
Abstract
Individuals with spinal cord injury (SCI) experience life-threatening cardiovascular events and various autonomic consequences in addition to the well-appreciated motor and neurological impairments. As a result, cardiovascular disease is a major cause of death after SCI, corresponding to a two-to-fourfold increased risk of cardiovascular events. A combination of neuroanatomical changes, unstable blood pressure, and rapid deconditioning as a result of decreased physical activity likely contributes to accelerated cardiovascular disease progression after SCI. Aortic pulse wave velocity (aPWV) is considered the gold-standard technique for evaluating central arterial stiffness, which itself is a correlate for greater cardiovascular disease risk in healthy individuals and a plethora of clinical conditions. In this review, we discuss central arterial stiffness after SCI, and demonstrate that it is consistently elevated in this population 2–3 m/sec, which corresponds to a 30–45% increased risk of cardiovascular mortality and an approximate 40-year acceleration of age-related cardiovascular decline. The potential factors contributing to increased central arterial stiffness are also reviewed in light of the available literature, including autonomic disruptions, blood pressure instability, metabolic changes, and physical inactivity. Further, measurement techniques, risk factors, cardiac dysfunction, and differences in arterial stiffness from able-bodied populations are discussed. Finally, potential therapeutic interventions for preventing or improving central arterial stiffening are also explored, including dietary, physical activity, and pharmacological strategies.
Introduction
C
Presently, a variety of techniques are used to assess central arterial stiffness, including but not limited to, direct vascular morphometrics using ultrasound or magnetic resonance, 16 waveform decomposition, 17 and pulse wave velocity. 18 Aortic pulse wave velocity (aPWV) has been touted as the “gold standard” of measuring central arterial stiffness, because of its noninvasive nature, high reproducibility, and strong predictive value. 18 –21 In turn, aPWV is calculated using distance travelled between the common carotid artery and common femoral artery, multiplied by a scaling factor of 0.8 and divided by the pulse transit time between the carotid and femoral arterial waveforms. 22,23 An individual presenting with aPWV of >10 m/sec is considered at elevated risk of a cardiovascular (CV) event and likely has significant subclinical vascular end-organ damage. 18 Every 1 m/sec increase in aPWV corresponds to an increased risk of 14% for total CV events, and a 15% increased risk for mortality when adjusted for age, sex, and risk factors for CV disease (such as diabetes and smoking). 24 Clinically, stiffness of the aorta is a sensitive measure for CV disease because of its central location within the circulatory tree, highly elastic composition, and, therefore, high susceptibility to stiffening and atherosclerosis. 25 –27
