
Abstract
Inflammation in traumatic spinal cord injury (SCI) has been proposed to promote damage acutely and oppose functional recovery chronically. However, we do not yet understand the signals that initiate or prolong inflammation in persons with SCI. High-Mobility Group Box 1 (HMGB1) is a potent systemic inflammatory cytokine—or damage-associated molecular pattern molecule (DAMP)—studied in a variety of clinical settings. It is elevated in pre-clinical models of traumatic spinal cord injury (SCI), where it promotes secondary injury, and strategies that block HMGB1 improve functional recovery. To investigate the potential translational relevance of these observations, we measured HMGB1 in plasma from adults with acute (≤ 1 week post-SCI, n = 16) or chronic (≥ 1 year post-SCI, n = 47) SCI. Plasma from uninjured persons (n = 51) served as controls for comparison. In persons with acute SCI, average HMGB1 levels were significantly elevated within 0–3 days post-injury (6.00 ± 1.8 ng/mL, mean ± standard error of the mean [SEM]) or 4–7 (6.26 ± 1.3 ng/mL, mean ± SEM), compared with controls (1.26 ± 0.24 ng/mL, mean ± SEM; p ≤ 0.001 and p ≤ 0.01, respectively). In persons with chronic SCI who were injured for 15 ± 1.5 years (mean ± SEM), HMGB1 also was significantly elevated, compared with uninjured persons (3.7 ± 0.69 vs. 1.26 ± 0.24 ng/mL, mean ± SEM; p ≤ 0.0001). Together, these data suggest that HMGB1 may be a common, early, and persistent danger signal promoting inflammation in individuals with SCI.
Introduction
T
Increasingly, there also is appreciation for the potential impact of systemic inflammation in persons with chronic SCI, where inflammatory mediators may promote many of the common medical complications of living with SCI and limit potential gains in functional recovery. 2 For example, autoimmune promoting mediators and elevated autoantibodies have been demonstrated in persons with chronic SCI. 7,8 Also, elevated pro-inflammatory cytokines have been demonstrated in the circulation of persons with SCI. 8 –12 As interventional trials for both acute and chronic SCI are increasing, there is renewed interest in identifying inflammatory mediators in persons with SCI that can be easily measured within clinically relevant time windows and tissues. 4,13,14 There also is interest in understanding how immune responses acutely after SCI may be related to persistent inflammation and other immune dysfunction in chronic SCI. 2
High-Mobility Group Box 1 (HMGB1) is a highly conserved DNA binding protein that can be released from cells into the extracellular milieu, where it can have potent pro-inflammatory activities. 15 –19 HMGB1 has both central and peripheral sources: It can be secreted by activated immune cells or released passively by dead and dying cells, such as damaged neurons. There are several cell surface receptors that bind HMGB1, including the pattern recognition receptors Toll-like receptor 2/4 (TLR2/4), and the receptor for advanced glycation end-products (RAGE). 19 –23 Of potential relevance to SCI, HMGB1 also binds to neuronal NMDA receptors, where it potentiates activation that leads to excitotoxicity. 24,25 Post-translational modifications, specifically oxidation status, of HMGB1 confers it different biological activities, partly reconciling its widespread constitutive intracellular expression and its potent inflammatory effects. 19,21,22,26 –28
HMGB1 is elevated in many acute pathophysiological settings, including sepsis, general trauma, traumatic brain injury (TBI), and cerebral ischemia. 18,29 –35 Systemic HMGB1 also is elevated in individuals with chronic disease, including multiple sclerosis (MS) and neuromyelitis optica (NMO). 36 –38 In pre-clinical studies, HMGB1 and its receptors are elevated after spinal cord ischemia or traumatic SCI. 39 –42 Most recently, HMGB1 was identified in a pre-clinical unbiased proteomics screen as enriched at the spinal cord injury lesion site and as a secreted product from injured spinal explants. 43 Anti-HMGB1 therapies or ablation of its receptors are protective of secondary damage and promote recovery after SCI. 39,44 Here, the objective was to determine if HMGB1 is elevated systemically in persons with acute or chronic SCI, compared with uninjured persons.
