
Abstract
Controversy exists regarding whether violent shaking is harmful to infants in the absence of impact. In this study, our objective was to characterize the biomechanical response of the infant head during shaking through use of an instrumented anthropomorphic test device (commonly referred to as a “crash test dummy” or surrogate) representing a human infant and having improved biofidelity. A series of tests were conducted to simulate violent shaking of an infant surrogate. The Aprica 2.5 infant surrogate represented a 5th percentile Japanese newborn. A 50th percentile Japanese adult male was recruited to shake the infant surrogate in the sagittal plane. Triaxial linear accelerometers positioned at the center of mass and apex of the head recorded accelerations during shaking. Five shaking test series, each 3–4 sec in duration, were conducted. Outcome measures derived from accelerometer recordings were examined for trends. Head/neck kinematics were characterized during shaking events; mean peak neck flexion was 1.98 radians (113 degrees) and mean peak neck extension was 2.16 radians (123 degrees). The maximum angular acceleration across all test series was 13,260 radians/sec2 (during chin-to-chest contact). Peak angular velocity was 105.7 radians/sec (during chin-to-chest contact). Acceleration pulse durations ranged from 72.1 to 168.2 ms. Using an infant surrogate with improved biofidelity, we found higher angular acceleration and higher angular velocity than previously reported during infant surrogate shaking experiments. Findings highlight the importance of surrogate biofidelity when investigating shaking.
Introduction
V
Duhaime's work has led to a longstanding controversy as to whether it is possible to harm infants by violently shaking them. The concept that “shaking doesn't hurt babies” has been discussed in the popular media. These sources highlight stories of people accused of abusing their children by shaking and quote defense experts who claim that biomechanical studies have shown that shaking an infant cannot cause subdural hemorrhages, encephalopathy, and retinal hemorrhages. Yet, extensive clinical experience resulting from a number of well-documented cases has demonstrated the harmful effects of shaking children. 6 –11 In a number of cases, adults have voluntarily reported violently shaking babies, sometimes associated with impact and sometimes not. 12,13 These infants often are found to have serious or fatal brain injuries and, in survivors, a poor prognosis. 14 –17 In addition, a program of intensive education of new parents about the dangers of shaking led to a substantial decrease in the incidence of serious infant TBI in Buffalo, New York. 18
We are left with a situation in which clinical experience is not consistent with the biomechanical data from previous laboratory experiments. 2,3 We used an instrumented anthropomorphic test device (ATD; often referred to as a “crash test dummy” or surrogate) scaled to the size of a human infant to characterize infant head kinematics during shaking. The ATD was specifically designed to have biomechanical responses similar to that of a human infant, especially as it relates to the spine and head-neck regions. We used an instrumented ATD to acquire kinematic and temporal-spatial data during shaking by an adult male.
Methods
The purpose of our testing was to characterize head-neck kinematics associated with violent shaking. Events were simulated in a laboratory setting using an instrumented infant ATD and videography.
Shaking scenario
A 50th percentile Japanese adult male (172 cm; 65.3 kg) volunteer was used to shake the infant ATD in a manner consistent with accounts given by adults who confessed to infant shaking.
Five repeat trials consisting of multiple shaking cycles (minimum of 12 cycles/trial) were conducted. The volunteer was advised to grasp the infant ATD with both hands about the upper torso just below the axillary region, suspending it in an upright posture facing them. The volunteer was instructed to “violently” shake the ATD fore and aft for a period of 3–4 sec. Videography was used to capture shaking.
Infant anthropomorphic test device or surrogate
An Aprica 2.5 infant ATD was used to conduct shaking experiments (Fig. 1). The Aprica 2.5 is a customized 12-segment, instrumented infant ATD that represents a 5th percentile Japanese newborn (GESAC, Inc., Boonesboro, MD). 19 The Aprica 2.5 has a mass of 2.6 kg and an overall length of 450 mm. Additional anthropometric and inertial properties of the ATD are provided in Table 1. As shown in Table 1, nearly one third of the ATD's mass (0.77 kg) is contained within the head, consistent with the ratio found in the human infant. 20

Aprica 2.5 anthropomorphic test device (ATD). Color image is available online at
Because of the paucity of biomechanical data describing infant response to mechanical phenomena, biofidelity of the Aprica 2.5 was established by scaling response during head impact tests, head-neck pendulum tests, chest impact tests, and lumbar flexion tests. Data were scaled from existing pediatric ATDs ranging from 6 months to 10 years of age. 19 Given that neck response is expected to greatly influence outcome measures in shaking, particular attention was given to development of the Aprica 2.5 neck. Little data exist to define the biomechanical response of a human infant neck. The ATD neck was constructed to produce an infant neck response to dynamic loading based upon scaling of adult ATD response characteristics. 21 The target neck stiffness for the Aprica 2.5 neck was determined to be 17 Newton-meter/radian (Nm/rad). 21,22 A head/neck pendulum test was used to verify the dynamic neck response. 23 Rangarajan et al. has provided an overview of the development of the Aprica 2.5 infant ATD. 19
Anthropomorphic test device instrumentation
The Aprica 2.5 ATD was instrumented with triaxial accelerometers (Kyowa ASM-200BA; Kyowa Electronic Instruments Co., Ltd., Tokyo, Japan) positioned at the center of mass of the head and at the apex of the head. Head accelerometers were oriented to allow for determination of angular acceleration in the sagittal plane. Accelerometers were calibrated following standardized procedures in accord with SAE J211. 24
Data acquisition and analysis
Data were sampled and collected at 10,000 Hz according to SAE J211. 24 Accelerometer data were filtered using a low-pass Butterworth filter with a channel filter class of 1000 Hz.
