
Abstract
Traumatic brain injury (TBI) is known to have a substantial though highly variable impact on cognitive abilities. Due to the wide range of cognitive abilities among healthy individuals, an objective assessment of TBI-related cognitive loss requires an accurate measurement of pre-morbid cognitive performance. To address this problem, we recruited 50 adults who sustained a TBI and had performed a cognitive baseline assessment in adolescence as part of the aptitude tests mandated by the Israeli Defense Forces. This group was matched with non-injured controls (n = 35). Pre- and post-injury cognitive assessments consisted of three domains—namely, verbal abstraction, mathematical reasoning, and non-verbal abstract reasoning (from the Wechsler Adult Intelligence Scale-Third Edition). The difference between post- and pre-injury scores was calculated as a measure of domain-specific cognitive decline. Voxel-based regression was used to correlate cognitive decline with modulated gray matter probability maps controlling for age, Glasgow Coma Scale, and total intracranial volume. Using objectively assessed cognitive scores, we found that abstract reasoning declined in both moderate-severe and mild TBI patients, whereas verbal abstraction declined only in the moderate-severe group. Mathematical reasoning was not affected by TBI. In the TBI patients, non-verbal abstract reasoning post-pre-injury change scores were negatively correlated with the volume of the insula. We conclude that access to pre-morbid neuropsychological data may have facilitated the discovery of the effects of mild TBI on abstract reasoning, as well as a significant correlation between TBI-related decline in this cognitive domain and the volume of the bilateral insula, both of which had not been appreciated in the past.
Introduction
T
In recent years, there has been a large increase in the number of studies on the neuropsychological sequelae of TBI and in particular that of mTBI. These studies often report conflicting findings, 5 –7 which could be the results of inconsistencies in tests used across studies, specific sample demographics, and injury-related characteristics. We hypothesized that an additional contributing factor could be lack of information on pre-morbid cognitive performance, and that known pre-morbid cognitive performance would allow researchers and clinicians to more conclusively demonstrate changes or lack of changes in cognitive performance. In most TBI studies, actual pre-injury assessment is not available and estimates obtained through various methods have a large margin of error. 8,9 This is understandable since cognitive loss induced by TBI or other pathologies is likely to be overestimated in individuals with low pre-morbid ability. These individuals may be erroneously deemed to have suffered a TBI-related deficit when compared with a population norm. 10
Conversely, pathology-related cognitive loss is likely to be underestimated in individuals with high pre-morbid ability, since even if they suffer significant cognitive decline they may test within the normal range. Consequently, a true assessment of individual TBI-related cognitive loss requires an accurate measurement of pre-morbid performance. Moreover, a comparison between pre- and post-injury cognitive scores is essential for reducing overestimates, as well as underestimates, of cognitive loss, 11 especially since pre-morbid cognitive ability itself may modulate cognitive outcome, as has been previously suggested by the cognitive reserve theory. 12,13
The effects of TBI also have been extensively studied with the use of magnetic resonance imaging (MRI). Decades of research have shown that TBI causes significant volume loss in gray and white matter, as well as ventricular enlargement. 14 –17 Past studies also have demonstrated an association between structural changes and clinical measures, such as injury severity, duration of post-traumatic amnesia, and cognitive functioning. 18 –20 Despite this impressive body of work, the associations between structural brain volumes and cognitive performance 21 –23 can and should be improved upon by inclusion of actual pre-morbid cognitive data, allowing a precise quantification of cognitive deficits post-TBI.
In the current study, we made use of a unique database containing results of a primary psychometric rating test performed on all Israeli teens by the Israeli defense forces' (IDF) draft board, which includes assessment of three cognitive domains: verbal abstraction, mathematical reasoning, and non-verbal abstract reasoning. Using this source of actual pre-morbid cognitive performance data facilitated the calculation of the extent of individual cognitive loss in these domains. The present work aims to: 1) examine the relation between long-term cognitive loss and severity of TBI as determined by the Glasgow Coma Scale (GCS), and 2) examine the association between long-term cognitive loss and regional gray matter volume post-TBI.
