
Abstract
Previous studies in pediatric traumatic brain injury (TBI) have been variable in describing the effects of injury severity on white-matter development. The present study used diffusion tensor imaging to investigate prospective sub-acute and longitudinal relationships between early clinical indicators of injury severity, diffusion metrics, and neuropsychological outcomes. Pediatric patients with TBI underwent magnetic resonance imaging (MRI) (n = 78, mean [M] = 10.56, standard deviation [SD] = 2.21 years) at the sub-acute stage after injury (M = 5.55, SD = 3.05 weeks), and typically developing children were also included and imaged (n = 30, M = 10.60, SD = 2.88 years). A sub-set of the patients with TBI (n = 15) was followed up with MRI 2 years post-injury. Diffusion MRI images were acquired at sub-acute and 2-year follow-up time points and analyzed using Tract-Based Spatial Statistics. At the sub-acute stage, mean diffusivity and axial diffusivity were significantly higher in the TBI group compared with matched controls (p < 0.05). TBI severity significantly predicted diffusion profiles at the sub-acute and 2-year post-injury MRI. Patients with more severe TBI also exhibited poorer information processing speed at 6-months post-injury, which in turn correlated with their diffusion metrics. These findings highlight that the severity of the injury not only has an impact on white-matter microstructure, it also impacts its recovery over time. Moreover, findings suggest that sub-acute microstructural changes may represent a useful prognostic marker to identify children at elevated risk for longer term deficits.
Introduction
S
Diffusion tensor imaging (DTI) is an MRI technique that provides the ability to characterize white-matter microstructure by measuring the degree of water diffusion in white matter. 4 It may be a valuable clinical biomarker for detecting injury and monitoring recovery of white matter post-injury.
A number of studies have used DTI to quantify white-matter damage after pediatric TBI; see Roberts and associates 5 for a review. The most commonly derived DTI metric is fractional anisotropy (FA); group differences in FA are often interpreted in terms of post-injury reorganization or damage to white matter. More recently, studies have highlighted the importance of the diffusion metrics mean diffusivity (MD), axial diffusivity (AxD), and radial diffusivity (RD) in terms of white-matter microstructure.
MD represents the average rate of diffusion in all directions and can increase with white-matter injury and neuronal loss, 6 –8 AxD represents diffusion parallel to axons and can increase with axonal injury, and RD represents perpendicular diffusion and can increase with demyelination. 9,10 Traditionally, many studies have focused on FA as a measure of white-matter integrity; however, AxD and RD have been identified as better indices for investigating axonal injury and myelination. In animal models, the acute stage of injury has been associated with decreases in AxD. 9,11
DTI studies have shown that pediatric TBI results in short- and longer-term alterations in white-matter microstructure, evidenced by decreases in FA that may suggest diffuse axonal injury. 12,13 Most commonly, FA changes have been noted in the corpus callosum, internal capsule, and longitudinal fasciculus, thought to be because of the shearing forces associated with the injury. 14,15
A meta-analysis by Roberts and associates 5 revealed that the timing of MRI after pediatric TBI dictates the direction of FA and MD change. Acute imaging post-TBI (1–4 weeks post-TBI) results in paradoxical increases in FA and decreases in MD in cohorts with mild TBI. 16 –18 This is likely because of axonal swelling, edema, and other pathological processes that can temporally alter diffusivity. 19 Longer-term imaging post-TBI (3–45 months) results in decreases in FA and increases in MD, 20,21 which supports the notion that a TBI results in white-matter damage, or disruption to white-matter organization. More research is needed to examine the effect of age at injury and injury severity on white-matter microstructure.
To date, studies examining relationships between injury severity and microstructural white-matter change in pediatric populations are largely inconsistent. Wilde and colleagues 22 showed that if a severe injury occurs during childhood in the developing brain, this has implications for development trajectories in white/gray matter and results in neurobehavioral and cognitive disturbances.
