
Abstract
Spinal cord injury (SCI) is believed to be associated with high rates of cognitive impairment, which can result in complications in recovery. This study concerned two groups of adults with SCI. The first sample involved 150 participants with SCI who were assessed once for cognitive capacity with comparisons made with 45 able-bodied adults. Sample 2 were drawn from Sample 1, and included 88 participants with SCI who were prospectively assessed for mood states (anxiety, depressive mood, and fatigue) and pain intensity at three time periods: at admission to SCI rehabilitation, at discharge, and 6 months after transition into the community. Results showed that the SCI sample had significantly lower cognitive performance than the able-bodied control group. Further, almost 29% of the adults with SCI had lowered cognitive performance believed to be indicative of cognitive impairment. The risk of an adult with SCI having cognitive impairment was almost 13 times that of someone without an SCI. Results from Sample 2 revealed that the development of negative mood states was a significant problem in those with cognitive impairment after they transitioned into the community, a time when personal resources are severely challenged. Findings suggest all adults with SCI admitted to rehabilitation should receive a cognitive screen, and that rehabilitation strategies should then be guided by the cognitive performance of the person. Special attention should also be given to improving skills of those with cognitive impairment before they transition into the community, so as to reduce risk of comorbid mental health problems.
Introduction
S
Studies have shown that cognitive impairment is prevalent in the SCI population, 6 –13 perhaps being as high as 60%. 11 Commonly reported cognitive deficits include poor attention and concentration, disturbed memory and learning, impaired visuospatial perception, and decreased problem solving ability. 6,9,10 Comorbid traumatic brain injury (TBI) is a common cause of cognitive impairment in people with SCI, 7 –9 and this is problematic, as TBI is most likely underdiagnosed in people with SCI. 8,9 Factors other than the presence of a TBI also contribute to cognitive impairment in SCI, and these include pre-injury learning difficulties and/or head trauma, fatigue, chronic pain, taking multiple medications, alcohol and substance abuse, and older age. 6 –10,13,14 Further, studies have generally failed to investigate for the presence of depression which has also been linked with reduced cognitive performance. 15
It is known that traumatic SCI is associated with widespread post-traumatic inflammation that results in repair as well as neurodegeneration. 16 –21 For example, recent research conducted on mice indicated that the neuroinflammation associated with SCI results in neuronal loss, disturbed cellular function through increased endoplasmic reticulum stress, and impaired neurogenesis in areas associated with cognitive decline and depression. 17 An implication of this research is that a degree of cognitive impairment may be triggered or exacerbated by this pathophysiological mechanism, which may also play a role in increased psychological morbidity. 15,16 –21 Elevated levels of depressive mood states have been found in the chronic SCI population, with rates ranging between 19% and 30%; 14,22 –24 chronic fatigue is estimated to range from 30% to 50%, 4 whereas alcohol and drug abuse is estimated to be prevalent in up to 16% of the SCI population. 14 However, Davidoff and colleagues showed that neuropsychological performance was weakly related to depressive mood, 25 although they only assessed depressive mood once using a cross-sectional design 8 weeks after the injury.
A major aim of the present study was to determine rates of cognitive impairment in a sample of people with chronic SCI, with comparisons with an able-bodied (AB) control. A second aim was to determine how mood states vary from admission, through discharge, and after transitioning into the community in those with cognitive impairment compared with those with normal cognitive performance. It was hypothesized that the SCI sample would have significantly poorer cognitive performance than the AB group. It was also hypothesized that cognitive impairment would be associated with elevated depressive mood, anxiety, and fatigue, especially after transitioning into the community where there is less support and substantial social and physical challenges.
Methods
Participants
Two samples of participants with SCI were recruited. Sample 1 (n = 150) was recruited to determine the influence of SCI on cognitive performance. Sample 2 (n = 88), a subgroup of Sample 1, was recruited to determine how mood states vary in those with cognitive impairment after transitioning into the community. Inclusion criteria for both samples consisted of: 1) the presence of an SCI; 2) a recent first-time admission to an SCI unit, a readmission to an SCI unit as an inpatient, or review in an SCI outpatient clinic; 3) being 18– 80 years of age at the time of interview; 4) having sufficient cognitive capacity to complete the questionnaires; and 5) speaking English. Exclusion criteria included the presence of severe TBI and/or severe psychiatric disorder that prevented the person from participating (e.g., florid schizophrenia or bipolar disorder with severe manic episodes). The study was in full compliance with the Code of Ethics of the World Medical Association, and research ethics approval was granted by the local institutional human research ethics committee. Written informed consent was obtained for all subjects prior to their participation in the study.