Methods
Participants
The study was performed in accordance with ethical standards of and approved by the local institutional review board (IRB). Data obtained from some of the same participants has been described previously. 6,9 Inclusion criteria for acute SCI participants (n = 16) were age ≥18 years old and initial traumatic SCI that had occurred ≤1 week prior. Exclusion criteria were documented medical history of cancer, autoimmune disease, or other neurologic disease. SCI was determined by clinical and radiographic presentation. Of the 16 participants with acute SCI, nine had their injuries assessed according to the International Standards for Neurologic Classification of Spinal Cord Injury by a physiatrist who was board certified in SCI medicine and INSTEP trained. For the remaining participants with acute SCI (n = 7), the physiatrist performed a retrospective review of clinical data, including consultation notes from occupational therapists, physical therapists, and physicians to interpolate American Spinal Injury Association Impairment Scale (AIS) grade and skeletal level of injury (neurological level could not be determined). Data for a single participant (#15) who did not survive their injury was too limited to determine more than that the injury was incomplete. Most participants (n = 13/16) had a mild (> 13) Glasgow Coma Scale score and most participants (n = 11/16) had a severe (> 15) injury severity score (ISS), assessed by a surgeon board certified in trauma and critical care. Steroids were administered to a minority (n = 6/16) of participants with acute SCI. The number of blood samples (n = 30) obtained was 24 within 0–3 DPI and six within 4–6 DPI from participants with acute SCI as indicated in Table 1.
SEM, standard error of the mean; SCI, spinal cord injury; I/C, Motor incomplete or complete; AIS, American Spinal Injury Association Impairment Scale; Samples DPI, the days post-injury (DPI) when samples were collected from each participant; LOS, length of stay; Y, yes; MVA, motor vehicle accident; N, no; YPI, years post-injury.
Participants with chronic SCI (n = 47) were recruited from an outpatient clinic of a department of physical medicine and rehabilitation. Inclusion criteria were ≥18 years old, history of SCI at any level, an initial injury occurring ≥1 year prior, an AIS grade of A-D. Exclusion criteria were pressure ulcers, cancer, chemotherapy, neutropenia, or autoimmune disease, or concurrent infection such as frank urinary tract infection as indicated by lab evidence and some clinical occurrence (e.g., hematuria, fever, incontinence between catheterizations). 9 For persons with acute or chronic SCI, injuries sustained by mechanisms other than falls, motor vehicle accident (MVA), sports, or violence were characterized here as “other” (Table 1).
For comparison, we utilized plasma samples from uninjured participants (N = 51) that were of similar age and gender distribution to SCI participants. Blood was drawn once from uninjured individuals who were ≥18 years old, without history of SCI, and within an age range and gender distribution similar to the SCI participants.
Biochemical analysis
A commercial enzyme-linked immunosorbent assay for HMGB1 (IBL International, Hamburg, Germany) was used to measure plasma HMGB1, according to the manufacturer's protocol. Assays were read on a Victor 3 platform (Perkin Elmer 1420 Multilabel Counter) and analyzed using Microsoft Excel and Prism GraphPad 6.0. Samples were assayed at least in duplicate and assay ranges (0.31–10 ng/mL) were essentially as specified by the manufacturer. According to the manufacturer, serum HMGB1 levels >1.4 ng/mL should be interpreted as “elevated.” Plasma HMGB1 was detectable in all SCI and in most of uninjured participants (Table 2). For statistical analyses, measurements below the limit of detection were assigned a value of half of the lowest detectable value, as done previously. 9 Data are reported as mean ± standard error of the mean (SEM) unless otherwise noted.
Units, ng/ml.
HMGB1, High Mobility Group Box 1; SCI, spinal cord injury; DPI, days post injury; NA, not applicable; SEM, standard error of the mean.