Physiologically, increasing central arterial stiffness is not simply a correlate of declining end-organ vascular health, but exerts its own direct deleterious impact on the CV system. To explain further, during systole, the left ventricle contracts to eject blood, generating the arterial pressure waveform. 25 This waveform travels away from the central arteries in the periphery, with the cumulative resistance resulting in a reflected proximally travelling pressure waveform. 25 In a healthy and elastic arterial system, this reflected waveform travels proximally at a sufficient delay such that it arrives in diastole, and contributes to coronary artery filling. The vast majority of this buffering effect occurs at the level of the aorta, because of its highly elastic nature. 25,28 In the stiffened arterial system in which aortic buffering capacity is impaired, the pulse wave travels at a higher velocity and is reflected earlier, in late systole that reduces the capacity for coronary artery perfusion. Further, as a consequence of the cumulative effect of forward and reflected pressure waveforms being superimposed on each other, systolic blood pressure (SBP) rises, with a corresponding increase in central pulse pressure. This elevation in blood pressure results in a greater left ventricular workload, which is associated with left ventricular hypertrophy and compromised coronary perfusion. 1,25,29 These structural and hyperemic changes are themselves independent risk factors for cerebrovascular disease and myocardial infarction, and demonstrate that central arterial stiffening is not just a marker for CV disease risk, but also exerts a direct deleterious effect on the CV system (see Fig. 1). 26,30,31
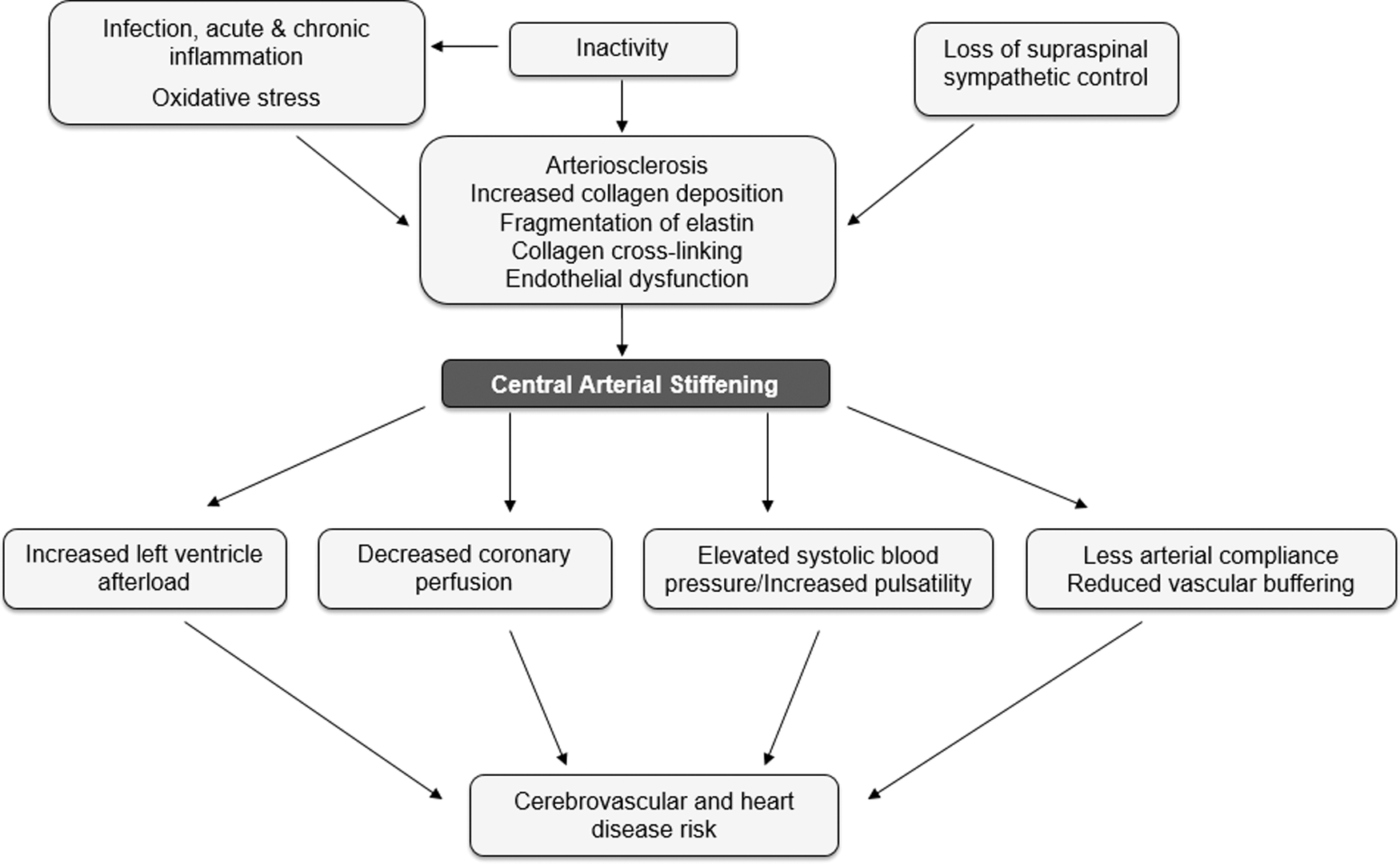
The “central“ prognostic role of central arterial stiffness after spinal cord injury. Central arterial stiffness is tightly linked with numerous critical functions of the systemic vasculature. This includes the buffering capacity of the aorta, endothelial function, and profibrotic remodelling. The combination of these factors, and the relatively small influence of acute hemodynamic changes (when covariating for distending pressure) is considered to represent the total arteriosclerotic burden. In addition to this, rigid central arteries are not only prognostic, but are also known to induce their own deleterious physiological effects on the cardiovascular system, including decreased coronary artery perfusion due to augmented reflected waveform velocity, higher systolic blood pressure, and left ventricular afterload, and increased traumatizing blood flow/pressure pulsatility. Following this, increasing central arterial stiffness is both a cause and effect of increased cardiovascular risk.