Sample 1 participants (n = 150) were recruited between 2010 and 2014 and had a mean age of 46.2 years (SD = 18), 76% were male, all participants had a mean 12.7 years of education (SD = 2.5) and a mean 3.4 years (SD = 8.7) post-injury, 54% had a partner, 58% had a tetraplegia, 47% had a complete lesion, and 10.4% sustained their SCI through nontraumatic causes. To make comparisons of cognitive performance, 45 AB adult participants were recruited from the community by convenience sampling between 2012 and 2014. The control sample had a mean age of 48.9 (SD = 19), 84% were male, they had a mean 13.6 years of education (SD = 2.2), and 59% had a partner. The control sample was not significantly different from Sample 1 in age, years of education or having a partner, or for the proportion of males.
Sample 2 consisted of a subgroup of Sample 1. This sample included 91 adults with SCI who agreed to participate and who met inclusion and exclusion criteria and who were admitted with a recent acute SCI to one of the three SCI units in Sydney, Australia over the 32 month period of the study between April 2010 and December 2012. In addition to these 91 participants, a further 170 individuals were also admitted to the SCI units over the same time period. Of the 170, 10 had severe TBI; 17 were >80 years of age; 66 had a very incomplete SCI or were ambulant, or were not in the rehabilitation unit long enough to participate in the study; 10 were showing symptoms of severe schizophrenia or bipolar disorder and were unsuitable for the study; 5 had a history of multiple suicide attempts and deemed unsuitable for the study; and 2 had dementia. The remaining 60 did not consent to participate for a number of reasons, including not being well at the time of interview because of serious disease (e.g., hepatitis C, cancer), not being interested, being too busy with conflicting rehabilitation tasks at the time of interview, or not speaking sufficient English to understand the questionnaires. These 60 were not significantly different in mean age, sex ratio, or length of stay in hospital from the study participants; however, the percentage of people with paraplegia was marginally higher (67% compared with 54% in the study sample).
Of the 91 participants who agreed to participate, 1 died soon after admission to the study and 2 chose not to continue in the study, resulting in Sample 2 having 88 participants who were assessed longitudinally. Figure 1 shows the recruitment and dropout details for Sample 2. Figure 1 shows that 7 participants did not complete the discharge assessments (therefore a total of 81), and a further 10 did not complete the 6 month community assessment, leaving a total of 71 participants. Sociodemographic and injury characteristics for Sample 2 are shown in Table 1. Completeness of the lesion was assessed by a medical specialist based on International Standards for Neurological Classification of SCI (
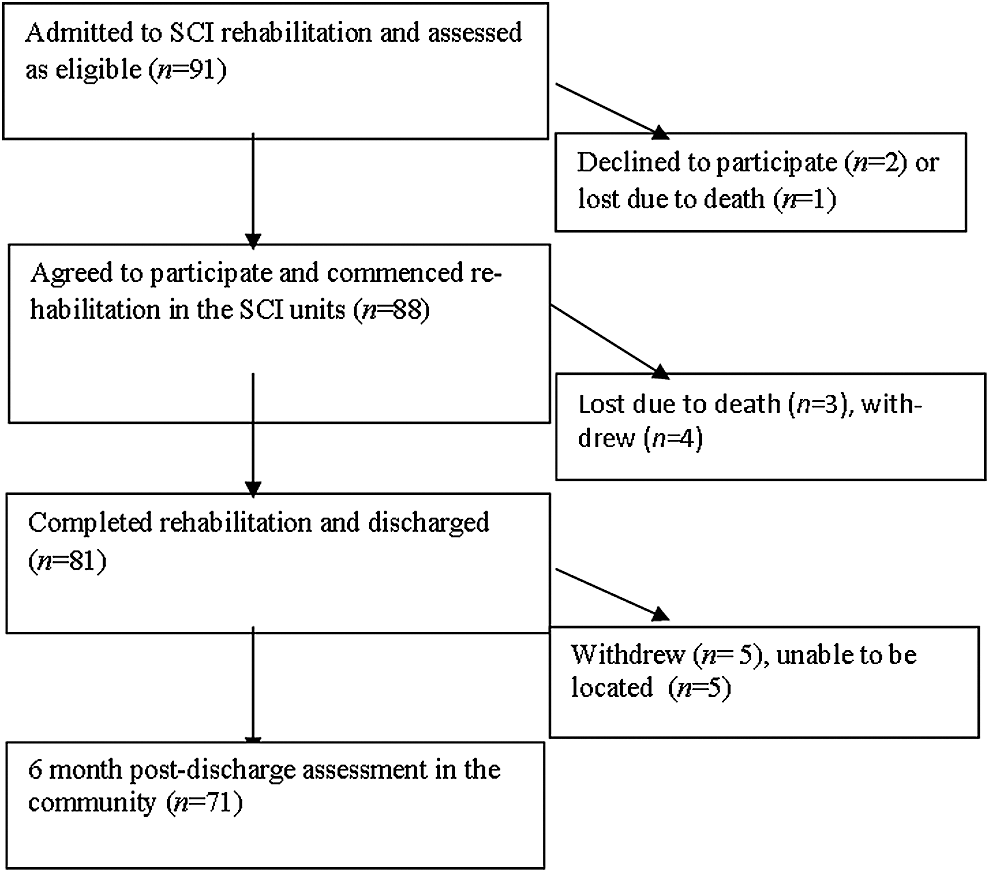
Recruitment and loss at each stage of assessment for Sample 2, including those who declined to participate, died, withdrew, or who were unable to be located 6 months after transition into the community.
