
Abstract
This study was performed to evaluate clinical biomarkers as prognostic values in dogs with traumatic brain injury (TBI) based on findings in human patients. Sodium levels of 158 dogs with TBI and 169 patients with trauma without involvement of the head except head trauma (EHT) were examined. TBI patients with hypernatremia had a slightly higher risk of dying (22.03 %) than dogs with normal sodium levels (19.76%). However, there was no significant correlation between sodium levels and outcome in TBI patients (p = 0.6357). Dogs with sodium levels >160 mmol/L were non-survivors. In dogs with late-onset post-traumatic epilepsy (PTE) more often hyponatremia was measured, and in dogs with immediate PTE mild hypernatremia or normal sodium levels were measured after the trauma. Evaluation of coagulation parameters in a subpopulation of dogs showed a strong correlation between partial thromboplastin time/prothrombin time (PTT/PT) and the Modified Glasgow Coma Scale (MGCS) (p = 0.0006; p = 0.0306). In conclusion, unlike in human patients, sodium levels displayed no significant correlation with survival in dogs with TBI in the current study. However, in cases with severe TBI, dog owners often elect euthanasia before severe hypernatremia can be measured. Late PTE was observed in cases with initial hyponatremia. Because of a significant correlation between PTT/PT and MGCS, coagulopathy might be considered as a prognostic clinical biomarker in canine TBI patients.
Introduction
T
As a consequence of these injuries, 18–24 % of dogs with TBI die. 8 TBIs can be divided into primary and secondary injuries. 6 The primary lesions include the initial impact and consequences of hemorrhage, axonal injury, bone penetration, or decreased perfusion. 3,6,9 Secondary injuries consist of biomechanical and pathophysiological changes such as oxygen free radical production, adenosine triphosphate (ATP) depletion, or intracellular sodium and calcium accumulation. 5,6,10 A possible consequence of secondary injuries may be a central/neurogenic diabetes insipidus (CNDI) with decreased secretion of antidiuretic hormone (ADH/ vasopressin). 11 CNDI occurs in 15.4% of human patients with brain injury, 12 and may cause hypernatremia in TBI-patients as a result of dehydration, and may evoke further electrolyte imbalances. 13,14 Therefore, studies had already been performed in human medicine evaluating the correlation between severe hypernatremia and death in TBI patients. 14 –16 In human medicine, hypernatremia was found to be an independent risk factor with an extremely high odds ratio for death in patients with TBI. 14 –16 In veterinary medicine, the appearance of hypernatremia as well as hyponatremia were evaluated in patients with different primary disease processes. 17,18 In human medicine, partial thromboplastin time (PTT) and prothrombin time (PT) are currently under evaluation as prognostic factors in TBI cases. 19,20 The aim of this study was to prove a correlation between sodium levels in dogs after TBI and probability of death. In addition, a potential correlation between PTT/PT and the Modified Glasgow Coma Scale (MGCS) should be calculated in a subpopulation of dogs. The hypothesis should be proven that hypernatremia and/or PTT/PT are useful biomarkers in daily routine examinations in veterinary clinics. Further, the opportunity to use the dog as an animal model for human coagulopathy in TBI patients should be discussed.
Methods
In this retrospective study, the clinic program Anidata (Comitas Software, Leipzig, Germany) was used for searching patients with trauma excluding head injuries (EHT) and TBI between 1998 and 2010. Thenceforward, the program easyVet (IFS Informationssysteme GmbH, Hannover, Germany) was searched for the time period between 2010 and 2015. Using these programs, 692 dogs with EHT and TBI could be evaluated.
Patients with TBI (n = 244) were identified using a selection of keywords including:
In EHT patients (n = 448), keywords for inclusion were also
Patients were excluded when results of blood work examination were not available and/or the animals died before a neurological examination could be performed. In total 327 dogs fulfilled all inclusion criteria, 158 for TBI and 169 for EHT.