Angular acceleration in the sagittal plane was derived from linear accelerometer data. At critical levels, angular acceleration of the head has been shown to correlate with concussion, diffuse axonal injury, and subdural hematomas.
25,26
Assuming that primary motion of the head was in the sagittal plane, an estimate of head angular acceleration can be determined by the difference of the linear accelerations in the anterior/posterior direction measured at two points in the sagittal plane divided by the distance between them (Equation 1).
where:
α = angular acceleration
a1 = linear acceleration measured at head center of mass
a2 = linear acceleration measured at superior aspect of head
r = distance between the accelerometers
The distance between the accelerometers positioned at the center of mass of the head and the apex of the head was 0.0432 m.
Peak values of head angular acceleration, angular velocity, maximum change in angular velocity, and time of exposure were determined for each shaking cycle, and mean peaks with 95% confidence intervals (CIs) are reported for a given trial and across all trials. Mean and 95% CIs of sagittal plane angular displacement time histories for a representative test series were also described to assess repeatability in shaking events.
Results
Five shaking test series, each 3–4 sec in duration, were completed using the Aprica 2.5 ATD surrogate and volunteer shaker. Figure 2 illustrates the sequence of a representative shaking event. As the volunteer flexed his elbows pulling the ATD toward himself, the neck/head of the ATD extended rearward in the sagittal plane. As the volunteer extended his elbows pushing the ATD away from himself, the neck/head flexed forward in the sagittal plane. This visual sequence also illustrates that the ATD chin impacted the chest at peak neck flexion. Given the flexibility of the torso, the occiput did not contact the posterior upper torso at peak neck extension because the torso arched forward.

