
Abstract
Blast-related traumatic brain injury (bTBI) resulting from improvised explosive devices is the hallmark injury of recent wars, and affects many returning veterans who experienced either direct or indirect exposure. Many of these veterans have long-term neurocognitive symptoms. However, there is very little evidence to show whether blast-induced acceleration alone, in the absence of secondary impacts, can cause mild TBI. In this study, we examine the effect of under-vehicle blast-induced hyperacceleration (uBIH) of ∼1700 g on the biochemical and microstrucutral changes in the brain using diffusion tensor imaging (DTI) and magnetic resonance spectroscopy (MRS). Two groups of adult male Sprague–Dawley (SD) rats were subjected to a sham procedure and uBIH, respectively. Axonal and neurochemical alterations were assessed using in vivo DTI and MRS at 2 h, 24 h, and 7 days after uBIH. Significant reduction in mean diffusivity, axial diffusivity, and radial diffusivity were observed in the hippocampus, thalamus, internal capsule, and corpus callosum as early as 2 h, and sustained up to 7 days post-uBIH. Total creatine (Cr) and glutamine (Gln) were reduced in the internal capsule at 24 h post-uBIH. The reductions in DTI parameters, Cr and Gln in vivo suggest potential activation of astrocytes and diffuse axonal injury following a single underbody blast, confirming previous histology reports.
Introduction
A
Several advanced in vivo imaging techniques, including diffusion tensor imaging (DTI) and proton magnetic resonance spectroscopy (MRS), have been explored to study TBI in pre-clinical animal models, to better understand the temporal microstructural and biochemical changes following TBI. 15 –21 Commonly used DTI parameters include mean diffusivity (MD) and fractional anisotropy (FA). MD measures the average water diffusion within the brain tissue, whereas FA measures the degree of diffusion anisotropy present within a voxel, as would be in the case of axons where water diffuses preferentially along the axon. Alterations in MD reflect pathological changes in the brain tissue caused by changes in the diffusion characteristics of the intra- and extracellular water compartments, including restricted diffusion (cytotoxic edema) and water exchange across permeable boundaries. 22 Changes in the FA, on the other hand, are indicative of the structural integrity of the tissue. The sub-parameters of FA include axial diffusivity (AD) and radial diffusivity (RD). Diffusion along the axon is measured by AD, and is a measure of axonal integrity, whereas RD measures diffusion across the axon and is reflective of myelin integrity. 23 Previous TBI studies on both humans and animals have shown altered MD 24 –27 and FA in white matter regions 19,28 –33 anywhere from 24 h to several days following injury, reflecting pathological conditions such as edema, fiber degeneration, cellular membrane disruption, and cell death. 20,32,34,35 High-resolution in vivo MRS provides complementary information and assesses metabolic irregularities following injury. Several metabolites such as N-acetylaspartate (NAA), choline (Cho), and lactate (Lac) are highly sensitive to the pathology that contributes to TBI. Reduction in concentration of NAA, glutamate (Glu), creatine (Cr), myo-inositol (Ins), and taurine (Tau) in tissues and increased concentrations of lactate, phosphocholine (PCho), and glutamine (Gln) at either acute or subacute stages have been reported, indicating conditions including ischemia, mitochondrial dysfunction, and imbalance of excitatory/inhibitory and astrocyte activation. 20,21,36,37 In this study, we use both in vivo DTI and MRS to evaluate early microstructural and biochemical alterations caused by uBIH in the rat brain.
Methods
Animal preparation
Six adult male Sprague–Dawley (SD) rats weighing 300–350 g underwent the uBIH procedure as described by Proctor and coworkers, 14 and another group of six male SD rats in the same weight range were assigned to be the sham group. 14 Briefly, all rats were initially anesthetized with ketamine (80 mg/kg) and xylazine (10 mg/kg). Each of two rats belonging to the uBIH group was wrapped in 2 cm thick cotton blankets to minimize movement, and placed in the prone position in one of two aluminum cylinders, 37 cm long by 3 cm wide, which was bolted onto a 38 cm2 and 5 cm thick aluminum platform. This platform was located immediately above a second 38 cm2 aluminum platform that was 2.5 cm thick. A 0.6 cm thick hard rubber pad was placed between the two platforms to dampen oscillatory accelerations. Both platforms had 2.5 cm wide holes located inside each of the four corners. Aluminum rods 90 cm high were inserted through each of the holes and secured to a steel base on which the platforms rested, thus allowing for only direct movement of the platforms vertically following the blasts. The steel base was bolted to the edges of a steel tank filled with water to a standoff distance of from the bottom platform of 0.25 cm. An explosive charge of 1.5 g pentaerythritol tetranitrate was placed in the water 5 cm under the center of the plate, which when detonated, generated maximal g forces of 1734 ± 90g (mean ± SEM; n = 6) as measured by an accelerometer attached to the top plate near the head ends of the cylinders. The explosion caused the plate to accelerate vertically to heights of ∼70 cm and then drop back down to the original location. During two experiments, we also attached pressure sensors to the top plate near the accelerometer. An increase of <1 psi was observed. Following the uBIH exposure, the rats were removed from the assembly and allowed to recover from the anesthesia. All animals recovered normal activity within 1 h and exhibited no signs of distress. Following the imaging measurements performed on day 7 after sham or blast exposure, the rats were euthanized.
