
Abstract
The aim of this study was to evaluate the effect of a continuous locomotor training on leg muscle electromyographic (EMG) exhaustion during assisted stepping movements in a patient with motor complete spinal cord injury (SCI). EMG exhaustion and loss of potentials starts to develop in untrained patients at ∼6 months after injury. In the trained patient examined in this study, exhaustion was also observed but occurred with a delay of several months. In contrast to an untrained patient, no more EMG exhaustion was observed in the very chronic stage. At this time (12 years after injury) a basic locomotor pattern of leg muscle activity of reduced amplitude could still be elicited, but it was resistant to exhaustion and unchanged in amplitude after 12 min of assisted stepping. It is suggested that fatigue-resistant motor units prevail at this stage and can still be activated during stepping as a result of the training.
Introduction
I
These observations might have consequences for future regeneration-inducing therapies, as these can only have a beneficial effect on walking ability if the function of the lumbar neuronal centers below the level of the lesion is preserved. Training of spinal neuronal circuits including an enhanced proprioceptive input might slow down the development of a neuronal dysfunction after SCI. 7 To obtain more insight into these mechanisms, the effect of a continuous locomotor training in a motor complete SCI patient was evaluated. The aim of this communication is to show to what extent exhaustion of leg muscle EMG can be prevented in chronic motor complete SCI patients.
Methods
The study conformed to the Helsinki Declaration and was approved by the local ethics committee. Two individuals with traumatic motor complete SCI were included after giving written informed consent. Characteristics of the patients are shown in Table 1. Patient 1 trained in a DGO (Lokomat, Hocoma, Switzerland) for >12 years starting 11 months after injury. One training session was conducted every week. The patient walked in the Lokomat for ∼30 min at a speed of 2 km/h with 65–80% BWS. EMG activity during walking was measured multiple times over the years. Patient 2 had no locomotion training and leg muscle EMG activity was recorded only once 12 years after injury. The two patients were typical motor complete SCI patients. They were already included in a greater sample of motor complete patients, showing leg muscle EMG exhaustion during Lokomat stepping. 2,3
Level of lesion: T, thoracic level; American Spinal Injury Association Impairment Scale (AIS) classification: A, sensorimotor complete, B, motor complete, sensory incomplete.
All assessments were conducted at 2 km/h and 70% BWS. EMG was recorded from the biceps femoris (BF), rectus femoris (RF), gastrocnemius medialis (GM) and tibialis anterior (TA) of the right leg using surface electrodes. Heel strike was used to trigger the EMG signals for averages over a step cycle. All EMG data were processed and analyzed using Soleasy (ALEA Solutions GmbH Software & Instrumentation, Switzerland). Offset correction and high-pass filter 10 Hz and low-pass filter at the Nyquist frequency was applied. A total of 350 steps starting from step 11 on were used for quantitative analysis. Root mean square (RMS) was calculated for each muscle over the first and the last 10 steps of these 350 steps after rectifying the signal. The difference was calculated as percent of the RMS of the first 10 steps. For illustrating purposes, the RMS of each step in each muscle was calculated after rectification, and normalized to the RMS of the first step. Then a moving average with a window of 25 steps; that is, ∼1 min of walking, was applied to these data to account for step-to-step variability. Noise level of the EMG was calculated as RMS between 30 and 20 sec before the first and 20–30 sec after the last step. The technique used for the evaluation of the RMS decrease of leg muscle EMG during Lokomat training over time after SCI has already been established. 2,3
Results
Patient 1 reported profiting from the training program in that he experienced less spastic muscle tone and fewer spasms, better bowel function, and an improved circulation after training sessions.
Figure 1 shows EMG activity of the right leg of this patient 1 year (Fig. 1a), 2 years (Fig. 1b), and 12 years (Fig. 1c) after injury, respectively. Four steps are shown each after 1 and after 12 min of assisted walking in the Lokomat. One year after injury, an almost “normal” pattern of leg muscle activation could be recorded without a major change over 12 min of walking (Fig. 1a). However, the activation was too weak to generate any mechanical effect. A modulated EMG pattern was preserved in BF, RF and GM muscles 2 years after injury. However, compared with the pattern 1 year after injury, there was a loss of potentials in all muscles. After 12 min of assisted stepping, a marked exhaustion of EMG activity took place (Fig 1b). Twelve years after injury (Fig. 1c), only BF and GM showed a gait-phase-related EMG activity at the beginning and after 12 min of assisted walking. RF and TA EMG activity could not be elicited any more. BF and GM modulation was markedly reduced compared with 1 year after injury. In contrast to the untrained patient, no more EMG exhaustion could be seen.
