFP group (p = 0.027). The weight at baseline in the NS, FFP, and OCTA groups were 370 ± 12, 367 ± 15, and 371 ± 19 g, with no difference between the groups, and at day 1, all groups had an identical weight loss and increase in plasma volume (PV; p < 0.001, for all; Fig. 6).
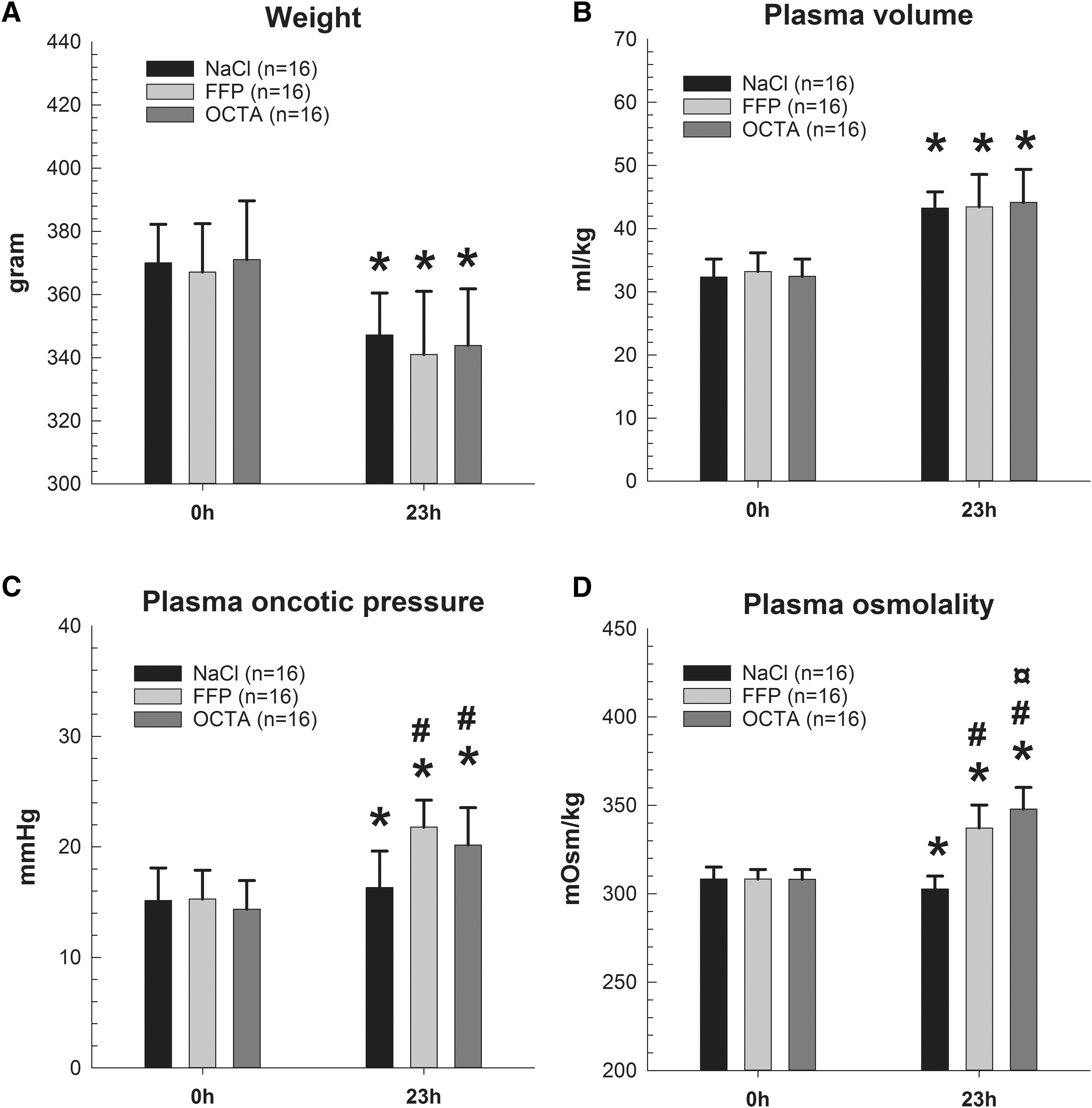
Body weight (
Arterial blood analysis
After resuscitation, OCTA and FFP resuscitated displayed a sustained metabolic alkalosis combined with increased lactate, potassium, glucose, and low sodium levels at 23 h (Table 1). After resuscitation, NS displayed a transient metabolic acidosis that changed to alkalosis at 23 h, combined with increased lactate and glucose levels. Hematocrit was lowered in all groups after resuscitation, but there was no difference between the groups during the experiment.