MGCS was available in 43 dogs based on the data from neurological examinations performed by residents and diplomates of the European College of Veterinary Neurology (ECVN). Only in patients with a complete documented neurological examination at an emergency service was a correct initial MGCS assessable. Evaluation of MGCS was based on the study of Platt and coworkers. 2
Dogs were assessed as survivors when they were sent home alive with a progressively improving clinical status. On the other hand, dogs were assessed as non-survivors when they died in the clinic as a consequence of the trauma.
Electrolytes were analyzed after blood collection in tubes containing lithium-heparin (micro-specimen cup, 1.3 mL, Sarstedt AG & Co., Nümbrecht, Germany) using Siemens RapidLab 1260 (Siemens Healthcare GmbH, Erlangen, Germany). Follow-up examinations of sodium levels were performed. The point in time and schedule depended on clinical development of individual patients. Patients were categorized in different groups according to their sodium levels at initial measurement within the first 24 h after trauma (Table 1). Ranges of sodium levels were based on Small Animal Critical Care Medicine. 21
Coagulation profile was determined by measuring prothrombin time (PT%) and partial thromboplastin time (PTT sec) in 25 selected cases of 43 dogs with available data for MGCS. In addition, in 58 dogs with TBI and 44 dogs with EHT, PT and PTT were measured. In these additional patients, MGCS data were not evaluable. Blood was collected in tubes containing citrate (micro-specimen tube, 1.3 mL, 3.2 % [1:10], Sarstedt AG & Co., Nümbrecht, Germany). PTT and PT were analyzed using the Coagulometer Schnitger and Gross (Fa. Amelung, Lemgo, Germany).
PT and PTT were classified as described in Table 2.
PT, prothrombin time; PTT, partial thromboplastin time.
Development of post-traumatic epilepsy (PTE) in dogs with TBI has already been evaluated. 22 PTE was characterized as described in Table 3. 23
PTE, post-traumatic epilepsy.
To discover the development of PTE, especially the late form, owners of patients that presented before 2009 were interviewed using a questionnaire and telephone interviews.
22
Owners of patients that presented between 2009 and 2015 were interviewed by telephone only, but using the same questions as described before.
22
Questionnaire and interviews included statements relating to the trauma, to occurrence of potential seizures including the time point of first seizure after the trauma, phenotype of seizures, diagnostic workup of seizures, and treatment. For translated questionnaire see supplementary text. (See online supplementary material at
Statistical analysis
All statistical analyses were performed using SAS® Enterprise Guide® 7.1. (SAS Institute GmbH, Heidelberg, Germany). Logistical regression and correlation analyzes were performed. As a statistical significant correlation between hypernatremia and PTE or MGCS, as well as between PTT/PT and MGCS in TBI patients, p < 0.05 was defined. The effect of serum sodium levels in patients with TBI and EHT in comparison with survivors and non-survivors was analyzed using distribution analyses and calculating the odds ratio. Categorical variables are presented as count and percentage. Normal distribution was tested by Shapiro–Wilk and Kolmogorov–Smirnov tests. “Cutoff levels” were recessed with receiver operating characteristic (ROC) curve analyses, and sensitivity and specificity were defined.
Results
Inclusion criteria were met by 327 dogs.
These dogs were divided into two groups. Group I (n = 158 dogs) consisted of patients with TBI and Group II (n = 169 dogs) consisted of dogs with EHT.
Group I (TBI)
Included in this group of 158 patients were intact males (69/158 dogs, 43.67%), neutered males (15/158 dogs, 9.49%), intact females (61/158 dogs, 38.61%) and spayed females (13/158 dogs, 8.23%). The most frequently affected dogs were mixed breeds (41 dogs, 12.54%) and terriers (40 dogs, 12.23%). All affected breeds were divided according to the scheme of the Fédération Cynologique Internationale (FCI) and were represented as shown in Table 4.
TBI, Traumatic brain injury; EHT, except head trauma.