Kinematic sequence of one shaking cycle. Color image is available online at
Mean peak neck flexion was approximately 1.98 radians (rad; 113 degrees [deg]; 95% CI, 1.68–2.28) and mean peak neck extension was approximately 2.16 rad (123 deg; 95% CI, 1.83–2.49) during a typical shaking cycle (Fig. 3). Relatively tight CIs illustrate the repeatability of the shaking cycles. As shown in Figure 3, one cycle occurs over approximately 0.25 sec, yielding a shaking frequency of 4 Hz.
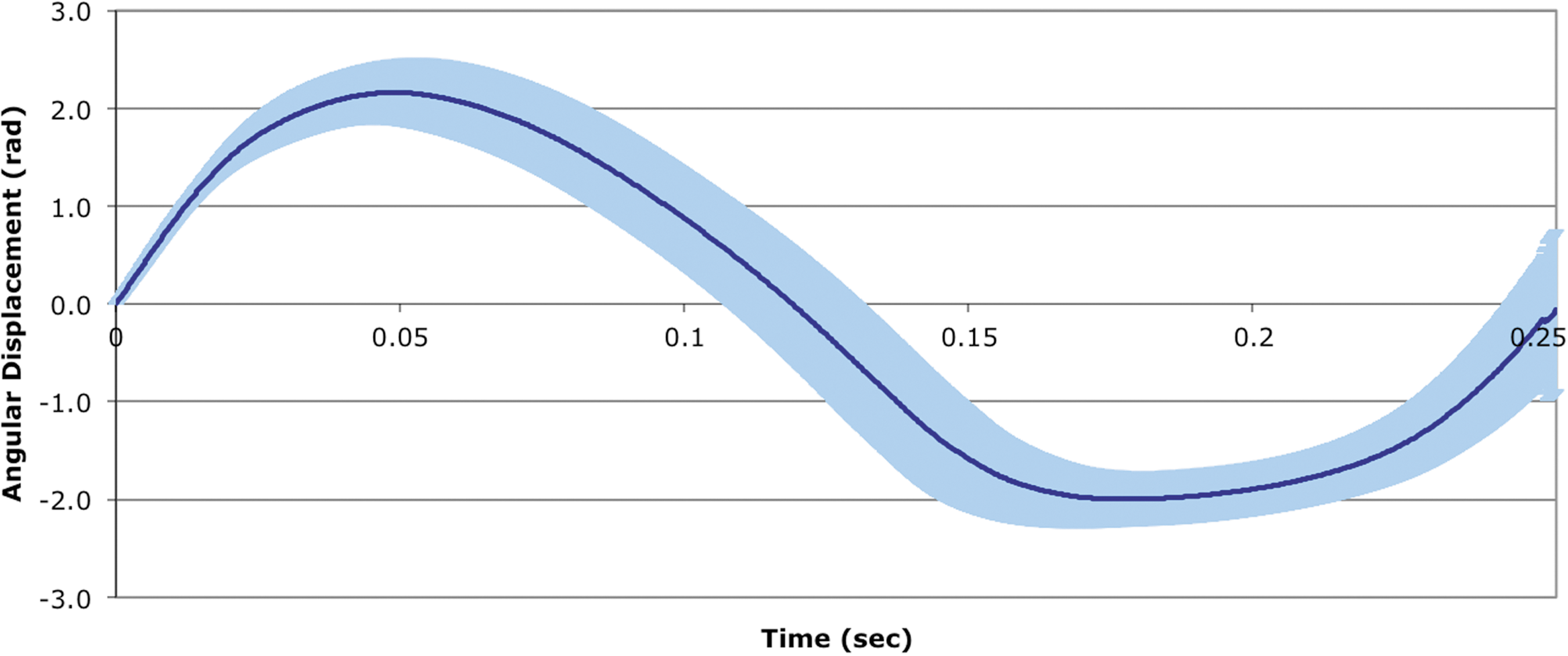
Mean angular head displacement time history for individual cycles of shaking for a representative test series (Test Series No. 3). One cycle occurs over approximately 0.25 sec (4 Hz). Positive values represent extension and negative values represent flexion. Error bars (appear as shading) represent 95% confidence intervals. Note: 1 radian = 57.3 degrees. rad, radians. Color image is available online at
Mean peak angular head accelerations in the sagittal plane fell within a range of 7035 rad/sec2 (radians/second2; 95% CI, 6168–7902) to 10,379 rad/sec2 (95% CI, 9304–11,452) across the five test series (Fig. 4). Peaks occurred during chin-to-chest contact. The maximum angular head acceleration across all shaking events was 13,260 rad/sec2 (Table 2), occurring during chin-to-chest contact in Test Series 4 during chin-to-chest contact.

Mean peak sagittal plane angular head accelerations for each test series. Error bars represent 95% confidence intervals. Ang Accel, angular acceleration; rad/sec2, radians per second2.