Methods
Participants
A total of 89 subjects were recruited. Fifty-four TBI patients were recruited from the Neurosurgery department of Sheba Medical Center and 35 healthy controls were recruited from the community to participate in the study. Of these, 24 TBI patients (12 mTBI and 12 moderate-severe TBI [msTBI]) underwent an MRI scan (for characteristics of TBI patients participating in the MRI session, please refer to Supplementary Table 1; see online supplementary material at
mTBI or msTBI vs. Controls. Analysis of variance Bonferroni post hoc, p < 0.05.
RPM-R, Raven's progressive matrices–R; SD, standard deviation; mTBI, mild traumatic brain injury; msTBI, moderate-severe traumatic brain injury.
Inclusion criteria for TBI patients were: 1) subjects (age 18+ years, age at injury <45) who had suffered TBI more than a year prior to enrollment (to allow stability in their neurological and neuropsychological status); 2) availability of medical records of TBI (computed tomography [CT] scan, GCS score at hospital admission, results of neurological examination at the time of injury); 3) CT or MRI scans at admission showing evidence of injury, including cortical or subcortical contusions, brain lacerations, intracranial bleedings (such as subarachnoid hemorrhages), or hematomas (such as subdural hematomas)—thus, both complicated mild and moderate-severe injuries were recruited; 4) moderate disability or good recovery on the Glasgow Outcome Scale (GOS; capable of using public transportation); 5) underwent pre-military cognitive assessment; 6) no TBI requiring hospitalization prior to the IDF assessment; and 7) able to understand and sign a written informed consent form.
Healthy control subjects (males and females, age range 18–45) with similar demographics were recruited from among siblings of the head-injured subjects. Nine of the 35 healthy controls were siblings of TBI patients. In TBI patients with no sibling willing to participate in the study, other controls were chosen from the community, matched by age and gender. Exclusion criteria for both TBI and control groups were: 1) history of significant neurological or psychiatric disorder, and 2) use of alcohol, recreational drugs. Additional exclusion criteria for participants in MRI scanning were claustrophobia and presence of metal in the body. Only one TBI patient exhibited focal brain lesions on his current MRI scan and was thus excluded from the study.
All subjects provided written informed consent prior to participating in the study.
Cognitive assessments and analysis
All participants had performed a first baseline assessment of cognitive performance at age 17 as part of the medical visit and aptitude tests mandated by the IDF's pre-military screening draft board. The draft board psychometric test battery yields a global cognitive score, which is a validated measure of general intelligence, equivalent to a normally distributed IQ score. 24,25
The post-injury cognitive performance assessment consisted of a screening stage with the GOS for eligibility to understand and sign a written informed consent form (equivalent to moderate disability or good recovery on the GOS), with the semi-structured clinical interview of the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition for psychiatric history and substance abuse; and a testing stage of analogous versions of the cognitive tests taken at baseline, namely: 1. The Similarities subtest (from the Hebrew version of the Wechsler Adult Intelligence Scale, Third Edition[WAIS-III]: assesses verbal abstraction and categorization.
26
2. The Arithmetic subtest (from the Hebrew version of the WAIS-III): assesses mathematical reasoning, concentration and concept manipulation.
26
3. The Raven's progressive matrices–R (RPM-R): measures non-verbal abstract reasoning, and visual-spatial problem-solving abilities.
27
Both pre- and post-morbid subtest scores were standardized based on population means and standard deviations. The pre-injury standardization was done according to the norms of the adolescents tested by the IDF, and post-injury standardization was performed using the WAIS-III and RPM-R adult norms. Changes in Z-scores between post-injury and pre-injury cognitive scores (post- minus pre-injury) were calculated for each individual for the three different tests to quantitate changes in cognitive performance.
To assess the influence of the injury severity on the change in cognitive scores, the TBI group was stratified by their GCS 28 scores to mild (GCS ≥13) and moderate-severe injury groups (GCS <13). The post-pre-injury change scores of each of the three cognitive tests were compared using a one-way analysis of covariance controlling for significant differences in pre-morbid baseline cognitive measures. Post hoc analyses (Bonferroni) were then conducted to evaluate pairwise differences among adjusted means.