In vivo DTI and 1H MRS
MR experiments were performed prior to the uBIH/sham procedure (baseline), 2 h, 24 h, and 7 days post-uBIH on a BrukerBioSpec 7.0 Tesla 30 cm horizontal bore scanner (Bruker Corporation, Ettlingen, Germany) equipped with a BGA12S gradient system and interfaced to a BrukerParaVision 5.1 console. A Bruker 72 mm linear-volume coil was used as the transmitter, and a Bruker1H four channel surface coil array was used as the receiver. The rat was under 2–3% isoflurane anesthesia and 1 L/min oxygen administration during the MR experiment. An MR compatible small-animal monitoring and gating system (SA Instruments, Inc., New York, NY) was used to monitor the animal's respiration rate and body temperature. The animal's body temperature was maintained at 35–37°C using a warm water bath circulation. Ear pins and bite bars were used to fix the animal's head to minimize head motion.
A three slice (axial, midsagittal, and coronal) scout image using rapid acquisition with fast low angle shot (FLASH) 38,39 was used to localize the rat brain. A fast shimming procedure (FASTMAP) was used to improve the B0 homogeneity covering the brain. 40 Both proton density (PD) and T2-weighted images were obtained for anatomic reference using a two-dimensional rapid acquisition with relaxation enhancement (RARE) sequence covering the entire brain. 41 Imaging was performed over a 3.5 cm field of view (FOV) in the coronal plane with an in-plane resolution of 137 μm using 24 slices at 1 mm thickness, at an effective echo time (TE) of 18.94 ms for the PD-weighted images and an effective TE of 56.82 ms for the T2-weighted images. The repeat time (TR) was 3500 ms.
Diffusion tensor images were acquired with a single shot, spin-echo echo-planar imaging sequence. An encoding scheme of 30 gradient directions was used with the duration of each of the diffusion gradients being 4 ms with a temporal spacing of 20 ms between the two diffusion gradients. Three b-values (1000 sec/mm2, 1500 sec/mm2, and 2000 sec/mm2) were acquired for each direction following the acquisition of five images acquired at b = 0 sec/mm2. The diffusion tensor images were obtained using a single average over the same FOV as the coronal PD/T2 images, but at an in-plane resolution of 0.273 mm at a TR/TE of 6000/49.90 ms respectively.
1H MRS data were obtained from voxels that covered the left internal capsule (3 × 3 × 3 mm3), left hippocampus (1.5 × 3.5 × 3 mm3), and left cortex (1.5 × 4 × 3 mm3) respectively. These regions were chosen because they were implicated in a previous study using the same injury model and also based on reports using other TBI models. 14,36 Prior to acquiring the spectra, adjustments of all first- and second-order shims over the voxel of interest were accomplished with the FASTMAP procedure. A custom modified short-echo-time Point-RESolved Spectroscopy (PRESS) pulse sequence (TR/TE = 2500/10 ms, number of averages = 360) 42 was used for MRS data acquisition covering the three regions of interest (ROI). The unsuppressed water signal from each of the prescribed voxels was obtained to serve as a reference for determining the specific metabolite concentrations. The total duration of the entire imaging experiment was ∼2.5 h. All animal procedures were approved by the University of Maryland, Baltimore, Animal Care and Use Committee, and by the United States Army Medical Research and Materiel Command Animal Care and Use Review Office.
Data processing and analysis
DTI reconstruction was performed on each voxel using in-house MATLAB program (Mathworks, Natick, MA) to generate MD, FA, AD, and RD maps. ROIs for each rat were manually drawn on the FA map within the cortex (left, right), hippocampus (left, right), thalamus (left, right), internal capsule (left, right), and corpus callosum (genu, trunk, splenium), respectively, as shown in Figure 1A.