Central Artery Stiffness after SCI: Implications and Contributing Factors
Central arterial stiffness is elevated in those with SCI, and there is substantial evidence for compromised central arterial structure and function when those with SCI are compared with uninjured individuals (see Tables 1 and 3). In terms of aPWV, there is consistent evidence of accelerated arteriosclerosis in those living with SCI: on average, those living with this condition have an aPWV that is increased 2–3 m/sec compared with AB individuals, 29,32 which corresponds a staggering 40 year acceleration of age-related CV decline. 22 A number of factors contributing to post-SCI arterial stiffness have been implicated, however, these require further elucidation (see Fig. 2). For example, those with SCI have been reported to be living in a state of chronic inflammation, which is a well-established risk factor for generalized CV disease progression. 33,34
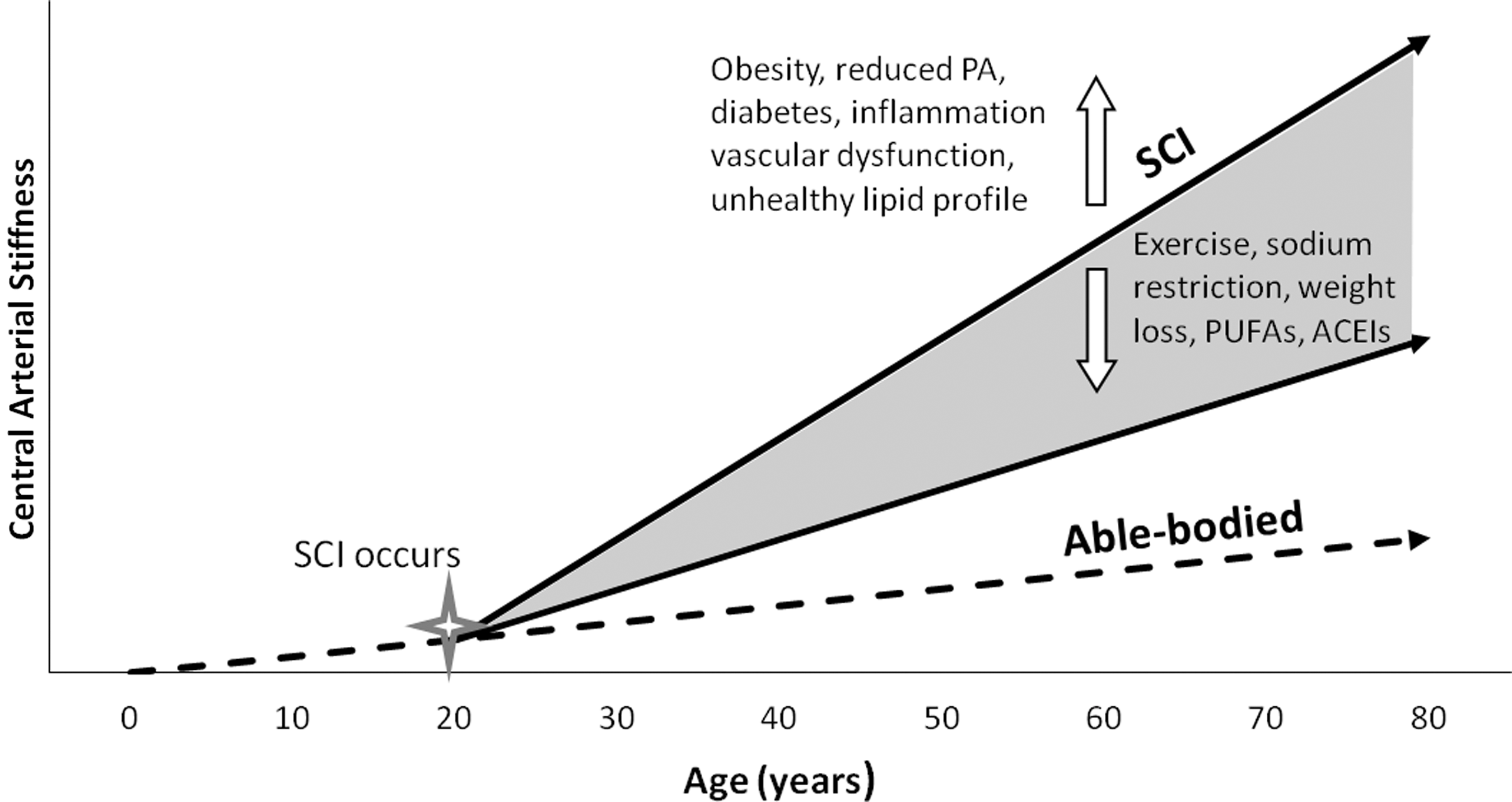
Trajectory of age-related decline in central arterial stiffness following spinal cord injury (SCI), which is accelerated with risk factors such as: obesity, chronic and acute reduced physical activity (PA), diabetes, inflammation, vascular dysfunction, and unhealthy lipid profile. Interventions that further modify this progression and mitigate arterial stiffening include aerobic exercise, sodium restriction, weight loss, increased consumption of omega-3 polyunsaturated fatty acids (PUFAs), and antihypertensive drugs such as angiotensin-converting-enzyme inhibitors (ACEIs).
AB, able-bodied; SCI, spinal cord injury; CCA, common carotid artery; CFA, common femoral artery; AIx, augmentation index; PWV, pulse wave velocity; aPWV, aortic PWV.
Significant differences between AB and SCI central arterial stiffness values.
AB, able-bodied; SCI, spinal cord injury; aPWV, aortic pulse wave velocity; AIx, augmentation index; β index, beta-stiffness index.
Blood pressure lability
Profibrotic remodelling has been shown to occur in response to heightened renin-angiotensin-aldosterone system (RAAS) activation, 35 and those with SCI have increased reliance on this system for blood pressure maintenance. 36 Considering that elevated blood pressure is one of the most powerful risk factors for advanced central arterial stiffening, it is likely that SCI patients exhibit increased PWV as a result of episodes of hypertension associated with autonomic dysreflexia. This condition is characterized by life-threatening rapid unregulated increases in blood pressure that occur on a daily basis in the majority of those with high level SCI (at T6 or above). 37 –39 Interestingly despite transient hypertension, those with high level SCI most commonly have low resting blood pressure and sustain further rapid blood pressure declines when moving from a supine to upright posture, termed orthostatic hypertension (OH). The role that OH plays in aortic stiffening is unknown.