Despite the abundance of results in the literature relating severe injuries with diffusion changes, to our knowledge, no studies have investigated the relationship between all injury severity types (mild, moderate, and severe) with diffusion metrics after pediatric TBI or explored the lasting impacts and recovery of these acute disturbances in diffusion metrics. Literature devoted to adults has suggested that more severe injuries lead to decreased white-matter load. 23,24 This knowledge, however, cannot readily be applied to children and adolescents, in whom the brain is immature, because injury in childhood can lead to differential disruption of white-matter maturation.
In this study, we examine both cross-sectional and longitudinal profiles of diffusion metrics commonly derived from DTI to determine the acute and longer term impact of a pediatric TBI on global white-matter microstructure. The main objectives of the study were: (1) to confirm differences in diffusion metrics sub-acutely after a pediatric TBI compared with typically developing (TD) children; (2) to determine the impact of injury severity on white-matter microstructure during the sub-acute phase and the relationship with cognitive outcomes at 6 months post-injury; and (3) to longitudinally assess the impact of injury severity on white-matter development 2 years post-injury.
Methods
Participants
The study was approved by our local ethics committee, and informed consent was obtained from each participant or the parent/guardian. All procedures were conducted in accordance with the Declaration of Helsinki. This prospective, longitudinal study comprised 122 children who completed diffusion MRI scans; of those, 14 were excluded because of motion or other missing data. A total of 78 children and adolescents with a range of mild to severe TBI were included in the current study (age at injury: mean [M] = 10.44, standard deviation [SD] = 2.21 years), and 30 age- and sex-matched TD controls (M = 10.60, SD = 2.88 years) who were recruited from local schools. A random sub-set of 15 patients with TBI were recruited into a sub-study and returned for a follow-up MRI post-injury (M = 22.3, SD = 2.3 months) with injury severity classification at baseline as mild (n = 6), moderate (n = 6), and severe (n = 3).
All participants were ascertained between 2007 and 2010 and were aged 5.8–14.5 years at time of recruitment. Children and adolescents with TBI were recruited at time of injury and represented consecutive admissions to The Royal Children's Hospital (RCH), Melbourne, Australia. Inclusion criteria for the study were: (1) age at injury 5.5–14.5 years; (2) evidence of a closed head TBI; (3) a period of altered consciousness; and (4) English speaking. Exclusion criteria were based on parent report and consisted of: a previous head injury; non-accidental injury; and any known pre-existing physical, neurological, psychiatric, developmental, or attentional disorder.
Injury characteristics
Patients were categorized according to clinical indicators of injury severity—mild (n = 43), moderate (n = 28), or severe (n = 7), using a combination of injury related information: mild TBI: Glasgow Coma Scale (GCS) score
25
on admission 13–15, indicating some alteration of conscious level (e.g., drowsiness, disorientation), with no evidence of mass lesion on clinical computed tomography (CT)/MRI and no neurologic deficits; moderate TBI: GCS on admission 9–15, indicating significantly altered consciousness, with reduced responsiveness and/or mass lesion or other evidence of specific injury on clinical CT/MRI, and/or neurological impairment; and severe TBI: GCS on admission 3–8, representing coma, and mass lesion or other evidence of specific injury on clinical CT/MRI and/or neurological impairment. Lesion location was further assessed using susceptibility-weighted imaging as described previously in Anderson and coworkers
26
using the same sample of children (Supplementary Table 1; see online supplementary material at
TBI, traumatic brain injury; TD, typically developing; M, mean; SD, standard deviation; MRI, magnetic resonance imaging; SES, socioeconomic status; WASI, Wechsler Abbreviated Scale of Intelligence; IQ, Intelligence Quotient; WISC, Wechsler Intelligence Scale for Children; GCS, Glasgow Coma Scale Score. Difference between TBI and TD groups defined using: aindependent samples t test; bchi-square test.
Demographics
Socioeconomic status (SES) was determined using the Australian Socioeconomic Index 2006 (AUSIE06), which translates data coded in accordance with the official occupational classifications of the Australian Bureau of Statistics—the Australian and New Zealand Standard Classification of Occupations (ANZSCO)—into occupational status. The AUSIE06 converts scores for ANZSCO major, sub-major, minor and unit group codes into a continuous scale, ranging from 0 (laborers) to 100 (medical practitioners).
