
Abstract
Wearable sensor assessment tools have proven to be reliable in measuring function in normal and impaired movement disorders during well-defined assessment protocols. While such assessments can provide valid and sensitive measures of upper limb activity in spinal cord injury (SCI), no assessment tool has yet been introduced into unsupervised daily recordings to complement clinical assessments during rehabilitation. The objective of this study was to measure the overall amount of upper-limb activity in subjects with acute SCI using wearable sensors and relate this to lesion characteristics, independence, and function. The overall amount of upper extremity activity counts, measures of wheeling (speed and distance), and limb-use laterality were measured in 30 in-patients with an acute cervical or thoracic SCI three months after injury. The findings were related to the international standards for neurological classification of SCI, the spinal cord independence measure, and the upper extremity motor scores of the Graded and Redefined Assessment of Strength, Sensibility, and Prehension. Overall upper extremity activity counts were successfully recorded in all patients and correlated with the neurological level of injury and independence. Clinical measures of proximal muscle strength were related to overall activity count and peak velocity of wheeling. Compared with paraplegics, tetraplegics showed significantly lower activity counts and increased limb-use laterality. This is the first cross-sectional study showing the feasibility and clinical value of sensor recordings during unsupervised daily activities in rehabilitation. The strong relationship between sensor-based measures and clinical outcomes supports the application of such technology to assess and track changes in function during rehabilitation and in clinical trials.
Introduction
W
In the field of spinal cord injury (SCI), Postma and coworkers 5 validated an accelerometer-based activity monitor in a laboratory setting. This monitor was able to detect wheelchair propulsion with a moderate accuracy in subjects with SCI. It was a multiple-sensor setup, however, requiring wired connections between the sensors and a 700 g data recorder that was worn on the body; hence, such a system is not applicable in unobserved/uncontrolled observations of daily activities. 5
Using a smaller and lighter tri-axial accelerometer, Sonenblum and colleagues 6 developed and validated a methodology to continuously measure wheelchair movements and distances traveled with an accuracy of about 90%. Recently, we have developed and validated a robust IMU-based assessment capable of distinguishing active and passive wheelchair propulsion with an accuracy greater than 93% and kinematic parameters such as distance traveled with an accuracy greater than 97% in a real-world setting. 7
Thus far, the use of such technology in SCI has been limited to studies that evaluate how much persons who mobilize with a wheelchair move, tracking distance wheeled, 8,9 or that evaluate whether physical activity recommendations are met 10 and whether behavioral interventions help meet those recommendations. 11 This is because it is well known that persons with disabilities are less likely to be physically active than healthy subjects 12 and that persons affected by SCI show a lower physical activity level than able-bodied persons. 13 A sedentary lifestyle in wheelchair-bound subjects increases the risk of secondary conditions such as diabetes or cardiovascular diseases 14 ; consequently an active lifestyle may reduce risk-factors such as high density lipoprotein and cholesterol concentration. 15
The advantages of portable-sensor technology may not be limited to an objective evaluation of public health guidelines but may provide notable benefits if used as a functional assessment during and after rehabilitation. 16 In a previous study, the relationship between the level of physical activity and lesion characteristics during in-patient rehabilitation was found to be rather weak. 17 However, lesion characteristics were assessed in a binary fashion (e.g., below or above the segment T1) and the level of physical activity was not compared with functional outcome. So far, a reasonable comparison between wearable sensors and functional or independence scores has not yet been established in SCI.
The purpose of this study was to prove the feasibility of wearable-sensor technology in a multi-center study design and to determine the relationship between sensor-derived upper limb (UL) activity-metrics and patients' characteristics according to sensitive, standardized clinical assessments in an in-patient cross-sectional setup three months after injury.