rad/sec, radians per second; rad/sec2, radians per second2.
Mean peak angular head velocity measured in the sagittal plane ranged from 71.2 radians/second (rad/sec; 95% CI, 68.5–73.9) to 98.4 rad/sec (95% CI, 95.71–101.1) across the test series (Fig. 5). The maximum angular velocity occurred in Test Series 2 and was 105.7 rad/sec (Table 2).

Mean sagittal plane peak angular head velocity for each test series. Error bars represent 95% confidence intervals. Ang Vel, angular velocity; rad/sec, radians per second.
The mean peak change in angular velocity was between 132 rad/sec (95% CI, 128.6–136.4) and 167 rad/sec (95% CI, 164.3–170.0) across all test series (Fig. 6). The maximum peak change in angular head velocity was 174 rad/sec in Test Series 2 and 3 (Table 2). Figure 7 presents the combinations of mean angular accelerations and mean peak change in angular velocities resulting from each test series.
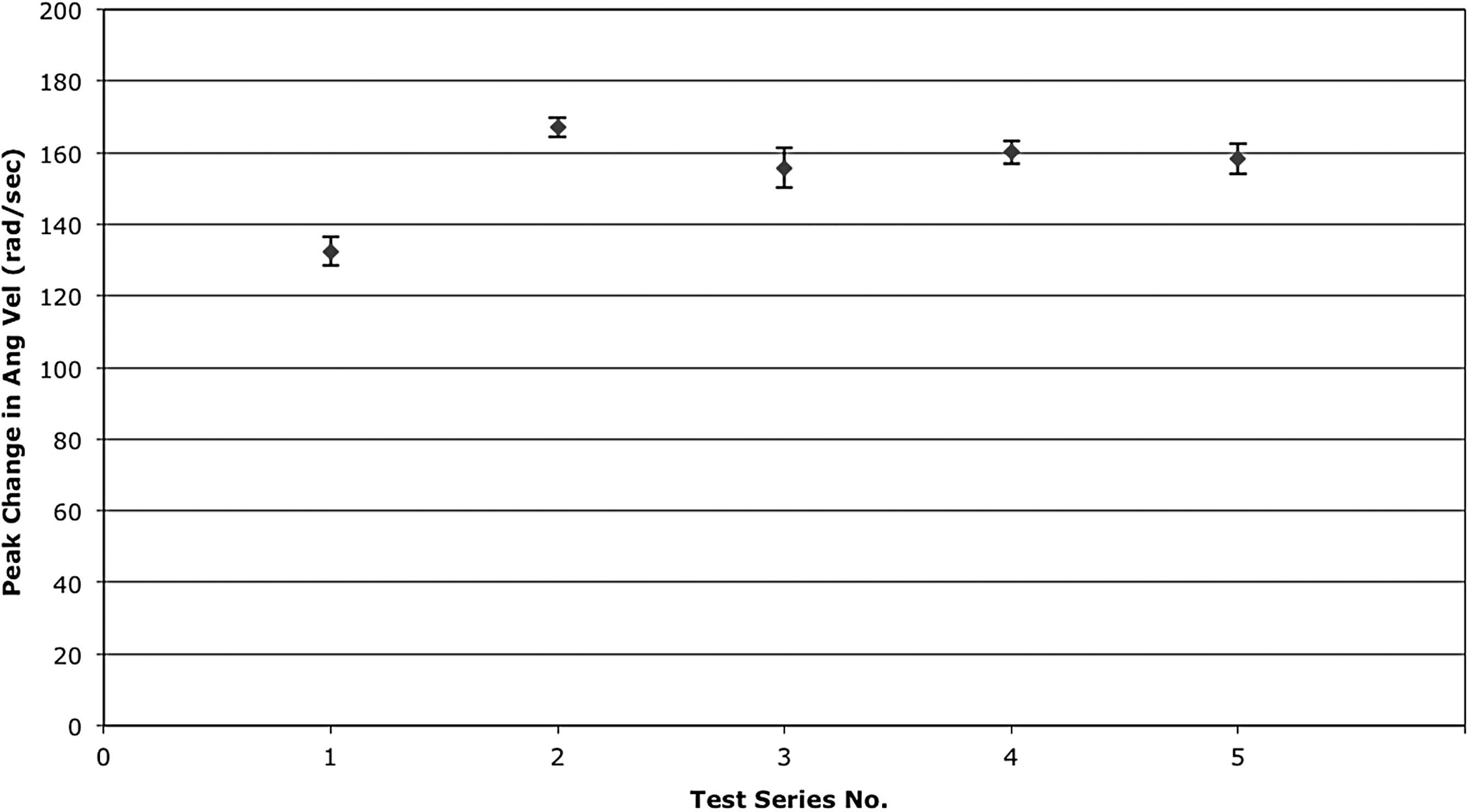
Mean peak change in sagittal plane angular head velocity for each test series. Error bars represent 95% confidence intervals. Ang Vel, angular velocity; rad/sec, radians per second.
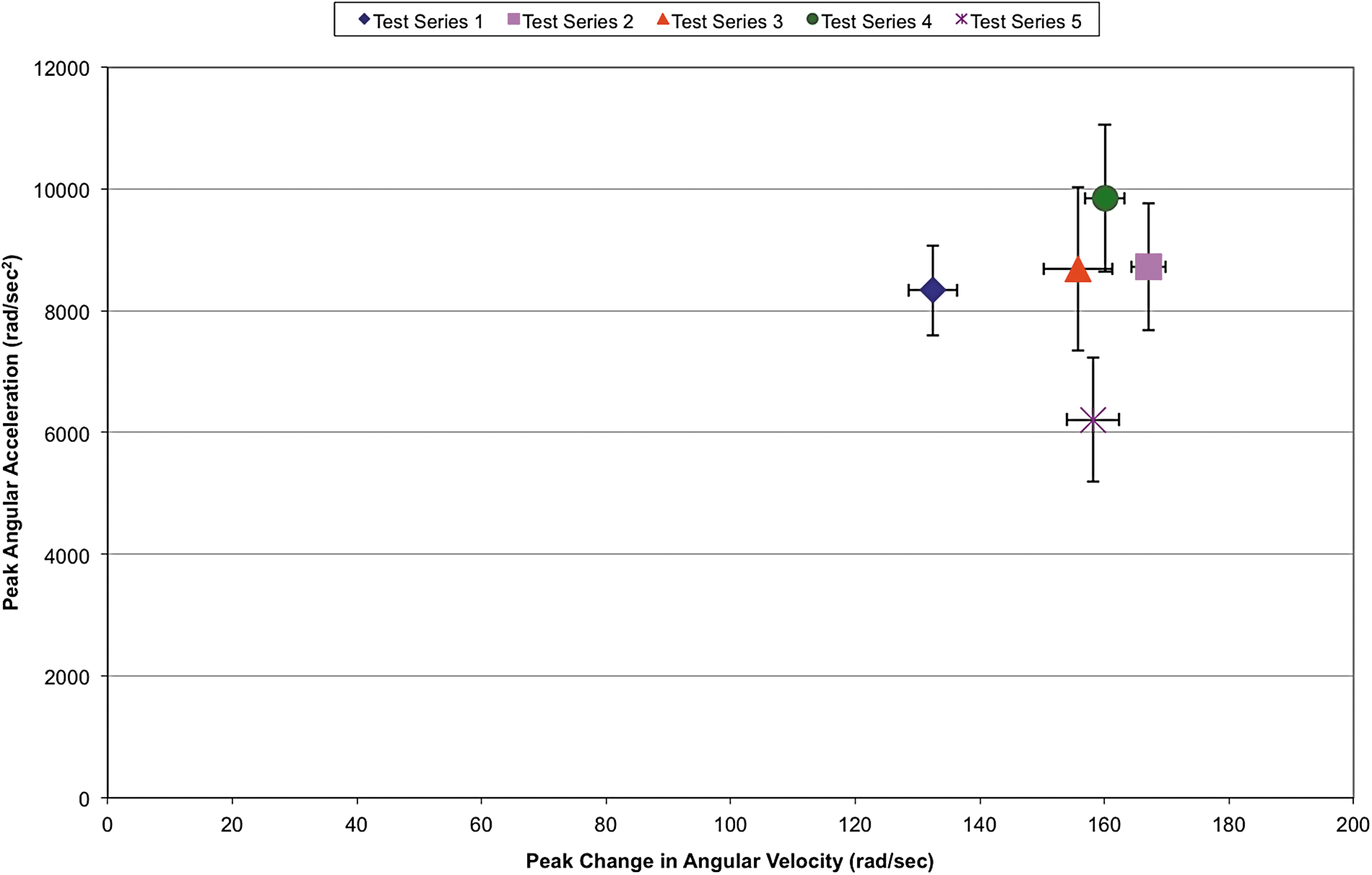
Combinations of mean angular accelerations and mean peak change in angular velocities for each test series. Error bars represent 95% confidence intervals. rad/sec2, radians per second2; rad/sec, radians per second. Color image is available online at
The mean time duration of acceleration/deceleration across the five test series ranged from 98.5 msec (95% CI, 93.2–103.8) to 137.1 msec (95% CI, 132.9–141.3; Fig. 8). The shortest duration (72.1 msec) occurred in Test Series 1, whereas the longest duration (168.2 msec) occurred in Test Series 5.