SCI, spinal cord injury.
Study design and procedure
The study adhered to STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) reporting guidelines. To test for cognitive differences between the SCI and AB groups, Sample 1 and the AB controls were only assessed on one occasion for cognitive performance and sociodemographics, and the mean years since the injury for participants with SCI in Sample 1 was 3.4 years (SD = 8.7). To test for change in mood states over time in Sample 2, a group cohort longitudinal design was employed; that is, they were assessed three times, first, within 4 weeks of admission to inpatient rehabilitation, second, within 3 weeks of discharge from inpatient rehabilitation, and third, at 6 months post-discharge after transitioning into the community. Table 1 shows that there was a mean 7.3 weeks (SD = 6.1) from the time of the injury to admission to the rehabilitation units when the initial assessment occurred, whereas the mean length of stay in the rehabilitation units for the 88 participants was 23.1 weeks (SD = 9). Therefore, the mean time to the third assessment (6 months post-discharge) was an approximate 54 weeks or just >12 months. The first two assessments were conducted when participants were inpatients, whereas the third assessment was conducted in the participants’ homes, by face-to-face interview or by telephone.
Cognitive capacity, mood state, and pain intensity measures
Cognitive capacity was assessed in all samples by the Neuropsychiatry Unit Cognitive Assessment Tool (NUCOG), a valid and reliable instrument for measuring cognitive impairment in people with psychiatric and neurological disorders. 26 The NUCOG consists of 21 items that assess cognitive function across five cognitive function domains, including attention, memory, executive, visuoconstructional, and language, and is based on established cognitive tests, with items similar to those found in other cognitive screening tools. 26 Senior neuropsychologists were involved in its development, and it is based on established cognitive tests, with NUCOG domains been shown to be highly correlated to established cognitive tests such as the Wechsler Adult Intelligence Scale (WAIS), Stroop and Trail Making Test B. 26 It has been designed to be administered in ∼20–30 min, providing a total score of 100, with each of the five domains having a total score of 20. Community norms and norms for neurological disorders such as stroke, brain injury, epilepsy, and Alzheimer's disease, and for psychiatric disorders (e.g., depression) are provided. 26 NUCOG norms for SCI are now also available. 27
Standard test administration for the NUCOG requires motor skills that people with some physical disabilities will not be able to perform. Therefore, alternative means of assessing some of the cognitive function domains were necessary. Modification is standard practice in cognitive testing in those with physical disability. 28 Research in adults with tetraplegia has resulted in examples of motor-free neuropsychological assessment or modification of existing tests. 6,7,11 Often, items requiring motor capacity are eliminated; for example, visuoconstructional items that require the person to point to an item or draw into a clock face specific times of the day. However, eliminating items could arguably lead to reduced validity of the cognitive test, whereas adapting and modifying items requiring motor function in the arms may possibly tap into slightly different cognitive functions. To maintain the validity of the NUCOG to assess cognitive performance in people with SCI, it was decided to retain all items that require motor capacity in the arms. Alternative instructions were provided to those with no or restricted arm movement. In all cases, it was believed the modifications made in the testing of the specific items tapped into cognitive functions very close to the original purpose of the NUCOG. For example, in a visuoconstruction reproduction task, participants with tetraplegia were asked to describe in detail the shapes rather than draw them with their hands. Evidence for this assertion is based on the scores for those with paraplegia and tetraplegia; those without arm function scored similarly to those with arm function in the visuoconstructional domain in which four of the five items required some motor capacity in the arms,. This was also true for the other domains that required some arm movement, such as executive function, memory, and language.
