
Abstract
Over the past 10 years, our team has attended numerous Paralympic games and International Paralympic Committee (IPC)–sanctioned events where we have accumulated the largest data set to date from elite athletes with spinal cord injury (SCI). This empirical evidence has allowed us to address critical questions related to health and athletic performance in these incredibly medically complex individuals. Namely, does autonomic function influence performance? Can we account for this with the present sport classification? How can we prevent the doping practice of self-inducing life-threatening episodes of hypertension to improve performance (termed “boosting”)? How does extremely high participation in routine upper-body wheelchair exercise impact cardiovascular and cerebrovascular disease risk? Is it possible to improve the sport classification to level the playing field between athletes with and without autonomic dysfunction? Herein, we will narratively address these questions, and provide our perspective on future directions and recommendations moving forward. Our extensive clinical experience and comprehensive dataset suggest preserved autonomic function is critical for elite performance. We will explore how an easy-to-execute test may be able to predict which individuals are most likely to develop autonomic dysfunctions that may negatively affect their health and performance. We also will evaluate the possibility that a level playing field may be even more difficult to establish than once thought, considering the importance of not only voluntary movement to performance, but also autonomic function. Finally, we also will discuss new changes in screening guidelines at Rio to assess the occurrence of boosting, which is a banned practice by the IPC.
Introduction
I
Pathophysiological Considerations
Autonomic dysfunction is remarkably common in athletes and non-athletes with spinal cord injury (SCI). 1 –3 Due to the integrated anatomical nature of the autonomic nervous system, individuals with central nervous system injury demonstrate a wide range of bodily dysfunctions, including cardiovascular abnormalities, bowel and bladder complications, and sexual dysfunctions, 4 and are at risk for life-threatening complications. 5,6 The dramatic negative impact on individuals, their family, and healthcare expenses, 7 as well as quality and quantity of life of individuals with SCI, has led to our long-term goal of improving autonomic function in athletes and non-athletes with SCI. In terms of athletics, it has been our goal to understand specifically how abnormalities in heart rate (HR) and blood pressure (BP) control impact not only health, but also athletic performance and exercise capacity after SCI. 1,3,8 –13
After severe cervical SCI, medullary cardiovascular centers are disconnected from pre-ganglionic sympathetic neurons within the spinal cord that are responsible for adrenergic input to blood vessels, as well as both to the sino-atrial node (i.e., to increase heart rate) and the myocardium itself (i.e., to increase the force of contraction). 14 –16 Through our work with athletes with SCI at IPC-sanctioned events, we have shown that if there is a complete disruption of descending sympathetic control due to the SCI, individuals will be unable to increase their HR above what can be achieved with vagal withdrawal nor appropriately raise their BP during exercise. As such, HRs beyond 130 beats per minute are often unachievable and thus may not provide a sufficient stimulus during high-intensity exercise in those with SCI. As both BP and HR are regulated by the same spinal descending pathways, 14 in-competition HR measurement provides crucial insight into the capacity of the sympathetic nervous system to activate cardiovascular end-organs in athletes with SCI and has aided us in our recommendations for the refinement of sport classification tools.
Our most recent data suggest that individuals with similar sport classifications competing in the same sport exhibit remarkably different responses in BP to orthostatic challenge, as well as maximum HR, during competition (Fig. 1). Upon close examination of the data, it is abundantly clear that individuals with high-thoracic or cervical SCI competing in Wheelchair Rugby have a lower resting arterial BP and are not able to increase HR to the same degree as those without SCI (e.g., amputees). Therefore, despite similar sport classifications, individuals with SCI are at a clear disadvantage in terms of cardiovascular capacity during competition. Thus, the logical next step is to develop the optimal autonomic assessment that can best predict cardiovascular capacity during competition in order to better even the playing field. We now have imminent data suggesting that a simple accessible orthostatic challenge is able to predict approximately 50% of the variability of maximum HR during competition. Therefore, we will provide a clear recommendation that this examination be included and considered when assigning individuals to their classification in their respective Paralympic sport.
