
Abstract
The aim of this study was to evaluate whether the effect of longer training times (50 instead of 25 min per day) using a robotic device results in a better outcome of walking ability of subjects with a subacute motor complete (American Spinal Injury Association Impairment Scale [AIS]-B) and incomplete (AIS-C) spinal cord injury. Twenty-one patients were enrolled in the study, whereof 18 completed, on average, 34 trainings in 8 weeks. Longer training times resulted in better locomotor function. The second important result of the study is that a beneficial effect can be achieved by the application of a robotic device for prolonged training sessions without requiring more personal resources. It has to remain open whether even longer training times (more than 50 min) would result in a still better outcome. In any case, the extent of possible recovery in an individual patient is determined by the level and severity of spinal cord damage.
Introduction
T
Another important principle in neurorehabilitation is that of motor learning. 9 Key elements of motor learning are task specificity, task variability, feedback or contextual interference, and the amount of exercise or repetitive execution of a task. 9,10 In patients with stroke, it has been shown that augmented exercise therapy had a favorable effect on activities of daily living and walking performance. 11,12 To provide an intense locomotor training at an early stage of rehabilitation in patients with an incomplete but severe SCI (i.e., AIS-B and AIS-C), major assistance of limb movements and partial body weight support are required. A training device that fulfills these requirements is the Lokomat (Hocoma AG, Volketswil, Switzerland), a computer-controlled driven gait orthosis that is operated in combination with a driven treadmill. 13 Training with the Lokomat is feasible for patients with a chronic incomplete SCI, and it has been shown that the patient's gait speed and endurance improved after 8 weeks of training. 14 In patients with stroke, 15 the combination of physiotherapy and training with electromechanical devices at an early stage of rehabilitation has a beneficial effect on functional outcome. However, the added value of locomotor training by using robotic devices in patients with SCI compared to standard physiotherapy is not clear. 16
The aim of this study was to evaluate whether SCI patients with severe sensory-motor deficit after acute traumatic SCI (AIS-B and AIS-C) show better locomotor function following prolonged Lokomat training compared to those who undergo Lokomat training of a shorter duration. The hypothesis is that patients with a severe but incomplete SCI (AIS-B and AIS-C) who undergo a more intense training (i.e., longer training sessions) achieve a higher level of walking ability compared to their controls who undergo conventional training (shorter training sessions). 17 The secondary aim was to evaluate how feasible prolonged locomotor training time is associated with adverse events/complications, such as spasticity, skin ulcerations, or pain.
Methods
The design of this study was developed in accord with acknowledged standards of good clinical practice. Medical ethical committees at all involved sites approved the study. Participants were given written and oral information and were enrolled after they provided a signed consent form. The present study has been registered at
Patients
All patients referred to one of the participating SCI rehabilitation centers were eligible for this study. Specific inclusion criteria were: • acute traumatic etiology of SCI (i.e., early post-injury); • initial SCI categorization AIS-B or AIS-C according to the ISNCSCI
1
; • ASIA motor level between C4 and T12; • limited walking ability, that is, Walking Index for Spinal Cord Injury (WISCI II) ≤5
19
; • study inclusion within 60 days post-trauma; and • able to follow the study intervention and assessment procedures.
Eligible patients that presented the following conditions were not considered for participation: • anthropometrics exceeding the possible range of the Lokomat (i.e., body weight >130 kg, body height >200 cm, or difference in leg length >2 cm); • concomitant injuries or pre-existing medical conditions interfering with the study procedures (e.g., osteoporosis, unstable fracture of lower extremity, restricted range of motion, decubitus ulcer of lower extremity, lower extremity fractures, unstable spine fractures, joint instability preventing weight bearing, severe soft tissue lesion, traumatic brain injury, total joint replacement, chronic pain, osteoarthritis, polyneuropathy, or cardiopulmonary disease); • age younger than 18 years or older than 60 years; or • patients who already participated in another rehabilitation or pharmacological study.