Impaired sympathetic nervous system (SNS) function
Disruption of the SNS almost certainly contributes to the development of arterial stiffness after SCI. In the uninjured individual, sympathetic preganglionic neurons (SPNs) innervate target organs such as the heart, arteries, and veins to maintain CV homeostasis. 38,40 Activation of the SNS is excitatory, resulting in an overall increase in blood pressure by way of systemic vasoconstriction and increased heart rate. 38 In the acute phase of SCI after supraspinal pathways are disrupted, an initial atrophy of SPNs and reduction in central sympathetic tone results in hypotension, bradycardia, and other vascular abnormalities because of the critical role that the SNS plays in CV regulation. 41,42 Although acute increases in sympathetic activation can lead to increased aortic stiffness, chronic sympathectomy in fact leads to profibrotic aortic remodelling and increased stiffness, with low blood pressure being a secondary consequence of the loss of SNS input. 43 –45 In contrast, acute increases in sympathetic activity certainly lead to acute increases in stiffness. 46 –49 Considering, however, that SCI leads to chronic disruption of sympathetic pathways, one would expect increased aortic stiffening after high-level SCI, which has been shown previously. 32,50,51
Deconditioning
Another factor likely playing a role in central arterial stiffening after SCI is rapid deconditioning of not only skeletal muscle, but also of the vascular smooth muscle. 52 It is likely that central arterial stiffening rapidly occurs in the acute phase of SCI, as other vascular beds have shown remarkably prompt declines in structure (i.e., femoral artery inward remodelling). 52 –54 Similar specific CV deconditioning occurs in both SCI and prolonged bed rest, resulting in increased RAAS activity, 41 decreased stroke volume, 55 reduced cardiac size, 56 lower resting blood pressure, 37 and orthostatic intolerance. 57 Presently, it is not specifically understood how and when central arterial stiffening occurs in the acute phase of injury, nor has the role of early versus late mobilization/rehabilitation in this important metric of CV disease risk been explored. This knowledge may greatly increase the capacity to prevent the decline during the period of most severe changes. In non-SCI populations, reduced arterial elasticity occurs with both chronic sedentarism and acute bed rest, which is potentially the result of a number of factors recently reviewed, including oxidative stress, inflammation, an unhealthy lipid profile, and reduced healthy shear stress, 58 –61 which together comprise severe vascular deconditioning and impaired endothelial function. 62,63 With respect to SCI, arterial compliance has been found to be lowest in SCI compared with both AB athletes and non-athletes. 63 When matched for age, sex, weight, and height, SCI individuals without exercise training had markedly lower arterial compliance than trained SCI, untrained AB, and trained AB individuals. 64 Central arterial stiffness was found to be inversely related to physical activity levels in the SCI population. 32 Interestingly, in this latter study, it was shown that some metrics of central arterial stiffness, but not others, were related to physical activity levels after SCI, suggesting that other factors affecting health after SCI are playing a significant role. In light of the evidence, it appears that bed rest and physical inactivity need to be considered as critical factors leading to increased central arterial stiffening after SCI.
Injury level
It is crucial to appreciate that within the human SCI population, there is a great degree of variability of CV function that is directly related to the specific level and degree of injury: individuals with higher lesion levels experience more severe CV abnormalities such as transient bouts of hypertension (autonomic dysreflexia). 39,65,66 Injury level and completeness of injury is, therefore, an important issue when considering aortic stiffness. Recently, a small study found that those with high level SCI (cervical: C2–C8) had less aortic stiffening than those with lower level thoracic (T2–T12) injuries. 50 This is highly surprising considering that every risk factor for increased central artery stiffness listed is reduced in those with lower level injuries. 39,41,67 –70 The rationale for this finding is unknown, but may be attributed to small sample size, or statistical (as opposed to physiological) normalization for lower mean arterial blood pressure. 71 Evidently, further investigation is needed to clarify this interesting finding, and to ascertain the relationship between lesion level and aortic stiffness.
Interventions for Improving Central Arterial Stiffness
A variety of interventions have been reviewed for their potential efficacy to decrease arterial stiffness. These are detailed below and in Table 2.
Recommendation for SCI.