Cognitive abilities 6 months post-injury
Neuropsychological data were obtained for 77 patients with TBI and 30 TD control children. General intellectual ability was assessed using the Wechsler Abbreviated Scale of Intelligence (WASI) 27 composite score (M = 100; SD = 15), which is a standard score reflecting verbal and non-verbal abilities based on performance on the vocabulary and matrix reasoning sub-tests.
Working memory was assessed using the Digit Span sub-test from the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV), 28 which requires the child to repeat a list of digits that are spoken by an experimenter at a rate of approximately one digit per second. The Digit Span Forward and Digit Span Backward process scores are summed and converted to a Digit Span Total Scaled Score (M = 10, SD = 3).
Processing speed was assessed using the Processing Speed Index from the WISC-IV, which is a composite index based on performance on two sub-tests measuring speed of thinking and motor speed (Coding, Symbol Search). This index score (M = 100, SD = 15) was derived from raw scores based on the Australian standardization sample data.
MRI acquisition
Patients with TBI underwent MRI post-injury (M = 5.55, SD = 3.05 weeks). TD control children also underwent MRI. Fifteen patients with TBI returned for a follow-up MRI post-injury (M = 22.3, SD = 2.3 months) and were imaged using the same imaging protocol on the same MRI scanner. Baseline scans we acquired between 2007 and 2010 and follow-up images were obtained between 2009 and 2012, and no major scanner upgrades occurred during the acquisition period.
Neuroimaging data were acquired at 3.0T (Siemens Tim Trio, Erlangen, Germany). Transverse two-dimensional single-shot echo-planar imaging images were acquired (repetition time/echo time [TR/TE]: 9300/104 ms, field of view = 256 mm, 64 slices, bandwidth = 1396 Hz/pixel, echo-spacing = 0.8 msec, slice thickness = 2.0 mm, voxel size 2.0 × 2.0 × 2.0 mm) with 60 diffusion-encoding gradient directions (b = 2000 s/mm2) and 10 images acquired with no diffusion weighting (b = 0 s/mm2).
To prepare this pediatric population for MRI, they each conducted a “mock” or practice MRI session, whereby participants were familiarized with the scanner environment and practiced lying still in the bore of the scanner with sound recordings of typical MRI sequences playing. In addition, participants had access to a television screen where they watched a movie of their choice, which was instrumental in engaging their attention and minimizing motion in the scanner. During the MRI session, radiographers were in constant contact with the participants and notified them if they were moving. Where possible, if excessive motion was detected on the image reconstructions, these sequences were repeated.
Image processing
Diffusion-weighted images were subjected to quality control (QC) tests by visual inspection for motion artefacts evidenced by slice-dropout or signal loss. Of the 122 scans, 14 participants were excluded because of poor imaging data as a result of motion. The resulting diffusion MRI data (78 TBI; 30 TD controls) were then pre-processed in Oxford Centre for Functional MRI of the Brain Software Library (FSL) 29 by correcting for eddy current distortions and subject motion using the “eddy correct” tool. Images were skull-stripped using the “BET” tool and fit to the diffusion tensor with weighted-least squares using FSL's diffusion toolbox.
A whole brain voxel-wise statistical analysis was performed using Tract-Based Spatial Statistics (TBSS) implemented in FSL. 30 The mean FA image was created and skeletonized (excluding voxels with an FA ≤0.3) and projected onto each participant's FA volume. These steps were repeated for MD, AxD, and RD maps.
Because of the nature of the current study, some participants had focal lesions visible in their white/gray matter. To assess the potential impact of focal lesions on our processing, we visually inspected structural images overlaid with the white-matter skeleton from TBSS, and there was minimal overlap between the skeleton and the visible lesions.
Statistical analysis
Sub-acute impact of TBI on white-matter microstructure
A whole-brain and voxel-wise approach was used to identify regional white-matter differences between the TBI and TD groups. For the whole-brain analysis, the mean value across the white-matter skeleton was extracted and subjected to further analysis. For the voxel-wise analysis, a general linear model (GLM) was generated using the FSL software, with age and sex added as nuisance variables, and each diffusion metric was analyzed using the permutation-based method “Randomize” in FSL with 10,000 permutations. Family-wise error rate (FWE) was controlled using Bonferroni correction with threshold-free cluster enhancement. 31 Only significance values corrected for FWE are reported. Regions of change were determined using the ICBM-DTI-81 white-matter labels atlas in FSL.