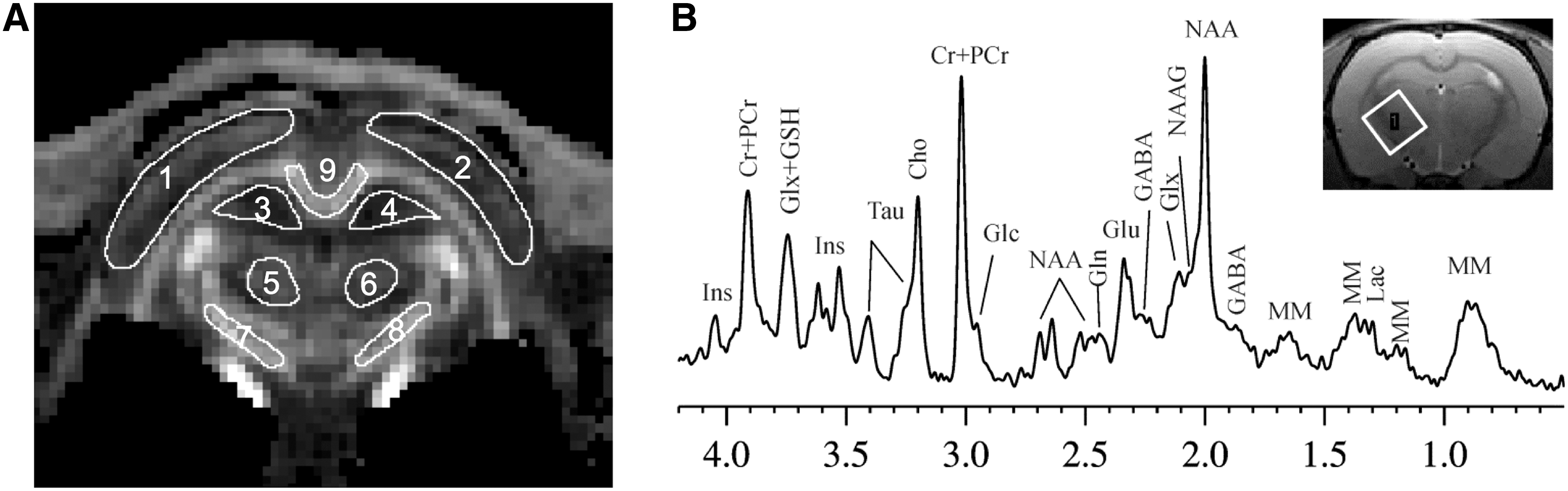
1H MRS data were fitted using the LCModel package. 43 Representative in vivo high resolution1H MRS from the internal capsule from one uBIH rat at its baseline is shown in Figure 1B. The Cramer-Rao lower bounds were estimated by the LCModel to assess the reliability of the reported metabolite concentration, and only metabolites with standard deviations (SD) <20 were included for further analysis.
DTI and MRS data from each region were normalized to its own baseline level (pre-uBIH). The ratio of post to pre-uBIH level was used to capture changes between the two time points. Statistical analysis was performed using SigmaPlot version 12.5 (Systat Software, Inc., San Jose, CA). Both DTI and MRS data of sham and uBIH rats at four time points were analyzed using a two way repeated measures ANOVA to examine temporal changes in each region, and group comparisons were made at each observation point. Statistical significance was defined as p < 0.05.