MRI data acquisition and voxel-based morphometry analysis
Patients were scanned at the diagnostic imaging department, Sheba Medical Center. Scans were acquired on a 3 Tesla whole–body MRI system (GE Signa HDxt, version 16 VO2) equipped with an eight-channel head coil. High-resolution (1 mm3; matrix, 256 × 256; field of view, 25.6 cm) images of the entire brain were acquired for each subject using a standard three-dimensional inversion recovery prepared fast gradient echo pulse T1-weighted sequence with the following parameters: repetition time = 7.3 sec; echo time = 2.7; flip angle = 20°; TI = 450 msec.
The voxel-based morphometry (VBM)
29
procedure was used to analyze the T1-weighted anatomical images for each subject. This procedure included automated iterative skull stripping, segmentation of the images into gray matter (GM), white matter (WM), and cerebrospinal fluid (CSF) probability images, and spatial normalization of the GM images to a customized GM template in standard Montreal Neurological Institute atlas space. The GM maps were smoothed with an 8-mm Gaussian kernel to optimize signal-to-noise and facilitate comparison between participants. Analysis of gray and white matter volume utilized an absolute threshold masking of 0.1 to minimize incorrect inclusion of tissue type. The image processing and statistics were accomplished with VBM extension tools developed by Gaser (
The associations between GM volume, WM volume, and cognitive change scores were assessed using whole-brain multiple linear regression voxel-wise analysis available in SPM8. Cognitive change scores on the RPM-R and Similarities tests were inserted as predictors in the models, while age at assessment and TICV were included as covariates.
Results
Cognitive performance and injury severity
Of the 54 TBI patients recruited, four patients were removed from the study: one due to unavailability of pre-morbid army data, one due to the occurrence of a psychotic episode during testing, and two for no clear finding of TBI in CT scan at admission. In addition, five of the TBI patients, one with mild injury (mTBI) and four with moderate-severe injury (msTBI) had missing pre-morbid data on two tests (Similarities and Arithmetic) due to army data coding errors; and four msTBI did not complete the post-injury RPM-R test due to lack of cooperation. Of the thirty-five healthy control subjects, two had unavailable pre-morbid data on two tests (Similarities and Arithmetic) due to army data coding errors.
The TBI patients' group initial GCS scores ranged from mild (GCS = 13–15, n = 19) to moderate-severe (GCS = 3–12; n = 31). The majority, 55% of the TBI patients, were injured in a motor vehicle accident, 19% were injured in a fall, 12% were injured while engaging in sports, 6% were assaulted, 2% were injured in combat, and 6% had other etiologies. Mean age at TBI was 28.62 (standard deviation, 5.75). The TBI patients' current assessment was performed a year or more post-injury (mean [M] = 35.2; standard deviation [SD] = 17.7 months post-injury) in order to test the TBI patients after the initial period of spontaneous recovery had elapsed and neuropsychological stability has been achieved. 30
The 50 brain-injured patients and 35 healthy controls did not differ significantly in age at assessment or gender (mean[SD] age: controls 28.66[5.38], TBI 31.60[5.91], t = -1.94, p = 0.056; gender [males/females]: controls 32/3, TBI 47/3; X2 = 0.21; p = 0.68). The mean global pre-morbid cognitive performance score of the TBI patients was equivalent to a mean IQ of 98.2 (15.28), while the mean value of the controls was significantly higher (105.03 [14.14]; t = 2.12; p = 0.04; d = 0.46). Controls also exhibited higher baseline performance in pre-morbid sub-tests scores of Similarities and Arithmetic (t = 2.50, p = 0.014, d = 0.58 and t = 2.06, p = 0.043, d = 0.47, respectively). The TBI group was stratified by injury severity (mTBI, n = 19; msTBI, n = 31), showing no differences between the two injury severity groups in age at injury or pre-morbid equivalent IQ scores (mean[SD] age: mTBI 30.32[7.02], msTBI 29.26[6.55], t = 0.53, p = 0.59; pre-morbid equivalent IQ: mTBI 95.06[14.2], msTBI 100.12[15.83], t = −1.17, p = 0.25). An effect on change scores was found for the RPM-R test (F[2,80] = 10.4, p = 0.00), with similar declines evident in the mild and moderate-severe TBI groups (M = −0.54, standard error [SE] = 0.18, d = 0.93; M = −0.59, SE = 0.15, d = 1.05; respectively; Fig. 1, Table 1) relative to healthy controls (M = 0.24, SE = 0.14). More than one half of the TBI patients (57.9% mTBI and 55.5% msTBI) exhibited deficits in the RPM-R cognitive measure defined as a RPM-R change score greater than 1 SD from the mean of the healthy controls. This analysis also revealed an injury severity effect for the Similarities post-pre-injury change scores (F[2,78] = 4.49, p = 0.014, d = 0.517; Fig. 1, Table 1), where the msTBI group had the greatest decline (M = −0.46, SE = 0.14), significantly greater than healthy controls (M = −0.10, SE = 0.13) and the mTBI group (M = 0.19, SE = 0.17). Sixty six percent of the msTBI patients exhibited deficits in the Similarities cognitive measure, defined as a Similarities change score that is greater than 1 SD from the mean of the healthy controls. The Arithmetic post-pre-injury change scores did not differ among groups (F[2,78] = 1.36, p = 0.26; Fig. 1; Table 1).