Data are presented as means ± standard deviation.
NS versus OCTA and FFP (p < 0.05).
NS versus FFP (p = 0.037).
FFP versus OCTA (p = 0.030).
FFP, fresh frozen plasma; OCTA, OctaplasLG® (Octapharma, Stockholm, Sweden).
Circulating biomarkers of glycocalyx shedding and cell damage
Plasma levels of syndecan-1 decreased in the NS group from 0 to 23 h (4.77 ± 1.78 vs. 1.89 ± 0.73; p < 0.000) compared to a nonsignificant decrease in the FFP (4.28 ± 2.00 vs. 3.28 ± 1.10; p = 0.103) and OCTA group (3.96 ± 1.94 vs. 3.27 ± 1.74; p = 0.055). At 23 h, syndecan-1 in the NS group was lower than in the FFP and OCTA groups (p < 0.001). Plasma hcDNA levels increased from 0 to 23 h in the NS group (9.38 ± 6.61 vs. 18.16 ± 16.20; p = 0.031), FFP (9.25 ± 5.92 vs. 32.32 ± 12.20; p < 0.001) and OCTA (7.88 ± 2.86 vs. 25.44 ± 12.27; p < 0.001) groups, and at 23 h, only NS and FFP were different (p = 0.016).
Mortality rates
A total of 78 animals were subjected to FPI, and 20 animals (26%) died directly after FPI from respiratory arrest or neurogenic pulmonary edema (Fig. 2). FPI deaths sustained a higher trauma (2.37 ± 0.05 vs. 2.29 ± 0.07 atm; p < 0.000) and had a lower body weight (355 ± 15 vs. 370 ± 15 g; p < 0.000) than FPI survivors. Animals included in the NS, FFP, and OCTA groups received an equal FPI of 2.29 ± 0.07, 2.29 ± 0.06, and 2.30 ± 0.06 atm (p = 0.920). Mortality rates in the NS, FFP, and OCTA groups were 0 of 16 (0%), 1 of 16 (6.25%), and 3 of 16 (18.8%). In the OCTA group, 1 animal died shortly after resuscitation and another died within 2 h, whereas 1 was dead by 22 h. In the FFP group, 1 was dead by 22 h. Relative risk of death in the NaCl versus FFP group was 1.07 (95% confidence interval [CI], 0.94–1.12; p = 1.000) and 1.23 (95% CI, 0.97–1.56; p = 0.226) in the NaCl versus OCTA group. Two animals were excluded and replaced because of technical problems in the brain water content measurement.
Fresh frozen plasma and OctaplasLG plasma composition
Osmolality was highest in OCTA plasma compared to FFP, whereas oncotic pressure was highest in FFP (p < 0.001 for both; Table 2). Syndecan-1 was only detectable in FFP, and hcDNA concentration was also highest in FFP (p = 0.001). Not measured at our laboratory was glycine, which is added as a stabilizer in OCTA plasma, and has been stated by the manufacture to be the main cause of the high osmolality in OCTA.
Data are presented as means ± standard deviation. Independent-sample t-test: FFP versus OCTA with p values in bold for p < 0.05. Plasma osmolality and oncotic pressure were measured in duplicate in all FFP and OCTA tubes used, and the means were subsequently pooled with means from the same transfusion group. Syndecan-1 and hcDNA levels were measured in duplicate in one tube from each of the two batches of OCTA and FFP, which was the same procedure used for arterial blood gas measurements.
hcDNA, histone complexed DNA; FFP, fresh frozen plasma; OCTA, OctaplasLG® (Octapharma, Stockholm, Sweden).