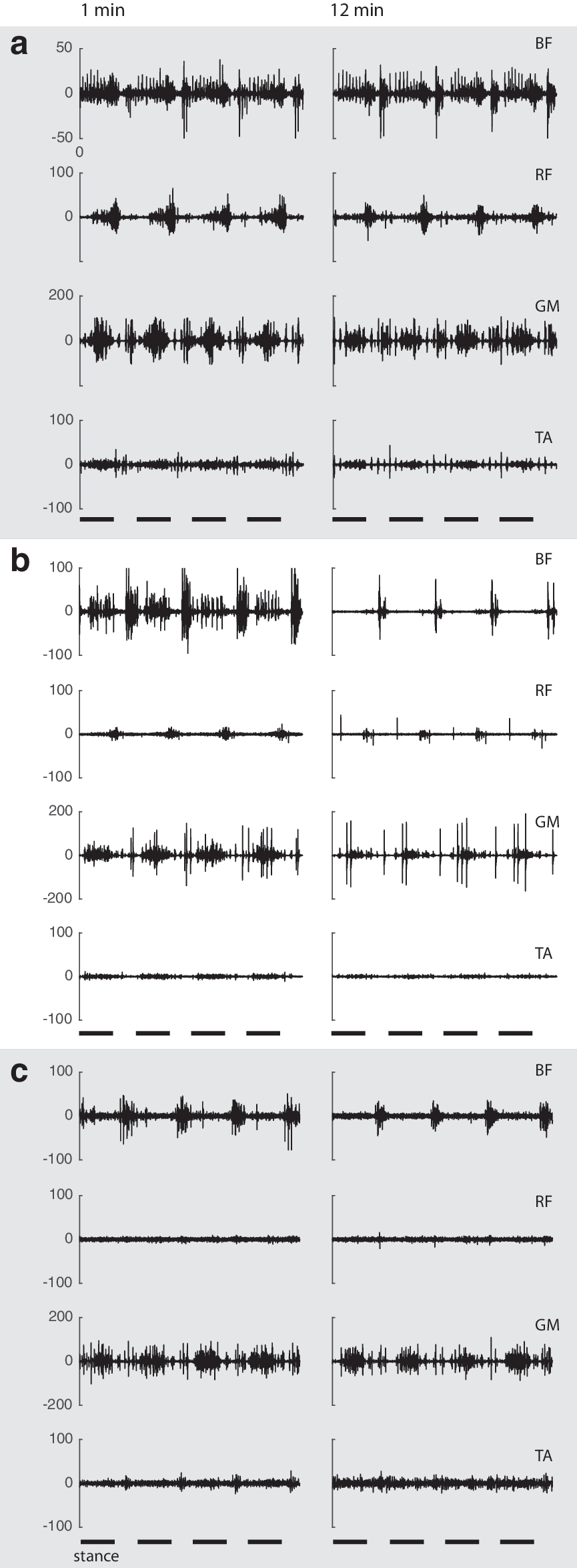
Course of locomotor electromyographic (EMG) activity after motor complete spinal cord injury (SCI). EMG recordings of right leg muscles from a patient with motor complete SCI after 1 min (left side) and after 12 min (right side) of assisted walking in a driven gait orthosis. EMG recordings were taken 1 year
Figure 2 shows the normalized RMS BF and GM values over the course of 350 steps from the trained (1) and untrained (2) patients taken 12 years after injury. Whereas the RMS of Patient 1 (black line) stays between 80 and 100% of the first step throughout the measurement, Patient 2 (gray line) shows a drop to ∼40% of EMG activity in both muscles. This EMG exhaustion occurred faster in BF, where a plateau corresponding to noise level was reached after ∼75 steps; that is, after 3 min. The GM activity did not reach noise level but dropped markedly. For quantified values of EMG exhaustion of the trained (Patient 1) and the untrained (Patient 2) subjects see Table 2. Values are only shown for BF and GM, because only these muscles produced a modulated EMG activity in all assessments.