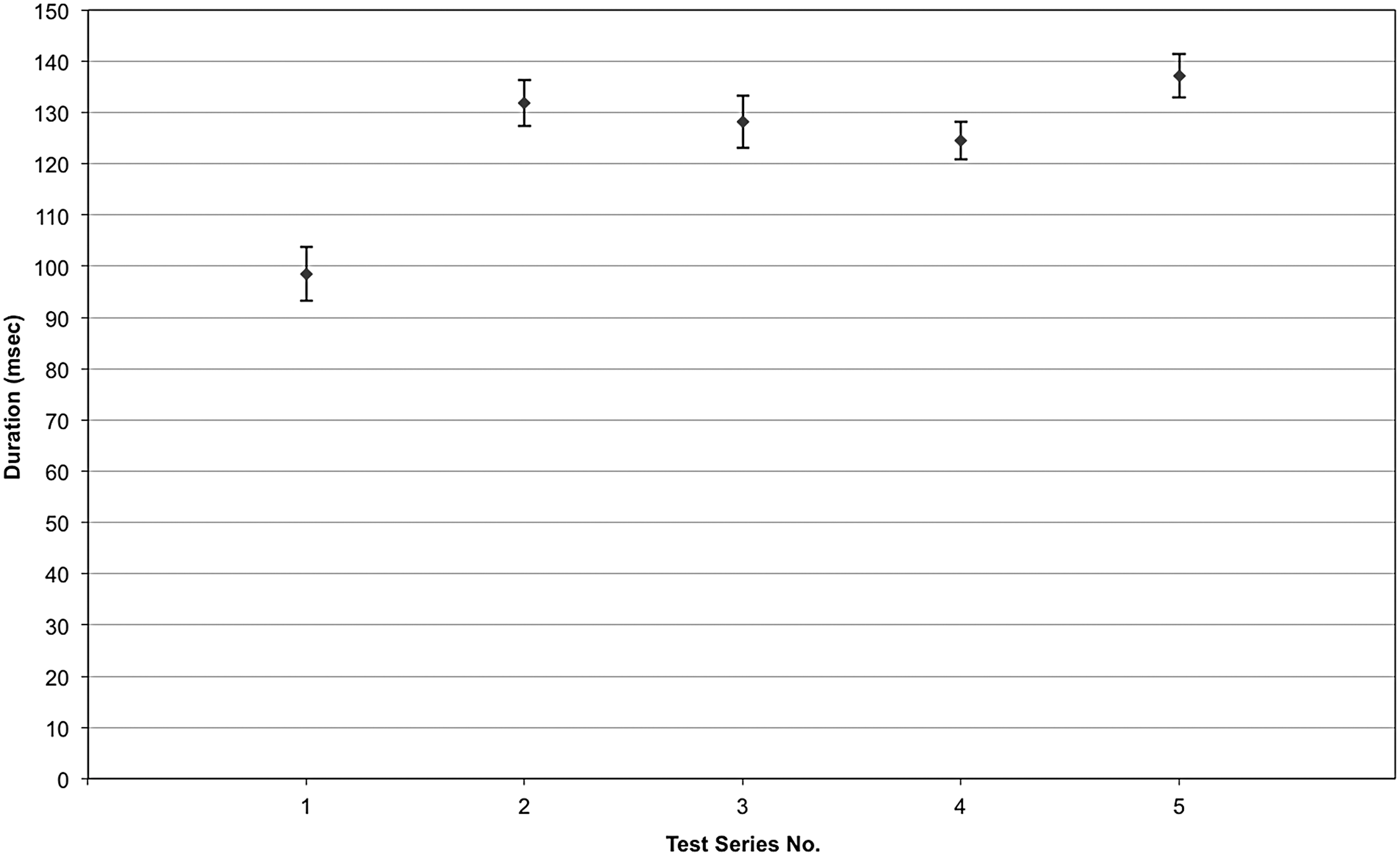
Mean time duration of acceleration/deceleration pulse for each shaking cycle each test series. Error bars represent 95% confidence intervals.
