
Abstract
Hypothermia and decompressive craniectomy (DC) have been considered as treatment for traumatic brain injury. The present study investigates whether selective brain hypothermia added to craniectomy could improve neurological outcome after brain trauma. Male CD-1 mice were assigned into the following groups: sham; DC; closed head injury (CHI); CHI followed by craniectomy (CHI+DC); and CHI+DC followed by focal hypothermia (CHI+DC+H). At 24 h post-trauma, animals were subjected to Neurological Severity Score (NSS) test and Beam Balance Score test. At the same time point, magnetic resonance imaging using a 9.4 Tesla scanner and subsequent volumetric evaluation of edema and contusion were performed. Thereafter, the animals were sacrificed and subjected to histopathological analysis. According to NSS, there was a significant impairment among all the groups subjected to trauma. Animals with both trauma and craniectomy performed significantly worse than animals with craniectomy alone. This deleterious effect disappeared when additional hypothermia was applied. BBS was significantly worse in the CHI and CHI+DC groups, but not in the CHI+DC+H group, compared to the sham animals. Edema and contusion volumes were significantly increased in CHI+DC animals, but not in the CHI+DC+H group, compared to the DC group. Histopathological analysis showed that neuronal loss and contusional blossoming could be attenuated by application of selective brain hypothermia. Selective brain cooling applied post-trauma and craniectomy improved neurological function and reduced structural damage and may be therefore an alternative to complication-burdened systemic hypothermia. Clinical studies are recommended in order to explore the potential of this treatment.
Introduction
T
DC (surgical removal of the part of the skull) is a simple and effective method to lower intracranial pressure (ICP) almost instantly. 4 –6 According to clinical studies, surgical decompression improves intracranial compliance 7 –10 as well as cerebral blood flow 11 –15 and brain metabolism. 16 –19 Positive effects of surgical decompression on neurological recovery have been assured in acute brain ischemia, both in animal studies 20 –24 and in clinical trials. 25 –27 However, data from neurotrauma research remain inconsistent and controversial. In animal studies using the controlled cortical impact and fluid percussion models, DC has been shown to reduce development of contusion and brain edema formation and improve neurological outcome. 28 –30 Nevertheless, when using the murine closed head injury (CHI) model for investigations on the effects of DC, an exacerbation of brain swelling and subsequent neurological impairment was demonstrated after surgical treatment. 31 Interestingly, the latter experimental findings were consistent with the results of the multi-center, randomized, clinical trial of the Australian /New Zealand research group (DECRA), demonstrating that early craniectomy performed on/in patients with sTBI was associated with more unfavorable outcomes. 32
These recent findings confirm the need for an auxiliary treatment alleviating the negative impact of mechanical trauma followed by surgical decompression.
For this purpose, selective brain hypothermia is a promising treatment option.
The positive impact of hypothermia on the damaged brain has been well documented in plethora of studies. In pre-clinical investigations, hypothermia provided a protective effect on sensomotor and behavioral function 33 –38 and led to a significant reduction of post-traumatic mortality. 39 Monocentric clinical trials have as well found a protective effect of mild-to-moderate hypothermia on neurological outcome in TBI patients. 40 –43 Unfortunately, this positive impact could not be confirmed by multi-center, randomized trials using systemic cooling in sTBI. 44 –48 Therapeutic failure was mainly attributed to the serious side effects of whole-body hypothermia, 44 –46,49 including circulatory constrain, increased risk of infection, electrolyte imbalance, and coagulopathy. Targeted brain cooling has been proposed as a reasonable alternative, and several reports have demonstrated feasibility of selective cerebral hypothermia through external cooling, both in animals 50 –60 and patients. 61 –64 Still, it remains questionable whether both treatment modes can be used effectively in combination for TBI patients. The potential of such a dual-mode therapy has been already tested in animals 22,65,66 and humans 67 with focal cerebral ischemia, where it proved to be effective in reduction of both neuronal damage and functional impairment. In a previous study on the feasibility of combined craniectomy and hypothermia treatment using the mouse CHI model, focal cooling reduced edema formation after surgical decompression. 68
In the pre-clinical investigation presented here, the murine CHI model is used again. The main goal of the current study is the analysis of the effects of selective brain hypothermia by craniectomy window on structural sequelae and on neurological outcome.
Methods
Animals and trauma model
All animal experiments were performed with approval by the local authorities, in line with the laws for the protection of animals and by following all institutional and national guidelines for the care and use of laboratory animals.
Male CD-1 mice weighting ∼32 g were acquired from the local animal keeping and breeding facility. Animals were kept under controlled light conditions with a 12-h/12-h light/dark cycle. Food and water were provided ad libitum. Mice were assigned in one of the following experimental groups (n = 8 each group): 1) sham-operated (sham); 2) CHI alone; 3) DC alone (DC); 4) CHI followed by DC at 1 h post-TBI (CHI+DC); or 5) CHI+DC and selective hypothermia maintained for 1 h (CHI+DC+H).
During the following treatments, all mice were kept under general anesthesia by isoflurane inhalation (initial dose 3% in 97% O2, maintenance 0.8–1.3% in 99.2–98.7% O2).