Methods
Subjects
A total of 30 SCI subjects (age 46.43 ± 16.91 years, range 19–74 years, 21 male, 11 paraplegic, and 19 tetraplegic) were recruited from three specialized SCI centers in Switzerland: the Swiss Paraplegic Centre in Nottwil (13 patients), Balgrist University Hospital in Zurich (12 patients), and Rehab Basel in Basel (five patients). Included in this study were patients with acute traumatic SCI (70–98 days post-injury) with any grade (A, B, C, and D) of the ASIA Impairment Scale (AIS) undergoing primary in-patient rehabilitation and mobilized to undergo an active rehabilitation program. A complete overview of the neurological level of injury (NLI) and completeness can be found in Figure 1.

Description of the study sample. The histogram shows the number of subjects belonging to each neurological level of injury (NLI). (
Because of the broad inclusion criteria, patients with different extents of walking impairment were eligible—i.e., from those who were independently ambulatory or walking with devices to wheelchair-bound patients relying on a manual wheelchair or powered wheelchair. Consequently, patients performed bouts of mobility according to their ability. There were 26 patients who were wheelchair-bound (two patients relied completely on a powered wheelchair, three patients occasionally used a complete or partial power assist on their wheelchair), four patients were fully ambulatory.
Sufficient cognitive ability to follow verbal instructions was required to participate in the study. Subjects with conditions, other than SCI, that were expected to affect UL function, such as neurological diseases (i.e., plexus paresis) as well as orthopedic or rheumatologic diseases (e.g., osteoarthritis) were excluded from the study. Subjects were also excluded in case that they had a pre-morbid or an ongoing depression or psychosis.
Assessments
To report on neurological impairment, capacity of motor function, and independence of patients, various standardized clinical assessments were performed. Neurological assessment was performed following the International Standards for Neurological Classification of SCI (ISNCSCI) 18 and summarized in the NLI and the extent of lesion according to the AIS. The UL muscle function was assessed using the motor domain of the Graded and Redefined Assessment of Strength, Sensibility and Prehension (GRASSP). 19 This domain is assessed with the manual muscle test (MMT) of 10 UL muscles on both arms (scores range 0–50 per arm).
To have a more sensitive measure of strength values from M3 to M5, 20 strength tests with a hand-held dynamometer (HHD) of three key UL movements were performed: elbow flexion (biceps), elbow extension (triceps), shoulder flexion (deltoid). 21 Finally, the Spinal Cord Independence Measure (SCIM) was used to assess the level of independence in daily life (scores range 0–100). 22
Sensor device
The IMU used in this study was the ReSense module. 23 This device records raw data with a three-dimensional (3D) accelerometer, 3D gyroscope, 3D magnetometer, and barometric pressure and with all sensing capacity turned on it can record for at least 24 h. For the analysis, signals coming from the magnetometer and the barometric pressure sensor were omitted.
Data collection and procedure
Research staff consisting of movement scientists, occupational therapists, and physiotherapists were trained to ensure that the GRASSP and HHD examinations, as well as ReSense measurements, were performed correctly. Independent clinicians rated the SCIM questionnaire and the ISNCSCI protocols. For the ReSense measurement, patients were fitted with one ReSense module on each wrist and one on the right wheel of the wheelchair, as reported previously. 7 Subjects were instructed to wear the modules continuously over the period of three weekdays (between Monday and Friday), covering their whole days—i.e., rehabilitation program and daily off-times.
The research staff was asked to start the ReSense measurement on Monday or Tuesday. Patients were told to remove the sensors only during bathing or any activity where the sensor would be submerged in water for long periods. The rehabilitation protocol was prescribed by independent clinicians at the separate centers, and, therefore, it was not influenced in any way by this study.
Because of battery life, the full sensing capacity of ReSense is limited to about one day, and, therefore, the sensors needed to be exchanged daily with a new set of fully charged modules. To measure distance traveled and speed over an extended period, an additional module with only the triaxial accelerometer enabled was fixed on the wheel, thereby increasing the recording time by up to seven days.