For Sample 2, assessment involved 2–3 h sessions during which participants were assessed for a range of factors; however, for this article only sociodemographic and injury-related factors, mood states (anxiety, depressive mood, and fatigue), and pain intensity will be presented. Assessment was conducted by psychologists experienced with psychiatric interviewing, and the psychometric measurements used. A standardized psychiatric interview was employed to determine the presence of psychological disorders; however, full details on psychological disorders following SCI has been presented elsewhere. 14 Sample 2 participants completed the Hospital Anxiety and Depression Scale (HADS), shown to be a valid and reliable psychometric measure of depressive mood states in AB and SCI people, and whose items have been shown to be relatively free of injury-related bias. 29 HADS assesses two domains, depressive mood and anxiety, and high scores indicate elevated levels. 29 SCI research has demonstrated the HADS to be suitable for classifying high versus low depressive mood and anxiety variability. 14,29 The third mood state was chronic fatigue, which was assessed by the Fatigue Severity Scale (FSS) which has been shown to be reliable and valid measure of fatigue. 30 The FSS is a nine item Likert scale with scores >4 indicating elevated and severe fatigue. Participants rated their average pain intensity over the past week using a 0–10 numerical rating scale, 31 with 0 = “no pain” and 10 = “pain as bad as can be imagined.” Numerical pain rating scales have been shown to have good test–retest reliability and validity. 31
Statistical analysis
Central tendency statistics were generated for the study variables. The occurrence (percentage) and level of cognitive impairment is reported, including 95% confidence intervals (CI). A multivariate analysis of covariance (MANCOVA) with age, sex, and years of education entered as covariates followed by analysis of variance (ANOVA) tests, were used to determine differences between the SCI and AB groups. For Sample 2, a repeated measures MANCOVA was used to examine change in mood states over time, with age entered as a covariate. Factors entered into the MANCOVA complied with rules governing normality. 32 A Pearson correlation analysis was also conducted to determine associations among variables. Given the number of variables examined, a Bonferroni significance correction on 0.05–0.01 was performed. Missing data were managed by listwise deletion of participants who failed or could not be contacted to complete assessments in the second and third assessments. For a small number of cases (< 10%), a regression substitution technique was used for missing values. This technique has minimal influence on data outcomes while preserving statistical power. 32
Based on a conservative effect size of 0.3 (Cohen's d), using a repeated measures MANOVA, a statistical power of 80%, and an α probability of 0.05, a total sample size of 32 was estimated. 33,34 Therefore, with a sample size ranging between 71 and 88, “a priori” statistical power was determined to be >90%. 34 Partial η2 effect size values are provided as an estimate of the size of the difference between the groups. A partial η2 of ∼0.03 is considered a small difference, 0.13 is considered a medium difference, and >0.2 is considered a large and substantial difference. 33 Post-hoc or retrospective statistical power of the tests is also provided.
NUCOG norms provided in the manual were used to distinguish between those with cognitive impairment and those with higher cognitive functioning. 26 The NUCOG total mean norm has been reported to be 92.9 (SD = 4.9). 26 Therefore, this mean norm score minus 1 SD was used to split the SCI samples (92.9 − 4.9 = 88) into two subgroups so that those with cognitive impairment had NUCOG total scores of ≤88.5, whereas the higher cognitive functioning subgroup had NUCOG total scores >88.5. Dichotomising the NUCOG scores may result in reduced statistical power and the underutilization of data that fall close to the split. 35 However, in defense of dichotomization in this study, dividing the sample into those with cognitive impairment and those with adequate cognitive performance occurs frequently in rehabilitation neurotrauma contexts. Further, the repeated measures MANCOVA conducted on the two subgroups revealed large effect sizes and post-hoc statistical power of ∼70%, adequate to protect against risk of type II errors. All analyses were performed using Statistica Software (Version 12, Statsoft).
Results
Level of cognitive impairment: Sample 1
Table 2 shows descriptive statistics for NUCOG total and domain scores for the SCI and AB groups. The MANCOVA indicated that the SCI group had significantly poorer cognitive capacity than the AB control group: Wilks λ = 0.88, F 6,179 = 4.07, p < 0.01, η2 = 0.12, power = 97%. Table 2 provides a breakdown of the significance levels for the NUCOG total and domain scores. NUCOG total score and all domains were significantly lower in the SCI group (p < 0.001). Figure 2 presents NUCOG domain scores and 95% CI for both groups in graphical form. Based on the cutoff NUCOG total score of 88.5, 28.6% (n = 43) of the participants with SCI in Sample 1 were 1 SD below, and would be classified as cognitively impaired, whereas 16.6% (n = 25) were 2 SD below. Only one person in the AB group had a score <88.5 (2.2%). The breakdown for both groups based on the 88.5 cutoff score was significant (χ2 = 13.8, p < 0.01), with the odds of an adult with SCI having cognitive impairment calculated to be 17.7 times greater than that for someone without SCI (z = 2.8, p < 0.01, 95% CI: 2.4–132.4), and the relative risk of cognitive impairment being present in an adult with SCI was 12.9 times more likely than that for someone without SCI (z = 2.6, p < 0.01, 95% CI: 1.8–91.1).