Discussion
In this study of TBI and HS, animals resuscitated with OCTA had reduced brain water content in the injured hemisphere at 24 h compared to NS resuscitated. This was associated with increased plasma osmolality and oncotic pressure in the OCTA group. No difference in brain water content could be detected between the FFP and NS groups. Biomarkers of endothelial glycocalyx shedding (syndecan-1) and cellular damage (hcDNA) was highest in the OCTA and FFP groups at 23 h, and plasma volumes and Ki for 51Cr-EDTA did not differ.
The lateral FPI model in the rat is widely used and reproduces several aspects of human TBI in terms of behavioral, physiological, and histological changes. 21 We have previously demonstrated that the FPI intensity in the range of that used in the present study results in neuron loss and reductions of motor performance, compatible with an injury in the moderate-to-severe range. 22 The observation that 26% of the animals died within 10 min post-FPI in this study is in the upper end of the mortality reported for a similar FPI, but was most likely associated with the lower body weight and higher trauma in this group. 3,23,24 Our results of reduced brain water content in the OCTA resuscitated are in line with previous findings that FFP decreased brain swelling 6 h post-TBI and HS in a porcine model, and suggest that the beneficial effects of OCTA may last at least 24 h after the initial resuscitation. 14 –16 The BBB is normally impermeable to small solutes, and the crystalloid osmotic pressure of ≈5500 mm Hg on both sides of the BBB is the main driver of fluid exchange. Thereby, any filtration of fluid rapidly creates an opposing crystalloid osmotic force (osmolality) that halts further filtration and maintains brain volume within tight margins. 25 After brain trauma, permeability of the BBB in injured parts of the brain to small solutes increases more than to larger molecules, which is suggested to increase the importance of the colloid osmotic pressure (oncotic pressure) as a force counteracting fluid extravasation. 2,3,6,26 Moreover, the increased permeability of the BBB to small solutes will mean that crystalloids such as NS will distribute into the brain interstitium of injured parts of the brain. 3 Analysis of the resuscitation fluids demonstrated a difference in both osmolality and oncotic pressure that clearly affected both the plasma colloid and crystalloid osmotic pressures in animals at 23 h.
Plasma colloid osmotic pressure was equal and highest in the FFP and OCTA groups, suggesting that this was a mechanism for the lower brain water content in these groups. 27,28 Further, the high crystalloid osmotic pressure in the OCTA group underlines that OCTA further attenuated fluid flux across the intact BBB in the less-injured areas of the brain, and that this was an additional mechanism through which OCTA reduced brain water content. 6 –8 It should be noted that resuscitation with FFP in a porcine model of TBI also has been suggested to reduce excitotoxicity, and we cannot exclude that such effects of OCTA may have contributed to the reduction in brain water content by reducing intracellular fluid accumulation. 29 In the NS group, the increase in oncotic pressure compared to baseline was possibly a result of de novo synthesis of proteins whereas the decrease in osmolality (from 308 to 303 mOsm/kg) reflect a normalization toward the normal levels, reported to be in the range of 295 mOsm/kg in the rat, given that the baseline levels of 308 mOsm/kg were increased because of the 90 min of surgical preparation and assumed free water loss before sampling. 3,6,30
Plasma products contain large amounts of citrate, which may have adverse effects in the setting of massive transfusion (MT). 31 –34 As a substrate of Krebs cycle, citrate can be taken up by cells, including hepatic cells, where it is converted to HCO3 −, which is a likely explanation to our finding that the FFP and OCTA groups presented with increased HCO3 − compared to the NS groups immediately after resuscitation. Given that citrate is a chelator of cations like Ca2+, it has the potential to lower free ionized calcium and impair cardiac and vascular function post-MT. 31 –34 We found that both FFP and OCTA resuscitated animals presented with an almost unchanged MAP immediately after resuscitation, in contrast to NS that experienced an increase in MAP. This difference in MAP occurred despite that NS, FFP, and OCTA were administered in equipotent doses, a notion supported by previous results from our laboratory, showing that resuscitation with colloids and crystalloids in the same ratio as we used resulted in similar plasma volume expansion. 3,35 Based on this assumption, the higher MAP at the end of the resuscitation in the NS group, compared to the FFP and OCTA groups, most likely was caused by the secondary effects on vascular resistance and cardiac contractility attributed to chelation of Ca2+ by citrate in the FFP and OCTA groups, and not by differences in plasma volume. 36,37 MTs have also been associated with hyperkalemia attributed to the load of transfused potassium, which was consistent with the findings in the FFP and OCTA groups at 23 h.