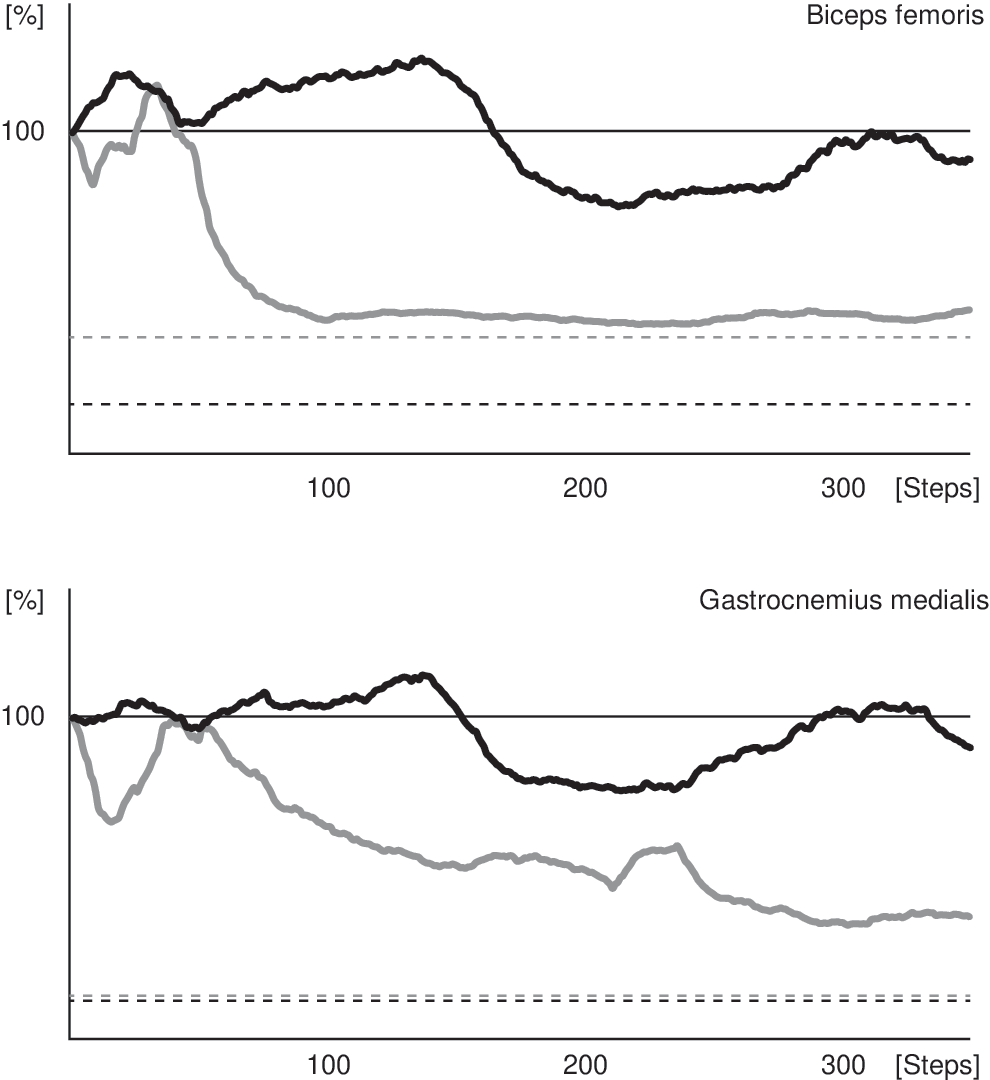
Effect of locomotion training on electromyographic (EMG) exhaustion. Course of relative root mean square values of EMG activity over 350 steps of assisted walking in a patient with locomotor training over 12 years (black traces) and an untrained patient 12 years after injury (gray traces). Dashed lines indicate noise levels of the biceps femoris and gastrocnemius medialis EMG recordings of the two patients.
Relative difference of root mean square between the beginning and the end of the EMG assessments over 12 min of assisted stepping are shown for the right biceps femoris (BF) and gastrocnemius medialis (GM).