Impact of injury severity on white-matter microstructure within the TBI group
For each diffusion metric, a whole-brain and voxel-wise approach was used (as above) to investigate the effects of TBI severity on diffusion metrics. In addition, a moderation analysis was performed to determine whether the relationship between injury severity and diffusion metrics was influenced by injury age (i.e., whether there was an interaction between injury severity and the age at which the injury occurred).
Neuropsychological performance classified on injury severity
To understand the relationship between injury severity and age-adjusted neuropsychological tests scores, separate GLMs were computed for each score. Using the regions that significantly regressed onto injury severity in the previous experiment, we tested the relationship between neuropsychological test scores and FA/MD/RD values in the white-matter skeleton using a Pearson R correlation.
Longitudinal change in diffusion metrics in TBI classified on injury severity
A similar analysis was performed for the 15 patients with data available at 2-year follow-up. Voxel-wise permutation testing was used to identify regions of differential change between the severity groups. Mean diffusion metrics were extracted for the whole white-matter skeleton and analyzed in subsequent GLMs to examine the relationship with injury severity. Sex and age at baseline MRI were included as nuisance variables.
All GLM analyses (except for voxel-wise analyses performed with FSL) were conducted using SPSS 22.0 (IBM Corporation). Effect sizes for the overall GLMs are reported as partial η2, with .02 considered a small effect, .13 medium, and .26 large. 32 Planned linear contrasts were computed for each analysis to test for a linear difference between groups. Effect sizes for linear contrasts are reported as the Bonett delta (d), where .02 is small, .05 is medium, and .08 is a large effect. 33 Significance values corrected for familywise error (p FWE) within each analysis (Holm method) are also reported. Moderation analysis was performed using the MODPROBE software. 34
Results
Demographics
The TBI and TD groups did not differ in age at MRI, sex distribution, age at neuropsychological testing, or any of the neuropsychological indices (Table 1). SES differed between the groups (p < 0.01), where the TD group had a higher SES score than the TBI group.
Sub-acute impact of TBI on white-matter microstructure
To ascertain whether TBI had sub-acute effects on white matter, we first performed an analysis of the mean for each diffusion metrics across the whole white-matter skeleton. The difference between TBI and TD control groups was statistically significant for AxD, t(106) = 3.26, p = 0.001, p FWE = 0.004, d = 0.70. There were no statistically significant differences in FA, t(106) = 0.27, p = 0.79, p FWE = 0.79, d = 0.06, MD, t(106) = 2.10, p = 0.04, p FWE = 0.12, d = 0.43, or RD, t(106) = 1.13, p = 0.26, p FWE = 0.52, d = 0.25, between the groups.
To identify regional differences further, we performed a voxel-wise analysis on diffusion metrics across TBI and TD groups (Fig. 1). The voxel-wise analysis revealed significantly higher MD and AxD in sub-acute TBI compared with TD children, when controlling for age and sex. There was no significant difference in FA and RD. Areas of MD differences were predominantly in the body of the corpus callosum, as well as the genu, splenium, and anterior corona radiata. Areas of AxD change were primarily in the corpus callosum, middle cerebellar peduncle, and anterior corona radiata.

Tract-Based Spatial Statistics results from the voxel-wise test comparing typically developing (TD) children with patients with traumatic brain injury (TBI). The white-matter skeleton is presented in green and overlaid on the MNI152 1 mm T1 image. The colored overlays are areas where mean diffusivity (MD, blue) and axial diffusivity (AxD, pink) are significantly higher in sub-acute TBI compared with TD children (family-wise error corrected). Regions of significance have been thickened for ease of visualization using the FSL toolbox. Slice coordinates are x = 13 mm, y = −21 mm, z = 30 mm, presented in radiological convention (left is right).
