
Abstract
The mechanisms of late recurrent neurological deterioration after conservative treatment for acute traumatic central cord syndrome (ATCCS) remain unclear. Seventeen operative cases sustaining late recurrent neurological deterioration after conservative treatment for ATCCS were reviewed to investigate the mechanisms. The assessment of neurological status was based on International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). Gender, age, cause of injury, results of image, conservative treatment and operative data, and neurological status at different time points were recorded. The mean age of 17 patients was 43.8 ± 2.3 years old, and the causes of the cervical injury were 14 vehicle accidents and 3 falls. The neurological deficits of 17 patients on admission were not serious, and patients recovered quickly after conservative treatment. No fractures or dislocation were found in any patient's radiographs or CT scan images. All 17 patients performed first MRI test in 4 days and there was a slight or mild compression on the spinal cord in 16 patients. Eight patients had a second MRI scan ∼6 weeks later, which showed that there was aggravated compression on the spinal cord in six patients. All patients underwent an anterior approach to cervical decompression and internal fixation operation. During the operation, there were loose discs found in all 17 patients, obvious ruptures of disks found in 3 patients, obvious ruptures of anterior longitudinal ligaments (ALLs) found in 8 patients, and obvious ruptures of posterior longitudinal ligaments (PLLs) found in 7 patients. There was serious adhesion between PLLs and cervical disks in 12 patients. In five patients, partial ossification of PLLs was detected. All patients had a good neurological outcome at 6 month follow-up. Ruptures of ALLs, PLLs, and discs resulting in cervical instability and secondary compression on the spinal cord were important causes for recurrent neurological deterioration after conservative treatment for ATCCS. With timely spinal decompression after recurrent neurological deterioration, patients could achieve a good neurological outcome.
Introduction
A
Many authors suggested that patients sustaining ATCCS without significant spinal instability or progress in neurological improvement after initial conservative treatment should receive constant nonsurgical treatment. 7 –9 Initial conservative treatment include external immobilization of the spine and the use of small-dose steroids and drugs improving microcirculation, which may be of benefit to some patients, enabling them to recover to a good neurological status. However, during the period of nonsurgical treatment, some patients sustained neurological deterioration after several weeks to months of good neurological function. 8,10 –15 However, the mechanisms of recurrent neurological deterioration after ATCCS were seldom discussed.
In this study, 17 operative cases from Shanghai Ninth People's Hospital sustaining recurrent neurological deterioration after ATCCS without bony injury were reviewed, and all these patients had good neurological function for >2 weeks. By retrospective analysis of the detailed demographic data and operative findings of these cases, this study aimed to investigate the mechanisms of recurrent neurological deterioration and the means of lowering neurological deficits after cervical spine cord injury.
Methods
Patients
All these retrospective case series were recruited at the Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine between January 2011 and May 2016. This orthopedic department with special spine surgeons admitted ∼50 patients for operations for traumatic cervical spine cord injury annually.
Treatment strategies
The treatment strategies for ATCCS without major fracture or dislocation in this hospital were as follows. Patients who presented with slight or mild neurological deficits and no serious spinal cord compression found on MRI images would be routinely given conservative treatment. During the first several days, the initial conservative treatment included cervical immobilization by cervical collar or continued cervical traction (1.5–2.0 kg), and use of small-dose steroids and microcirculation-improving drugs. After conservative treatment, if the neurological deficits disappeared or only small neurological deficits remained, patients would be treated with cervical immobilization by cervical collar for 6–8 weeks as further treatment. Otherwise, patients would be recommended for a cervical operation as soon as possible. Follow-up on neurological status lasted ∼6–8 months, and if the neurological function became worse, patients would be suggested for a timely cervical operation.
Diagnostic tests and evaluating indicators
Assessment of neurological status was based on International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). 16 Radiographs and CT were used to rule out fracture or dislocation. MRI was used to assess spinal cord compression and degree of spinal cord and soft tissue injury. Gender, age, cause of injury, conservative treatment, and operative data were noted from the clinical data of all patients. The date of neurological deterioration and neurological status on admission, first discharge, preoperation, and 6 months postoperation were also recorded in this study.
Statistical analysis
Statistical analysis was performed using SPSS version 14.0, and the results represented as mean ± standard deviation (SD). Intergroup differences were analyzed by analysis of variance. The differences of neurological score of first admission VS first discharge, preoperation, and 6 months postoperation were analyzed by t test. Significance was set at p < 0.01.