Statistical analysis
In acute SCI participants, data was binned for analysis into 0–3 and 4–7 DPI, as done previously. 6 Mean and peak values were calculated for each participant per bin. If only a single sample was obtained from a participant, then the same value was used for mean and peak. A single sample was analyzed from each chronic SCI (n = 47) or uninjured (n = 51) participant. The Mann Whitney test was used to compare HMGB1 levels in bins (acute SCI) and used to perform comparisons between and within participant groups (acute or chronic SCI), according to individual demographic variables, as described. 6,9 The Kruskal-Wallis test was used to compare HMGB1 levels according to mechanism of injury, and when available, AIS grade. Secondary analyses among participants with SCI were conducted to examine the relationship between HMGB1 levels and time from injury using the Spearman correlation. Analyses were generated using SAS 9.3 (SAS Institute Inc., Cary, NC) and graphs were generated using Prism Graphpad.
Results
HMGB1 is significantly elevated in persons with acute SCI
Clinical and demographic variables for all participants are shown in Table 1. There were 51 uninjured participants, 16 participants with acute SCI, and 47 participants with chronic SCI. Participants in all groups were mostly male and within a comparable age range (Table 1A). Among persons with acute SCI, the most common etiology of injury was fall (50%), followed by MVA (25%), and sports (12%; Table 1B). Among persons with acute SCI, injuries were mostly at the cervical level (75%) and neurologically incomplete (69%). Among persons with chronic SCI, the most common etiology of injury was MVA (38%), followed by fall (26%), and sports (23%; Table 1C). Among persons with chronic SCI, injuries were mostly at the cervical level (62%), but were most commonly neurologically complete (AIS A, 59%).
Average levels of HMGB1 were significantly elevated in persons with acute SCI, compared with uninjured persons (p < 0.0001, analysis of variance; Fig. 1A). Peak (maximum) levels of HMGB1 in persons with acute SCI were more than nine-fold higher than in uninjured persons and were significantly elevated at both 0–3 and 4–6 DPI (p < 0.001 and p < 0.01, compared with controls; Fig. 1B; Table 2). HMGB1 levels were elevated in persons with neurologically complete or incomplete injuries, compared with uninjured persons (Fig. 1C; 6.75 ± 1.7 vs. 10.8 ± 4.7 ng/mL, respectively). Peak levels of HMGB1 were significantly elevated in persons with injuries at T5 and above (p < 0.0001), as well as at T6 and below (p < 0.05; Fig. 1D).
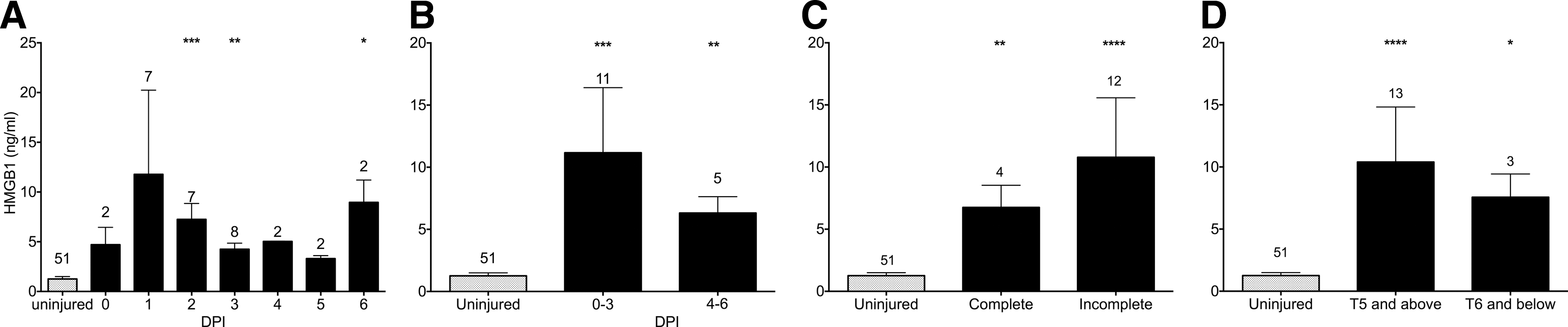
High-Mobility Group Box 1 (HMGB1) levels are elevated in persons with acute spinal cord injury (SCI). In all panels, gray dotted bar indicates HMGB1 value obtained from uninjured persons (n = 51).