Impact of injury severity within the TBI group on whole brain and regional white-matter microstructure
To investigate whether there were differences in white-matter microstructure associated with injury severity (mild, moderate, severe), we computed a GLM to examine the relationship of injury severity on mean diffusion metrics over the white-matter skeleton. As shown in Table 2, there was a significant main effect and linear contrast for injury severity in FA, F(2,73) = 11.89, p < 0.001, p
FWE = 0.001, η2 = .25, MD, F(2,73) = 4.93, p = 0.01, p
FWE = 0.02, η2 = .12, and RD, F(2,73) = 9.71, p < 0.001, p
FWE < 0.001, η2 = .21. The group differences for AxD did not reach statistical significance (p = 0.99, p
FWE = 0.99). The table of values can be found in Supplementary Table 2; see online supplementary material at

Box plots of diffusion tensor imaging metrics in the white-matter skeleton across traumatic brain injury (TBI) severity. Mean diffusion values for each participant were calculated in the white-matter skeleton and plotted according to TBI severity. Typically developing (TD) control children were also included for comparison. Pairwise comparisons of diffusion metrics are between TD and TBI groups. Horizontal brackets represent significant differences between TD control children and each injury severity type: p < 0.05 (*); p < 0.01 (**); p < 0.001 (***). FA, fractional anisotropy; AxD, axial diffusivity; MD, mean diffusivity; RD, radial diffusivity.
FEW, family-wise error; FA, fractional anisotropy; MD, mean diffusivity; AxD, axial diffusivity; RD, radial diffusivity.
Bold indicates significant differences (p<0.05) in diffusion metrics across severity type.
To localize white-matter alterations, we performed TBSS and subsequently tested the impact of injury severity on diffusion metrics. Permutation-based testing revealed there was a significant linear relationship between injury severity and FA, MD, and RD—where FA was negatively associated with injury severity (i.e., lower FA with increasing injury severity), and MD and RD were positively associated with injury severity (i.e., higher MD/RD with increasing injury severity). These changes were predominately noted in the body of the corpus callosum across all diffusion metrics (Fig. 3).
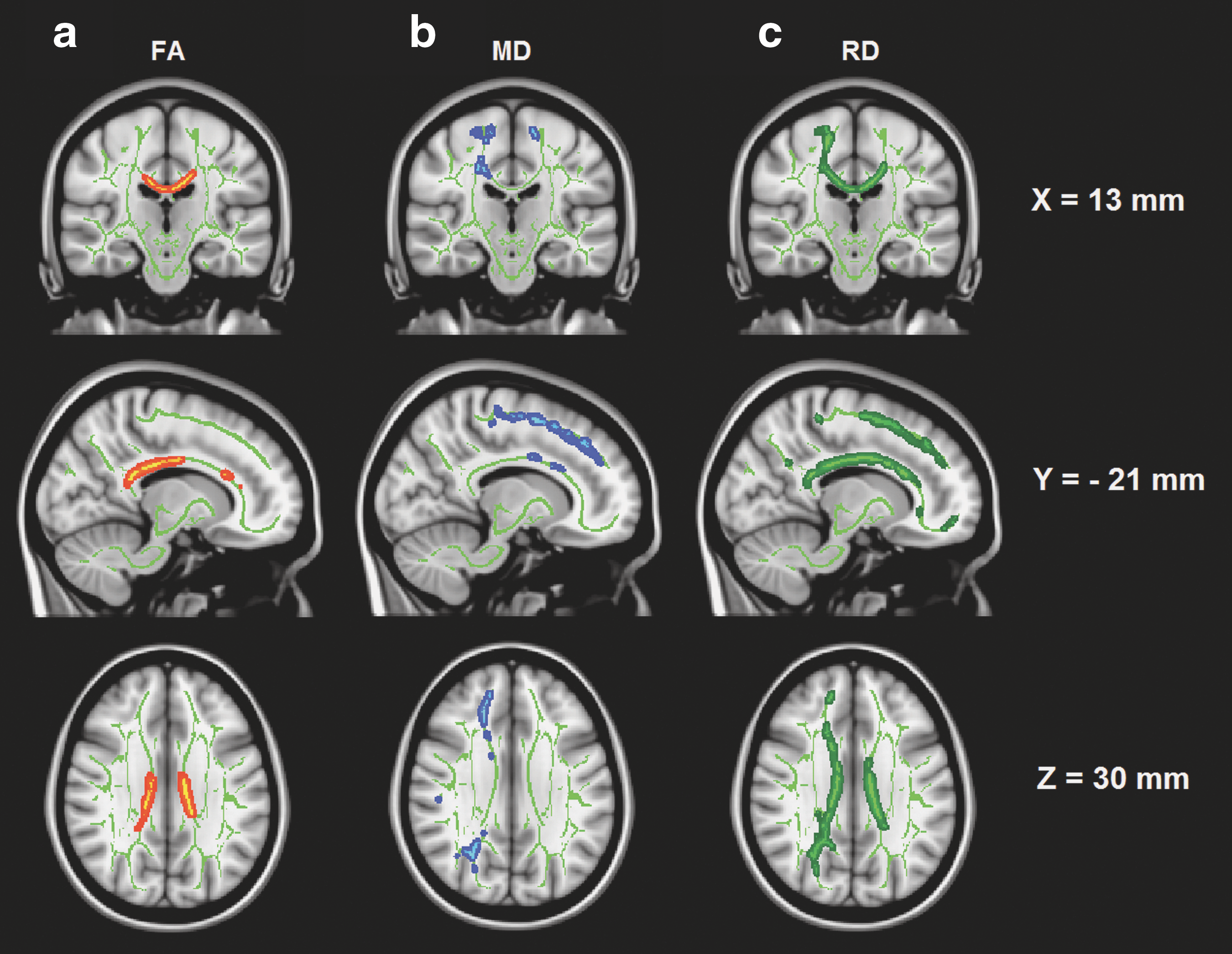