Neuropsychiatry Unit Cognitive Assessment Tool (NUCOG) total and domain scores for the spinal cord injury (SCI) and able-bodied groups.
Significant differences between groups are indicated, determined by multivariate analysis of covariance with covariates age, sex, and years of education.
p < 0.001.
NUCOG, Neuropsychiatry Unit Cognitive Assessment Tool; SCI, spinal cord injury.
Of interest, when the participants with SCI in Sample 1 were divided into those with NUCOG total scores ≤88.5 and those with NUCOG total scores >88.5, and comparisons were made with the NUCOG scores of the AB group, those participants with NUCOG scores >88.5 were not significantly different from the AB group NUCOG domain scores. No differences in cognitive performance were found in the SCI sample as a function of sex or level of injury (paraplegia vs. tetraplegia). Not surprisingly, age was negatively although weakly correlated with NUCOG total (r = −0.14, p < 0.05), memory (r = −0.26, p < 0.05), and executive function (r = −0.22, p < 0.05). Age was not correlated with cognitive performance in attention, language, or visuoconstruction function.
Variation in mood states and pain intensity over time as a function of cognitive impairment: Sample 2
In Sample 2, after the split based on a NUCOG score of 88.5, 25.3% (n = 18) were classified as having impaired cognitive performance. Table 3 shows descriptive statistics and the variation in mood states (anxiety, depressive mood, and fatigue) and pain intensity in the two SCI subgroups from admission, discharge, and 6 months post-discharge when living in the community. The interaction effect for a repeated measures MANCOVA for dependent variables HADS anxiety and depressive mood, with age as a covariate, indicated that the cognitively impaired subgroup had significantly elevated HADS anxiety and depressive mood compared with the normal cognitive performance subgroup: Wilks λ = 0.86, F 4,66 = 2.62, p = 0.04, η2 = 0.14, power = 70%. Figures 3 and 4 show changes in anxiety and depressive mood, respectively, in the two SCI subgroups. Table 3 and Figures 3 and 4 show that there was little difference between the two subgroups when assessed at admission and discharge. However, anxiety and depressive mood increased in the cognitively impaired subgroup when assessed in the community. The 6 month community assessment was significantly different from all other time periods for anxiety (p < 0.05) and significantly different from assessment at discharge for depressive mood (p < 0.05) using least squared difference (LSD) t tests (given that there was no purpose in testing differences among measures at admission and discharge between subgroups).