While not statistically significant, some intriguing correlative trends were observed between HMGB1 levels and clinical variables among persons with acute SCI. Average HMGB1 levels were higher in participants (n = 4) who did not survive acute hospitalization (21.47 ± 13.6 for non-survivors vs. 6.00 ± 1.0 for survivors; p > 0.05). Accordingly, HMGB1 levels tended to be higher in participants with severe (n = 11) rather than mild/moderate (n = 4) ISS (10.72 ± 5.2 vs. 7.31 ± 1.8 for severe vs. mild/moderate, respectively; p > 0.05). The minority of participants (n = 6) who were given steroids tended to have lower HMGB1 levels than those who did not (3.31 ± 0.7 vs. 7.93 ± 2.0; p > 0.05). HMGB1 was not significantly correlated with age or hospital length of stay.
HMGB1 is significantly elevated in persons with chronic SCI
To investigate whether HMGB1 also may be relevant in the chronic phase of SCI, we next measured HMGB1 levels in a separate cohort of persons who had been injured at least 1 year prior to study enrollment. The time from initial injury ranged from 1–44 years (15 ± 1.6 mean ± SEM), with participants living with SCI for <5 (n = 12) or >5 years (n = 35). Persons with chronic SCI also had significantly higher average levels of HMGB1 than uninjured persons (p < 0.0001; Table 2; Fig. 2A). HMBG1 levels were elevated significantly in persons living with SCI for less or more than 5 years (Fig. 2B), and did not correlate with time from initial injury. HMGB1 levels were significantly elevated in persons with chronic SCI who had motor and sensory complete (AIS grade A) or incomplete (AIS grade D) injuries (p < 0.001; p < 0.05; Fig. 2C), corresponding to the two most common AIS grades. HMGB1 levels were significantly elevated in persons with injuries above or below level T5 (p < 0.0001; p < 0.01; Fig. 2D). Average HMGB1 levels were two-fold higher in persons with acute SCI at 0–3 or 4–7 DPI than with chronic SCI (6.03 or 6.1 vs. 3.5 ng/mL, p < 0.05; Table 2).
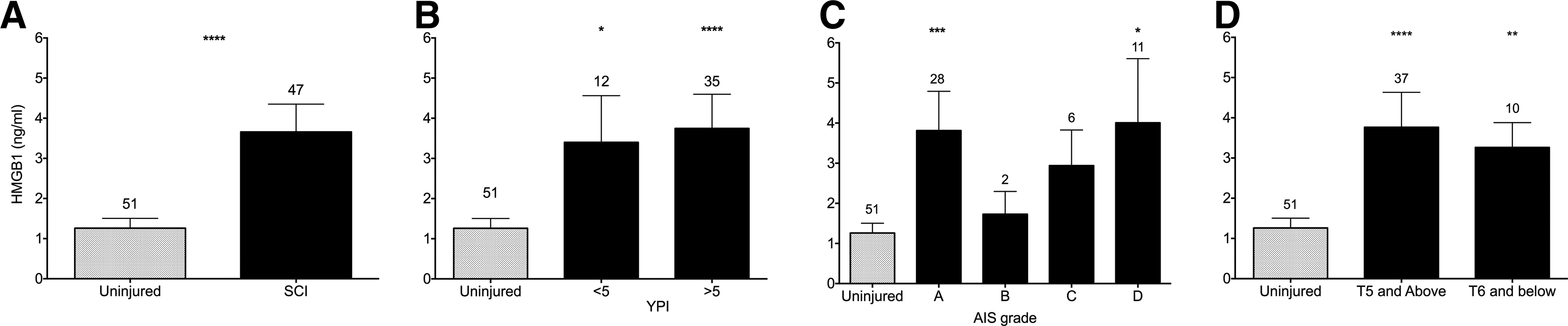
High-Mobility Group Box 1 (HMGB1) levels are elevated in persons with chronic spinal cord injury (SCI). In all panels, gray hatched bar indicates mean HMGB1 value obtained from uninjured persons (n = 51).