For groups 2, 4, and 5, experimental TBI was induced using a weight-drop device (adapted from Chen and colleagues). 69 Briefly, the animals were placed on a heating pad, and an additional heat lamp was used if necessary. The target core and head temperatures were measured by a rectal probe and a needle temperature probe placed in the right temporal muscle, respectively, and maintained at 37 ± 0.5°C during the whole experiment. After a midline longitudinal head skin incision, the skull was exposed, the head was held manually on the base of the weight-drop device (Laboratory Tools Workshop, Department of Pharmacology, School of Pharmacy, The Hebrew University of Jerusalem, Jerusalem, Israel), and a 75-g weight was dropped from a height of 30 cm on a silicone cone resting on the exposed skull, resulting in focal brain injury to the left hemisphere. For groups 1 and 3 (sham and DC alone), the same procedure was performed without weight dropping. In the CHI+DC and CHI+DC+H groups, unilateral DC was performed 1 h post-trauma as described previously. 31 In brief, a bone flap was created in the parietal and temporal bone using a dental drill. The temporal bone was then removed down to the skull base, and a dura opening over the occipital lobe was created using microscissors and microforceps. Subsequently, the skin was closed using 5-0 polypropylene sutures (Premilene®; Aesculap AG, Tuttlingen, Germany).
In the DC group, the same procedure was performed on nontraumatized brain/skull 1 h after sham injury.
In the hypothermia group (CHI+DC+H), additional selective brain cooling was applied using a CO2-driven cryosurgery device. For selective, controlled cooling of the traumatized area, a cryosurgery apparatus (Erbokryo AE; Erbe Elektromedizin GmbH, Tübingen, Germany) was modified. Primarily, this device is designed for tissue ablation, using extreme cold generated by controlled decompression of pressurized CO2 (Joule-Thomson effect) inside a pen-shaped cryosurgery probe. The described cryosurgery setup and technical principle are presented in Figure 1. By modification of the CO2 pressure regulator, the target temperature could be raised to a level well suited for animal experiments, facilitating cooling instead of freezing (original setting, −45°C; after modification, up to +4°C). 68,70

Setup used for application of focal hypothermia. (
For hypothermia treatment, a 3-mm cooling probe with thermocoupling (Erbokryo AE; Erbe Elektromedizin GmbH) was placed on the skin covering the craniectomized area and then chilled to 4°C. Utmost care was taken in order to avoid compression of the underlying brain in the process of cooling. After reaching the target temperature, consecutive cooling was maintained for 1 h.
After 3 h of anesthesia, the temperature probes were removed, anesthesia was withdrawn, and the animals were put back to their cages and allowed to recover. During animal recovery, additional heating devices were not used (passive rewarming in controlled room temperature environment).
Neurological assessment
Functional status of the animals was evaluated by an observer blinded to the treatment applied. Neurological impairment was measured in terms of the Neurological Severity Score (NSS) and the Beam Balance Score (BBS).
For the NSS, a 10-point version scale adapted from Stahel and colleagues was used. 71 Functional neurological status was assessed based on the presence of certain reflexes and the ability to perform motor and behavioral tasks, such as beam walking, beam balance, and spontaneous locomotion. Animals are awarded 1 point per failure to perform a task (see Table 1).
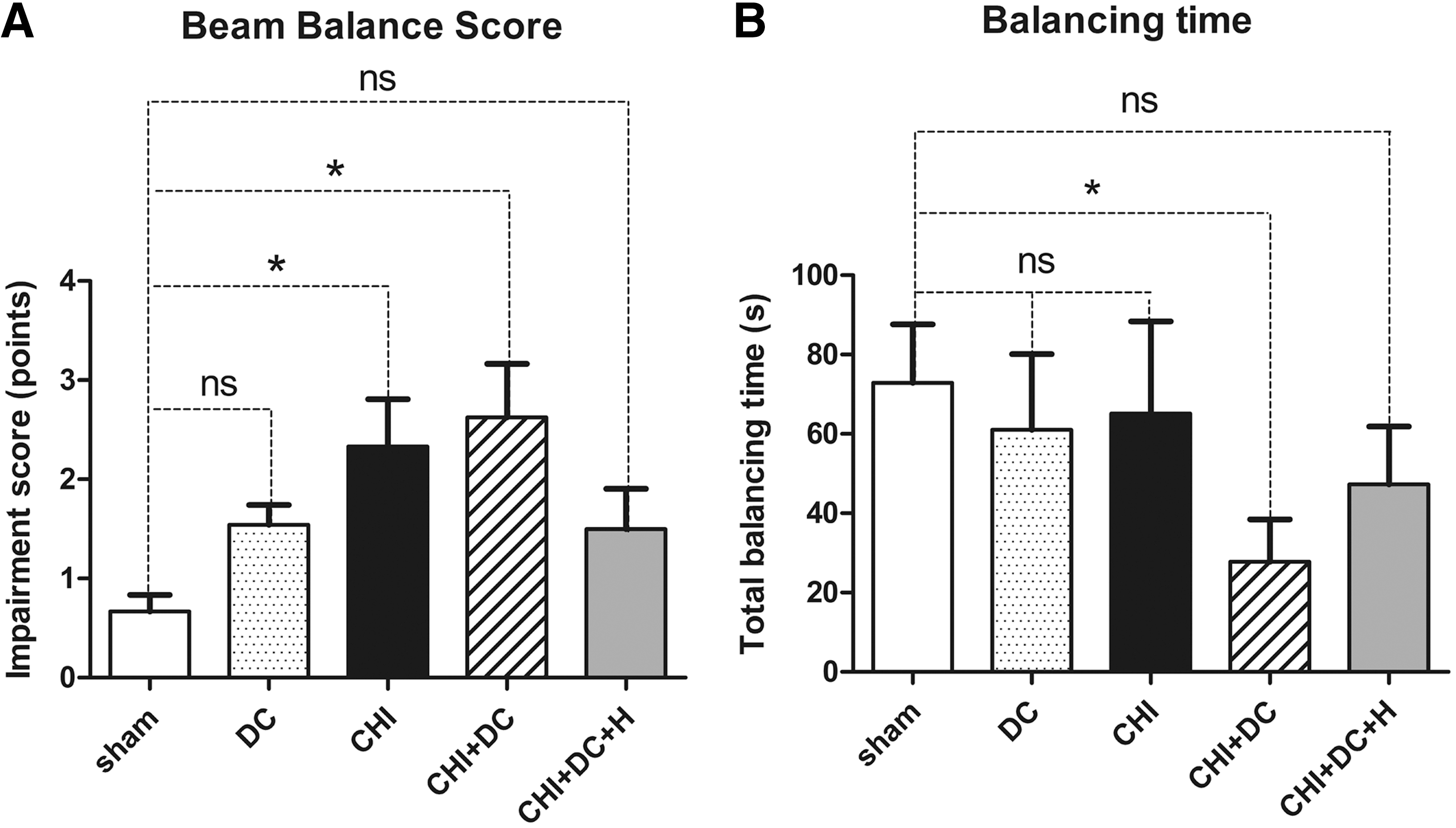