Discussion
The controversy over whether shaking alone can lead to severe TBI in infants began with the study by Duhaime and colleagues in 1987. 2 Using an infant surrogate constructed from a doll, Duhaime and colleagues found that lower angular and linear accelerations of the head were generated with shaking of the surrogate than by inflicted impact. They reported a mean angular head acceleration of 1138 rad/sec2, with a mean angular velocity of 61 rad/sec and a mean acceleration pulse duration of 107 msec in their shaking experiments.
Prange and colleagues repeated this study, attempting to improve the biofidelity of the infant surrogate, and found that inflicted impacts against hard surfaces were more likely to be associated with angular accelerations reaching injury thresholds than shaking or falls from 1.5 m or less. 3 Compared to the Prange et al. study, a recent study by Coats et al. found markedly lower peak angular acceleration and velocity, and increased pulse durations during similar impact events using an ATD with a more biofidelic neck design, a deformable, sutured skull, and a more biofidelic body mass distribution. 27 The Coats et al. study did not investigate shaking, but their differing findings compared to those of Prange for head impacts highlights the marked influence ATD design can have on injury-related outcomes.
The findings of our study differed substantially from those of Duhaime and Prange. Our maximum angular head acceleration was found to be 13,260 rad/sec2 occurring during chin-to-chest contact, a 10-fold increase over Duhaime's findings and more than twice that reported by Prange and colleagues. Further, peak angular head accelerations across all test series in our study exceeded those reported by Prange and Duhaime. Similarly, peak change in angular velocity measured in our study (174 rad/sec) was almost 3 times greater than that measured by Prange and Duhaime. The mean angular acceleration pulse duration for shaking measured in our study ranged from 98 to 137 msec and was similar to that found by Duhaime and Prange.
Differences between our findings and those of Duhaime and Prange are likely attributed to differences in the surrogates used to represent an infant and, possibly, differences in the delivery of shaking by volunteers both potentially leading to differences in head kinematics. When considered in isolation, differences in surrogate design that could lead to increases or decreases in head accelerations include the following.
Body design
The ATD used by Prange used a torso that combined the mass of arms and legs of an infant, represented as wooden structure, along with a neck and a head. The surrogate used in our study consisted of a segmented flexible torso/spine, along with a head, neck, and upper and lower extremities. A less than complete ATD body, such as that used by Prange, would reduce the overall inertial resistance to motion during shaking and could increase torso acceleration. That is, the lack of upper and lower extremities would offer less resistance to the back-and-forth motion of the torso during shaking, allowing for greater ease of torso motion.
Surrogate mass
The mass of our ATD was 2.6 kg, whereas the mass of the surrogates used by Prange and Duhaime were 4.83 and 3.0–4.0 kg, respectively. Increased mass increases the inertial resistance of the surrogate body to motion and tends to decrease torso acceleration.
Head mass
The mass of the surrogate head used in our study was 0.77 kg, wheras the head mass of ATDs used by Prange and Duhaime was 1.13 and 0.77–0.87 kg, respectively. The lower head mass used in our study would offer less inertial resistance, leading to higher head accelerations with shaking.
Neck structure and stiffness
Neck structure and stiffness play a critical role in the head's response to shaking. Duhaime and colleagues examined the effects of various neck designs and found that a resistance-free hinged neck design was associated with the highest head accelerations with shaking. 2 Prange and colleagues utilized a negligible-resistance hinge neck to generate a worst-case head acceleration scenario. 3 The neck assembly used in our surrogate consisted of urethane tubing with a centered safety cable joining superior and inferior aluminum plates that allowed for head-neck rotation in the sagittal, coronal, and transverse planes. The safety cable was adjusted to provide desired neck-bending properties (Fig. 9). 19 Duhaime and Prange did not report on neck properties of their surrogates, but given the negligible resistance offered by their hinge structures, we estimate that our surrogate neck was likely stiffer and provided greater resistance to head-neck motion during shaking. Both surrogates used by Duhaime and Prange constrained head-neck motions to the sagittal plane (anterior-posterior directions) by utilizing a hinged neck (worst-case scenario), whereas our surrogate's neck was free to move in three planes. When considering the constraint of head-neck motion in the sagittal plane in isolation, it would tend to increase head accelerations during shaking, given that out-of-plane lateral motion is not permitted.