Results
From January 2011 to May 2016, 138 patients sustaining ACCTS were given nonoperative treatment after initial conservative treatment at our hospital, and 111 patients had satisfactory neurological function at the last follow-up. However, 19 patients sustained late recurrent neurological deterioration, and among them, 17 patients received a cervical operation at our hospital. Another eight patients were lost to follow-up.
The basic clinical data are summarized in Table 1. Our study included 17 patients whose mean age was 43.8 ± 8.2 years, among whom 12 were male and 5 were female. The time of neurological deterioration was 57.1 ± 21.2 days after first admission, and all operations were performed <5 days after neurological deterioration.
LS, light tough sensory score; PS, pin prick sensory score; M, motor score; first discharge, first discharge after conservative treatment. Injury of posterior longitudinal ligaments (PLLs): normal, 0; suspected rupture, 1; significant rupture, 2. Injury of anterior longitudinal ligaments (ALLs): normal, 0; suspected rupture, 1; significant rupture, 2. Injury of discs: normal, 0; suspected rupture, 1; significant rupture, 2.
The causes of cervical injury were vehicle accidents (14 patients, 82%) and falls (3 patients, 18%). The neurological deficits on admission in all 17 patients were not serious; 15/17 patients presented with neurological deficits only in the upper limbs and the neurological recovery of all patients indicated a sensitive reaction to drug treatment and cervical traction. Neurological status on admission included: mean light tough sensory score of 101.65 ± 4.30, mean pin prick sensory score of 104.29 ± 3.72, and mean motor score of 88.5 ± 4.5. The neurological status on first discharge, after ∼3–7 days of conservative treatment included mean light tough sensory score of 108.65 ± 1.90, mean pin prick sensory score of 110.35 ± 1.17 and mean motor score of 96.8 ± 1.6.
All 17 patients received radiographic and CT scans after cervical trauma. In radiographs, there were thicker prevertebral fascia found in 8 patients and an abnormal cervical curve found in 13 patients. In CT scans with two-dimensional (2-D) reconstruction images, there was no evidence of vertebral fractures found in any of the 17 patients, and thicker prevertebral fascia was found in all 17 patients.