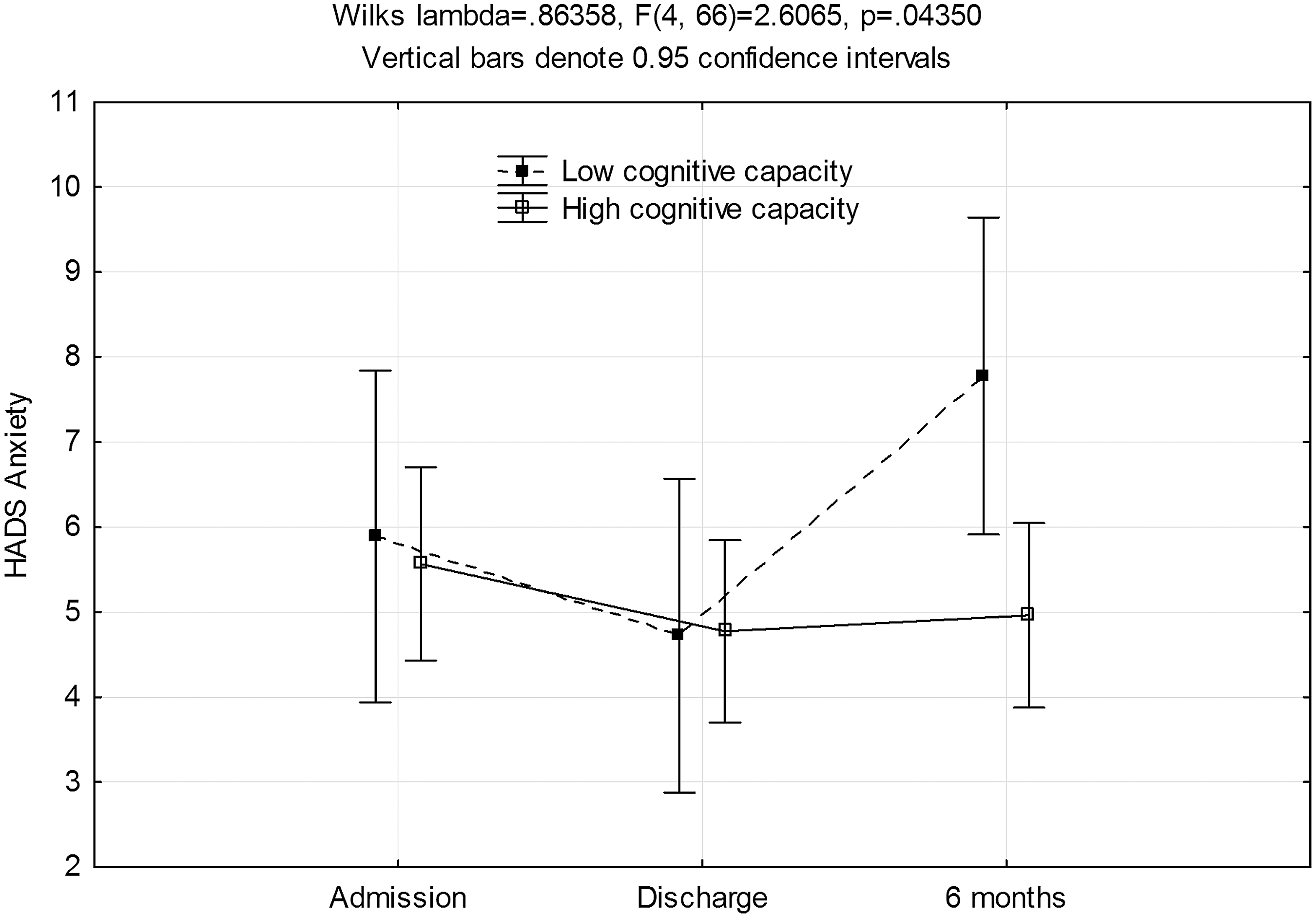
Shows variation in anxiety between the cognitively impaired spinal cord injury (SCI) subgroup and the normal cognitive performance subgroup. The cognitively impaired group had significantly increased anxiety when assessed in the community.
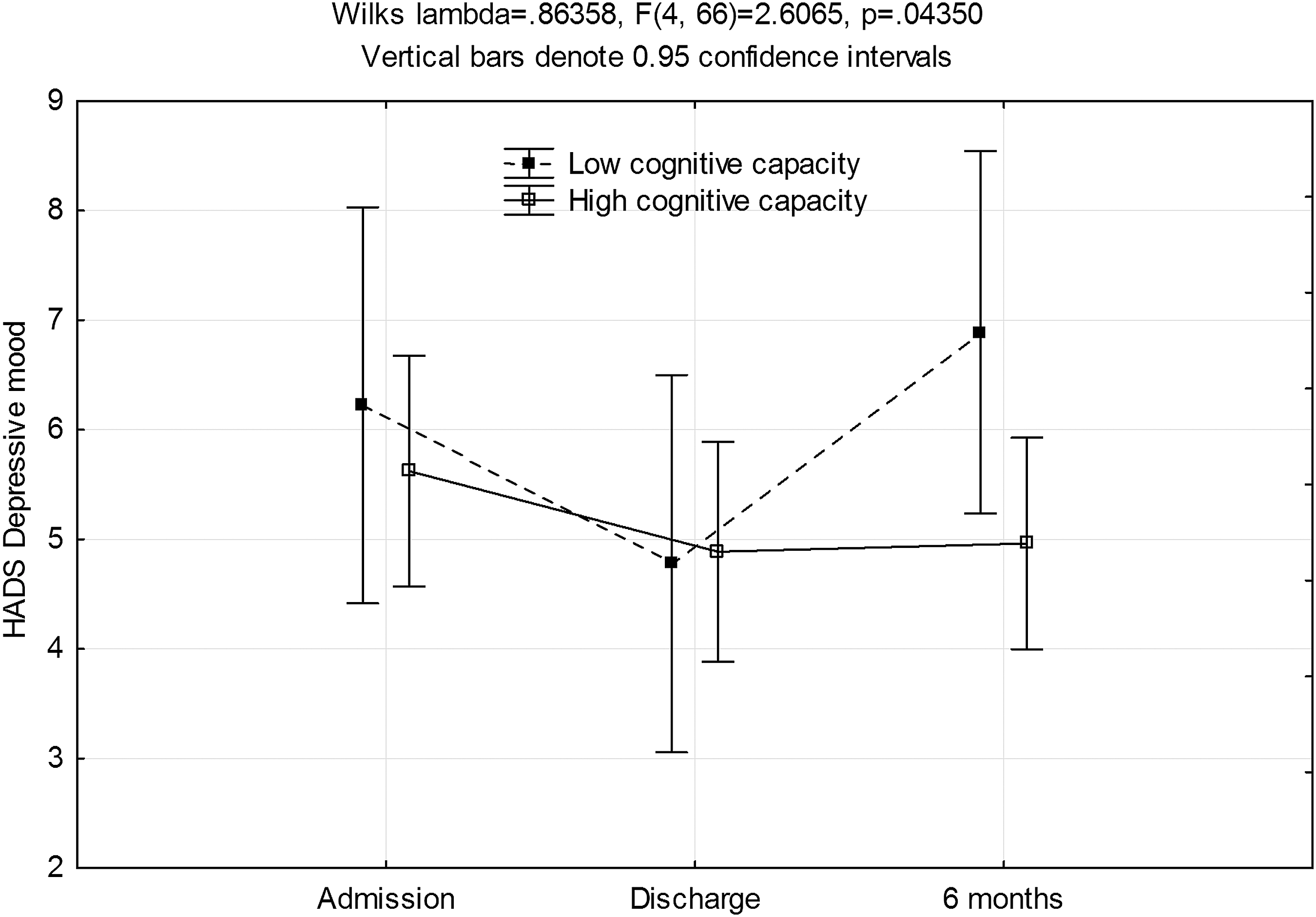
Shows variation in depressive mood between the cognitively impaired spinal cord injury (SCI) subgroup and the normal cognitive performance subgroup. The cognitively impaired group had significantly elevated depressive mood when assessed in the community.
A further 21 missing values for pain intensity at 6 months.
HADS, Hospital Anxiety and Depression Scale; FSS, Fatigue Severity Scale.
Table 3 shows that the cognitively impaired subgroup also had elevated fatigue levels at the 6 month community assessment compared with the normal cognitive performance subgroup; however, the interaction effect for a repeated measures MANCOVA for dependent variable fatigue, with age as a covariate, was not significant: F 2,134 = 2.84, p = 0.06, η2 = 0.04, power = 55%. Table 3 shows that the cognitively impaired subgroup also had elevated pain intensity at the 6 month assessment compared with the normal cognitive performance subgroup. However, this difference was also not significant: F 2,92 = 0.98, p = 0.38, η2 = 0.02, power = 22%.
A Pearson product-moment correlation coefficient analysis revealed that HADS anxiety and depressive mood measures at 6 months post-discharge were significantly and positively associated with all admission and discharge HADS anxiety and depressive mood measures (p < 0.01). Fatigue at 6 months was only significantly and positively correlated with anxiety and depressive mood at 6 months post discharge (p < 0.01). Pain intensity was not significantly associated with anxiety, depressive mood, or fatigue at any time period (p > 0.01). Further, no demographic (e.g., years of education, sex, presence of a partner) or injury (e.g. presence of a TBI, level of injury) variables were significantly associated with any of the mood state or pain intensity measures (p > 0.01).