Discussion
The aim of this study was to evaluate how far a continuous stepping training can prevent or slow down the development of dysfunction of locomotor neuronal circuits below the level of a motor complete SCI. A phase-dependently modulated EMG pattern can be induced during locomotion years after a motor complete SCI; that is, the neuronal circuits underlying locomotion remain preserved.
The presence of leg muscle EMG activity depends on the presence of appropriate afferent input during stepping, essentially signals from hip joint and load receptors; that is, contact forces of the foot sole with the ground. 8 However, after ∼6 months after injury, an exhaustion of EMG activity occurs during assisted stepping that is more pronounced in the flexor than in the extensor leg muscles. This means that during a training session, the EMG activity drops down in amplitude within the first minutes of stepping. This remains unchanged over many years after injury. 3
The EMG exhaustion phenomenon shown in Figure 1b might be attributed to EMG variability. However, the recordings from motor complete SCI patients showed a low variability, and over longer recording times, we never observed an increase of EMG activity during a successive training session. 3 In addition, the session to session variability of EMG activity in the lower leg muscles during gait has been shown to be low. 9
The fact that the EMG exhaustion concerns the leg flexor muscles more than the extensor muscles is suggested to be the result of differential neural control of different leg muscles. 3,10 During stepping, leg extensors are mainly activated by proprioceptive input that is still present in motor complete SCI subjects. In contrast, leg flexor muscles are controlled more centrally. This central control gets lost after motor complete SCI.
Further, a loss/reduction of activity takes place that was suggested to be the result of a transsynaptic degeneration of motoneurons. 10 The exhaustion phenomenon was assumed to be the result of an imbalance between excitatory and inhibitory signals to the neuronal circuits; that is, a loss of excitatory proprioceptive drive while centrally programmed inhibitory influences on spinal neuronal circuits prevail. Consequently, continuous locomotor training might prevent or delay the development of EMG exhaustion. This view is supported by rodent experiments showing that when an appropriate proprioceptive input is provided by regular training, a directed sprouting of axons deprived of their supraspinal control occurs. However, without such an input, an undirected, chaotic sprouting takes place. 11 The latter situation might reflect the development of neuronal dysfunction in wheelchair- bound human chronic SCI subjects.
In this study, a motor complete SCI subject was continuously trained in a DGO. One year after injury, the patient showed a modulated EMG pattern in all four leg muscles without exhaustion. This is not fully in line with the usual development of EMG exhaustion after motor complete SCI, which occurs at ∼6 months after injury. 2 However, training started only shortly before the measurement, and the delay in the development of EMG exhaustion might not have been solely the result of training. Two years after injury, in the same patient, an EMG exhaustion as well as a loss of EMG potentials was seen to a similar extent as described for untrained motor complete SCI subjects. 3
Although the present observations are based only on recordings from one patient, they indicate that regular, continuous training delays but does not prevent the development of neuronal dysfunction and a loss of EMG potentials. This might be primarily because a training of short duration performed weekly is not enough to provide sufficient excitatory drive to the neuronal circuits to bring them in balance with the inhibitory drive. In addition, because of the specific condition of unloading during assisted stepping movements, less proprioceptive input is produced. In contrast to the untrained patient, no more exhaustion of EMG activity was observed during the assisted stepping movements of the trained patient when assessed 12 years after injury. Both the trained and untrained patient showed EMG activity in the BF and the GM, but no more activity in the RF and the TA. However, whereas the EMG activity recorded in the untrained patient exhausted shortly after beginning of training, as described for other untrained motor complete subjects, 3 the EMG of the trained patient stayed at the initial level. One might argue that because of the regularly performed training sessions, a pattern of fatigue-resistant motor units becomes established and persists over the time of training. 12
The development of neuronal exhaustion might alternatively be the result of centrally induced synaptic changes that can hardly be compensated for by the provision of an appropriate proprioceptive input. It is known that after a motor complete SCI, centrally driven neuronal changes occur, such as the remote transsynaptic degeneration of motoneurons. 10,13 This most probably accounts for the loss of EMG potentials. However, this mechanism could also contribute to the development of neuronal dysfunction after an SCI. Therefore, in chronic SCI patients at present, interventions to induce spinal cord repair might be hampered in their success by the presence of neuronal dysfunction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.