All 17 patients received their first MRI test within 4 days after cervical trauma. There were diffuse hyperintense signals in the prevertebral fascia on T2 weighted images (T2WI) in all 17 cases, which indicated injuries of anterior longitudinal ligaments (ALLs). There was cervical disc herniation combined with mild compression of the spinal cord in 11 patients and abnormal signal in the spinal cord in 1 patient. There was cervical disk herniation combined with slight compression on the spinal cord in five patients. There was cervical disk injury without obvious herniation in one case (the only hyperintense disc at T2WI). Approximately 6 weeks later, eight patients received a second MRI test, and there was obviously aggravated compression on the spinal cord seen in six patients. One patient showed additional abnormal signals in spinal cord. The typical alterations between the first and second MRI are seen in Figure 1.
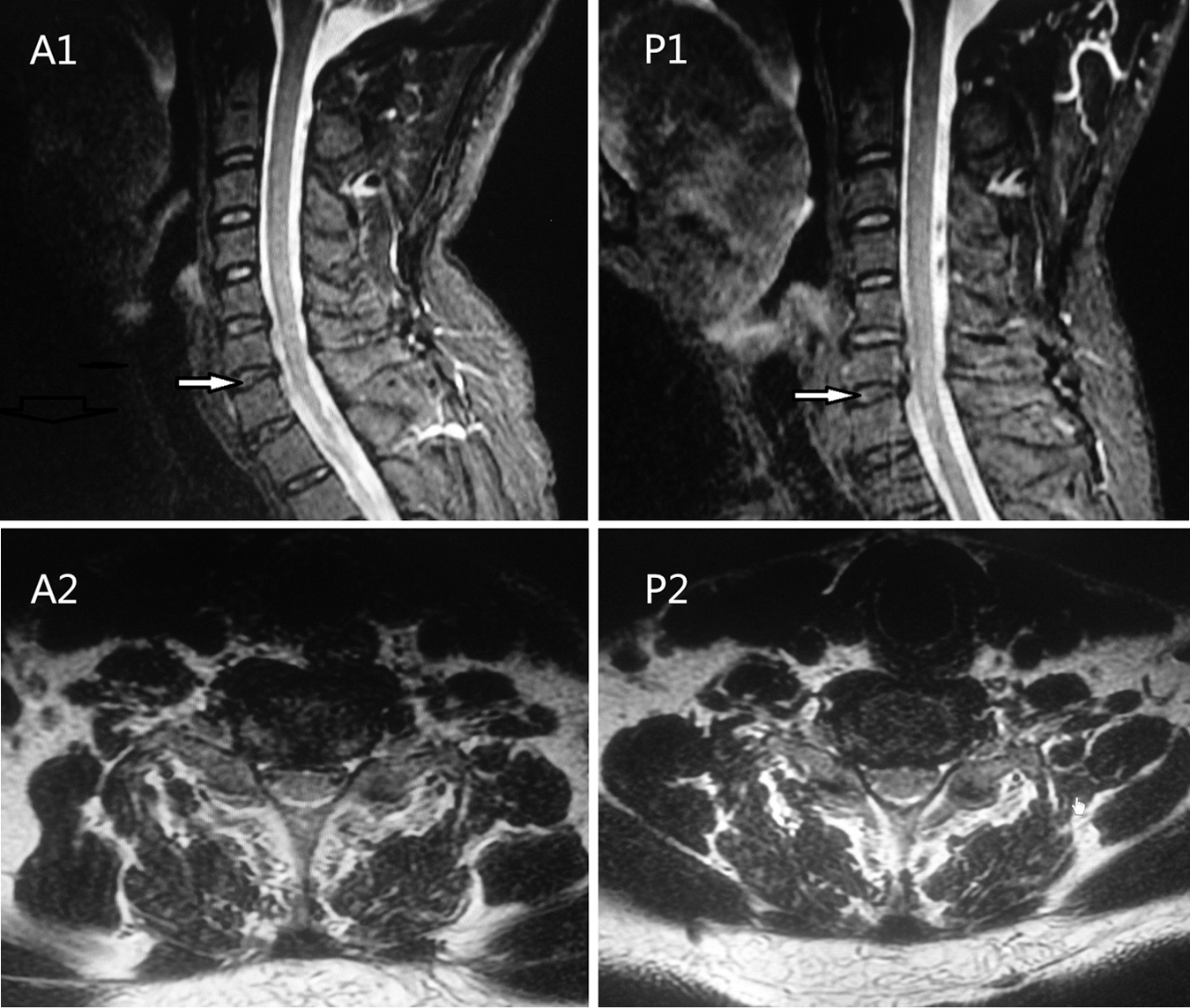
The alterations of spinal cord compression on MRI images. MRI images from a 54-year-old man.
All patients underwent an anterior approach to cervical decompression and internal fixation operation, including corpectomy and discectomy combined with intervertebral fusion by plate-screw internal fixation. Seven patients underwent one segment decompression and fusion, eight patients underwent two segment decompression and fusion, and another two patients underwent three segment decompression and fusion.
During operation, there was at least one segment of disc loosened in all 17 patients, which was confirmed by operating surgeons. There was obvious rupture of loosened discs in 3 patients, and suspected rupture of loosened discs in 11 patients. There were obvious ruptures of ALLs in eight patients, and suspected ruptures of ALLs in nine patients. There was obvious rupture of posterior longitudinal ligaments (PLLs) in seven patients, and suspected ruptures of PLLs in seven patients (detailed injuries of ligaments and discs seen in Table 1). There were thicker prevertebral fascia in all patients, and serious adhesion between PLLs and cervical disks in 12 patients. Partial ossification of PLLs was detected in five patients. Typical hematoxylin and eosin (HE) stain images of adhesive specimens between discs and PLLs are seen in Figure 2.