In the BBS, 38,72 performance in balancing attempts is rated from 0 (good performance) to 5 points (not attempting to balance; see Table 2). From three independent tries, the mean score was calculated and used for further analysis. Additionally, the balancing time (maximal 60 sec each attempt) was recorded and analyzed separately.
Each animal is given three attempts of maximal 60 sec each; the performance and balancing time are analyzed separately.
NSS and BBS were assessed at 24 h post-trauma.
Magnetic resonance imaging
Twenty-four hours post-CHI or sham treatment, 5 (n = 5) animals from each group were enrolled in imaging experiments. For magnetic resonance (MR) imaging (MRI), anesthesia was induced after placing the animals in an airtight box, by applying a 3.0%/97.0% mixture of isoflurane and O2 to the spontaneously breathing animals. Anesthesia was maintained by application of a 2.5%/97.5% to 0.8%/99.2% mixture of isoflurane and O2 by a nose cone integrated into the animal support. Respiration rates were recorded by a pneumatic cushion (Graseby infant respiration sensor; Smith Medical Germany, Grasbrunn, Germany), while cardiac rates were collected by electrodes for neonatal humans (3M Red Dot 2269T neonatal monitoring electrode; 3M Germany, Düsseldorf, Germany), both with a dedicated animal montoring system with an external computer and special software (PC-SAM32; SA Instruments Inc., Stony Brook, NY). Temperature was maintained at 37°C by placing the animals on a special tray with an integrated heating system.
MR images were acquired using a system developed for imaging of rodents, with a static magnetic field strength of 9.4 Tesla (T; Bruker BioSpec Avance III 9.4/20 with ParaVision 5.1 operating software; Bruker, Billerica, MA), equipped with an actively shielded gradient (Gmax, 675 mT/m; gradient rise time, 114.8 μs). An actively detuned single-channel volume coil with an inner diameter of 70 mm, a maximum peak pulse power of 1000 W, and a maximum single-pulse energy of 5 Ws served as transmitter (in transmit-only mode). For receiving MRI signals, an actively decoupled pre-tuned phased-array surface coil with 2 × 2 elements designed for imaging of the mouse brain was placed over the skull and centered over the brain midline. After placing the animal in the isocenter of the magnet, a fast low angle shot localizer sequence was performed (field of view [FOV], 3.84 × 3.84 cm2; matrix size = 256 × 256; slice thickness, 1 mm; interslice distance, 0.5 mm; repetition time/echo time [TR/TE] = 100/20 ms; Number of excitations = 2; duration, 25sec 600 ms), generating a set of five subsequent slices in axial, sagittal, and coronal orientation. The symmetry axis of the brain was identified, evaluating the position of the inner and outer parts of the ear and various lobes of the cerebellum and cerebrum. A three-dimensional fast imaging with steady-state precession sequence (FOV, 1.76 × 1.50 × 1.73 cm3; matrix size = 236 × 200 × 23; resulting slice thickness, 0.75 mm; interslice distance, 0.0 mm; TR/TE = 8.0/4.0 ms; number of excitations = 3; duration, 1 min 25 sec 423 ms) in axial orientation was then used to verify correct positioning with symmetric imaging of the brain, and slice geometry data were loaded into standard T1- and T2-weighted MRI sequences and an echo planar imaging technique.
T1-weighted imaging for morphological analysis and planning of T2-weighted and diffusion-weighted image (DWI) experiments were performed with a multi-slice multi-echo technique (FOV, 1.76 × 1.50 cm2; matrix size = 234 × 200; slice thickness, 0.75 mm; interslice distance, 0.0 mm; number of slices = 23; TR/TE = 1000/10 ms; number of excitations = 4; duration, 13 min 20 sec), generating a set of images covering the whole brain.