Experimental procedures
After the inclusion criteria were met, eligible patients were informed of their eligibility by the local principal investigator. After patients gave written informed consent, they received a study ID number and baseline assessments were performed. This ID was then transmitted to the coordinating center where a research assistant who was not involved in the study otherwise assigned the patient randomly to either the intervention or the control group. We adopted a four-block randomization scheme that was generated using dedicated computer software. 20
Intervention
Patients of both groups performed 3–5 days of training per week of robotic assisted locomotor training, which were observed for a period of 8 weeks. The robotic device was the Lokomat. In order to ensure that the training was similar in the participating centers, a written guideline was developed and oral instructions were conducted. At each study site, a person was responsible for the study procedures. For the initial five training sessions, no defined specifications were made. These training sessions served to optimize the setup and for the patients to familiarize with the robotic locomotor training device. During subsequent trainings, the following guideline was adopted: • body weight unloading: the legs were as much loaded with body weight as tolerated by the patient (no knee buckling or toe dragging) • speed: within the range of 1.6–3.5 km/h • force with which the device guided the legs of the patients: 100% to minimum tolerated (0% guidance force represents no assistance) • feedback: line graphs representing patients own activity at hip and knee joints were presented on a screen placed in front of the patients. • structure of a single training: - 3 min walking without specification - every third minute walking speed or guidance force were changed or the feedback was switched on or off in order to avoid that the training became monotonous.
Training duration/dose
• Intervention group: The walking time per training was set at a minimum of 50 min.
• Control group: The walking time per training was kept at a maximum of 25 min.
Clinical assessments
Besides demographical and clinical characteristics the following assessments were performed.
Spinal Cord Independence Measure III. 21
The Spinal Cord Independence Measure (SCIM) measures the independence in the performance of daily living tasks in an ordinal manner. The measure has been developed for the SCI population. Each item is rated according to descriptors. The possible total score ranges from zero (totally dependent) to 100 (totally independent). The SCIM is divided into three subdomains: 1) self-care (six items; score range, 0–20); 2) respiration and sphincter management (4 items; score range, 0–40); and 3) mobility (nine items; score range, 0–40). The measure has an ordinal property. For the present study, the domain mobility (SCIMmob) has been adopted at baseline and after completion of 8 weeks of training.
Walking Index for Spinal Cord Injury II. 19
The WISCI is a SCI-specific measure of mobility based on the requirement of the kind of assistive devices, bracing, or personal assistance. It ranges from zero (not able to walk) to 20 (independent). The WISCI score was recorded at baseline and after completion of 8 weeks of training.
Modified Ashworth Scale. 22
The Modified Ashworth Scale (MAS) is a generic scale to monitor and quantify muscle tone in patients with neurological conditions. The resistance against a passive movement is rated on an ordinal scale ranging from zero (no increase in muscle tone) to five (affected parts rigid in flexion or extension). For the present study, hip flexion and extension and knee flexion and extension were rated according to the MAS every 2 weeks during the training period.
Modified Penn Spasm Frequency Scale. 23
The Modified Penn Spasm Frequency Scale (Penn) rates how many spasms a patient experienced in the last 24 h in affected muscles or extremity. The scale comprises two parts. The frequency part ranges from zero (no spasms) to four (spontaneous spasms occurring more than 10 times per hour). The severity part has three categories (1, mild; 2, moderate; 3, severe). Patients were asked about their spasms every 2 weeks throughout the training period.
For each training session, the following items were recorded in a designated training-protocol: • training duration; • distance walked within the Lokomat; • extraordinary events or complications, for example, pain, excessive spasticity, skin breakdown, or joint stress or scheduling problems; and • rate of perceived exertion (RPE). Patients were asked about his or her perceived exertion using a numeric rating scale ranging from 1 (very light) to 10 (represented very, very hard, or maximum).
Global Impression of Change Scale. 24
After the completion of 8 weeks of training, patients were asked to rate their subjectively experienced change in response to the locomotor training using two questions. The first question used a 7-staged Likert scale (0 “no change or condition has got worse”; 7 “a great deal better, and a considerable improvement that has made all the difference”); the second question used a numerical rating scale ranging from 0 “much better” to 10 “much worse” whereas 5 represented “'no change.”
Statistical analyses
Descriptive statistics, including mean and standard deviations or medians and ranges, as appropriate, have been used for the characterization of the included sample and the performed interventions. The differences between the intervention and control treatments regarding walking time, gait speed, body weight unloading, and distance walked were analyzed using independent t-tests. Within-group changes in SCIMmob were analyzed using Wilcoxon's signed-rank test.
For the analysis of the effectiveness of the experimental intervention in contrast to the control intervention, a proportional odds model with random effects has been fitted to the data, using SCIMmob as a dependent variable. Proportional odds models are suited for ordered categorical responses (with K ordered categories) and model the log odds of the event that the response falls in a category j or above (j = 1,…,K-1). In a first model, the covariates group (with values intervention and control), time (with values pre and post), AIS at baseline (with values B or C), the time-group interaction (representing the treatment effect of interest), and a random intercept allowing for within-subject correlation were considered. A likelihood ratio test for nested models was performed to test whether AIS at baseline could be removed from the model.