The age of the patients ranged from 3 months to 18 years (mean 3.79 years); 152 (152/158, 96.20%) dogs from this group had sustained a blunt trauma and 6 (6/158, 3.80%) had sustained a penetrating trauma; 79.11% of TBI patients recovered within a median time of 5 days (1–31 days of hospitalization). A total of 33 (20.89%) dogs with TBI died spontaneously or were euthanized. Of these 33 dogs, 20 (20/158 dogs, 12.66%) were euthanized at the owner's request for being in agony or because of poor prognosis. Sixteen dogs were euthanized within the 1st week after trauma and four dogs were euthanized after >1 week after trauma. The other 13 dogs (13/158 dogs, 8.23%) died suddenly within the 1st week after trauma (Fig. 1, Table 5). At initial examination of the 158 dogs with TBI, 13 (13/158 dogs, 8.23%) developed hyponatremia, 86 (86/158 dogs, 54.43%) had normal sodium levels, 48 (48/158 dogs, 30.38%) had mild hypernatremia, and 11 (11/158 dogs, 6.96%) had severe hypernatremia (Table 5).

Survivors (79.11%) and non-survivors (20.89%) after traumatic brain injury (TBI). Non-survivors were divided into dogs that died suddenly (8.23%) or that were euthanized (12.66%).
TBI, traumatic brain injury; EHT, except head trauma.
Dogs with severe and mild hypernatremia had a higher mortality rate than dogs with normal sodium levels or hyponatremia. In these dogs with severe and mild hypernatremia (59/158 dogs, 37.34%) the mortality rate was 22.03% (13 non-survivors/59 dogs). In comparison, dogs with normal sodium levels had a mortality rate of 19.76% (17 non-survivors/86 dogs). However, in TBI patients, the correlation between sodium levels and survival was not significant in logistical regression tests (p = 0.6357) and in correlation analyses (p = 0.6864). Although a significant correlation between sodium levels and survival could not be detected, the mortality