Matching axial T2-weighted images for identification and quantification of possible hemorrhage were acquired with a turbo spin echo sequence (FOV, 1.76 × 1.50 cm2; matrix size = 234 × 200; slice thickness, 0.75 mm; interslice distance, 0.0 mm; number of slices = 23; TR/TE = 2500/30 ms; number of excitations = 5; duration, 5 min 12 sec).
For accurate quantification of brain tissue inflicted by edema, axial diffusion-weighted echo planar imaging was performed with the following parameters: Field of View 1.92x1.92 cm2, Matrix Size = 192x192, Slice Thickness 0.75 mm, Interslice Distance 0.0 mm, Number of Slices = 7, TR/TE = 2000/18.2 ms, Number of Excitations = 1, Duration 48 s, B Values of 6.45 s mm2 and 786.74, 789.19 and 789.19 s mm2 in sagittal, axial and coronal direction.
Hemorrhage and edema were identified in T2 weighted images and apparent diffusion coefficient (ADC) maps calculated from the DWI data, and matching Regions of Interest were manually created with the ParaVision (version 5.1; Bruker) region-of-interest tool. Resulting size measurements (in pixels and mm2) were exported by a specially adapted macro, and the total volume of the different lesions was calculated from the areas on the single maps and the thickness of the scan slices after importing the data into Microsoft Excel (2003® for Windows XP®; Microsoft Corporation, Redmond, WA) and thereafter into GraphPad Prism® software (version 5.0; GraphPad Software Inc., La Jolla, CA) for further analysis (see Statistical analysis).
Histological analysis
Twenty-four hours post-trauma induction, animals were sacrificed using in situ freezing (n = 5 each group) or transcardial perfusion with buffered formaldehyde solution (n = 3 each group): The snap-frozen brains were dissected from surrounding tissue and serial frozen coronal sections of the brains (12 μm) were obtained and stained with hematoxylin and eosin (H&E) as well as with the Nissl technique; additionally, 3 animals of each group were perfused transcardially with 10% phosphate-buffered formalin; the brains were removed and fixed in the same solution for 7 days. The brains were paraffin embedded and serial coronal sections of the brains (8 μm) were generated and stained the same way as the cryosections (H&E, Nissl). Thereafter, the slices presenting hippocampal area C1 and C3 were identified as the anatomical reference using a stereotactic mouse brain atlas. 73 The coronal section underwent qualitative analysis by an observer blinded to a treatment of the animals, utilizing a light microscope (Olympus, × 40/ × 100/ × 200; Olympus Corporatiopn, YTokyo, Japan).
Statistical analysis
Values of mean oxygen flow and mean isoflurane concentration used during surgery, mean head and core temperature, neurological impairment according to NSS and BBS, balancing time in BBS test, and volume of edema and of contusion calculated from MRI scans were expressed as mean ± standard error of the mean. Comparison of data from different groups was performed using a one-way analysis of variance followed by a post-hoc t-test with Bonferroni correction for individual comparisons.