Aprica 2.5 ATD neck flexion properties derived from pendulum impact testing. deg, degrees. Color image is available online at
Whereas it is interesting to study surrogate design characteristics in isolation of one another, one characteristic may outweigh or nullify the influence of another characteristic when the surrogate is considered as a whole (i.e., all characteristics together). Such is the case with head motion constraint or lack thereof. That is, even though the lack of head motion constraint tends to decrease head acceleration (as compared to constrained head motion), other design characteristics had a greater bearing on the resulting head acceleration in our experiments. It is the combination of surrogate design characteristics (e.g., head mass, neck length, torso stiffness, surrogate mass, neck stiffness, etc.), along with severity of shaking that dictate the resulting head acceleration. Together, these factors drive key kinematic features of the head, such as chin-to-chest contact, which can generate large peaks in head acceleration. Chin-to-chest contact occurred in our experiments and was associated with peak head accelerations, but was not reported in experiments conducted by Duhaime and Prange. This kinematic feature likely contributed to head accelerations exceeding those measured by Duhaime and Prange during shaking experiments.
Another study examining biomechanical outcomes during shaking of an infant surrogate was conducted by Cory and colleagues. 4 They reproduced the Duhaime 1987 experiments using an adjustable replica of their surrogate to determine the influence of surrogate parameters on head response outcomes during shaking, varying head-neck joint location (i.e., occipital condyle location), neck construction (rubber neck vs. hinged neck), torso padding (cotton wool vs. silicone), and location of the surrogate center of gravity (CG). Under a combination of worst-case parameters, Cory measured a peak angular head acceleration of 10,217 rad/sec2 and a peak angular head velocity of 61 rad/sec. Cory's results exceeded peak angular accelerations reported by both Duhaime and Prange and approach those measured in our experiments. 2,3 Cory found that the combination of a high surrogate CG, hinged neck, and cotton wool padded torso produced worst-case angular head acceleration values.
One of the differences between the Aprica 2.5 ATD and the surrogate used by Cory is the flexibility of the thoracic spine and torso stiffness. During shaking, Cory and colleagues described both chin-to-chest and posterior head-to-posterior torso contact (likely contributing to higher accelerations than those measured by Duhaime and Prange). The Aprica 2.5 ATD also displayed chin-to-chest contact, but the posterior aspect of the head did not contact the torso during shaking. The Aprica 2.5 ATD has a flexible thoracic spine, allowing for arching of the torso during the extension portion of shaking, which diminishes the likelihood of head contact torso, thoracic spine, or with the posterior torso. Cory and colleagues did not quantify torso, thoracic spine, or neck properties of the surrogate used in their study, and thus a direct comparison with the Aprica 2.5 ATD torso, thoracic spine, and neck was not possible.
The location of the center of rotation of the head also influences the rotational response of the head to shaking. That is, for a given shaking event, as the distance to the center of rotation increases in length, the angular acceleration would decrease, assuming all other parameters were held constant. Although the Aprica 2.5 ATD neck joins the torso at a point 5 cm below the base of the skull, the design of the neck allows for a moving center of rotation as the head rotates. This can effectively provide a radius of rotation that is less than 5 cm in length at various points in the head's rotation about the neck. In contrast, the surrogates used by Duhaime, Cory, and Prange that led to worst-case head accelerations had fixed centers of rotation that were located 3.3, 3.3, and 4.5 cm, respectively, below the base of the skull. The Aprica 2.5 ATD neck allowed for a moving center of rotation mimicking that of a human infant. Given this moving center of rotation (i.e., the center of rotation can change during neck flexion/extension), it is difficult to evaluate how the neck center of rotation would affect angular head acceleration in comparison to the surrogates used by Duhaime, Cory, and Prange. In general, if the Aprica 2.5 ATD center of head rotation was located such that the radius of rotation was less than that of the other surrogates, there would be a tendency toward increased angular head acceleration for a given shaking input.
To determine the likelihood of injury from exposure to a given phenomenon (i.e., impact or shaking), outcome measures known to be associated with injury risk are typically compared to published injury thresholds. During Aprica 2.5 ATD shaking experiments, injury threshold levels for concussion reported for primates with 400-g brains (similar in mass to a young infant) were exceeded, 28 whereas published injury thresholds for diffuse axonal injury were not exceeded. 26 To date, however, there are no validated infant brain injury thresholds. Scaling thresholds from adult cadaver and primate studies to infants based on brain mass alone can produce misleading pediatric TBI thresholds. 29 Other factors, such as brain material properties and geometry, must also be considered when attempting to assess brain injury risk. 30 Further, published pediatric TBI thresholds fail to account for repetitive exposure to acceleration or deceleration that occurs in shaking, but instead consider only exposure to a single event. Repetitive TBIs in animal models have been shown to cause greater injury at lower peak rotational velocities than do single impulse loads. 31 The effects of repetitive cyclic events, such as those involved in shaking, have not been systematically studied in animal models other than mice and piglets. 32,33
The duration of exposure to acceleration is also an important factor when attempting to predict the risk of and type of brain injury that can result from an event. In our experiments, duration of exposure (i.e., acceleration pulse duration) ranged from 72.1 to 168.2 msec. Löwenhielm and colleagues described accelerations and associated pulse durations of 15–44 msec leading to subdural hematomas, substantially shorter pulse durations than experienced by our ATD during shaking. 34 Ommaya and colleagues found that lower levels of acceleration are capable of producing injury in cases of longer pulse duration. 35 Genaralli and Thibault suggested that longer acceleration pulse durations permit brain tissue strains resulting from accelerations to propagate deeper into the brain, leading to functional damage found in cerebral concussion or structural damage found in axonal injury. 25
Other studies have noted the extreme vulnerability of the infant brain to the metabolic effects of brain injury when compared to the adult brain. 36,37 This would suggest that the infant brain is more susceptible to injury and might account for the poor outcomes noted in children surviving abusive head trauma (AHT). 15,16 Another worrisome aspect of infant abuse that could account for the hypoxic injury to the brain is the finding that in a large percentage of infant abuse cases resulting in death, subtle injury to the high cervical cord and lower brain stem is observed on autopsy. 38 It is postulated that these cord injuries could lead to apnea or changes in autoregulation of cerebral blood flow, causing the typical hypoxic changes observed in infant victims of AHT.