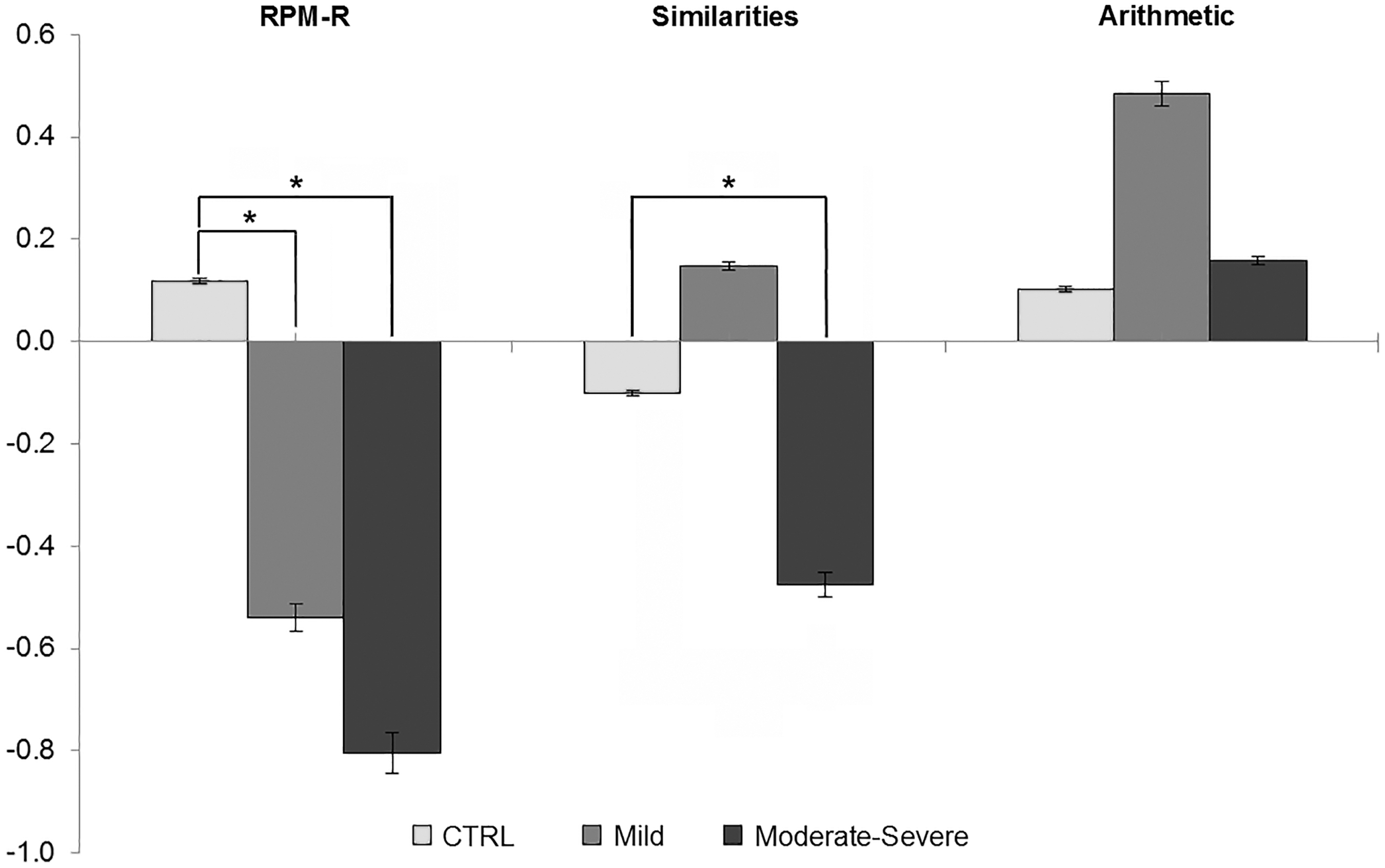
Effect of injury severity on post-pre-injury change score of the cognitive tests. Bars represent mean ± standard error standard error of 19–35 subjects per test. The post-pre-injury change scores were compared using a one-way analysis of covariance controlling for significant differences in pre-morbid baseline on all three cognitive measures. The traumatic brain injury (TBI) group was stratified by their GCS scores to mild and moderate-severe injury groups and compared with healthy controls. Post hoc analyses (Bonferroni) were conducted to evaluate pairwise differences among adjusted means. *p < 0.05. CTRL, control; Mild, mild TBI; Moderate-Severe, moderate-severe TBI.
TBI-related cognitive change and brain volumes
Twenty-four of the TBI patients described above (12 mTBI and 12 msTBI) also had an MRI scan. The 24 TBI patients who had an MRI scanning did not differ from those who did not participate in this procedure on demographic or clinical characteristics (gender, age at assessment, TBI age, post-injury interval, IQ equivalent, GCS group (Supplementary Table 2; see online supplementary material at
VBM analysis revealed a significant positive correlation between RPM-R change scores and GM volume in left and right insular cortices (Fig. 2; Table 2) after adjustment for age at assessment and TICV. A