Given that the lesion volume in MRI scans of sham animals clearly showed non-Gaussian distribution (no lesion observed in all animals), the Kruskal-Wallis test was used for comparison of results of lesion volume determination (edema or contusion).
Significance was set at p < 0.05. Statistical analyses were performed with GraphPad Prism software (version 5.0; GraphPad Software Inc.).
Results
No statistically significant difference was found between the different treatment groups with respect to mean core temperature, mean oxygen flow, and mean isoflurane concentration used during anesthesia.
Continous measurement of head temperature recorded by a probe placed in temporal muscle demonstrated efficient cooling by the cryosurgery device, almost instantly leading to reduction of head temperature to around 32–33°C, without affecting the core temperature recorded by a rectal probe (Fig. 2).
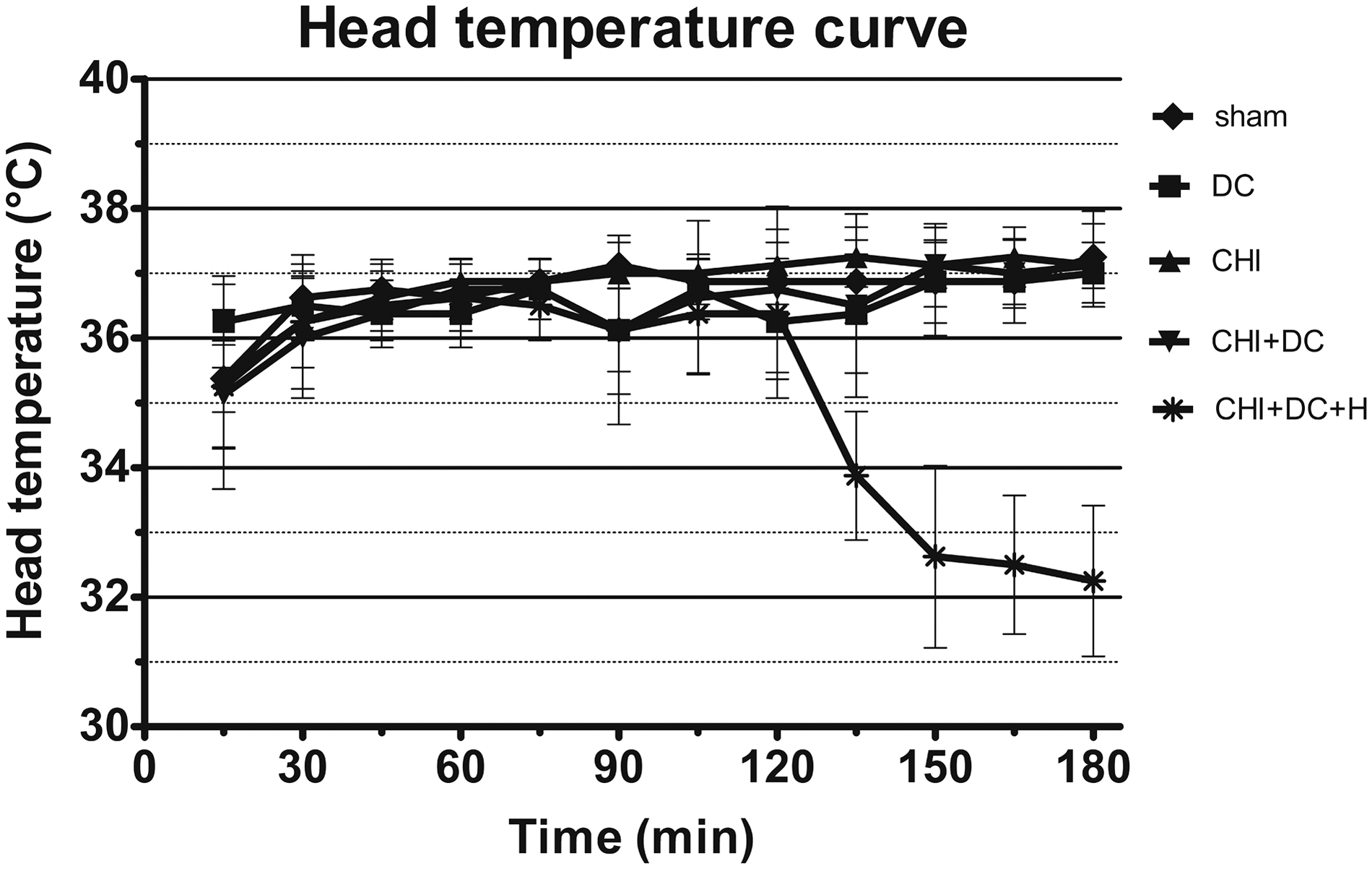
Graph presenting a feasibility of selective brain hypothermia by external cooling of the murine head. The points/bars on the graph present the head temperature (mean/standard deviation) measured in temporal muscle of the side contralateral to decompression/placement of the cooling device probe. The data were sampled every 15 min. Note the drop in head temperature after launching the cooling device (>120 min of the experiment). CHI, closed head injury, DC, decompressive craniectomy; H, hypothermia.
Neurological outcome
The results of assessment of neurological impairment according to NSS and BBS are presented in Figures 3 and 4, respectively.

(
(
All animals subjected to CHI (CHI group, CHI+DC group, and CHI+DC+H group) performed poorer according to NSS when compared to sham group (Fig. 3A). NSS performance of animals subjected to both trauma and craniectomy was worst, given that these animals scored significantly poorer than animals treated with craniectomy only, as reported previously. 31 This deleterious effect of combined treatment disappeared when additional head cooling was applied (no significant difference between DC and CHI+DC+H groups; Fig. 3B).
In BBS, both animals subjected to trauma (CHI group) and to trauma and craniectomy (CHI+DC group) performed significantly poorer than sham animals. This negative effect of brain injury was not present when hypothermia was added to the treatment protocol (Fig. 4A).
Animals subjected to both trauma and craniectomy presented again the poorest performance, when mean balancing time was analyzed. Impairment by craniectomy could be alleviated by additional hypothermia (Fig. 4B).
Volumetric analysis of magnetic resonance imaging scans
Figure 5 shows selected MRI scans from animals with CHI. Figures 6 and 7 display the results of the volumetric analysis of the scans. Given that no brain damage could be identified in MRI scans of sham group animals, the craniectomy-only group (DC) was chosen as the reference group for further analyses.