AB, able-bodied; SCI, spinal cord injury; PWV, pulse wave velocity; aPWV, aortic PWV; PUFAs, polyunsaturated fatty acids; PM, postmenopausal; AASI, ambulatory arterial stiffness index; AIx, augmentation index; AGE, advanced glycation end-product crosslink breaker; ACEI, angiotensin-converting-enzyme inhibitors; RAAS, renin–angiotensin–aldosterone system; ARB, angiotensin receptor blocker; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; ALT-711, alagebrium chloride.
Exercise
Aerobic exercise is a tenet of healthy living in the AB population, and can significantly reduce a number of CV risk factors. 72 –76 Even brief periods of routine aerobic exercise can significantly improve central arterial stiffness in AB populations. 77 –80 As little as 13–14 weeks of aerobic exercise (5.3 ± 0.2 days/week, 42 ± 1 min/day) yielded improvement in a sample of AB middle-aged and older men. 79 However, these effects do vary along with the type of exercise employed, and baseline arterial stiffness of the participant (aerobic exercise was more efficacious for reducing stiffness when performed at higher intensities, and for participants with more rigid baseline). 61 Conversely, resistance training in AB subjects is reported to either increase or have no effect on central arterial stiffness across multiple exercise intensities and modalities (i.e., lower limb vs. upper limb training). 81
The therapeutic potential of exercise training is more ambiguous in SCI populations. Considering that those with SCI often have stiffer central arteries, exercise should be a viable therapy in this population. 32,50,51 The evidence is not so clear, however. For example, some cross-sectional data demonstrate that athletes with SCI display significantly less arterial stiffness than both AB and SCI non-athletes, 51,64 and that there is similar large arterial compliance between AB and SCI groups when matched for physical activity. 32 Further, recent data where those with SCI adhered to physical activity guidelines for adults with SCI (i.e., two times/week of 20 min moderate to vigorous aerobic exercise combined with both upper body and hybrid resistance training) yielded no improvement in central arterial stiffness or endothelial function. 82 These surprising results were attributed to a lack of differentiation between aerobic and resistance exercise and a large influence of a non-physical- activity-dependent mechanism that is not compensated for by upper body exercise alone, as well as variability in outcome measurements. It is possible that routine upper body exercise after SCI is insufficient to modify central arterial stiffness in the same positive manner that whole body exercise elicits in AB populations. In support of this contention, the only study to look at routine upper body exercise in a non-SCI population showed that moderate to vigorous arm cycling three times a week for 12 weeks in AB hypertensive patients also did not improve central arterial stiffness. 83 Together, these findings indicate a need to further establish understanding of exercise as therapy for SCI individuals experiencing CV complications, particularly with regard to which category is most effective (upper body and/or lower body; continuous vs. interval vs. resistance training). No study to date has assessed the role of specific upper versus lower body exercise intervention in central arterial health over a sufficient duration, nor has there been a longitudinal comparison and combination of different exercise methods.
Diet
A number of dietary interventions have shown promise in reducing arterial stiffness in the AB population, such as omega-3 polyunsaturated fatty acids (PUFAs), 84 soy isoflavones (plant-derived compounds found in legumes and beans), 85 and fermented-milk products. 86 Most notably, central PWV was reduced by chronic (but not acute) consumption of the PUFAs eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA), 86 and combined intake of EPA and DHA showed the largest clinical effect in reducing arterial stiffness among all PUFA trials. 84 Several randomized controlled trials have explored other dietary changes as a means of reducing arterial stiffness, finding isoflavones 87 and fermented milk supplements had a positive impact, 86,88,89 but that generalized vitamins, micronutrients, and herbal supplements did not.