Results
Microstructural alterations after uBIH
Six rats were exposed to uBIH that generated maximal g forces ranging from 1500 to 1900g, with a mean value of 1734 ± 90g. All of these rats and the six sham rats that were similarly anesthetized but not subjected to uBIH survived to 7 days, at which time they were euthanized. No animal demonstrated any visible changes on T2-weighted brain images at 2 h, 24 h, and 7 days post-blast or post-sham blast. However, broad reductions of DTI parameters were observed in the hippocampus, thalamus, and internal capsule of rats in the uBIH group compared with the sham group. Significant alterations of MD were observed in the hippocampus (right: F = 2.44, p = 0.017), and the thalamus (left: F = 7.092, p = 0.024; right: F = 5.257, p = 0.045) (Table 1) in the uBIH rats compared with the sham group. The reductions of MD were significant at 2 h (p = 0.044) and 7 days (p = 0.025) in the hippocampus (Fig. 2A) and at 24 h in the thalamus (left: p = 0.008; right: p = 0.018) (Fig. 2B, C) in the uBIH cohort compared with the sham cohort. AD was significantly reduced in the hippocampus (right: F = 7.208, p = 0.023) (Table 1) at 24 h (p = 0.006) and 7 days (p = 0.008) (Fig. 3A) and in the internal capsule (right: F = 5.222, p = 0.045) at 24 h (p = 0.006) (Fig. 3B) in the uBIH group compared with the sham group. RD was significantly reduced in the thalamus (left: F = 14.291, p = 0.004; right: F = 7.861, p = 0.019) (Table 1) at 2 h (left: p < 0.001; right: p = 0.001), 7 days (left: p = 0.013; right: p = 0.041) (Fig. 4A,B) and in the genu of the corpus callosum (F = 8.407, p = 0.016) at 2 h (p = 0.031) and 7 days (p = 0.004) (Fig. 4C) after uBIH.
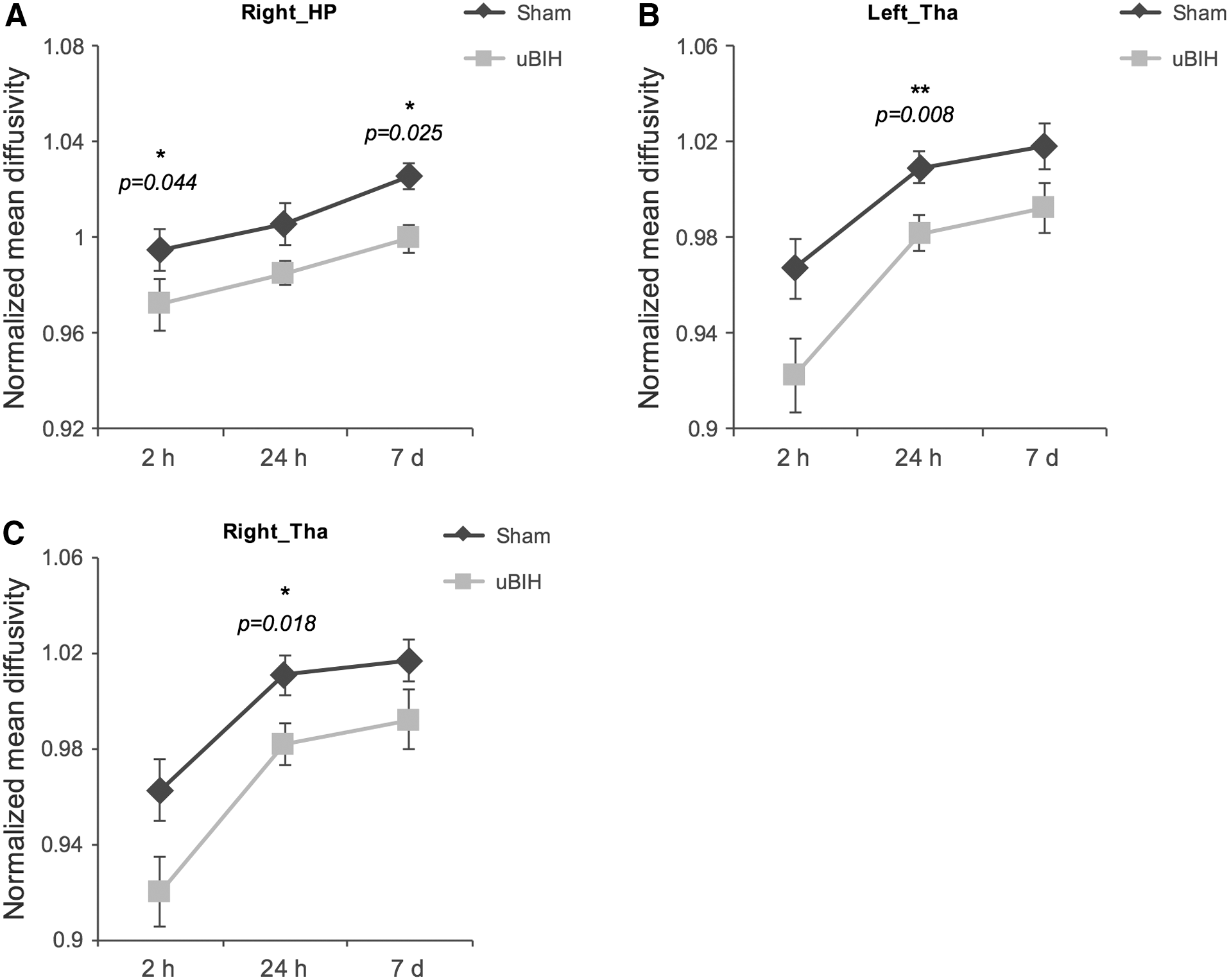
Mean diffusivity alterations (ratio to baseline level) in right hippocampus (HP)
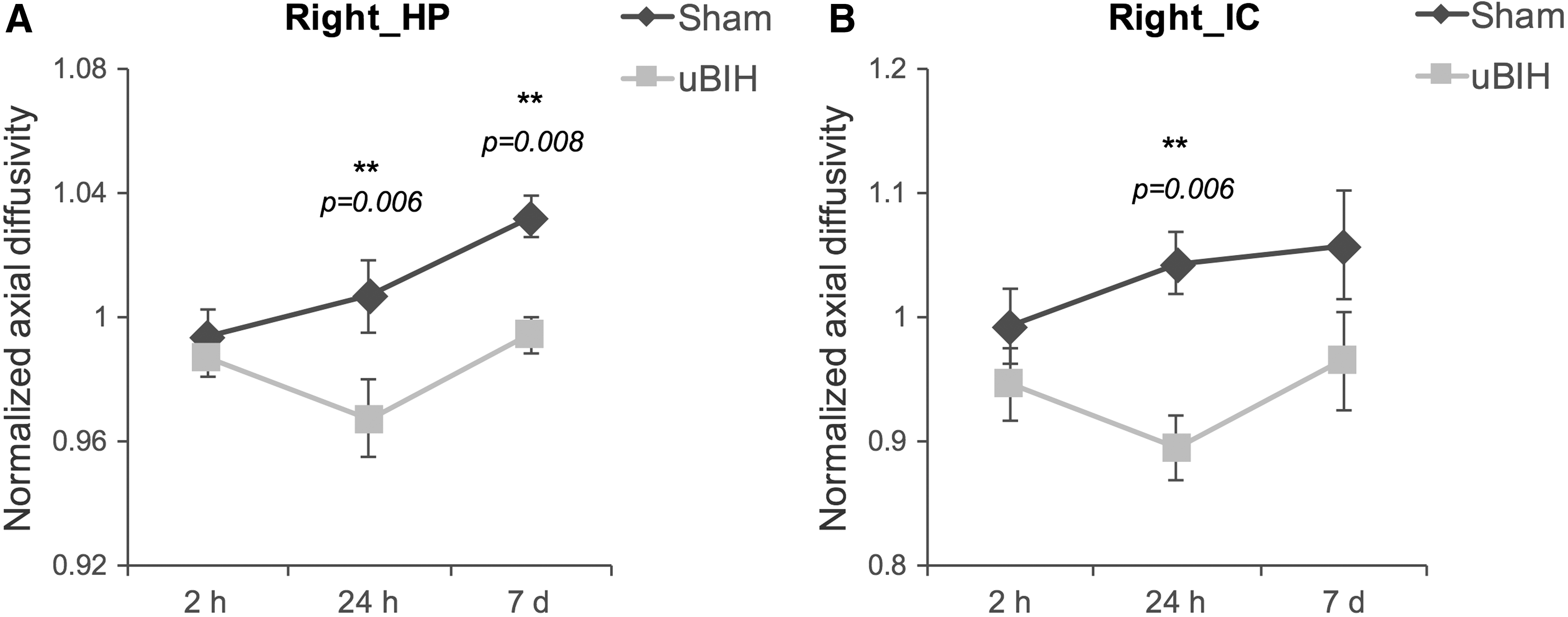