was 100% in three dogs with severe hypernatremia (>160 mmol/L) within the first 24 h after trauma. Sodium levels >151.5 mmol/L can be considered as “cutoff levels” between surviving and non-surviving dogs with TBI in the current study (Fig. 2) with a specificity of 83.33% and a sensitivity of 37.50%, and with the highest Youden index. In Figure 2, follow-up examinations of sodium levels are displayed. During the first 24 h after trauma there is a tendency for an increase in sodium levels, which is followed by a decrease to normal levels. Not all patients were measured at all time points, because some dogs either did not survive, or else the clinical status improved dramatically. In these patients, follow-up examinations were not performed.
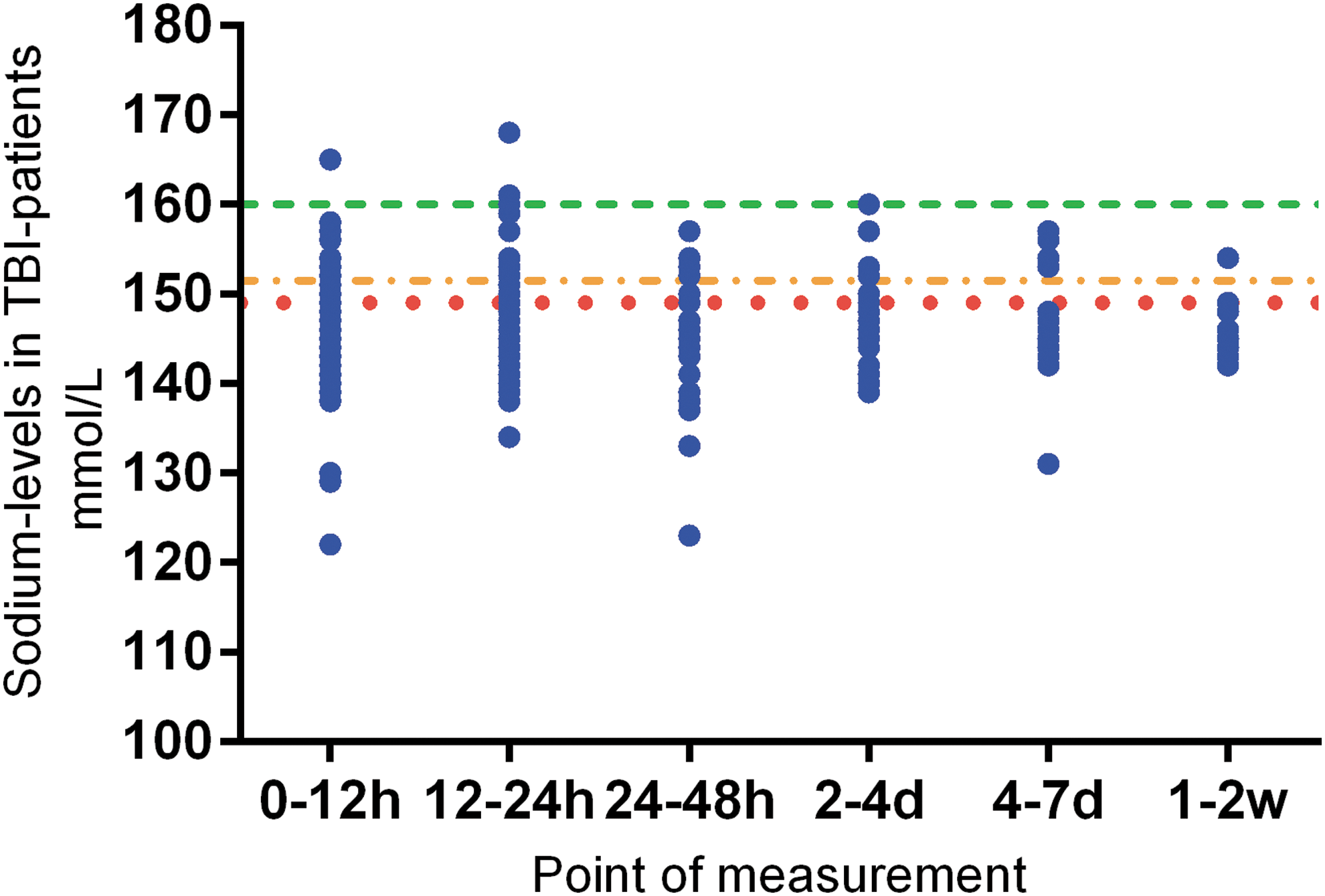
Follow-up examinations of sodium levels in traumatic brain injury (TBI) patients. Measured sodium levels in TBI-patients (blue dots) depended on the time period of measurements. Horizontal red dotted line represents the “cutoff level” for hypernatremia (149 mmol/L). Horizontal green dashed line displays the “cutoff level” for survivors. Dogs with sodium levels >160 mmol/L did not survive. The median value was 146 mmol/L, with a variance between min, 121 mmol/L; and max, 168 mmol/L. Horizontal orange dashed and dotted line displays the specificity and sensitivity with the highest Youden index at the level of 151.5 mmol/L.
PTT and PT were evaluable in 58 TBI patients, in a subpopulation of 25 dogs with TBI and available MGCS, and in 44 dogs with EHT. Within the group of 58 TBI dogs, no significant correlation between PT/PTT and survival could be detected (p = 0.0919). However, the negative correlation between PTT and MGCS was significant (p = 0.0006; r = -0.6583) (Fig. 3a) as was the positive correlation between PT and MGCS (p = 0.0306; r = 0.4515) (Fig. 3b).