The influence of shaking on the infant brain and the pathophysiology of infant brain injury is more complicated than can be represented in existing surrogate models used in biomechanical shaking experiments. For example, the immature brain could be more vulnerable to angular acceleration than the adult brain. Raghupathi and colleagues found the immature piglet brain to be more vulnerable to a single inertial load than that of the adult pig brain. 39 They also found that repeating an inertial load on the piglet head twice, 15 min apart, led to more diffuse axonal injury in the piglet brain and to a significant decrease in arterial blood pressure 60 min post-injury. 33 Given that violent shaking of infants involves repetitive inertial events occurring within a few seconds, the mechanical phenomena necessary to cause injury in the immature brain could be less severe than would be necessary to cause a single impact injury. In addition, surrogate experimental outcomes do not take into account the well-known deficits in cerebral autoregulation that occur after infant brain injury, leading to profound cerebral hypotension and hypoperfusion. 40
These factors suggest that the infant brain is likely more susceptible to injury than the adult brain. Taking these factors into account, predictions of risk based upon comparison with published brain injury thresholds are not likely to be reliable given the limitations inherent in these thresholds.
Another factor that complicates the estimation of infant brain injury thresholds is the fact that infants who experience AHT are often subjected to multiple bouts of trauma over days to weeks. Several studies have shown that infants presenting with AHT are likely to have suffered previous AHT. 41 –43 Using an animal model, Huh and colleagues demonstrated a graded pathological response to repetitive mild injury in immature rats. 31 Rats experiencing three mild impacts to the head (not resulting in fracture) over 15 min developed axonal injury and brain atrophy, compared to rat pups receiving only a single mild impact. When an immature brain experiences multiple injuries, some “priming” might occur that makes the brain more susceptible to damage from subsequent injuries. Additionally, vulnerable infant axons within the brain may not be capable of repair between bouts of trauma. These phenomena may effectively lower infant brain injury thresholds, which are used to predict probability of injury when compared to experimental outcomes such as angular acceleration.
In addition to the lack of data on the biomechanical properties of the infant neck, animal models may not adequately represent the lack of supporting musculature found in the human infant neck. 44 However, the neck of a newborn goat has been estimated to be equivalent in strength to the neck of a 1-year-old human. 45 When studying the effects of shaking, the lack of protective infant neck musculature is a key factor that must be represented in any model.
This study is limited by the inability of any currently available ATD to represent the biomechanical characteristics of an infant with complete accuracy. The Aprica 2.5 ATD, however, was designed to match a newborn infant's anthropometrics and to be biofidelic within the limits of technology and published human response data. In addition, only one volunteer was used to induce shaking of the ATD. Using multiple individuals for ATD shaking may produce varying inputs, leading to a different biomechanical response. However, our intent was to investigate shaking response generated by a nominal representative average (50th percentile) male, providing the first step toward understanding the influence of improved ATD biofidelity. Similarly, one's interpretation of the instruction to “violently” shake the ATD is subjective and may vary across individual shakers. However, the volunteer shaker used in this study was educated on perpetrator actions when abusively shaking a child and was asked to replicate shaking that would occur during rage or anger. Methods used to estimate angular acceleration and velocity were limited by ATD instrumentation. Finally, the Aprica 2.5 ATD represents a small newborn infant. Shaking an ATD representing an older infant would undoubtedly lead to a differing biomechanical response attributed to differences in mass, neck flexibility, and torso/spine flexibility.
Higher levels of angular acceleration and angular velocity measured using the instrumented Aprica 2.5 ATD during shaking, and attributed to chin-to-chest contact, suggest a higher potential for injury with shaking alone than previously reported. These findings parallel clinical experience documenting that violent shaking of infants is potentially harmful. 46 –48 This study also demonstrated the importance of biofidelic ATD torso/spine and head-neck regions when investigating kinematics associated with shaking. Although biofidelic ATDs can improve our understanding of kinematics during shaking, infant neuropathological response to measured accelerations and velocities still remains unclear.
Footnotes
Acknowledgments
This study was supported by the Aprica Childcare Institute (Nara, Japan). This article is dedicated to Tariq Shams, one who embodied generosity, kindness, and genius.
Author Disclosure Statement
Drs. Jenny, Bertocci, and Rangarajan have testified in courts of law regarding infant TBI.