Axial diffusivity alterations (ratio to baseline level) in right hippocampus (HP)
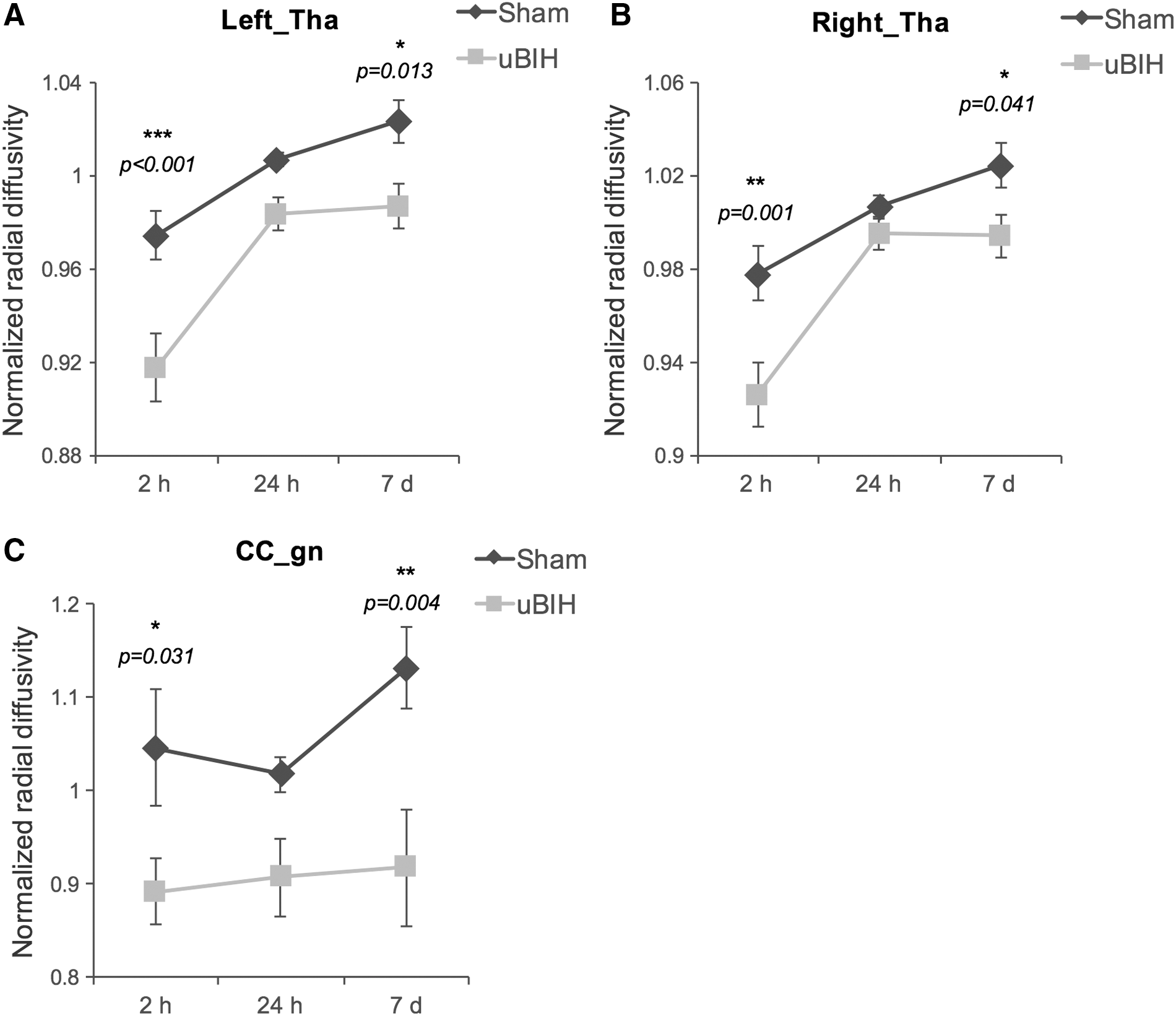
Radial diffusivity alterations (ratio to baseline level) in left
DTI, diffusion tensor imaging; MRS, magnetic resonance spectroscopy; HP, hippocampus; Tha, thalamus; IC, internal capsule; CC_gn, genu of corpus callosum).
Biochemical alterations after uBIH
Biochemical alterations were observed in the internal capsule where changes in the levels of Cr (F = 5.844, p = 0.036) were substantial, and marginal Gln (F = 3.877, p = 0.077) changes were also observed in the uBIH group compared with the sham group (Table 1). Both Cr (p = 0.005) and Gln (p = 0.021) levels were significantly reduced at 24 h in the uBIH group compared with the sham group (Fig. 5). No other significant biochemical alterations were detected in any other regions at any time points in the uBIH rats compared with the sham rats.