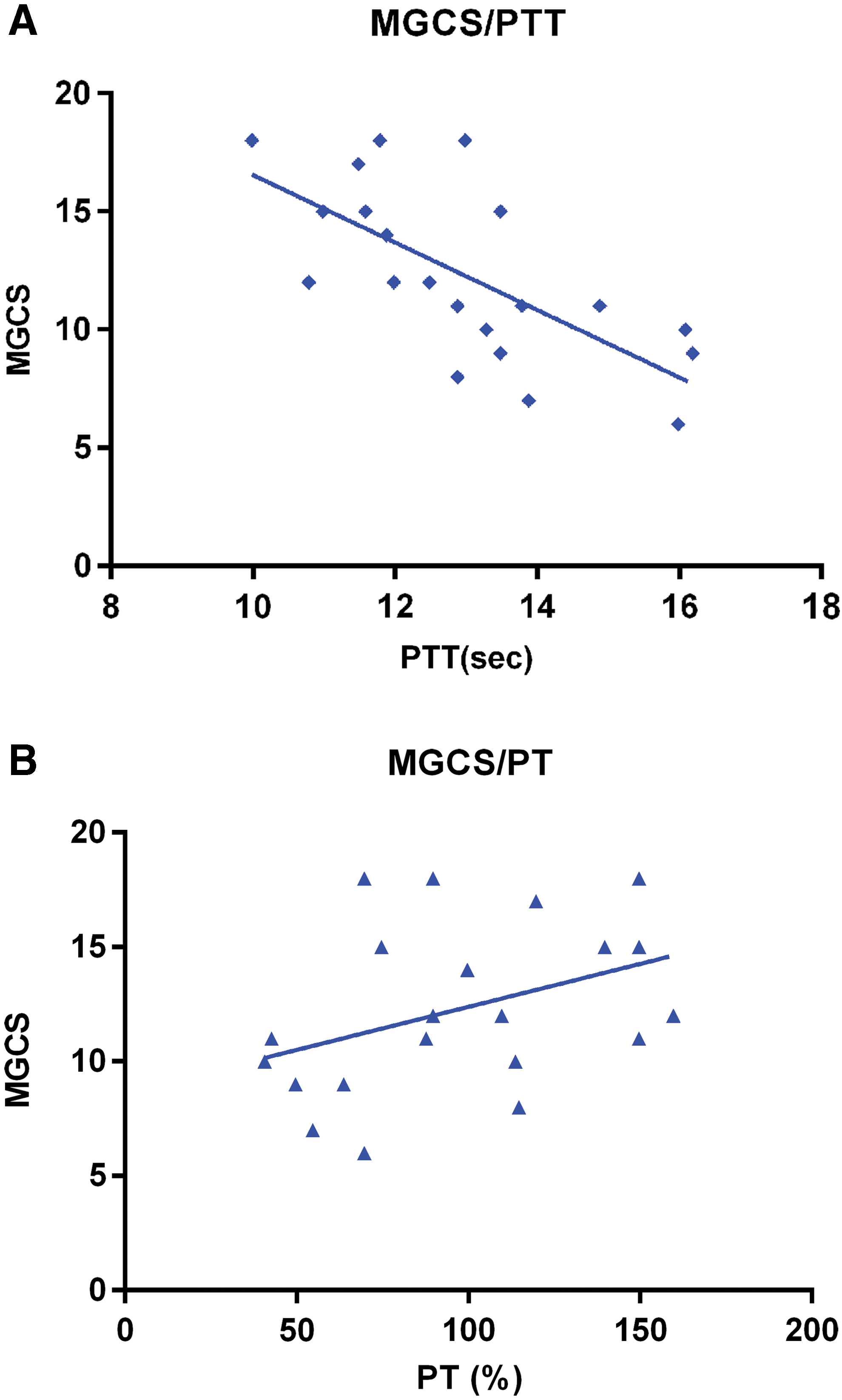
Correlations between MGCS and PTT/PT.
In 33 dogs (33/58 dogs, 56.90%), the PTT was prolonged (Fig.3a). In 15 dogs (15/58 dogs, 25.86%) the PT was decreased (Fig.3b). Twelve dogs (12/58 dogs, 20.69%) had simultaneously prolonged PTT and decreased PT values.