threshold of uncorrected 0.001 and cluster size of 200 voxels was applied. This threshold is equivalent to a corrected threshold of 0.01 according to Monte Carlo simulation implemented in 3dClusterSIm program in the AFNI software package 31 (i.e., the probability to find false positive clusters in this size is less than 1%). Figure 2 shows a maximum intensity projection depicting significant locations in two orthogonal views of the brain (top: coronal; bottom: axial). There was no significant correlation between the Similarities change score and GM volume.
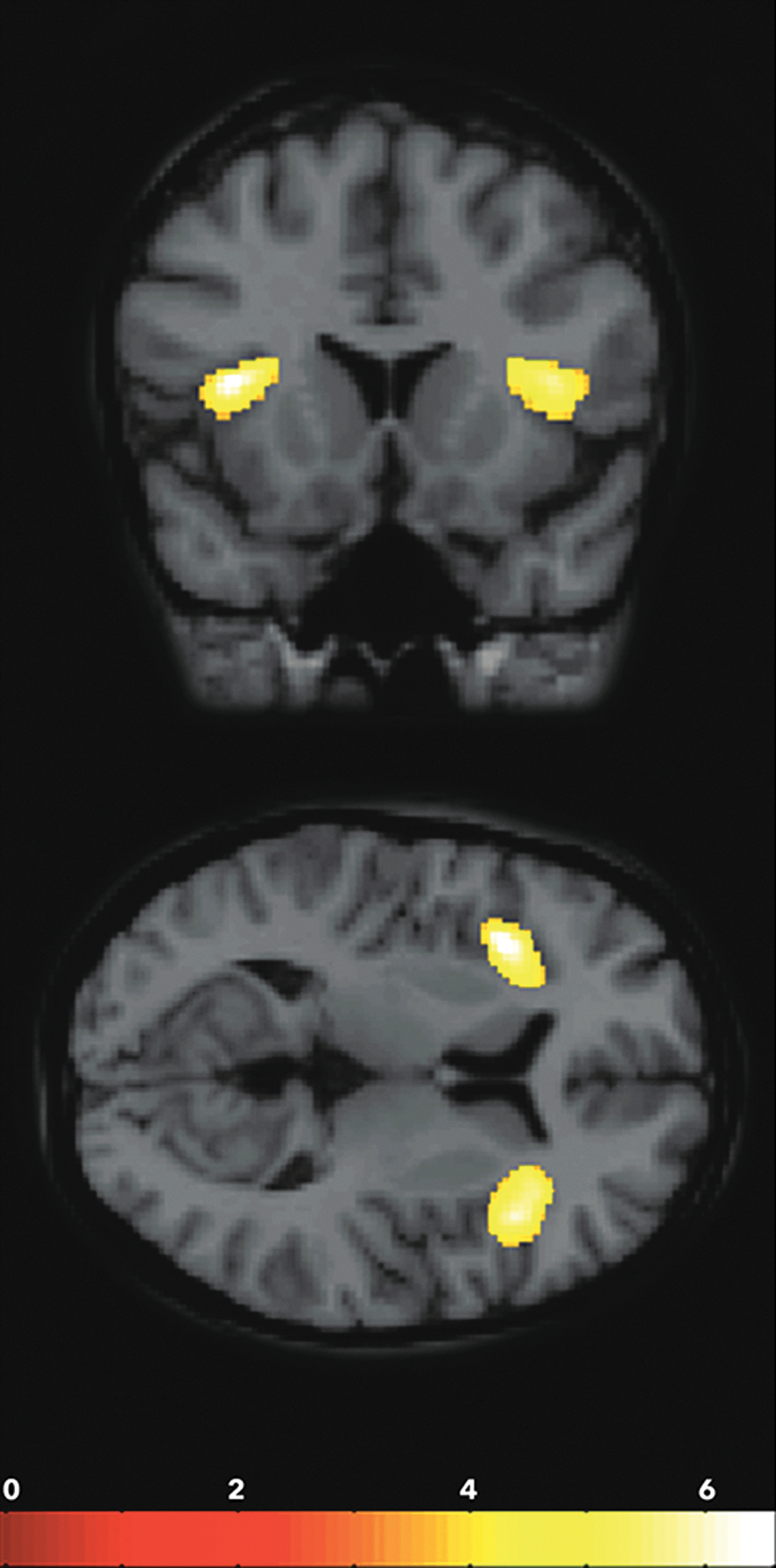
Regression plots of gray matter (GM) volume in insula and Raven's progressive matrices–R (RPM-R) change scores. Locations of significant clusters in which a correlation was found between RPM-R change-score and GM volume (arbitrary units) at a threshold of p < 0.01, K > 200, according to Monte Carlo correction for multiple comparisons, while controlling for age at assessment and total intracranial volume.
All t-statistics are thresholded to a value of 0.01, k > 200, corrected according to Monte Carlo correction.
RPM-R, Raven's progressive matrices–R; GM, gray matter; TBI, traumatic brain injury; MNI, Montreal Neurological Institute.
Discussion
The current study examined the long-term effect of mild and moderate-severe head injury on post-injury cognitive performance following TBI, the effect being defined as the difference between post-injury and actual baseline scores on validated tests addressing three cognitive domains. Our study shows for the first time that mild TBI patients present a decline in non-verbal abstraction abilities (as measured by the RPM-R test). In addition, we support previous publications indicating that severe TBI patients also decline in this measure. 32 We further strengthen previous research reporting differences on verbal abstraction ability (as measured by the Similarities test) between severe TBI and controls and no differences between the mild TBI and controls. 33,34 Finally, we are the first to report an association between decline in non-verbal abstract reasoning measured as a post-pre-injury change score and gray matter volume of insula bilaterally in TBI patients.
Due to our unique ability to access the IDF's database of actual pre-morbid cognitive scores of TBI survivors and healthy controls, we were able to truly quantify the decline in different cognitive domains and to further assess the influence of injury severity on cognitive outcome post-TBI. Thus, our study design overcame the methodological limitations imposed by estimated cognitive change scores or comparisons to populations norms used in the majority of previous studies published in this research area.