Data analysis
After completing the recording, data were transferred from the internal, secure digital card via a custom-designed base station to a personal computer. All data were re-sampled at 50 Hz using a cubic spline interpolation function. This enables the temporal alignment of recordings from different sensor modules. The raw data were analyzed off-line using MATLAB R2013a (MathWorks, Natick, MA). To ensure the integrity of the data, visual inspection was performed. Data recorded during sleep phases and phases when the sensors were taken off were removed before the analysis. As a consequence, sensor-based metrics are derived from the time the patients are awake.
Calculation of UL activity metrics
An IMU-based multi-sensor setup consisting of three ReSense modules (right wrist, left wrist, and right wheel) and an accelerometer-based single sensor set-up (right wheel) were used (Table 1). The multi-sensor setup was used to extract UL activity metrics and label behavioral events (i.e., active-propulsion). The long-lasting single sensor setup was used to extract speed and distance parameters because wheelchair-mobility metrics require an extensive measurement time to achieve adequate reliability. 9
IMU, inertial measurement unit; 3D, three dimensional; RSAL, ReSense Assessment of Laterality; RSWA, ReSense Wheeling Algorithm.
IMU derived outcome measures
Overall activity counts (AC)
The ACs were used as a measure of UL activity. To derive AC, the acceleration signal of each wrist sensor was filtered with a second order Butterworth high-pass filter with a cutoff frequency of 0.25 Hz. The magnitude was calculated and integrated over an epoch of 1 min. To compute the total UL AC over the complete measurement, all AC epochs of the right and left arms were summed and normalized by time.
Limb-use laterality
This was assessed with the ReSense Assessment of Laterality (RSAL), a new IMU-based methodology validated in stroke 24 and in SCI, 25 capable of measuring the prevalence of limb-use laterality in day-to-day activities. Absolute laterality is scored from zero to infinite where the higher the value, the more pronounced the limb-use laterality.
Speed-distance parameters and percentage active wheeling
Data were further analyzed with the ReSense Wheeling-Algorithm (RSWA, setup II.a), an algorithm developed previously by our group, 7 capable of reliably discriminating active (self-propelled) and passive (attendant-propelled) wheelchair propulsion and estimating speed and distance parameters. The labeling of active wheelchair propulsion allows the distinction of total UL activity compared with UL activity related to active wheeling and therefore allows the computation of the count ratio (self-propulsion counts divided by the total number of counts). Distance (in meters) and peak velocity (m/sec) were also computed with the RSWA using the acceleration signal of the single-sensor setup of the right wheel (RSMA setup III.b). Peak velocity was computed using the 90th percentile (10th percentile for backward peak velocity) to have a more robust metric against outliers in peak velocity.
Statistical analysis
The statistical analysis was performed using IBM SPSS Statistics version 19 (IBM, Armonk, NY).
Sample size
We recruited 30 patients with SCI who were heterogenic in terms of their mobility and impairments. Hence, the number of subjects included in different analyses varies to permit robust, non-biased, statements. For example, to evaluate the relationship between muscle function and peak velocity, only wheelchair-bound subjects who did not use any kind of power assist were included, because power assist permits the user to reach higher velocities with less muscle effort. Sample sizes for each analysis are presented in Table 2.
IMU, inertial measurement unit.
Variable reduction
To reduce redundancy in the multiple GRASSP variables, a Principal Components Analysis (PCA) was performed with the MMT values of the tetraplegic subjects. The set of variables was reduced into principal components. Each GRASSP item was analyzed as an individual ordinal variable scored from 0 to 5 and treated as an interval scale variable because the number of levels for each variable is higher than three-level items. 26
Components were retained following subjective judgment by examining the leveling off of the eigenvalues, and their meaning was analyzed. For this purpose, a rotated solution was computed with an orthogonal rotation. The interpretation of the extracted components was based on the component loading on the variables. Finally, for each extracted component, component scores were computed to relate each component with overall UL activity.