Sodium and coagulation parameters at the initial examination in 58 dogs (58/158 dogs) were not significantly correlated (p = 0.4447).
Evaluation of questionnaires and telephone interviews revealed that 20 dogs (20/158 dogs, 12.65%) developed PTE after TBI. Of those 20 dogs with PTE, 16 dogs developed seizures immediately after the trauma. Only one dog had seizures within the 1st week after trauma, and in three dogs, the onset of seizures was delayed up to 2 years after trauma.
Evaluating this low number of dogs with PTE, more dogs with a late- onset PTE had hyponatremia (2/3 dogs), whereas dogs with immediate seizure onset had normal sodium levels (6/16 dogs) or hypernatremia (8/16 dogs) (Table 3). Dogs with hypernatremia after TBI had no higher risk of developing PTE (p = 0.4520) than did dogs with normal sodium levels or hyponatremia (p = 0.5565).
In 43 dogs, an MGCS was calculated. Only dogs that were initially examined by residents and diplomates of the ECVN were included, to receive comparable MGCS values. The mean of MGCS values was 12.64 (min 6, max 18). The MGCS did not correlate with sodium levels (p = 0.4006) (Fig. 4). In dogs with hypernatremia, the correlation between MGCS and hypernatremia was present but not significant (p = 0.0602)

Distribution of sodium levels and Modified Glasgow Coma Scales (MGCS). TBI, traumatic brain injury; +, mean.
Of 22 dogs with hypernatremia, 3 had an MGCS of 3–8, 12 had an MGCS of 9–14, and 7 had an MGCS of 15–18. In the groups of dogs with normal sodium levels and hyponatremia, only one dog had an MGCS of 3–8 in each group. In summary, dogs with hypernatremia more often had lower MGCS values.
Group II (EHT)
In this group, there were 73 intact males (73/166 dogs, 43.98%), 26 neutered males (26/169 dogs, 15.66%), 58 intact females (58/169 dogs, 34.94%), and 9 spayed females (9/166 dogs, 5.42%) were included. The most frequently occurring breeds were mixed breed dogs (45 dogs, 13.76%) (Table 4). Ages for dogs in this group ranged from 2 months up to 15 years (mean 4.41 years). Fourteen dogs (14/166 dogs, 8.28%) died as a direct result of the trauma. Eight (4.73 %) of these 14 dogs were euthanized at the owner's request because of poor prognosis or being in agony. Within the 1st week, seven of these eight dogs were euthanized, and one dog was euthanized after 9 days (Table 5). The other six (3.55 %) dogs died spontaneously within the 1st week after trauma (Table 5).
In this group of 169 dogs, 12 (12/166 dogs, 7.10%) experienced hyponatremia, 120 (120/166, 71.01%) had normal serum sodium levels, 33 (33/166, 19.53 %) had a mild hypernatremia, and 4 (4/166, 2.37%) developed severe hypernatremia. In comparison with Group 1, dogs did not have an increased mortality rate if they developed severe or mild hypernatremia. Dogs with severe hypernatremia or mild hypernatremia had a probability of dying of 2.70% (1/37 dogs, 2.70%). Dogs with normal sodium levels had a even higher probability of dying (11/120 dogs, 9.17%).
Evaluation of PT and PTT in EHT patients was performed in 44 patients (44/166 dogs). There was no significant correlation between survival and coagulation parameters (p = 0.6299).
Discussion
In the present study, the correlation between serum sodium levels and outcome after TBI was investigated in dogs, as well as the correlation between development of PTE and sodium levels within the first 24 h after trauma. Additionally, the correlation between PTT/PT and MGCS as well as survival and coagulation parameters were evaluated to detect useful clinical biomarkers for the survival odds of patients with TBI.