Apart from dietary supplementation, chronic restriction of sodium and caffeine has been suggested as a therapy for improving central arterial stiffness, as the acute intake of these substances is associated with increased vasoconstriction and arterial stiffness. 86 Chronic restriction of sodium intake has yielded improvement in arterial stiffness as measured by aPWV. 90,91 High sodium levels are associated with increased arterial stiffness through increased collagen production and cross-linking, as well as activation of RAAS 92 and impaired endothelial function. 34,93 Another dietary intervention included a low-cholesterol/low-saturated fat diet for 8 weeks, which also yielded significantly decreased aPWV from baseline in hypercholesterolemic patients. 94 In AB populations, liver fat and serum triglycerides were found to be independent predictors of aPWV, suggesting the therapeutic potential of reducing hepatic fat. 95 Unfortunately, no studies have evaluated the potential role of any of these interventions in improving arterial stiffness in SCI. It is suspected that PUFA dietary supplementation would be a promising therapy because of its capacity to improve arterial stiffness without exacerbating hypotension after SCI. 86,96 On the other hand, sodium restriction does not seem to be a viable therapy, as sodium intake is critical to maintaining blood volume after SCI. 41,97
Pharmacology
A number of pharmacological interventions have been studied for their potential impact on reduction of central arterial stiffness. Statins, in particular fluvastatin, have been shown to be moderately impactful in the AB population. 98,99 Unfortunately, when looking at statin therapy itself, more clarification is required regarding dosing, specific statins used, and populations in which these are effective. For example, following statin therapy, central arterial stiffness as measured by aPWV has been found equivocally to decrease, increase. and change nonsignificantly across various studies. 99 Further, these studies assessed only AB participants who were typically hypertensive or hypercholesterolemic. Another therapy currently being evaluated for improving central arterial stiffness in the AB population is advanced glycation end product (AGE) cross-link breakers, which operate on the basis of “de-stiffening” therapy, by interrupting the cross-linkages of proteins such as collagen. The findings are promising, and have yielded reductions in age-related vascular stiffening independent of blood pressure. 100
By far, antihypertensive drugs have demonstrated the most consistent and efficacious reductions in vascular stiffness in the non-SCI population. Pharmaceuticals that inhibit the RAAS such as angiotensin-converting enzyme inhibitors (ACEIs) and aldosterone receptor blockers (ARBs) ameliorate aortic stiffness in hypertensive patients; combining the two has a potentially synergistic effect in reducing aPWV. 101 Although the rationale for administering antihypertensives appears tenuous given the high incidence of low resting blood pressure in SCI individuals, 57 these drugs do not operate exclusively by lowering blood pressure. Anti-inflammation-based reduction in arterial stiffness has been examined in thiazolidinediones 102 and ACEIs. Given that ACEIs inhibit production of angiotensin II to counter inflammation, fibrosis, and vascular stiffening without drastically affecting brachial SBP, 103,104 this drug class remains worthy of consideration for testing in SCI patients, particularly in combination with ARBs to target aortic stiffness.
Conclusions
Central arterial stiffness is a robust and powerful index of CV health that is higher in individuals with SCI, as seen by an average PWV elevation of 2–3 m/sec and an associated 40 year acceleration of CV decline. The SCI population presents as higher risk, likely because of a combination of autonomic dysfunction, vascular remodelling, and changes in physical activity patterns. The available evidence is limited by small sample sizes and a paucity of age-, gender-, lesion level- and health status-specific analyses. Future work should include more longitudinal studies assessing rapid changes in central arterial stiffness in the acute phase of SCI, as well as combining pharmacological and nonpharmacological interventions for mitigating decline. As upper body exercise generally does not yield changes in central arterial stiffness in SCI and non-SCI populations, other modalities should be explored, such as passive lower limb exercise and/or functional electrical stimulation. Extrapolating from research in non-SCI populations, adjunct lifestyle and diet therapies may also be viable interventions for mitigating central arterial stiffening after SCI. The most promising of these strategies is increased intake of PUFAs, because of the low cost, high adherence, consistent positive outcomes, few side effects, and smaller likelihood of exacerbating the low blood pressure that this population already experiences.
Footnotes
Author Disclosure Statement
No competing financial interests exist.