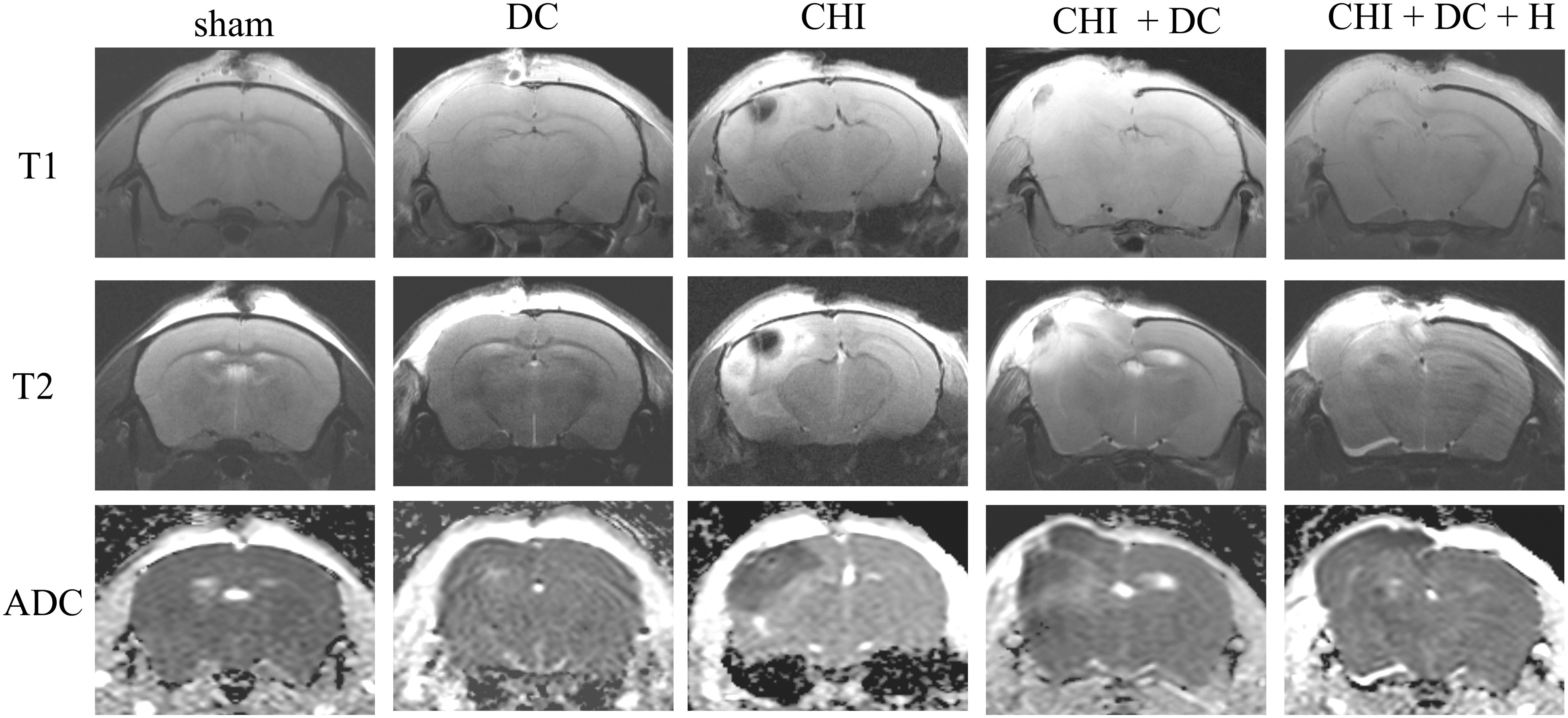
MRI scans from animals subjected to sham injury, DC, CHI, closed head injury followed by decompressive craniectomy (CHI+DC) or CHI followed by combined therapy with craniectomy and subsequent hypothermia (CHI+DC+H). All scans were obtained 24 h post-injury. In the sham group, no structural damage could be discerned. In animals with decompressive craniectomy, there is an area of cortical edema without damage to subcortical structures. Animals subjected to trauma displayed a space-occupying effect of contusion as manifested by slight midline shift. The edema and contusion area reaches the subcortical brain structures. The animals with craniectomy performed post-CHI present the most dramatic brain injury pattern, including massive brain edema and presence of hemorrhagic contusion (reproduced from Szczygielski and colleagues 31 in order to visualize the effect of hypothermia). In animals treated with decompression and hypothermia post-injury, still the diffuse cortical damage can be discerned, however; the subcortical areas are partially preserved. The scans were obtained in representative animals using a 9.4 Tesla MRI scanner. ADC, apparent diffusion coefficient; CHI, closed head injury, DC, decompressive craniectomy; H, hypothermia; MRI, magnetic resonance imaging.

Histogram presenting calculated volume of edema 24 h post-trauma/sham injury according to ADC-weighted scans. No edema was depicted in sham animals; therefore, the craniectomy-only group was used as a reference for further comparison. No difference in quantity of edema was observed between the craniectomy and trauma groups (DC vs. CHI, ns; p > 0.05). Animals subjected to trauma and craniectomy presented more accentuated edema (CHI+DC vs. DC, *p < 0.05). This effect was effaced if additional hypothermia had been used (CHI+DC+H vs. sham, ns; p > 0.05). ADC, apparent diffusion coefficient; CHI, closed head injury, DC, decompressive craniectomy; H, hypothermia; ns, not significant.

Histogram presenting calculated volume of contusion 24 h post-trauma/sham injury according to rapid acquisition with refocused echoes (RARE)-weighted scans. Obviously, there is no contusion in sham animals; again, the craniectomy group serves as a reference group. No difference in quantity of hemorrhagic area between the craniectomy and trauma groups (DC vs. CHI, ns; p > 0.05). The contusion zone is most prominent in the trauma and craniectomy groups (CHI+DC vs. DC, **p < 0.01). Again, hypothermia treatment significantly reduced contusion development (CHI+DC+H vs. sham, ns; p > 0.05). CHI, closed head injury, DC, decompressive craniectomy; H, hypothermia; MRI, magnetic resonance imaging; ns, not significant.
Paralleling the results of neurological assessment, brain edema was most pronounced in animals with trauma subsequently treated by craniectomy. Again, this deleterious synergistic effect vanished when hypothermia was added to the experimental regime (Fig. 6). Also, analyzing contusion volume, the extent of damaged brain was significantly increased in animals subjected to both trauma and craniectomy (Fig. 7), but not in trauma followed by craniectomy and hypothermia (CHI+DC+H).