Changes in creatine
Discussion
To the best of our knowledge, this is the first in vivo study to apply a combination of DTI and MRS to detect biochemical and microstructural changes following hyperacceleration from a blast in isolation from the overpressure from the blast (primary impact) or other secondary impact-related injuries. We demonstrate early metabolic alterations and tissue microstructure following hyperacceleration, which persist until 7 days following the exposure. Our study reveals three main findings: 1) no visible brain injuries were observed on conventional T2-weighted imaging, even when the animals were exposed to an average of 1700g; 2) Cr and Gln levels decreased in the internal capsule at 24 h post-uBIH, and returned to baseline values by 7 days; and 3) shearing injuries as observed by changes in diffusion tensor parameters were observed in the internal capsule corpus callosum, hippocampus, and thalamus as late as 7 days following injury. When compared with the histological findings from our previous study performed under conditions that generated much lower g forces (50g), and that resulted in diffuse axonal injury and astrocyte activation, 14 the present study not only confirms these findings, but also provides further evidence that neuropathology changes can be detected in vivo using DTI and MRS techniques.
In the present study, decreased AD level in the internal capsule at 24 h, decreased RD to the corpus callosum, and decreased MD and AD levels in the hippocampus at both 2 h and 7 days post-uBIH are indicative of mild diffuse axonal injuries, which agrees with the histology findings using the same uBIH model. 14 In addition to these changes, we also observed a decreased MD at 24 h and decreased RD at 2 h and 7 days post-uBIH in the thalamus, indicating cell swelling. These results indicate that the sequelae of pathological events occur at a different rate in each vulnerable brain, which is well captured noninvasively from the longitudinal DTI data. The low Cr and Gln levels found in the uBIH rats at 24 h in the internal capsule may indicate an imbalance in astrocytic function after exposure to uBIH. Synthesized in the liver and transported to the brain, it has been shown that Cr is two- to four-fold more concentrated in glial cells than in neurons, 44 with quite large regional variations. Astroglial cells are virtually the sole site for Gln synthetase activity in the brain to convert Glu to Gln. 45 A prior study using this injury model demonstrated astrocyte activation in the internal capsule at 7 days post-uBIH. 14 It is, therefore, likely that the depletions of Cr and Gln are related to this astrocyte activation. The in vivo longitudinal localized MRS findings in this study provide further evidence that gliosis in the internal capsule is a prominent pathology following uBIH. 14,36 Quantitative analyses of cellular inflammatory responses, axonal injury, and behavorial alterations are in progress to further characterize the pathophysiology of uBIH.
Various animal models have been developed to replicate different aspects of human TBI over the past several decades. The most widely used ones are the controlled cortical impact (CCI) model, 46 the fluid percussion injury (FPI) model, 47 and blast tube bTBI models. 48,49 CCI and FPI models result in direct brain deformation and neuronal cell death, which we have not detected in the uBIH model (not shown). Depending on the severity of injury, tissue damage from CCI and FPI is focal, and may be directly visible even with conventional MRI. Studies have shown that the changes from these focal injuries lead to various changes in local conditions including ischemia, mitochondrial dysfunction, and imbalance of excitatory/inhibitory and astrocyte activation. 15,20,37,50
Studies using blast overpressure primary bTBI models are more comparable to our uBIH model because they do not introduce direct impact on the brain, and they result in relatively mild injuries without severe tissue damage and broad biochemical disturbances. In primary bTBI models, injury is generated by blast overpressure waves or shock waves to the head, and often to the chest and abdomen. Previous in vivo or in vitro primary bTBI studies using shock tube or direct cranial blast reported increased mean kurtosis (MK), Gln levels, and expression of glial fibrillary acidic protein (GFAP), indicating astrocyte and microglial activation in subcortical regions such as the internal capsule, hippocampus, and hypothalamus at the subacute stage following injury. 36,51,52 Diffuse axonal injury was also observed as increased FA in the internal capsule and decreased MD in the hippocampus up to 14 days post-blast, indicating axonal swelling or a disruption of ionic homeostasis resulting in an imbalance in intra- and extracellular water. 18,19,36 A more recent study assessed the value of manganese-enhanced magnetic resonance imaging (MEMRI) using manganese chloride (MnCl2) at various time points following a 30 psig blast in a shock tube, and found manganese uptake to be a promising biomarker of TBI. 53 Although future preclinical studies on hyperacceleration may benefit form MEMRI, the use of manganese in humans has been shown to be neurotoxic, and the translation of such studies may take some time, as research continues to make less toxic manganese-based chelates.