Tract-Based Spatial Statistics results from the voxel-wise test of injury severity against diffusion metrics in the group with traumatic brain injury (TBI). The white-matter skeleton is presented in green and overlaid on the MNI152 1mm T1 image. The colored overlays are areas that have a significant linear relationship between TBI severity and diffusion metrics (red, fractional anisotropy [FA]; blue, mean diffusivity [MD]; dark green, radial diffusivity [RD]). Regions of significance have been thickened for ease of visualization using the FSL toolbox. Slice coordinates are x = 13 mm, y = −21 mm, z = 30 mm, presented in radiological convention (left is right).
Other regional clusters of FA change were observed in the splenium and genu of the corpus callosum, as well as the left external capsule and anterior corona radiata. In addition, higher MD was observed in the right corona radiata (anterior, posterior, and superior) and left external capsule. Higher RD was also noted in the genu, splenium, as well as left and right anterior corona radiata. There was no significant association between injury severity and AxD.
Relationship between TBI and age
Given that white-matter diffusion metrics change over development and the range of injury age in this study, we also examined whether age at injury moderated the relationship between injury severity and white-matter microstructure. As shown in Table 3, age at injury did not moderate injury severity; that is, the relationship between injury severity and diffusion metrics was similar at all ages of injury.
DF = 2,71
FEW, family-wise error; FA, fractional anisotropy; MD, mean diffusivity; AxD, axial diffusivity; RD, radial diffusivity.
Neuropsychological performance classified on injury severity
GLM analysis revealed a significant effect of injury severity on WISC Processing Speed Index, F(2, 74) = 4.24, p = 0.018, p FWE = 0.05, η2 = .10, with a statistically significant linear contrast (p = 0.005, p FWE = 0.02, d = 4.53). There was no effect of injury severity on WASI intelligence quotient (IQ), F(2, 74) = .82, p = 0.45, p FWE = 0.90, η2 = .02 or Digit Span Total, F(2, 74) = .05, p = 0.96, p FWE = 0.98, η2 < .01. We then examined the relationship between diffusion metrics across the whole white-matter skeleton and cognitive test scores.
Information processing speed was correlated with the significant regions of FA (r = .36, p = 0.001, p FWE = 0.004) and RD (r = −.32, p = 0.004, p FWE = 0.012), but not MD (r = −.25, p = 0.031, p FWE = 0.062) or AxD (r = −.02, p = 0.86, p FWE = 0.86). Therefore, a more severe injury resulted in poorer information processing speed, which correlated with higher FA and lower RD. No significant relationships were observed between IQ or digit span and diffusion metrics in these regions.