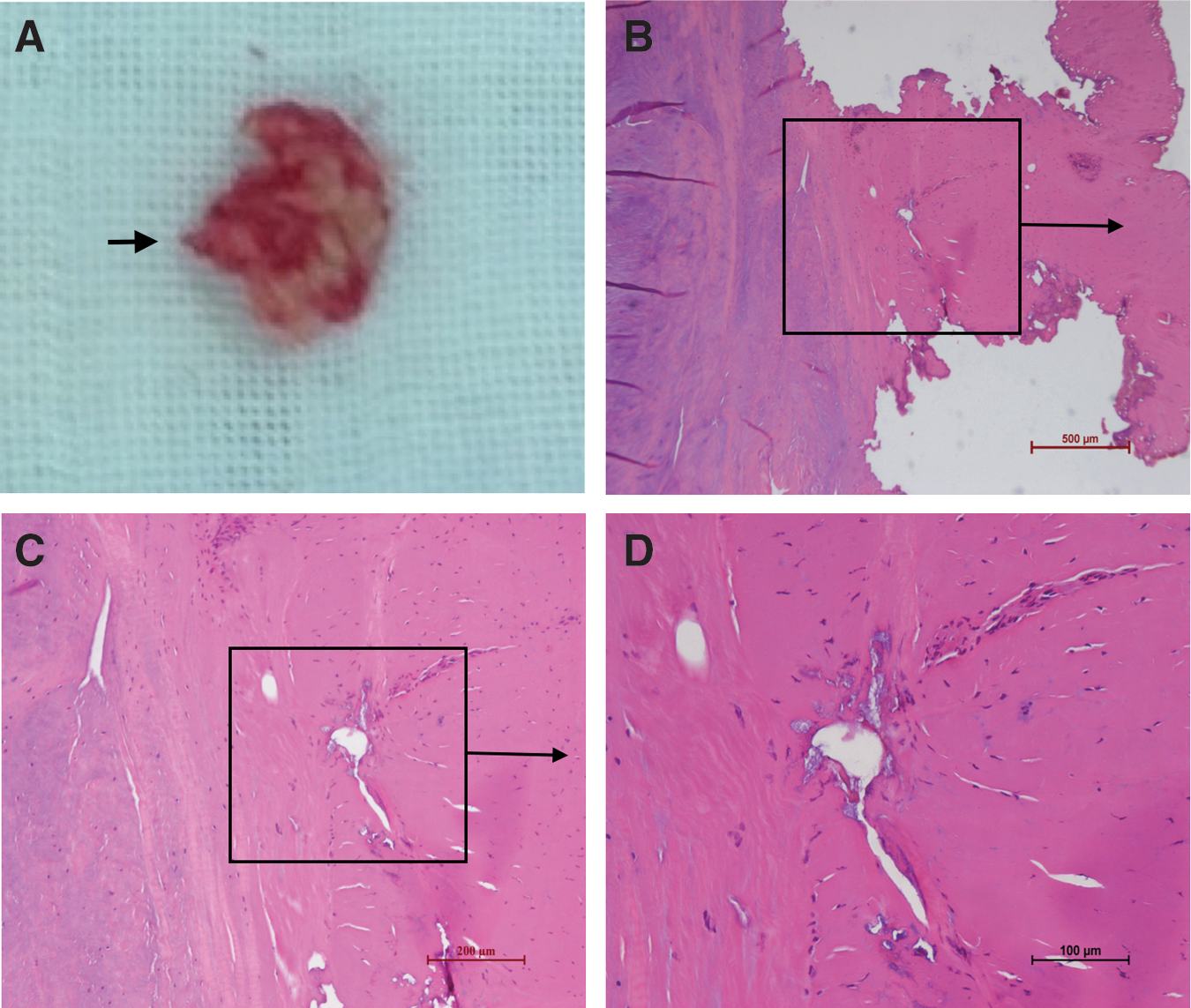
Typical intraoperative specimen and corresponding hematoxylin and eosin (HE) stain images of adhesion and ossification of posterior longitudinal ligaments (PLLs). The specimen and HE stain images are from a 46-year-old female.
The preoperational and 6 month postoperative ISNCSCI scores are also listed in Table 1 and statistical data are listed in Table 2. The mean preoperational light tough sensory score was 105.59 ± 2.96, the mean pin prick sensory score was 107.65 ± 2.34, and the the mean motor score was 88.4 ± 2.7. Six month postoperative ISNCSCI score recovered significantly, with a mean light tough sensory score of 109.71 ± 1.26, a mean pin prick sensory score of 111.24 ± 0.90, and a mean motor score of 97.4 ± 1.7.
First discharge, first discharge after conservative treatment. Values are presented as mean ± standard deviation
p < 0.01 vs. admission
p > 0.05 vs. admission.
Discussion
Conservative treatment played an important role in traumatic cervical spine cord injury in the early stage, and also could be the ultimate therapy. 17 In this study, all 17 cases with ATCCS presented a more sensitive reaction to initial conservative treatment and recovered to nearly normal neurological status quickly. Some authors found there was a high rate of achieving good neurological outcome when patients with ATCCS were treated with conservatively. 5,7,8,18 –20 Age and severity of initial injury were considered as two important factors affecting neurological recovery. 21 –23 Therefore, the relative young age (mean 43.8 years) and slight initial neurological deficits in this study might explain the effective outcome of conservative treatment. In our previous clinical practice, older patients sustaining ATCCS with serious neurological deficits were seldom found to recover quickly after early conservative treatment.