Lactate is commonly suggested to be a marker of poor inadequate organ oxygenation/perfusion, but may also be influenced by other mechanisms, such as decreased clearance of lactate and acid base disturbances, that are unrelated to perfusion defici. 38 Based on the conclusion that plasma volumes are similar in all groups, the higher lactate in the OCTA and FFP groups is most likely attributed to mechanisms other than differences in preload. A contributing factor is likely to be the fact that both plasma preparations contain lactate, but also other mechanisms are likely to contribute. We found no difference in mortality between the groups, but it should be noted that the study was not powered to detect differences in mortality. Hence, we cannot exclude that such differences could have been detected if we had included more animals.
The beneficial effects of FFP resuscitation has in part been referred to restoration of the endothelial glycocalyx layer. 39,40 In contrast to this, we found the highest levels of syndecan-1 in the FFP and OCTA groups and the lowest in the NS group at 23 h. A reason for this difference could be that we measured the long-term effects of resuscitation, and that the previously reported positive effects were short-term effects measured after 2–6 h. 14 –16,39 These positive short-term effects might gradually disappear. However, it should be noted that HS has been suggested to decrease messenger RNA (mRNA) levels of syndecan-1, and the lower syndecan-1 levels in the NS group could reflect a decreased synthesis relative to the FFP and OCTA groups, also demonstrated by increased syndecan-1 mRNA levels in FFP resuscitated animals. 39 The finding that BBB permeability was similar in all groups at 24 h, however, suggests that the observed differences in biomarker levels were not associated with a functional change of the BBB. Cellular release of nuclear proteins like histones and DNA fragments (hcDNA) post-trauma have been associated with cell damage and organ failure. 41 –43 But these and cytoplasmic proteins have also been identified to be released by the neutrophils as “neutrophil extracellular traps,” believed to modulate the immune response and kill bacteria. 44 –48 Therefore, the true nature and interpretation of hcDNA molecules have been challenged in a way where “good” or “bad” most likely is an expression of a balance between a positive and negative activation of the innate immune system, and in a porcine model of TBI and HS, hcDNA levels were increased. 42 We also found increased hcDNA levels in all groups at 23 h, with the highest levels in the FFP group. Despite tissue injury, this is most likely related to the relative high levels found in FFP plasma, and the overall tendency of higher hcDNA levels in both plasma groups at 23 h also demonstrates the impact of this model as described previously. Overall, the role of histones post-TBI requires more investigation given that high levels have been associated with hypocoagulability, inflammation, and endothelial damage post-trauma. 41 –43
Limitations and strengths
Limitations of the study include that the effects of FFP and OCTA on cognitive or motor function were not performed, and we therefore cannot know whether the beneficial effects on brain water content translate into improved outcome. Also, we only measured biomarkers at one time point, and our data therefore provide a snapshot of the events, not reflecting the effects over time. Further, our model of plasma-based resuscitation of a class III hemorrhage differs somewhat from clinical practice, in which hemorrhage of such a magnitude would normally be resuscitated with packed red blood cells, platelets, and plasma. Strength of the study include that we used a well-characterized model of TBI and HS, which replicates many aspects of human trauma. Measurement of PV allowed us to draw conclusions regarding the influence of PV on the observed effects.
Conclusion
SD-treated plasma reduces brain water content at 24 h post-FPI compared to 0.9% NaCl. This effect may be explained by increased crystalloid and colloid osmotic pressures in animals resuscitated with SD-treated plasma. Whether the observed effects of plasma translate into improved outcome is an important area for future studies.
Footnotes
Acknowledgments
The authors thank Helén Axelberg, BA (Technician, Department of Anesthesiology and Intensive Care, Lund University, Lund, Sweden), for skilled technical assistance and Mårten Jungner, MD, PhD (Department of Anesthesiology and Intensive Care, Lund University, Lund, Sweden) for skilled advices regarding the model.
Author Disclosure Statement
No competing financial interests exist.