Associations
The Spearman rank-order correlation coefficient was used to inspect the associations between assessment scores and sensor metrics, because of the ordinal nature of the ISNCSCI protocol, the SCIM, and the domain scores of the GRASSP. If the data were continuous and normally distributed, the Pearson product-moment correlation coefficient was preferred. Parameters were checked for normality with the Shapiro-Wilk test of normality. A Spearman or Pearson rho value larger than 0.60 was considered as a strong correlation, and the significance level was set to p < 0.05.
Differences between groups
The comparison between paraplegic and tetraplegic groups was performed with a Mann-Whitney U test or an independent samples t test, depending on the nature of the values being compared and their distribution. When the variable was not normally distributed and/or in the case of ordinal data, the Mann-Whitney U test was preferred.
Results
Recordings
The mean length of the genuine data analyzed for the IMU-based setup was 2.87 ± 0.35 days (shortest recording two days, longest recording three days) and for the accelerometer-based setup 6.15 ± 1.12 days (shortest recording four days, longest recording seven days). Patients were awake for 15.31 ± 1.09 h/day (range 13.38–17.76). Wheelchair users actively propelled the wheelchair for 95.70% ± 14.76% (range 39.06–100%) of the wheeling time. They actively covered 2120.50 ± 1296.27 m per day (range 46.03–4936.59) wheeling forward and 167.62 ± 158.58 m per day (range 5.06–812.01) maneuvering or wheeling backward.
Relation between independence and overall UL activity
To investigate the relationship between independence in daily living and overall UL activity, UL activity was correlated with the SCIM self-care sub-domain, which is the sub-domain that reflects UL activity. Overall, UL activity strongly correlated with SCIM self-care (N = 30, p < 0.01, r = 0.692, Spearman correlation, Fig. 2).
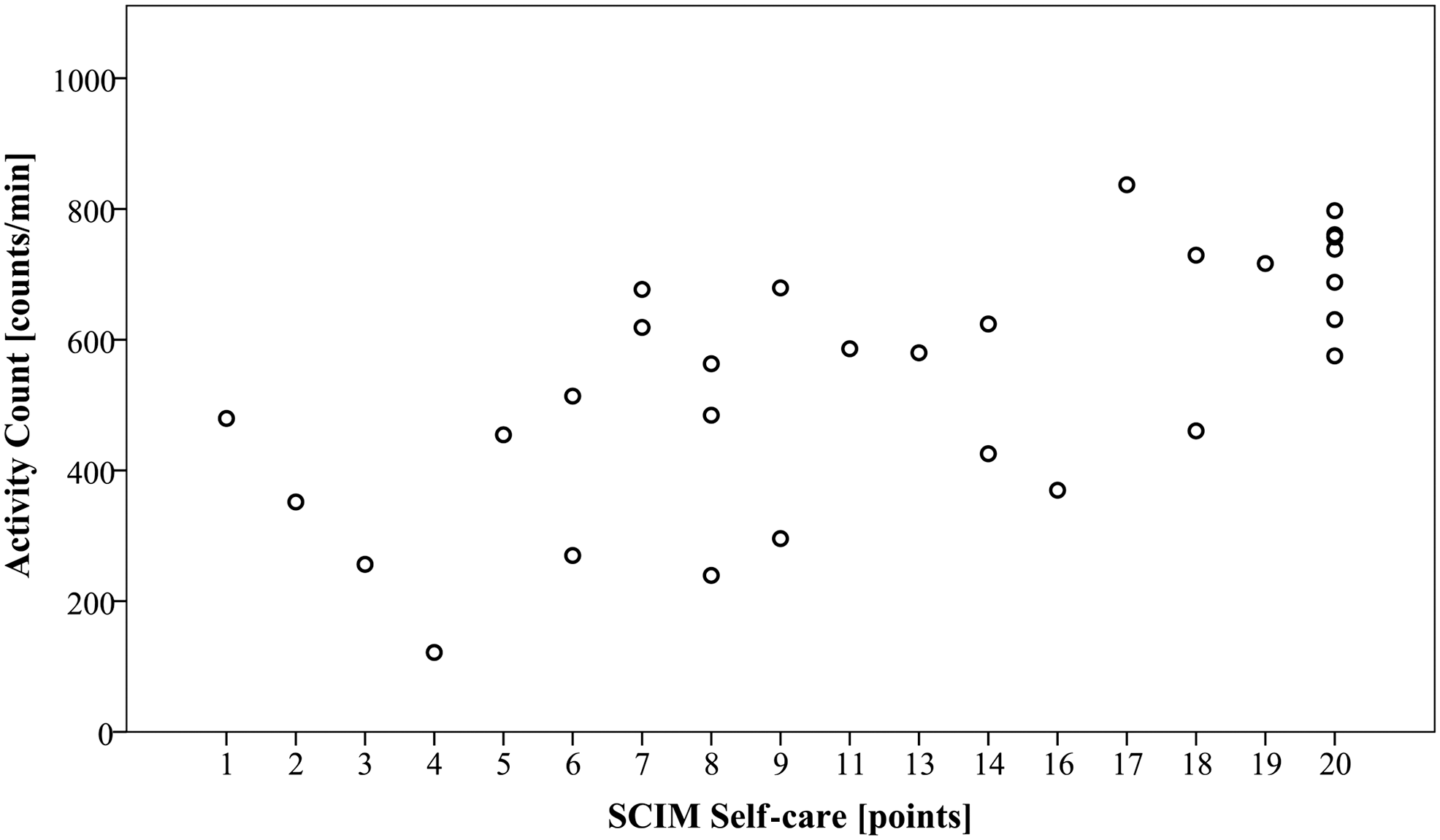
Strong correlation between overall upper limb (UL) activity and independence in daily living. The graph shows the strong correlation between the overall amount of UL activity and the independence in self-care (p < 0.01, r = 0.692, Spearman correlation) for 30 patients with spinal cord injury. SCIM, Spinal Cord Independence Measure.
Relation between lesion characteristics and overall UL activity