WISCI values were not considered for the analyses because data variability was too sparse to fit a general model.
In addition, values of the MAS, Penn, Global Impression of Change Scale (PGICS), and the RPE of the two groups have been compared using Mann-Whitney U tests.
For the analyses, SPSS for Windows (Version 23; SPSS, Inc., Chicago, IL) and R statistical software (R version 3.3.0; 2016-05-03; R Core Team; R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing, Vienna, Austria, 2015) have been used.
Results
Sample characteristics
Twenty-one patients were enrolled in this study. Eleven were randomly assigned to the intervention group, 10 to the control group. Three patients were not able to complete 8 weeks of training and were not considered for further analyses. One patient of the control group terminated training after 2 weeks because of knee pain without any clinical sign of overstrains. Two patients of the intervention group stopped training after 5 weeks because of to a spine surgery not related to the training and after 1 week because of a wheelchair accident with consequent foot lesion, respectively. Whereas the distribution of age, sex, and neurological level of injury were about equal, there was a difference in scores according to the AIS classifications. However, this difference was not statistically significant (Table 1).
The table shows the characteristics of the study sample ordered by group allocation. Figures for age represent mean ± standard deviation (range); the other figures concern number of patients.
SCI, spinal cord injury; Tetra, tetraplegia; Para, paraplegia.
Interventions
Start of training post-SCI and number of trainings were not different in the intervention and control groups. However, there was a significant difference in training duration and distance walked. No differences between groups were observed in the average walking speed at weeks 1 and 8 as well as in the percentage of body weight unloading, respectively (Table 2).
The table shows the comparison between the experimental groups regarding the completed interventions.
Figures are mean ± standard deviation (range), except for RPE: median (range).
Statistically significant differences in bold.
SCI, spinal cord injury; BWS, body weight support; RPE, rate of perceived exertion (0–10).
Effectiveness of longer trainings