Impact of injury severity on longitudinal diffusion metric changes in pediatric TBI
To deduce the impact of injury severity on white-matter development, voxel-wise analysis was performed on a sub-set of participants with TBI who were followed-up 2 years post-injury. Voxel-wise permutation-based testing revealed that injury severity significantly predicted the longitudinal change in a number of diffusion metrics.
For diffusion metrics across the whole white-matter skeleton, group differences were statistically significant for MD, F(2,11) = 7.65, p = 0.008, p FWE = 0.03, η2 = .58, AxD, F(2,11) = 7.61, p = 0.008, p FWE = 0.03, η2 = .58, and RD, F(2,11) = 4.23, p = 0.04, p FWE = 0.04, η2 = .44. Linear contrasts were significant for MD (p = 0.003, p FWE = .02, d = 1.37), AxD (p = 0.004, p FWE = 0.02, d = 1.19), and RD (p = 0.02, p FWE = 0.04, d = 0.91). Longitudinal change in MD, AxD, and RD was positively associated with injury severity over time. There was no significant linear relationship between injury severity and FA.
Voxel-based analysis revealed that the regions most commonly associated with longitudinal changes in MD were the retrolenticular part of the internal capsule (L & R), corona radiata, right superior longitudinal fasciculus, and genu of the corpus callosum. Regions of AxD change were noted in the genu and left anterior corona radiata, and changes in RD were noted in the right posterior corona radiata.
Discussion
The current study aimed to investigate the sub-acute and longitudinal effects of mild, moderate, and severe TBI on commonly derived diffusion metrics in a large, representative sample of children and adolescents who were recruited on the basis of consecutive hospital admissions for TBI.
Group comparison between TD and TBI groups using TBSS confirmed microstructural differences in TBI, revealed by increases in AxD and MD in the TBI group compared with TD control participants. This is in keeping with some studies showing TBI can result in diffuse axonal injury, which is reflected by changes in diffusion metrics. 35,36 There was no evidence for a difference in FA between the groups, which may be a result of confounding time from injury to MRI, where FA can increase in the short-term and decrease in the medium to long term after injury. 5
Within the TBI group, injury severity was linearly associated with absolute FA, MD, and RD values, suggesting a clear relationship between more severe injury and greater impact on white-matter microstructure. Interestingly, the voxel-wise analysis revealed very well delineated associations between TBI severity and the corpus callosum—with minimal peripheral regions involved in this relationship. This supports the literature that has shown severe TBI is associated with white-matter damage in the corpus callosum.
In both child and adult TBI studies, corpus callosum microstructure is usually considered a “surrogate marker” of general injury severity. 37 The corpus callosum is a region commonly affected by TBI and has been investigated extensively as a region because it is vulnerable to local changes in volume and diffusion metrics because of the impact of shearing/stretching forces on the midbrain sustained during an injury. Long-term diffuse atrophy of the corpus callosum has been well documented in children who have sustained TBI early in life, 38 and this is also supported by changes in FA and MD, 39,40 which is consistent with the findings of the current study. This may relate to the pattern of injury mechanism in our sample.
White matter develops and becomes better organized with age, reflected by changes in diffusion metrics. 41,42 Our results demonstrated a linear relationship between age and diffusion metrics; however, we were interested in investigating whether the age at injury moderated the relationship between injury severity and diffusion metrics. In the moderation analysis, age at injury did not moderate the relationship between injury severity and diffusion metrics, which is important to note because regardless of the age at injury, the impact on white-matter microstructure seems to be consistent across all ages investigated in this study (5–15 years).
Concordant with previous findings, 43 there was a significant linear relationship between processing speed and injury severity. With respect to DTI metrics, processing speed was significantly associated with mean FA and RD values in the white-matter skeleton, highlighting the potential impact of these microstructural disturbances on cognition. In addition, the implication of corona radiata as a region associated with TBI severity may explain processing speed disturbances, which has been described previously. 44,45 It is well established that TBI results in changes in processing speed and cognition; however, the structural link between damage to white matter and injury severity, which in turn leads to cognitive disturbances, is a novel finding in the pediatric context.