To investigate the relationship between lesion characteristics and overall UL activity, correlations between the neurological level of the lesion and completeness scored as part of the ISNCSCI protocol were investigated. Overall UL activity moderately correlated with NLI (N = 30, p < 0.05, r = 0.412, Spearman correlation) but was not significantly related to completeness (N = 30, p = 0.28, r = −0.203, Spearman correlation).
Relation of UL muscle function and overall UL activity
The GRASSP MMT tests several proximal and distal UL muscles. To reduce multi-collinearity and therefore reveal variables that are rather closely correlated and identify variables that are less correlated, a PCA was performed with the MMT values of the tetraplegic subjects. Two principal components (PC1 and PC2), which explained 55.29% and 21.56% of the total variance, respectively, were retained (cumulative 76.85% of total variance explained).
An orthogonal rotation was used to interpret the results, and it revealed strong loading of distal muscle items on component 1 and proximal muscles items on component 2 (Table 3). The relationship between overall UL activity and component scores showed that the overall UL activity was not significantly related to PC1 (N = 18, p = 0.580, r = 0.140, Pearson correlation) but was strongly related to PC2 (N = 18, p < 0.01, r = 0.649, Pearson correlation). Note that one subject was excluded from this analysis because of missing MMT values.
MMT, manual muscle test; GRASSP, Graded and Redefined Assessment of Strength, Sensibility and Prehension.
GRASSP MMT items are visualized in the first column whereas the component loadings are visualized in the second and third column. Higher loadings are visualized in bold (if >0.6). PC1 load mainly on distal MMT items, whereas PC2 load mainly on proximal MMT items.
Speed and distance parameters, activity count of self-propulsion, and limb-use laterality
In the interest of evaluating the relationship between total distance traveled and peak velocity with muscle function, correlation analyses between kinematic metrics and muscle function according to the MMT and the HHD of three key muscles were performed (Table 4). The results show that muscle strength is most closely related to peak velocity and less related to distance, suggesting that longer distances can be achieved with slow speeds and impaired muscle function.
MMT, manual muscle test; HDD, hand-held dynamometer.