Histological analysis
As presented previously, 31 according to microscopic evaluation of serial coronal slices, there was no discernible brain damage in sham animals. In animals subjected to craniectomy only (DC), no deep cortical damage or subcortical necrosis could be detected. In a subset of animals from this group, superficial swelling of cortical areas, underlying the area of craniectomy, was observed (Fig. 8, DC).

Photomicrographs of coronal paraffin sections stained with hematoxylin and eosin, obtained from animals subjected to DC, CHI, CHI followed by DC (CHI+DC), and CHI with craniectomy followed by selective brain hypothermia (CHI+DC+H). All animals were sacrificed 24 h post-injury. In the craniectomy group (DC), there is no significant neuronal loss. Animals subjected to trauma present deep cortical lesion and significant neuronal depletion in the CA1 area of the hippocampus. The most massive neuronal loss can be observed in trauma + craniectomy animals. Here, the explicit contusional blossoming with hemorrhagic cortical changes can be distinguished (reproduced from Szczygielski and colleagues
31
in order to visualize the effect of hypothermia). In animals subjected to additional hypothermia (CHI+DC+H), the neuronal loss is restricted to the sporadic appearance of pyknotic neuronal nuclei. Note the significant reduction of hemorrhagic transformation in the contusion zone as compared to the animals without additional hypothermia treatment (CHI+DC). The sections were obtained in representative animals. Panel (
All experimental groups subjected to trauma (CHI, CHI+DC, and CHI+DC+H) presented well-defined cortical and subcortical lesions, surrounded by edematous tissue. In these groups, significant neuronal damage in ipsilateral hippocampus could be documented. The most extensive damage was observed in animals subjected to trauma and craniectomy (CHI+DC), where additional hemorrhagic transformation of contusion, as well as much more widespread cortical and subcortical necrosis, could be identified (Fig. 8, CHI+DC).
Also, histological analysis retrieved impact of hypothermia on structural sequelae of TBI: Although the impact of trauma on the cortical layers was quite the same in the trauma-craniectomy-hypothermia group (CHI+DC+H) and in the trauma-only group (CHI), the contusional area was not hemorhagically transformed as in the similarly treated group without hypothermia (CHI+DC). Moreover, the damage did not reach deep subcortical areas, and (opposite to both other groups with trauma—CHI and CHI+DC) no overt hippocampal neuronal loss could be distinguished (Fig. 8, CHI+DC+H).
Discussion
Our current study showed that focal brain cooling applied post-TBI at the area of DC effectively decreases structural brain damage and improves neurological outcome at 24 h post-trauma. These effects were documented in an experimental setting using a period of hypothermia of only 60 min.
In multiple previous reports, positive effect of hypothermia on post-traumatic outcome has been documented, regarding ICP, 74 –77 lesion volume, 56,78 –80 blood–brain barrier integrity, 81 –83 cerebral perfusion, 77,84 metabolic changes, 85 –87 excitotoxic response, 88,89 inflammatory changes, 60,84,90 –93 cytoskeletal damage, 94 –98 apoptotic process, 99,100 and neuronal loss, 101,102 as well as regarding stimulation of post-traumatic regeneration and neuroplasticity. 103,104 The designs of these studies differed significantly and, in particular, considering duration, level, and form of hypothermia. For our experimental procedure, we used selective cooling aiming at the epicentre of brain injury. 68 The main reason for the choice of local (instead of global) hypothermia was clinical evidence: in large, randomized trials, positive effects of global hypothermia seemed to be deleted by the often serious side effect of whole-body cooling 44,45 that can be life threatening. 105,106
In our experiments, utilizing temperature measurement of the contralateral temporal muscle (which correlates well with cortical temperature 33,107 ), a constant head temperature reduction of around 4°C under the body temperature was documented during applying focal cooling of the injured area. These results are similar to previous studies in rodents documenting feasibility of external targeted brain cooling without decreasing whole-body temperature. 50,108 –112 Still, it has to be mentioned that the thermodynamic properties of the large human head and brain are quite different from the settings in the small rodent experiment. 111,113 Nevertheless, numerous reports have documented the clinical feasibility of external cooling of the human or primate head and at least superficial brain areas. 57,61,62,105,114,115
Despite concerns about spatial and thermodynamic restrictions, cooling of the damaged brain hemisphere through a window within the skull is an enticing experimental treatment option. Nevertheless, previous attempts to combine DC with hypothermia have mainly focused on whole-body cooling. In animal models of stroke, synergistic reductive effects of this treatment combination has been shown for infarct size 22,65,116 as well as for activation of apoptosis 22 and neurological outcome. 65 Results from animal experiments have led to initiation of clinical studies demonstrating improved functional outcome for patients suffering from malignant stroke, treated with both craniectomy and hypothermia. 67 Further, successful clinical application of whole-body hypothermia, added to decompressive craniectomy in neurotrauma patients, has been reported, 117 –120 and the impact of such combined therapy on cerebral blood flow and brain metabolism has been discussed. 118,119
Results of experiments on focal cooling of the traumatized brain have been published by Dvilevicius and colleagues, 121 who used a cortical impact model with cooling of a small area of the brain exposed by skull trephination. Prandini and colleagues have described this combined treatment in a rabbit stroke model, again reporting decreased size of infarction in animals subjected to cooling of decompressed brain. 66 Similar results have been presented by Wang and colleagues, describing improved motor deficits and decreased area of infarction in rats treated by brain cooling and cranial decompression after fluid percussion injury. 112 Also, Kim and colleagues reported efficient treatment with focal cerebral hypothermia analyzed in a canine model, attributing the protective effect to the reduction of secondary damage by modulation of glia activation. 60 Previously, our research group has demonstrated reduction of brain edema formation attributed to focal cerebral cooling in murine TBI/decompression. 68 The main advantage of our experimental setup lies in the animal species utilized: The predominant number of available genetically modified animals is mouse lines; this makes our study paradigm more attractive for basic research on the underlying mechanisms of brain damage.