In contrast to previous studies, which have identified robust associations between IQ, working memory, and white-matter microstructural integrity in the chronic phase of injury, 37,39 these relationships did not reach statistical significance in the present study. Because there was limited evidence for group differences on these behavioral measures at 6 months post-injury, it may be that these diffusion metrics have greater prognostic value for identifying children who are likely to show late-emerging cognitive impairments and may fail to make age appropriate gains in the chronic phase of injury.
In addition, because the TBI sample comprised a high proportion of mild cases (55%), performance in the “mild” group 6 months post-injury may have returned to baseline levels, thus inflating the scores of the TBI group overall. Future studies should consider baseline and follow-up neuropsychological testing coinciding with imaging to elucidate a clearer causal relationship between DTI biomarkers and cognitive performance.
A strength of the current study is its prospective, longitudinal design, which supports the notion that injury severity is a key determinant of outcome in terms of white-matter microstructure, as well as information processing speed. We showed a significant linear relationship between injury severity and the change in diffusion metrics over 2 years. The children with a more severe injury had a smaller magnitude of change in their diffusion metrics after 2 years, which may suggest the typical development of their white matter was impeded, with less recovery, because of the severe TBI.
Few longitudinal pediatric TBI imaging studies exist, but this research is important in determining whether these changes impact recovery and development of white-matter microstructure. One study 46 investigated a cohort of children with TBI at 3 months and 18 months post-injury and found decreases in FA and increases in MD compared with an orthopedic control group, consistent with our findings. A similar study 47 revealed that, in a moderate/severe pediatric TBI sample, MD and RD were increased in patients with TBI 13–19 months post-injury.
Our results largely agree with these findings, but further extend on this knowledge with the inclusions of a large sub-set of participants with mild TBI compared with previous longitudinal studies, which have only looked at the impact of moderate/severe TBI on microstructure. Despite the small number of cases followed up longitudinally in the present study, we believe this knowledge is an important contribution to the literature.
Limitations and future directions
Time dependence of neuroimaging after TBI is a confounding factor when looking at group differences, because the pathophysiological response to diffuse axonal injury varies from time of injury. Edema, swelling, and inflammation can be present at the sub-acute stage of injury, which can result in paradoxical increases in diffusivity metrics; this may cause issues with voxel-based analyses such as TBSS whereby the highest FA value is chosen for inclusion in the white-matter skeleton.
Ideally, imaging needs to be performed in a relatively tight interval post-injury, which we have attempted to do in the present study. In addition, the absence of longitudinal typically developing data meant that we could not directly compare the developmental changes as a result of TBI against a TD sample. Future research might benefit from standardizing the time between injury and imaging, and re-scanning TD children.
Subsequent investigations should focus on chronic neuroimaging to deduce the full impact of TBI severity on recovery and development of white matter, as well as investigate the prognostic utility of these techniques for chronic neuropsychological outcomes. Moreover, future work would benefit from using region-of-interest based approaches, tractography, and graph theoretical analyses with the use of longitudinal pipelines, which may assist to elucidate relationships between injury-related impairments and topological alterations in large-scale networks of the developing brain.
Conclusion
In this large representative sample of pediatric patients with TBI, injury severity is strongly associated with diffusion metrics at the sub-acute stage of injury and their change after 2 years in a smaller sub-sample. This knowledge is important, because white-matter disturbances at an early age can significantly impact the recovery and development of white matter, as well as information processing speed.
Footnotes
Acknowledgments
This work was supported by a grant from the Victoria Neurotrauma Initiative, Australia. This research was conducted within the Australian Centre for Child Neuropsychological Studies and Developmental Imaging research groups, Murdoch Childrens Research Institute and the Children's MRI Centre, Royal Children's Hospital, Melbourne, Victoria. It was supported by the Murdoch Childrens Research Institute, The Royal Children's Hospital, The Royal Children's Hospital Foundation, The Department of Paediatrics, The University of Melbourne and the Victorian Government's Operational Infrastructure Support Program.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.