Discussion
Cognitive impairment in adults with SCI has been found to be prevalent, with estimates suggesting that it occurs in 30% to possibly as much as 60% of the adult SCI population. 6,7,9,10 The findings presented in this article suggest that cognitive impairment may be toward the lower end of this range; that is, occurring in almost 30% of the adult SCI population, with more severe cognitive impairment (i.e., 2 SD below the norm) occurring in ∼16%. The risk of an adult with SCI having cognitive impairment was almost 13 times that of someone without an SCI.
Comparison with the cognitive performance of the AB control group also indicates that overall, adults with SCI as a group have lowered cognitive capacity, shown by a mean NUCOG total difference of six points between the AB (mean 96.3) and SCI (mean 90.4) groups. However, it is important to recognize that when the SCI sample was divided into those with cognitive impairment (NUCOG total score ≤88.5) and those without (NUCOG total score >88.5), the cognitive performance of the normal cognitive performance SCI subgroup was not significantly different across all NUCOG domains from that of the adult controls without a neurological injury. This finding, that the majority of adults with SCI have normal and adequate cognitive function, whereas a large minority have impaired cognitive performance, is important. This also raises implications for SCI rehabilitation. Given these findings, it is critical that adults admitted to SCI rehabilitation are screened for cognitive impairment. Further, the complex array of secondary health conditions that need to be understood and self-managed by those with SCI will be a challenge even for those with normal cognitive function. Therefore, to achieve optimal rehabilitation outcomes for those with cognitive impairment and prevent confusion, feelings of helplessness, and possible mental health disorders, it will be prudent to adapt SCI rehabilitation intervention guidelines to suit the comprehension levels of those adults identified as having reduced cognitive performance. This will certainly be true for the self-management skills required after discharge from the hospital. It also has important implications for education and training of caregivers to be able to support client self-management or provide more directive care, if required.