Recurrent neurological deterioration had also been reported in other studies after a period of ATCCS; 24 –28 however, the mechanisms of neurological deterioration were rarely discussed according to operative results. From our operative findings, we thought that cervical instability was responsible for neurological deterioration. There was obvious loosening at the intervertebral disc space with spinal compression in all 17 patients, which was an important proof of spinal instability. There was a general agreement that the intervertebral discs and ligaments around the vertebrae were the important structures affecting the stability of cervical vertebrae. 29 –31 Higher ratio of ruptures of ALLs, PLLs, and discs found during operation were also important evidence for spinal instability.
According to MRI images and operative findings, we considered that cervical instability after trauma could result in secondary spinal compression. Among eight patients who had a second MRI test, there was obvious aggravated compression on the spinal cord found in the second MRI in six cases. Serious adhesion between PLLs and cervical discs in 12 cases, and partial ossification of PLLs in 5 cases indicated existence of inflammatory reaction around the spine. Except for herniated disks, the chief oppressive matter found during operations was thickened PLLs, hyperplastic granulation, or moderate ossification of PLLs.
According to results described, we believed that recurrent neurological deterioration of ATCCS after cervical trauma could be related with two factors. First, sustained cervical instability increasingly led to disc degeneration and disc herniation, which resulted in spinal compression. 32 Second, secondary inflammation and ossification of PLLs caused by cervical instability aggravated the extent of spinal compression, which was consistent with points made by Chen and coworkers. 33 Another opinion about late neurological deterioration (> 7 days) was that it is caused by vertebral artery injuries, as reported by Harrop and coworkers, 34 but this was not verified in this study.
Injury of ligaments had an important effect on cervical stability after trauma. Dynamic radiography was most common method for assessing the stability of cervical structure and the union of cervical ligaments after cervical trauma. 31,35,36 However, the efficacy of dynamic radiography is limited, because the high rate of inadequate stability of the entire cervical spine and premature movement of cervical vertebra may influence the union of ligaments. 37 The interval time for recurrent neurological deterioration was too short (∼ 2 months) for ligament repair in this study; we did not perform dynamic radiographic tests on all patients.
MRI was another important method for identifying spinal instability. It can help show prevertebral edema, and injuries of discs and ligaments that maintain the stability of cervical vertebra. 38 Maeda and coworkers reported that after CSCI without any major bone injury or dislocation, 85% of the patients had varying degrees of prevertebral hyperintensity, and approximately half of them were shown to have ALLs and/or disc injuries on MRI, both of which were significantly associated with cervical segmental instability. 31 However, MRI may overestimate the extent of disruptive injury of ligamentous structures when compared with intraoperative findings. 39 Therefore, cervical MRI is an important preferred adjunctive physical examination for ATCCS or CSCI; however, it cannot provide the definite diagnosis. It is necessary to combine clinical symptoms and imaging findings to make a diagnosis. In this study, MRI was not chosen to indicate ruptures of ALLs and PLLs. Assessing cervical stability and predicting the union of cervical structure are not easy.
Szwedowski and coworkers believed that cervical external immobilization up to 12 weeks was a necessary therapeutic method for patients after traumatic CSCI. 25 In our hospital, patients were commonly given neck immobilization with continuous use of a rigid cervical collar over 6 weeks; however, all 17 patients did not strictly obey this suggestion because they had less pain in the neck or the cervical collar hindered their work. We believed that irregular cervical collar use was one factor affecting the union of important ligaments in this study, which was responsible for spinal instability.
Most researchers believed that earlier surgical decompression would provide a better chance to reverse neurological function. 26,27 However, there were also some authors who reported that late cervical decompression operations on incomplete CSCI also obtained a good prognosis. 3,8,9,40 We performed late operations for spinal decompression after trauma; however, timely operations after recurrent neurological deterioration could also obtain a good neurological outcome.
There were still some limitations to this study. First, there were no comparison data for patients who maintained good neurological function after conservative treatment, which would have helped us investigate more about the mechanisms of neurologic deterioration. Second, because the time for neurological recovery often lasts >2 years, the 6 month follow-up time was not long enough. Third, because we did not find standardized descriptions of ruptures of ALLs, PLLs, and discs, the degree of rupture was determined only according to the assessment of operating surgeons, which was not objective.
Conclusion
Young patients with ATCCS with slight initial neurological deficits often recover well. Ruptures of ALLs, PLLs, and discs resulting in cervical instability and secondary compression on the spinal cord were the main causes of recurrent neurological deterioration after conservative treatment for ATCCS. Recurrent neurological deterioration was difficult to predict early. With timely spinal decompression after recurrent neurological deterioration, patients could achieve a good neurological outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.