According to our results, focal hypothermia reduced functional impairment post-TBI. These data are consistent with numerous reports published previously, describing significant improvement of neurological function post-TBI, when animals were treated with whole-body cooling 33 –35,38,122,123 or brain cooling. 103,112,124 Thus far, a narrow time window for effective hypothermia initiation has been expected, given that hypothermia started later than 60 min post-trauma has not yet been shown to provide any neurological improvement. 125 In our study, however, focal brain cooling applied in a delayed manner (2 h post-TBI) for a short period (1 h) was able to significantly reduce the impact of mechanical injury and/or of surgical stress on neurological function. We therefore believe that profound hypothermia applied focally is able to exert its protective effects more efficiently. Moreover, the positive impact of such a treatment is not jeopardized by side effects, as commonly attributed to the use of whole-body cooling (see exhaustive review by Polderman 126 ).
As demonstrated by histopathological evaluation, extent of cortical damage and loss of hippocampal neurones were clearly improved by focal brain cooling. Although a similar impact of different forms of hypothermia on neuronal survival post-TBI has been documented in previous studies (on the subacute phase of brain damage), 101 –103,127 other investigations of medium- to long-term outcome have not demonstrated significant differences in neuronal loss between normothermic and hypothermic groups of animals subjected to trauma. 35,79 In the CHI model, used in our experimental study, the size of structural damage, including the number of affected neurons, correlated well with neurological impairment assessed by NSS and BBS. 69,71,128,129 We therefore conclude that preservation of neurons attributed to hypothermia treatment is, in our experimental settings, the main mechanism protecting brain function.
It must be pointed out that focal cooling also did lead to restraint of secondary structural damage to the brain caused by contusional changes. Both in histopathological analysis and in MRI scans, a consistent pattern of distinct brain contusion, with partial hemorrhagic transformation, was observed. In particular, in animals subjected to post-traumatic craniectomy, a regular contusional blossoming was found, not present when additional hypothermia had been applied. Our observation is strongly supported by results of Kinoshita and colleagues, who reported, in an investigation in rats with fluid percussion injury, a reduced extravasation of hemoglobin in hypothermia-treated animals. 130
Yet another positive effect of hypothermia on the evolution of contusional changes might be associated with prevention of post-traumatic edema. According to current results, as well as to our own previous investigations, brain edema formation can be halted by focal cooling. 68 Similar effects could be documented by other research groups for rat models of traumatic 59 or spontaneous intracerebral hemorrhage, 131,132 as well as in patients suffering from intracerebral bleeding. 133 In these studies, reduced edema formation has been described as a benefit of hypothermia treatment. As a putative mechanism of action, a reduced heme concentration with attenuated hemoxygase-1 (HO-1) upregulation and subsequent reduction of edema formation has been proposed. 59 Previous investigations have demonstrated that overexpression of HO-1 plays a pivotal role in microglia activation and oxidative stress damage in neural tissue in the presence of extravasated blood. 134 –138
Based on published data and our own investigations presented here, we suggest that, in our experimental setting, focal brain hypothermia reduces damage both in very nascent form by restricting contusional bleeding as well as subsequently by inhibition of formation of perifocal edema.
In summary, we demonstrated, by our animal experiments, that selective brain hypothermia may be applied through a cranial window after DC and that this therapy combination seems to be reasonable in reducing post-traumatic structural and functional damage. Our results (yet limited by experimental setup: small rodent model, short observation period) are of great value, given that this treatment paradigm enables hypothermia to exert its beneficial impact on the traumatized brain without causing systemic side effects. Our current report supports further clinical investigations into this promising therapy. It is anticipated that clinical usefulness of focal brain cooling by craniectomy window will mostly rely on the proper selection of the patients treated. An adequate impact of focal hypothermia is rather not to be expected in patients craniectomized for diffuse brain damage, given that penetration of the cooling effect in the relatively large human brain is probably limited to superficial areas. In contrast, patients with early craniectomy performed because of ICP increase attributed to the focal injury (i.e., superficial contusion) would be much better candidates for the focal cooling applied after surgical decompression on the skin covering the damaged area.
The results of our short-term analysis also imply a follow-up study on the long-term outcome of craniectomy and hypothermia as concomitant treatments in animals, which we have already started.
Footnotes
Acknowledgments
We gratefully acknowledge the technical assistance of Ms. Svetlana Beletskaya, Ms. Sonja Hoffmann, Ms. Sigrid Welsch, and Mr. Peter Hidiroglu in the experimental part of the study.
We kindly thank the Erbe Elektromedizin GmbH company for support in providing sketches and images illustrating the physical principles of the cooling technique used (![]() ).
).
This work has been supported by financial award of voluntary association “Friends of Saarland University Medical Center” (for J.S.).
Author Disclosure Statement
No competing financial interests exist.