Forward and backward peak velocity is highly related to proximal and distal muscle function, according to the Graded and Redefined Assessment of Strength, Sensibility and Prehension MMT. Correlation analysis between forward and backward peak velocity and HHD scores on three key muscles revealed that delta, biceps, and triceps highly influence forward velocity but that only the triceps seems to play a role in backward velocity.
To determinate whether there was a difference in behavioral parameters, such as limb-use laterality, between paraplegic and tetraplegic patients, comparisons between group means were performed. The mean count ratios (self-propulsion counts divided by the total amount of counts) were 0.27 ± 0.11 for paraplegic patients and 0.19 ± 0.12 for tetraplegic patients.
A Mann-Whitney U test revealed that the count ratio of paraplegic subjects (mean rank = 15.90) was significantly higher than for tetraplegic subjects (mean rank = 10.07, U = 36, z = −1.991, p < 0.05), meaning that in paraplegic patients, a much higher amount of UL activity came from self-propulsion. The same two groups of patients showed a significant difference in overall UL activity, where paraplegic subjects performed an average of 656.24 ± 124.72 counts/min and tetraplegic subjects an average of 491.70 ± 166.19 counts/min (t(22) = 2.639, p < 0.01, independent sample t test), suggesting that self-propulsion counts make a high contribution to the overall UL activity.
Finally, mean absolute limb-use laterality was 0.17 ± 0.12 (range 0.01–0.46) for paraplegic patients and 0.93 ± 1.11 (range 0.03–3.57) for tetraplegic patients (Fig. 3). A Mann-Whitney U test revealed that limb-use laterality of tetraplegic subjects (mean rank = 18.00) was significantly higher than for paraplegic subjects (mean rank = 11.18), U = 57, z = −2.044, p < 0.05.
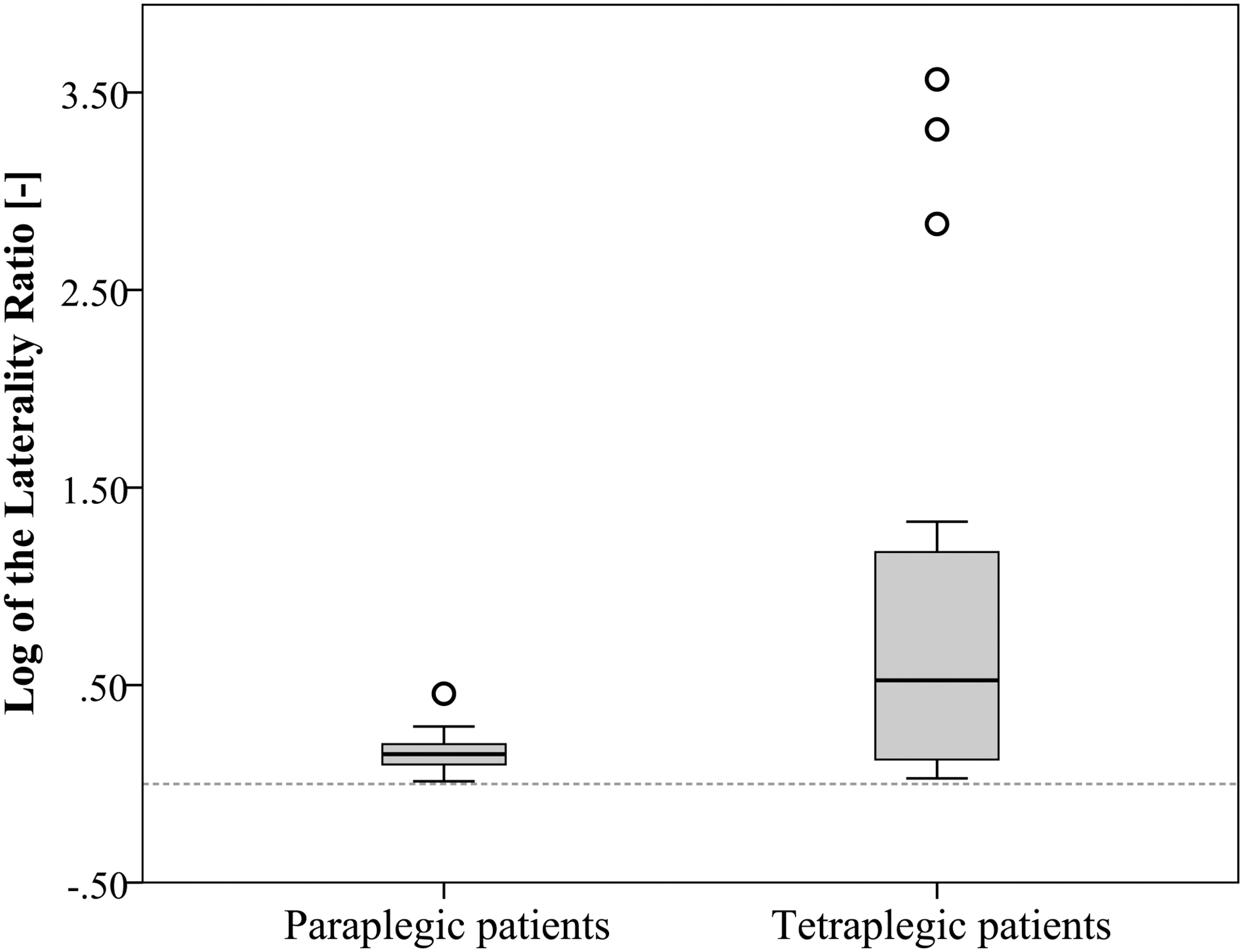
Absolute limb-use laterality between groups. The box plot shows the median (the bottom represents the first quartile, the top represents the third quartile and the whisker is 1.5 times the interquartile range) of limb-use laterality calculated as the absolute log of the laterality ratio for a group of 11 paraplegic subjects and a group of 19 tetraplegic subjects. A Mann-Whitney U test showed that the mean rank (18.00) for tetraplegic subjects were statistically significantly higher than for paraplegic subjects (mean rank = 11.18), U = 57, z = −2.044, p = 0.041.
Discussion