The clinical relevance of results obtained using this small scale underbody blast model depend to some degree on the scaling of the g force and its relationship with the g forces experienced by individuals present within vehicles targeted by land mines and improvised explosive devices. The issue of scaling is important but not straightforward. To our knowledge, there are no empirical data from comparisons obtained with small or large animals exposed to small- and large-scale explosions relevant to under-vehicle blasts. The closest estimate is a scaling factor of 10, based on buried explosions of different intensities. 54 Experiments with full scale models of military vehicles indicate that land mines generate g force loads of between 200 and 4000g at floor level, 55 which would be somewhat lower at the level of the passenger. If indeed the g force scaling factor is close to 10, our explosions generating 1700g would be equivalent to a full-scale under-vehicle blast generating 170g, which is close to the measured level of 200g load on full- scale vehicles generated by commonly used explosives.
The present study demonstrates that in uBIH, the changes are localized primarily to the internal capsule and the hippocampus, with changes occurring at different time points, depending on the parameter measured and the brain location. The results show some consistency with previous primary bTBI reports. In a previous study on a direct cranium only blast traumatic brain injury (dc-bTBI) rat model that was silent on conventional T2-weighted imaging, diffusion kurtosis imaging (DKI), and proton MRSalso demonstrated impairments in the internal capsule and the hippocampus, with peak changes observed at ∼21 days after dc-bTBI. 36 Significant microglial activation and neurodegeneration were observed even at 28 days in the hippocampus.
It is generally accepted that TBI without physical signs of brain injury can potentially contribute to post-traumatic stress disorder (PTSD). 5,56 The hippocampus and the internal capsule are reported to play a role in triggering the typical symptoms of PTSD. 57 –64 PTSD patients with a history of combat trauma show a considerable reduction in the volume of the hippocampus, and hippocampal dysfunction. 58 –60 Treatments that resulted in neurogenesis in the hippocampus or increased hippocampal volume were shown to improve PTSD symptoms. 61,63,64 PTSD symptoms induced by mTBI are also associated with white matter damage to the internal capsule and uncinate fasciculus, inducing a loss of inhibitory control of the autonomic nervous system (ANS), which results in alterations in ANS-driven defense and socially adaptive physiological states. 57 Significantly reduced FA in the internal capsule was also reported to be closely related to major depressive disorder (MDD) after mTBI. 62 Although the present study did not assess the long-term behavioral outcome on the rats, given the spatial locations that are implicated in this study and the dc-bTBImodel, the results suggest the possibility of vestibular dysfunction and memory impairment. 34 Our findings also suggest that both the cranium-only blast injury and the hyperacceleration-associated injury may combine synergistically, resulting in comorbidities that are worse than from a single type of injury. This is a more likely scenario, in which a person exposed to blast injury may also be exposed to a certain amount of hyperacceleration.
This study on microstructural and biochemical alterations after uBIH should be viewed in the context of certain limitations. First, no studies were performed to assess the long-term behavioral outcomes of these animals. Although we expect similar behavior changes as in the dc-bTBI model, given the similarity in the regions affected, future studies should include comprehensive behavioral testing and correlate with in vivo findings. Second, histological confirmation was not possible on these animals at this time. However, histology results from the previous study using the same uBIH model are supportive of the observed results in this study. 12 Third, this study only used male rats, and, therefore, the results cannot be generalized across the sexes. The effect of sex on the outcomes and recovery of TBI has been emphasized in multiple clinical and animal studies. 65 –68 Given the limitation of this pilot study, future longitudinal studies should incorporate behavioral testing of the animals and histological confirmation incorporating both sexes.
Conclusion
In this study, we demonstrate for the first time that uBIH alone in the absence of the blast overpressure component results in acute mild TBI that continues to persist up to 7 days post-uBIH. These findings offer useful information in understanding the pathophysiology of uBIH-induced mild TBI. uBIH induces diffuse axonal injury and astrogliosis in the internal capsule and hippocampus. Given that similar regions were implicated in dc-bTBI, it is likely that the hyperacceleration along with the ensuing blast may synergistically lead to more comorbidities in the long term. The internal capsule and hippocampus may be potential therapeutic targets for treating bTBI and preventing delayed mental health problems.
Footnotes
Acknowledgments
This material is based on research sponsored by the United States Army grant W81XWH-13-1-0016 and by the United States Air Force grant 711HPW/XPT under Cooperative Agreement numbers FA8650-11-2-6142 and FA8650-11-2-6D04. The United States government is authorized to reproduce and distribute reprints for governmental purposes notwithstanding any copyright notation thereon. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Air Force, the Department of Defense, or the United States government.
Author Disclosure Statement
No competing financial interests exist.