Comparing breed distributions of TBI and EHT, one obvious difference occurred. In dogs with TBI, terriers were as much represented as mixed-breed dogs (terriers 40 dogs; mixed-breed 41 dogs). Dogs with EHT were mostly mixed-breed dogs (n = 45), whereas other breeds were equally distributed.
One possible reason for overrepresentation of terriers in TBI patients might be the height of the head in relation to the front side of cars, and the independent character of those dogs.
Mortality in TBI patients (20.89%) was higher than mortality in patients with EHT (8.28%). The mortality rate in TBI patients with hypernatremia was slightly higher (22.04%) than the mortality rate in patients with normal sodium levels (19.76%). In contrast, the mortality rate was higher in EHT patients with normal sodium levels (9.17%) than in those with hypernatremia (2.70%). Hypernatremia, most probably caused by CNDI, 13,24 was more common in TBI patients than in patients with EHT as expected. Although dogs with TBI had a higher risk of dying if they developed hypernatremia, this risk factor did not reach the level of significance (p = 0.6357). Additionally, dogs with measured sodium levels >160 mmol/L within the first 24 h after trauma had a probability of dying of 100%. Therefore, sodium levels >160 mmol/L can be considered as “cutoff levels” between surviving and non-surviving dogs with TBI in the current study. However, this statement's limitation is the low number of patients with such high levels (n = 3). Therefore, using the lower “cutoff level” with the highest Youden index of 151.5 mmol/L, specifity only reached 83.33% and sensitivity only reached 37.50%. One explanation for the relatively high mortality rate in dogs with TBI can be the development of a CNDI. In human studies the development of CNDI correlates with a worse outcome in TBI patients. 12 In the study by Ueda and coworkers, a significant correlation between sodium levels and case fatality rates in canine patients with different diseases was shown. 17 On the other hand, Sharma and Holowaychuk could not detect hypernatremia as a prognostic factor in canine TBI patients. 8 In comparison with reports in human medicine, 14 TBI patients in the current study rarely developed severe TBI with MGCS lower than grade of 8, 2 and only 11 dogs with severe hypernatremia were detected (6.96%). The incidence of hypernatremia in human patients ranged between 16% and 40%. 16
Hypernatremia in patients with TBI might be caused by CNDI as a result of primary or secondary injuries of the pituitary gland, pituitary stalk, and hypothalamus. 11 Such injuries lead to decreased secretion of antidiuretic hormone (ADH) of the neurohypophysis or decreased impact of ADH on the kidneys. 11 In consequence, CNDI could be the reason for hypernatremia in patients with severe TBI. 12,24 In mildly or moderately affected TBI patients, the pituitary gland might not be involved in the traumatic brain lesions, and brain edema or hemorrhages do not necessarily cause compression of the pituitary gland. Therefore, probably the sodium levels only correlate with the odds of survival in patients with severe hypernatremia, 15 and, respectively, the development of CNDI correlates with a worse outcome in TBI patients. 12 Despite an originally high number of TBI patients, a relatively small number of patients with severe hypernatremia could be detected in the current study, and such calculations were not possible. Additionally, most probably because of this small number of patients with severe hypernatremia, the correlation between sodium levels and MGCS showed no significance in the described group of patients (p = 0.4006). Interestingly, in one single case with a MGCS of 6, the sodium levels showed a classical development as observed in human medicine in follow-up examinations. The sodium level measured at presentation was 144.7 mmol/L. Twenty-six hours after trauma, the sodium level increased to 168.7 mmol/L and the dog had to be euthanized 30 h post-injury on request of the owners.
As mentioned before, in studies including dogs with TBI, severe TBI cases are not often presented in referral practice because of the high cost of treatment and/or early euthanasia. 25 This might be one reason why only five patients with severe TBI (MGCS ≤8) could be considered in the current study. One further reason for the low number of dogs with severe hypernatremia might be the retrospective nature of the current study performed in a referral clinic. Pre-treatment by local practitioners including different types of perfusion might have affected the electrolyte balance.