Our results indicate persistent domain-specific effects of TBI on cognitive abilities. We found that the extent and severity of cognitive decline after TBI were modulated by injury severity. In particular, our findings indicate a significant dose–response relationship between TBI severity and non-verbal abstract reasoning and visual-spatial problem-solving abilities. The healthy controls did not show any decline in this ability, whereas both the mild and the moderate-severe injury groups showed a decline related to the severity of injury. To the best of our knowledge, only two studies examined the performance of mild TBI patients on the RPM-R test. 32,35 In one study, severe closed-head injury patients demonstrated poorer performance on the RPM test relative to orthopedic control participants and healthy controls 32 similar to our results. Conversely, our results do not correspond to those of Gentilini and colleagues, who reported that in spite of a general trend toward lower performance of the mild TBI patients 1 month post-injury, there was no statistically significant difference between mild head-injured patients and controls on the RPM-R test. 35 In addition, the RPM-R test is often considered to be a measure of general intelligence. 36,37 Hence, our finding that the mildly brain-injured patients present a significant decline in this measure provide a better understanding of the sequelae of mild TBI, as the literature provides conflicting results regarding the cognitive deficits post-mTBI. 5,33,34,38,39 The inconsistencies in the reported long-term consequences of mild TBI are probably due to the fact that subjects suffering from mild TBI are likely to have more subtle impairments that can pose challenges for clinicians without pre-injury cognitive performance test scores, whereas the existence of change in moderate-to-severe TBI may be easier to identify.
We also show that verbal abstract reasoning (measured by the Similarities test) decreased in moderate-severe but not in mild injuries. Our finding supports those of Langeluddecke and Lucas and of Carlozzi and colleagues, who also reported a performance deficit in severe TBI patients relative to controls on the Similarities test. 33,34 The finding of verbal abstraction deficits in moderate-severe but not in mild injuries is interesting in the context of the notion that verbal skills, such as verbal knowledge and reading pronunciation skill, can be used as pre-morbid IQ “hold” tests, 8,40 which are tests in which scores are believed to be maintained after TBI. 9 We assume that moderate-severe TBI patients presented deficits in this domain due to the abstraction aspect, which may present a higher cognitive demand.
Langeluddecke and Lucas 38 also noted that brain trauma had the strongest effect on tasks that tap verbal conceptual abilities and the smallest effect on mathematical reasoning. Mathematical reasoning ability of controls did not differ from that of mild and of moderate injury patients but did differ from that of severely injured patients. 33 Carlozzi and colleagues reported all injury severities differed from controls on this measure. 34 Contrary to those findings, the current study is the first to find that mathematical reasoning did not decrease in either mild or moderate-severe injuries, perhaps due to our unique ability to measure actual cognitive decline based on change scores from pre-morbid performance. If replicated, this result raises the interesting possibility of considering the use of Arithmetic as a test of hold ability.
The selective effect of injury severity on specific cognitive abilities is of great importance for predicting cognitive outcome after TBI. In the clinic, knowing which skills tend to be more vulnerable to the effects of TBI may help choose which specific cognitive sub-tests should be given priority when time constraints or TBl-related attention deficits 41 prevent the administration of a full neuropsychological test battery. An important caveat in this regard is that only the three domains for which we had pre-morbid data were tested, and these did not include all of the domains in which cognitive deficits are reportedly most prevalent post-TBI, such as speed of processing, attention, executive function, and memory. 42,43 This limitation may serve also as a strength of our study given that the tests we did employ are not included in standard cognitive batteries commonly administered post-TBI.
An additional implication of our findings is that knowing whether persistent deficits following TBI are specific or not would provide a more precise prognosis and fine tuning of rehabilitation strategies. In the present study, we also explored the association between cognitive deficits and GM volume. We found significant correlations with insula bilaterally. A substantial body of literature suggests that TBI may induce widespread volume loss of brain parenchyma and disrupted WM connectivity as part of the primary and secondary effects of the injury, which are identifiable via neuroimaging methods. 44 Moreover, previous studies have investigated the association between volumes of specific brain region and performance on cognitive tests. Bergeson and colleagues reported a correlation between frontal and temporal lobe atrophy and deficits in memory and executive function in mild-to-severe TBI patients. 45 Gale and colleagues reported gray matter loss in frontal, temporal, cingulate, subcortical, and cerebellar regions, some of which were correlated with performance on tests of attention and GCS. 46 Levine and colleagues showed that neuropsychological performance in patients with TBI is related to a distributed pattern of volume loss in regions mediating mnemonic and attentional processing. 20 Tests of speeded attention, working memory, and verbal learning were associated with a dispersed volume loss over temporal, ventromedial prefrontal, right parietal regions, and cingulate regions. These studies and others have correlated cognitive performance with GM loss; nonetheless, none of these studies were able to assess the true cognitive decline based on pre-morbid cognitive performance and its association with regional brain volume.