Discussion
Here, we provide the first evidence that HMGB1 is elevated systemically in persons with acute or chronic traumatic SCI. The average level of HMGB1 within the first week post-SCI was greater than four-fold higher than in uninjured persons (Fig. 1; Table 2). The maximum HMGB1 level in persons with acute SCI was more than nine-fold higher than in uninjured persons and more than two-fold higher in persons with chronic SCI (Fig. 1A, 1B; Table 2). HMGB1 levels were elevated in persons with acute SCI independent of neurological completeness of injury or level of injury (Fig. 1C, 1D). HMGB1 levels were about three-fold higher in persons with chronic SCI than in uninjured persons (Fig. 2A) and were significantly elevated independent of time from initial injury (Fig. 2B). When examined by AIS grade, HMGB1 levels were significantly elevated in persons with chronic SCI who had motor and sensory complete (AIS A) or incomplete (AIS D) injuries (Fig. 2C), which were the largest subgroups of participants with chronic SCI. In persons with acute or chronic SCI, HMGB1 was significantly elevated in persons with injuries at levels T5 and above, as well as T6 and below, the site of sympathetic nervous system outflow from the spinal cord that has been implicated in the dysregulation of immune responses in SCI (Figs. 1D, 2D). 2
While this study included a relatively small number of participants with acute SCI, HMGB1 levels and trends are similar to those measured in other acute clinical settings. To compare the data shown here with plasma HMGB1 levels in general trauma or other medical conditions, see Table 3. For example, HMGB1 levels ranged from ∼2.5–10 ng/mL (n = 168) in patients with acute general trauma. 45 In children or adults with acute traumatic brain injury (TBI), HMGB1 levels were similarly significantly elevated (5.73 ± 1.45 ng/mL within 24 h and 13.5 ± 3.6 ng/mL) and levels correlated with clinical outcomes. 34,18 In adults with subarachnoid hemorrhage, HMGB1 levels (10n g/mL) correlated with survival status. 46 In acute stroke, HMGB1 is released from brain, with the inflammatory (reduced) isoform predominating, and elevated plasma HMGB1 correlated with stroke severity and poor functional outcomes. 32,33,35 Most persons with SCI are in the chronic phase, where inflammation may oppose the potential for functional recovery, as well as promote many secondary medical complications, such as atherogenesis and other risks for coronary heart disease. 2 However, the biological signals promoting inflammation in chronic SCI are not well understood, and may be both central and/or peripheral. HMGB1 is present in active lesions from autopsy tissue and messenger RNA (mRNA) for its receptors are elevated in peripheral blood mononuclear cells isolated from persons with MS. 36 In persons with MS or NMO, plasma HMGB1 levels (1.33 or 3.99 ng/mL) were similar to those measured here in persons with chronic SCI. 17 Elevated levels of HMGB1 mRNA and protein, as well as its receptors RAGE, and TLR2/4, have been demonstrated in spinal cord tissue of amyotrophic lateral sclerosis patients. 47,48
(n) Indicates number of participants with the medical condition indicated in first column and does not include number of healthy controls or other cohorts in the study.
HMGB1, High Mobility Group Box 1; ELISA, enzyme-linked immunosorbent assay; SIRS, systemic inflammatory response syndrome; OF, organ failure; DIC, disseminated intravascular coagulation; NMO, neuromyelitis optica; MS, multiple sclerosis.