Regarding SCIMmob, there were two missing values, one in each group at week 8. Instead, the corresponding values from week 6 have been used (last observed, carried forward). Both groups were comparable at baseline. There were larger improvements observed in the intervention group. However, both groups improved to a statistically significant level (Fig. 1; Table 3). The likelihood ratio test revealed that AIS at baseline could be removed from the model (p = 0.55). Within this reduced model, the estimated treatment effect (time-group interaction) on the log odds scale was 3.0 (95% confidence interval [CI], 0.2–5.8), corresponding to a significant odds ratio (OR) of 20.1 (95% CI, 1.2–335.7)—that is, the odds of the event that the SCIM falls in a category k or above (k = 1,…,K-1) was 20.1 times larger if a subject received intervention relative to control.
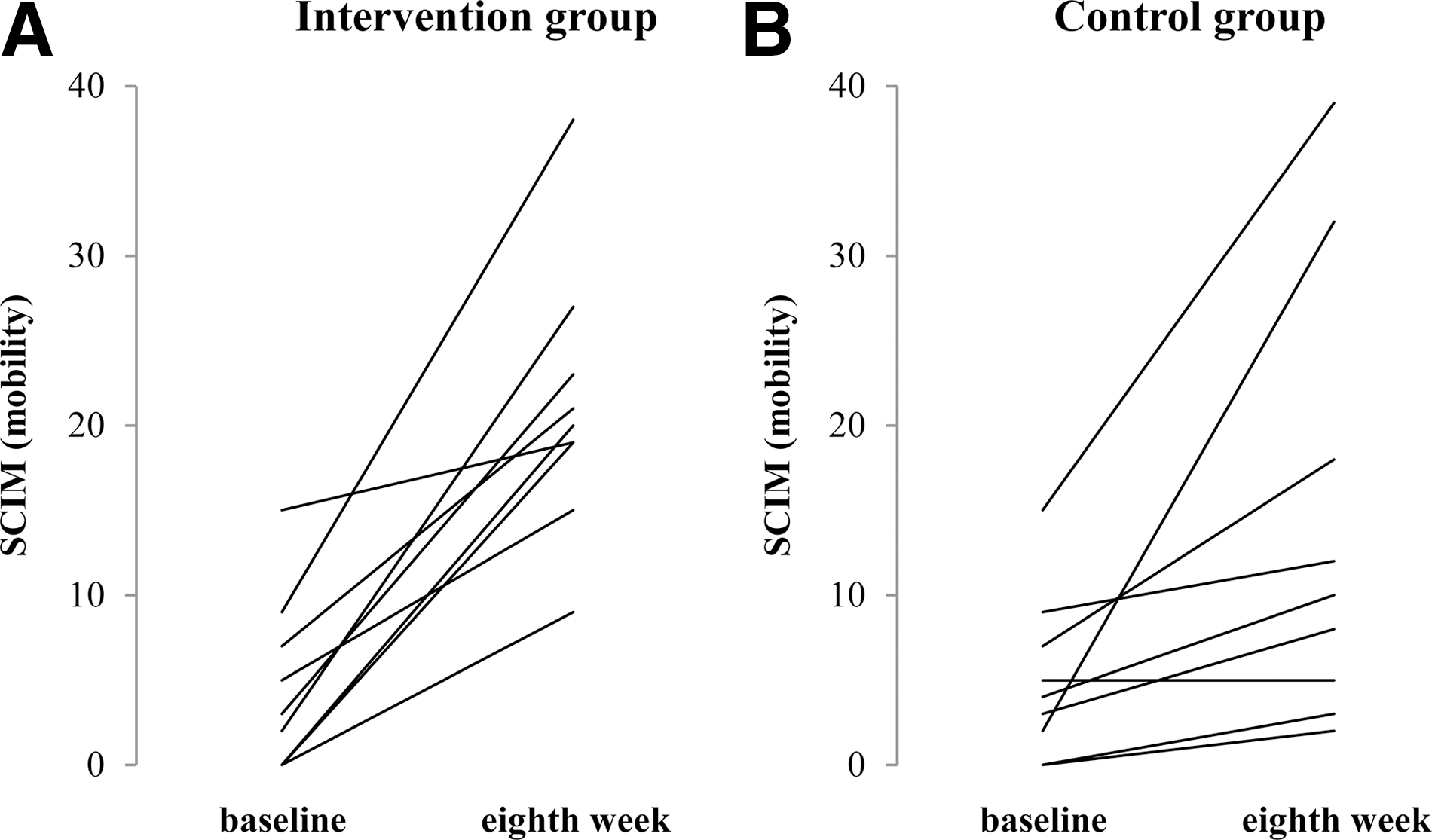
Individual changes in SCIM mobility scores over the period of training. The figure shows the changes in the SCIM mobility score at baseline (week 0) and after 8 weeks of training of all individuals included in the “Intervention group” (
Table shows values for the SCIM at start of the training (week 0) and after completion of the training (week 8) and the mean change in score. There was a statistically significant improvement in both groups. However, changes in the intervention group were markedly greater.
Figures are median values (range).
Within-group contrasts showed a significant OR of 20.4 for the time effect for the control group (95% CI, 2.3–183.4) and a significant OR of 410.7 for the time effect in the intervention group (95% CI, 18.4–9170), the ratio of the time effects representing the above treatment effect. Regarding spasticity as measured using the MAS and Penn scales, respectively, there was no difference between the groups at baseline and after 8 weeks of training (Table 4).
Table shows values for the Modified Ashworth Scale (MAS; median of hip flexion, hip extension, knee flexion, and knee extension; range, 0–5) and the Modified Penn Spasm Frequency (Penn; range, 0–4) and Severity (range, 0–3) scale at start of the training (week 0) and after completion of the training (week 8). Figures are median values (range).
Patient ratings
No difference was found between the groups pertaining to the two questions of the PGICS (p = 0.525; p = 0.555). Also, no difference was found in the RPE (p = 0.963; Table 2).
Discussion
The aim of the present study was 2-fold. One focus was directed to evaluate whether more intense, that is, longer daily locomotor training time results in improved walking outcome as compared to the standard duration. The second focus was directed to the question whether markedly longer training times are feasible by the application of a robotic device. Although not a focus of this study, the latter aspect is especially of economic interest given that longer training times using physiotherapeutic approaches would be associated with higher personal resources. In contrast, an important rationale to apply robotic devices in neurorehabilitation is that they allow intensive functional training approaches.