The aim of this study was to assess unsupervised upper-limb activity during rehabilitation in SCI using non-obtrusive wearable sensors and to relate this to clinical assessment scores. We showed that wearable sensors are feasible and provide valid and sensitive information about UL activity and function in SCI. Moreover, this is the first study to reveal that these measures strongly correlate with neurological impairment and are applicable for tracking clinical outcomes in SCI rehabilitation.
The relationship between lesion characteristics and the level of physical activity has been addressed before in in-patients with acute SCI. Van den Berg-Emons and coworkers 17 evaluated whether the level of lesion (above or below the T1 segment) and completeness (motor complete or incomplete) were determinants of changes in physical activity during in-patient rehabilitation but found no relationship.
The assessment of lesion characteristics in a binary fashion, however, is rather less sensitive for analyzing the relationship between lesion characteristics and upper extremity activity in the heterogenic SCI population. 27,28 Therefore, we assessed lesion characteristics applying the ISNCSCI protocol that compiles multiple information about level of lesion, motor and sensory scores across all spinal segments. The latter approach showed a positive relationship between neurological impairment (level of lesion) and overall UL activity in contrast to the simplified distinction of AIS grades. This is not surprising because the AIS grades are biased toward the definition of sacral sparing and therefore do not necessarily reflect the overall impairment after SCI. 27
The introduction of novel treatments in SCI has been challenging because of the need to target appropriate patients and provide satisfactory clinical efficacy. 29 –31 In essence, the latter depends on revealing meaningful improvements in neurological impairment and performance, such as independence during daily life. 32 For this purpose, the SCIM is recommended as a comprehensive assessment of functional recovery because it assesses overall ADL. 29
The present study revealed a strong relationship between the SCIM self-care and sensor-based overall UL activity and indicates that activity measures, as measured by IMU during daily activities, can be used as a surrogate for ADL levels. While sensor-based measures are scored on a continuous scale, instead of the ordinal scale of the SCIM, they may be more sensitive at revealing even small differences and therefore are complementary to clinical scores for tracking changes in clinical trials. In addition, IMU measures are unsupervised and unobtrusive and therefore applicable over a longer and continuous period and do not require the therapist or the patient to fill out a questionnaire.