Psychological morbidity is prevalent in the SCI population. 14,22 –24 It is also known that adults with cognitive impairment have increased risk of mental health problems such as depression and elevated anxiety. 15 In adults with SCI, the relationship between mental health and cognitive impairment has been under-investigated. The findings revealed in this article confirm that adults with SCI who have cognitive impairment are at risk of developing elevated psychological problems. However, our findings suggest this risk is linked to post-discharge living. In the inpatient rehabilitation phase, the risk of depressive mood and elevated anxiety in those with cognitive impairment was no different from the risk in those with normal cognitive performance. Nonetheless, levels of depressive mood and anxiety were shown to increase substantially and significantly after 6 months of living in the community in those adults who had cognitive impairment. Nonsignificant trends for increased fatigue and pain intensity also occurred in this subgroup. This is an important finding not previously reported in the literature. When adults with SCI are discharged into the community they receive considerably less professional support and input, and their personal (cognitive, emotional, mental, social) resources required to self-manage and adjust will be tested and challenged. It is known that social participation, overcoming barriers, and maintaining autonomy are substantial challenges following transition into the community. 5 What has not been identified previously is that this is more of a challenge for adults with SCI who have cognitive impairment, and that many will consequently develop mental health problems. Future research should be concentrated on developing strategies for addressing this problem.
It was a surprise that pain intensity was not significantly associated with the risk of anxiety, depressive mood, and fatigue, given that a majority of adults with SCI suffer chronic pain, which has been shown to be highly related to depressive mood in the longer term. 35,36 Perhaps the major contributor to the development of negative mood states in this study was the psychosocial pressures involved in coping in the community. Demographic and injury factors were found to be unrelated to psychological morbidity, as was found in prior work. 14 It was unexpected that the presence of a TBI was not associated with reduced cognitive performance. This finding, however, does support research showing that cognitive impairment can be related to multiple factors such as fatigue, intense pain, depressed mood, medication usage, and abuse of alcohol and recreational drugs, as well as the presence of a neurological injury such as SCI that results in neuroinflammation. 14,16 –21
Limitations
The study had several limitations. The NUCOG, used to assess cognitive capacity, is a screening tool, and results of this research may need replication with specialized neuropsychological tests that assess cognitive domains more comprehensively. The NUCOG also contains items that require motor function, and these items were modified as described in the Methods section. These modifications may well be a limitation, although we believe that the modifications maintained the integrity of the NUCOG assessment. Sample 2 did not include a consecutive sample of all eligible patients admitted to the units, and excluded those with severe TBI, which, therefore, may have led to some bias in results. Another limitation involved loss of statistical power over time in the prospective arm of the study, especially at the 6 month follow-up after discharge. This was, in part, because the medical complications associated with SCI resulted in it being a challenge to recruit and keep participants engaged in such a prospective study. However, sufficient numbers of participants were recruited, providing valid estimates of cognitive capacity, although increased participant numbers may be required in future studies to confirm the cognitive impairment rates found. A further limitation was the lack of long-term follow-up, although a 4–5 year post-discharge assessment is being planned.
Conclusion
Cognitive impairment is prevalent, and is a high risk in adults with SCI, and for these people, there is a comorbid high risk of the development of psychological disorders such as elevated anxiety and depressive mood after they transition into the community, when psychosocial and physical challenges can become highly taxing. These findings should not be a surprise given the substantial physical and mental health impact associated with SCI and its associated impairment. 1 Further, the study findings highlight the importance of the need to provide constructive and supportive psychosocial care during the transition into the community for those in the high-risk cognitive impairment group. It is hoped that these results will provide direction for improving rehabilitation for people with SCI who also have cognitive impairment, as well as exhibiting elevated levels of anxiety and depressive mood. In addition to the appropriate use of prescribed medications, skill-based strategies are required that help a person to relax when distressed by ongoing life challenges, such as strategies that boost self-management skills and resilience, and that can help strengthen social and vocational support networks, for example, through assistive technologies and cognitive behavior therapies. 37,38
Footnotes
Acknowledgments
We acknowledge financial support in the form of a competitive grant from the Lifetime Care Support Authority (NSW, Australia): LTCSA 08/209. We also thank Dr Dianah Rodrigues, Associate Professor Kathryn Nicholson Perry, and clinical psychologists Annalisa Dezarnaulds and Catherine Ephraums for assisting in collecting NUCOG assessments.
Author Disclosure Statement
No competing financial interests exist.