For individuals with SCI, functional training is the most effective approach to exploit neuroplasticity as a substrate to recover motor function. The mechanisms of plasticity underlying the effects of functional training have been explored in rodent and cat models of SCI. 25 –28 According to these studies, rehabilitation of sensorimotor function post-SCI is directed toward training of lost movements. 27
Comparable with what has been shown in animal studies, locomotor training post-SCI can improve locomotor ability even in individuals with low motor score. 29,30 The benefit of such functional training does not depend on the approach used, that is, body-weight–supported treadmill training is equally effective as assisted overground walking. 31 –33 Even in chronic incomplete SCI, when no more spontaneous recovery can be expected, an improvement of stepping ability can be achieved. 14,34,35
In post-stroke subjects, it could be demonstrated that the effects of locomotor training can be enhanced by high-intensity 36 and high-velocity 37 training, as well as by longer training times. 38 These observations led to the question of how far these factors might be translated to subjects with SCI. The present study shows that longer locomotor training times indeed lead to a better outcome of walking ability in subjects with motor complete and incomplete SCI. In addition, the results demonstrate that such longer training times can be achieved by the application of a robotic device. The latter aspect seems to be important insofar that a robotic device such as the Lokomat was suggested to provide too much support to achieve similar training effects as an assisted overground walking approach. 39 Although no comparison was made in the present study between the different locomotor training approaches, the positive effect of the robotic training performed here is obvious.
The observation of a beneficial effect of training with a robotic device is important given that a longer overground training time would require substantially more physiotherapy resources without such training devices. Obviously, the Lokomat-assisted device is similar to overground training because they provide sufficient proprioceptive feedback to induce a locomotor pattern in the thoracolumbar spinal cord as a basic requirement to achieve positive effects on stepping function. 40 This proprioceptive input includes signals from leg extensor muscles that provide load-related afferent information to the spinal cord. 41 Further, hip-joint–related afferent input is required for the initiation of the swing phase. 42 These signals are essential for the generation of a locomotor EMG pattern in subjects with SCI and, consequently, for a beneficial effect of this training for the outcome of walking ability. 42 Nevertheless, it has to be noted that, after an SCI, the recovery of function is limited and is determined by the level and severity of spinal cord damage, 43 that is, the amount of spared spinal neural tissue determines the effectiveness of training.
Although the technology of robotic devices for the rehabilitation of sensorimotor deficits is still in its early stages, 44 such devices are not superior to other approaches of training per se. 39,45 However, they allow longer training times in patients with severe deficit. In the future, such devices should become more flexible in order to adapt the training to the individual needs, that is, to allow challenging training in the different stages of functional recovery and catered to individual limitations and needs. For example, in elderly patients with an SCI, it is known that the spontaneous recovery of neurological deficit is similar to that of younger individuals. However, older patients have greater problems in translating this recovery into improvement of daily life activities. 46
The main message of this study is that longer training times have a beneficial effect on outcome of walking function in patients with an acute incomplete SCI. It remains open whether even longer training times than applied here would result in a still greater improvement of function. Longer trainings cannot be achieved by the use of new technologies alone. For their proper operation, the specific clinical knowledge and skill of trained therapists are required in order to adapt and modify the training parameters to appropriately meet the individual needs of patients.
Study limitations
The present study was a pragmatic trial insofar that the study reflects the reality of rehabilitation. It was embedded in the routine rehabilitation procedures at four centers. This made it necessary to adapt the study in various aspects. The training duration was somewhat limited because of available Lokomat time and other scheduled therapies. The contrast regarding training time between intervention and control group amounted to 426 min/month, which still exceeds the difference reported in other studies. 11 Follow-up assessments 6 months after training were planned in the design of the original studies, but not included in the analyses. The reasons for this were irregular check-up visits so that the time span of these assessments differed too much, or, in some participants, the follow-up assessments were not available. Also, there was no monitoring of the interventions provided beyond the 8 weeks of training (e.g., some patients continued locomotor training). One of the study limitations was the relatively strict inclusion criteria. Those were defined to represent the clinical indication for automated locomotor training and with the intention to include a potentially homogeneous sample. The latter was achieved by limiting admittance to the study for patients with a traumatic SCI. However, clinical experience shows that today an incomplete SCI is mostly attributed to a nontraumatic cause. 47 The inclusion criteria led to a small recruitment rate, which is the reason that enrollment stopped before the intended number of participants could be recruited. Looking at the baseline characteristics, it seems that there is an imbalance regarding the impairment according to the AIS scale in favor of the intervention group. Although this was statistically not significant, it might have influenced the observed results to a limited extent. Although results confirm the hypotheses made at beginning of the study, these need to be confirmed in a larger trial.
Footnotes
Acknowledgment
The authors thank Mr. André Meichtry for his statistical support.
Author Disclosure Statement
No competing financial interests exist.