To evaluate clinically meaningful changes, it is important to explore relationships between neurological function and performance-based outcome measures. Upper extremity motor scores using either the ISNCSCI or GRASSP key muscles, have been proven to assess recovery profiles of the UL over one year after injury. 32 –34
Accordingly, we showed that, specifically, the proximal motor scores of the GRASSP are strongly related to overall UL activity. Even more specific is the strong correlation between the peak velocity of wheeling and the function of specific muscles (i.e., biceps strength). Therefore, the combination of activity measures (i.e., activity counts in relation to independence) and measures of specific motor functions (i.e., detailed assessment of active wheeling) will enable a comprehensive evaluation of changes in UL function and an appreciation of the effectiveness of a therapeutic intervention.
Measures of limb-use laterality have been performed and show that UL activity is more lateralized in adults who have stroke (median absolute magnitude ratio −2.2, interquartile range [IQR] = 6.2) compared with non-disabled adults, where dominant and non-dominant ULs were active to a similar degree (median absolute magnitude ratio 0.1, IQR = 0.3). 35 In a previous study, we showed that limb-use laterality in tetraplegic subjects negatively influences independence because laterality values ranged from 0.00 to 1.60 and were negatively related to scores of independence in self-care. 25
These findings were also confirmed in the present study during unsupervised recordings with laterality values higher in tetraplegic subjects compared with paraplegic subjects who had laterality values in the same range as non-disabled adults. Our findings provide additional evidence that changes in everyday limb-use laterality are most likely caused by functional impairments rather than hand-dominance. This supports the assumption that in the healthy condition much of what we do every day involves the use of both arms regardless of handedness. 36
Limitations
We acknowledge a number of limitations. For the analysis of the relationship between the structure of the lesion and the overall activity, first, a more sensitive assessment may be considered (e.g., neuroimaging) because certain aspects of the ISNCSCI may be insensitive and highly variable. Second, UL activity may be influenced, to some extent, by the clinical setting (e.g., therapies) or by decreased trunk control (e.g., some persons use their arms to stabilize the upper body increasing UL activity or perform fewer UL movements because of the loss of balance), influencing the aforementioned relationships.
Last, we would like to state that measures of overall UL activity and limb-use laterality measure the prevalence of UL activity and limb-use laterality during day-to-day activity but, with the exception of active wheeling, are not able to distinguish, in detail, the type of activity performed.
Conclusion
This study showed the clinical applicability of wearable sensors for measuring UL activity in day-to-day, unsupervised and non-obtrusive recordings in patients with SCI. Sensor-based metrics allow a comprehensive evaluation of UL recovery because measures of overall UL activity and peak velocity were closely related to clinical assessments of function and independence. Wearable sensors are promising as complementary clinical assessments because they can quantify patient activities outside of rehabilitation sessions and thus provide novel insights into overall performance that likely have an impact on outcome in clinical trials.
Footnotes
Acknowledgments
This work was supported by the Clinical Research Priority Program (CRPP) for Neuro-Rehab of the University of Zurich, by the International Foundation for Research in Paraplegia (IRP), by the Swiss Paraplegic Foundation (SPS) and the ETH Zurich Foundation. The authors would like to thank the following persons for the precious help given (in alphabetical order): Karin Akermann, Annika Ballmer, Deborah Bergman, Isabelle Debecker, Dr. med. Margret Hund, Dr. med. Kerstin Hug, Dr. Kaspar Leuenberger, Nils Reiner, Dr. Inge-Marie Velstra.
Author Disclosure Statement
No competing financial interests exist.