In addition to correlations between sodium levels and survival, the correlation between hypernatremia and PTE was evaluated. Although no significant correlation was ascertainable (p = 0.4520), those dogs developing immediate or early PTE more often showed mild hypernatremia or normal sodium levels. Because initial hypernatremia is more common in dogs with severe primary injuries, seizures at this early stage are most probably associated with the primary injury. 23 On the other hand, late PTE is thought to be related to secondary injury. 23 Especially in mild forms of TBI, the long-lasting physical and neuropsychological morbidity is relevant. 26 Therefore, it is also important to prevent possible inflammatory reactions and other forms of secondary injury in mild TBI. 27 In the current study, three of five dogs with late PTE initially developed hyponatremia after trauma. Therefore, hyponatremia should be further evaluated as a potential trigger of late PTE or a biomarker for epileptogenesis secondary to TBI.
The correlation between PTT/PT and MGCS was already discovered in a study in human medicine as a possible prognostic factor needing further investigation. 19 Indeed, data from canine patients in the current study revealed a strong correlation between a prolonged PTT and a low MGCS (p = 0.0006; r = -0.6583), and a moderate correlation between decreased PT and a low MGCS (p = 0.0306; r = 0.4515), but these could only be investigated in a subpopulation of patients (n = 25). Because MGCS is a well-established prognostic factor for canine TBI-patients, 2,8 PTT and PT can be highly recommended for further development as prognostic clinical biomarkers in TBI patients. Although the correlation between survival and altered coagulation profile in TBI patients (n = 58) is statistically not significant (p = 0.0919), the relationship between survival and coagulation is stronger than in EHT patients (p = 0.6299). This finding may support the significant correlation between MGCS and PT/PTT as well as the relevance of the development of a coagulopathy in TBI patients to the emergency service.
The pathomechanisms of coagulopathy in trauma patients include tissue trauma, shock, hemodilution, hypothermia, academia, and inflammation, and they differ from mechanisms described in sepsis or other conditions. 28,29 In TBI patients, consumptive coagulopathy is described 30 and may explain the prolongation of PT and PTT in the dogs described in the current study.
The suggested early platelet dysfunction, especially in TBI patients, remains to date unknown. 20 In one recent study, correlation between a decrease in the ability of adenosine diphosphate (ADP) to activate platelets and a lower survival rate in human TBI patients could be shown. 31 In summary, the most accepted hypothesis implies changes in local and systemic coagulation as well as fibrinolytic pathways secondary to the release of tissue factor (TF), disseminated intravascular coagulation, platelet dysfunction, and activation of protein C pathways secondary to hypoperfusion. 32,33 Until now, there has been no animal model that might show the same platelet dysfunctions as are seen in human TBI patients. 31 Because in a selected number of dogs with TBI in the current study prolonged PTT/PT were detected and a correlation with MGCS was calculated, it might be reasonable to develop the dog as an animal model to investigate the pathogenesis of TBI coagulopathies in future studies. 25
Conclusion
Although hypernatremia did not reach the level of significance in correlation to survival rate, hypernatremia can be recommended as a partial means of determining prognosis in dogs with severe TBI. Dogs with sodium levels >160 mmol/L were non-survivors. Additionally, PTT and PT correlate with the MGCS, and might be useful as prognostic biomarkers in TBI patients. Further, the dog seems to be a good animal model for naturally acquired TBI in further clinical studies investigating coagulopathy. No correlation between PTE and sodium levels could be shown in TBI patients, but late PTE is more common in patients with hyponatremia, which underlines the suggestion that late PTE evolves out of secondary injury whereas immediate and early seizures are more common in dogs with mild hypernatremia or normal sodium levels.
Footnotes
Acknowledgments
We thank Andreas Köppen for technical assistance, and also thank all veterinarians working in the emergency service in the Department of Small Animal Medicine and Surgery.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.