HMGB1 has been proposed as a therapeutic target in acute SCI. 44,49,50 In a rat compression model of SCI, HMGB1 was upregulated in the spinal cord at 0–3 DPI, including in apoptotic cells. 49 In a rat contusion model of SCI, HMGB1 mRNA and protein was upregulated within the first 14 DPI, an effect that was attenuated by treatment with hyperbaric oxygen. 44 Using a novel method to extract extracellular matrix molecules at the lesion site in a pre-clinical study of SCI, Didangelos and colleagues identified HMGB1 as a critical alarmin promoting inflammation, while inhibition of TLR4, one of its receptors, dampened the inflammatory response. 43 Thus, both active and passive release of HMGB1 appears to contribute to elevated levels acutely in pre-clinical models of SCI. The biology of HMGB1 receptors TLR2/4 and RAGE in SCI models is complex, likely reflecting contributions of their multiple endogenous and exogenous ligands. TLR2/4 was elevated acutely in the mouse spinal cord in a moderate contusion model of SCI, but interestingly, its genetic deletion led to worsened functional outcomes and aberrant inflammation. 41 Genetic deletion of another HMGB1 receptor, RAGE, improves outcomes in a mouse contusion model of SCI. 51 Therapeutic interventions with agents that neutralize the inflammatory activities of HMGB1, such as ethyl pyruvate or glycrrhizin, are protective in ischemic models of SCI. 39,52 Intriguingly, it was recently discovered that the inflammatory properties of HMGB1 also can also dampened in vitro by binding to salicylic acid, a metabolite of aspirin. 53 As pre-clinical studies of anti-inflammatory agents in SCI increase, it may be important to note that in rheumatoid arthritis patients, treatment with an anti-tumor necrosis factor inhibitor did not alter HMGB1 levels in synovial fluid; therefore, it may be desirable to neutralize HMGB1 in a targeted manner. 54
HMGB1 is a pleotropic molecule and has many cellular sources; thus, there may be multiple pathways by which elevated systemic levels of HMGB1 may contribute to worse outcomes in SCI. There are likely to be multiple sources, both central and peripheral, as well as different post-translationally modified forms, of elevated HMGB1 in the circulation of persons with acute or chronic SCI and future studies are needed to investigate this. Pre-clinical experiments show that the disulfide (inflammatory) form of HMGB1 promotes glutamatergic excitotoxicity in vitro and promotes seizures in vivo; therefore, it is possible that elevated HMGB1 in acute or chronic SCI may promote neuronal excitability and loss. 24,25 In pre-clinical studies of peripheral nerve injury, HMGB1 was persistently released by injured sensory neurons and interacts with RAGE to activate nociceptive neurons, supporting the notion that HMGB1 may promote neuropathic pain, which is experienced by the majority of persons living with chronic SCI. 55,56
There are several limitations to this study, which are common to clinical studies of SCI. 6,9 Due to the challenges of conducting research in an acute traumatic setting, the relatively small group of participants with acute SCI did not have the same sampling rate or frame, nor was all clinical data available for each participant. Due to IRB restrictions and the widespread clinical applicability of blood samples, we measured HMGB1 in plasma and not cerebrospinal fluid (CSF). Based on the study of Kwon and colleagues, which compared inflammatory mediators in plasma and CSF obtained from the same persons with acute SCI, we may have underestimated the differences in HMGB1 levels between participant groups. 3 Finally, the observations made here were from plasma obtained from separate cohorts of persons with acute or chronic SCI, therefore we do not yet know how HMGB1 levels change over time within the same individuals after SCI, as they transition from the acute to chronic phase. As a result, we do not know if or how HMGB1 levels vary with functional recovery or medical complications of living with SCI. Taken together, these data support further investigations into the roles of HMGB1 in SCI, including the attempt to replicate our findings of elevated peripheral HMGB1 in larger cohorts of persons of SCI.
Footnotes
Acknowledgments
We thank the participants for enabling this study and Ms. Rachel Monahan and Chrissy Demers, RN, for excellent clinical research coordination. Support was provided by the Craig H. Neilsen Foundation (grant to OB), the New York State Empire Clinical Research Program (grant to OB). The Feinstein Institute for Medical Research previously received a grant (#M01RR018535) from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), to support a General Clinical Research Center. The contents here are solely the responsibility of the authors and do not necessarily represent the official view of NCRR, NIH, or any other funding agency. We thank Northwell Health for additional institutional support.
Author Disclosure Statement
For Angelos Papatheodorou, Katie Gibbs, Cristina Sison, Peter Davies and Matthew Bank, no competing financial interests exist.
For Ona Bloom, no competing financial interests exist; however, she received grants from the Craig H. Neilsen Foundation and the New York State Empire Clinical Research Investigator Program, and her institution received a grant from National Center for Research Resources during the conduct of the study. Dr. Bloom received an honorarium from the Craig H. Neilsen Foundation for membership on a peer review panel, outside the submitted work.
For Adam Stein, no competing financial interests exist; however, he reports personal fees from the Craig H. Neilsen Foundation, Stem Cells Inc., and In Vivo Therapeutics outside the submitted work. No compensation is associated with his board membership in the following organizations: Association of Academic Physiatrists and American Spinal Injury Association.