To the best of our knowledge, only one study assessed the association between pre and post-injury cognitive performance scores and high-resolution MRI parameters. 47 In that study, Kesler and colleagues examined the relationship between total intracranial volume and ventricle-to-brain ratio, with cognitive performance obtained before and after injury. Their results suggested that large pre-morbid brain size is a protective factor against the cognitive effects of TBI. However, these authors did not attempt to correlate specific deficits with regional loss of GM volume. In the current study, we report that non-verbal abstract reasoning deficits are significantly correlated with GM volume in insula bilaterally. The insula has anatomical and functional connections with several other cortical and subcortical areas, including the parietal, occipital, and temporal association cortices; the anterior cingulate cortex; the ventromedial prefrontal cortex; thalamus; amygdala; and ventral striatum. 48 A recent review published on the effects of focal insular lesions described multiple disturbances to functions of different levels of complexity, from abnormalities in autonomic mechanisms to impairments on high level cognitive functions. 49 Consequently, several researchers 50,51 have suggested a theoretical model in which the insula is an important node in brain networks mediating and integrating external with internal processes, controlling cognitive function, emotional processing, and behavior. In this context, our results of an association between smaller insula volume and reduction in RPM-R performance is in line with the insula's role as an essential integrating node needed to control high order cognitive functioning as is required by this test. We were not able to find a neural correlate of the decline observed in the verbal abstraction abilities, perhaps due to the small number of patients exhibiting decline, which was evident only in the moderate-severe TBI patients.
Our results are limited due to the fact that the severity of injury was classified only by GCS. Other injury severity indices, such as duration of post-traumatic amnesia and loss of consciousness, were not available for most patients. However, although the prognosis of TBI is correlated between these indices and the more severe injuries, the relationship between milder severity of injury and these indices is not as clear. 30 Consequently, our sample only included patients who presented evidence of brain damage in their initial CT or MRI scan at admission.
Interestingly, the TBI group pre-injury intelligence global score was significantly lower than that of the control group. This could be due to sampling bias but also to low intelligence being a risk factor for TBI. 52 Due to this difference, pre-morbid scores where used as a covariate in our analyses of the effects of TBI. Our results are limited due to the fact that the MRI scanning was performed only on males due to the low incidence of head injury in females both in the population and in our cohort. Future studies should include female participants to elucidate how gender differences influence the neurobiology of cognition in recovery from TBI. Our results also are limited because we recruited only patients who had no more than moderate disability on the GOS and were able to consent; thus, the msTBI participants were not necessarily representative of the entire population of those with moderate-severe brain injury (aphasic patients were excluded). Finally, our MRI sample size was relatively small, although analysis nonetheless yielded a significant negative correlation in a whole–brain regression analysis of non-verbal abstract reasoning with GM volume.
In this article, we used a unique study design in order to examine the effect of head injury severity on cognitive abilities in TBI survivors. Using objectively assessed pre-injury cognitive scores to calculate post-pre-injury change-scores, we found that TBI has a selective effect on specific cognitive skills, as different cognitive abilities were affected to different degrees and modulated by injury severity. Our finding that RPM-R, a measure of both general intellectual ability and executive functioning, declines in mTBI is an exceptional observation. Moreover, this specific deficit was associated with volume loss in bilateral insula, an essential node for many neural networks and in particular for high order cognitive functioning. Finally, specific quantitative morphometric alterations observed with high resolution MRI may reflect actual cognitive deficits and provide substantial predictive value for cognitive outcome post-TBI.
Footnotes
Acknowledgments
We would like to acknowledge the support of the head of the Department of Diagnostic Imaging, Prof. Eli Konen, for allowing us access to the MRI scanner.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.