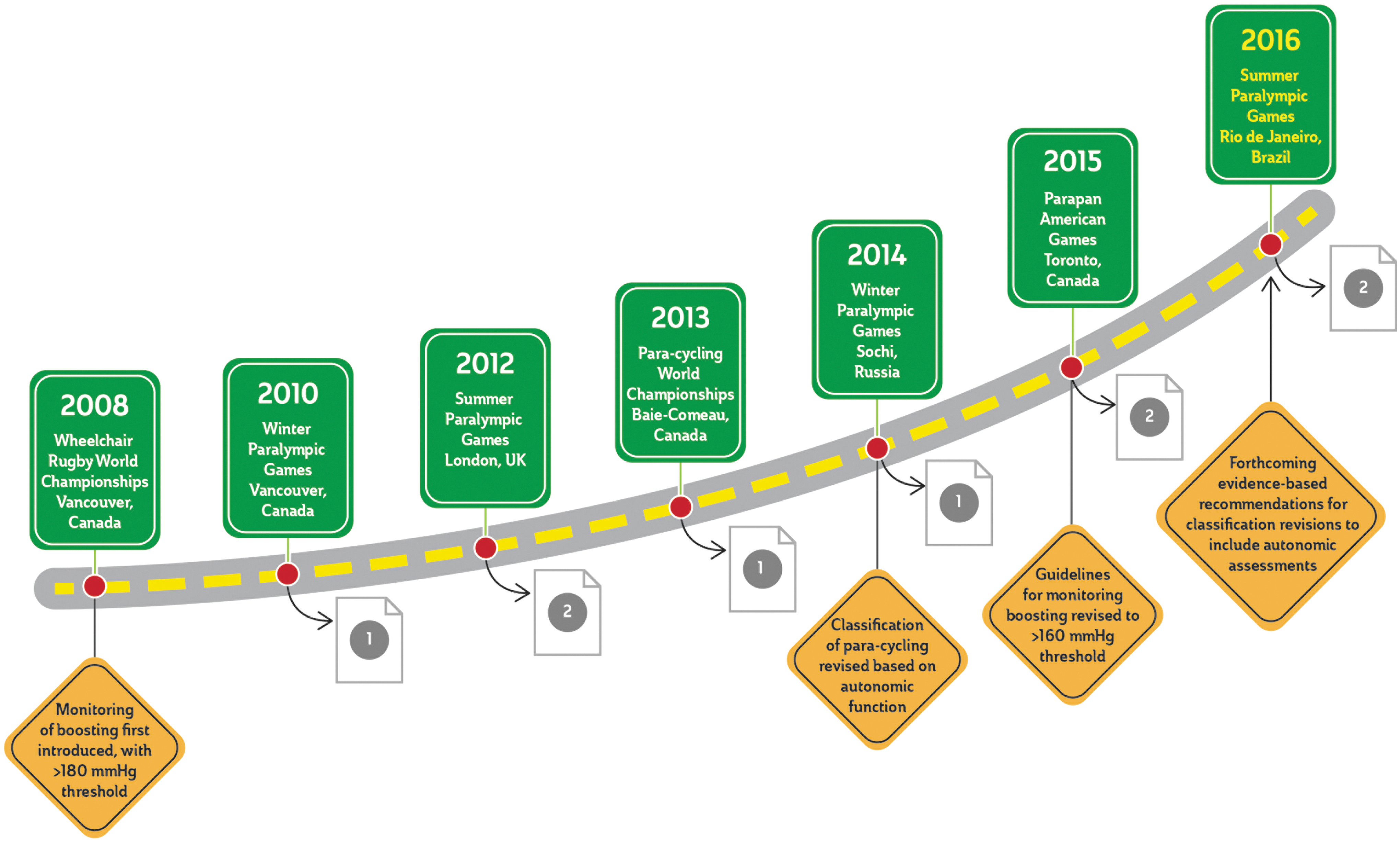
The Road to Rio. A schematic representation of the major International Paralympic Committee-sanctioned events during which our team has examined athletes (top), as well as a brief description of the significant changes in the management and classification of Paralympic athletes (bottom), which have resulted from this work. Curved arrows represent the publication of our work throughout this process; specific references are as follows. Mills and Krassioukov, (2011)
8
; Phillips and colleagues (2012)
35
; Krassioukov (2012)
13
; West and colleagues,(2013)
11
; West and colleagues (2014)
2
; Krassioukov and colleagues (2015)
12
; Gee and colleagues (2015)
10
; West and Krassioukov (2016)
9
; Currie and colleagues (2016).
3
Color image is available online at
Evolution of Sport Classification
Only recently has the evaluation of autonomic functions following SCI become a crucial part of the clinical assessment of all individuals living with SCI. 17 Further, autonomic function is becoming increasingly recognized as an important factor in various Paralympic sports where cardiovascular dysfunction may be a limiting factor. 1,2,18 In fact, the ability of individuals to mount an appropriate cardiovascular response during competition is critical to performance at such an elite level. 1,10,18,19 However, not a single Paralympic sport classification includes any aspect of autonomic function in its criteria, despite long-standing evidence that the autonomic nervous system's capacity to mount an appropriate cardiovascular response to exercise is a critical factor in aerobic and sport performance. 2,19,20 Moreover, a lack of information about these individuals' cardiovascular capacity may leave some individuals at a distinct disadvantage due to high levels of motor function but little to no ability to elicit a cardiovascular response to the increasing physiological demands. While it is intuitive that completeness of injury in terms of motor function (i.e. American Spinal Injury Association Impairment Scale) 21 has implications for functional sport skill (and thus classification), there is now strong evidence that motor and autonomic function are often differentially preserved in this population 22 and therefore require independent consideration.
In contrast to motor completeness, autonomic completeness refers to the amount of supraspinal descending sympathetic control that is preserved after SCI. 23 In terms of exercise performance, the sympathetic nervous system plays a critical role in increasing BP as well as increasing HR. Moreover, increased sympathetic capacity is now appreciated to provide a performance advantage after SCI. 10,18,22 Ultimately, it is not surprising, then, that current evidence indicates a general discontent with present sport classification schemes, with many individuals feeling both the classification as well as the restrictions for functional impairment could be improved. 24 However, this is currently not being assessed during sport classification, largely due to the lack of a standardized evidence-based strategy to assess autonomic function.
Some of the hesitance to incorporate an autonomic score in the classification of athletes has stemmed from uncertainty regarding which tool best evaluates autonomic function. Although a number of clinical tests are available, including an orthostatic challenge test, sympathetic skin responses, and the cold-pressor test, there is hesitation even among clinicians in terms of how best to implement these tests, how to prepare subjects for the tests, and how to interpret the results. Our team has used all of these tests for a number of years clinically and in our research studies. 2,18,22,25 These tests not only reflect specific autonomic function but are also used to diagnose the severity of disruption within the descending sympatho-excitatory projections. 26,27
Recently, we have compared the utility of each of these tests to best predict cardiovascular capacity during athlete's performance in IPC athletes. Our large data set shows that the orthostatic challenge test (validated sit-up test), which is easy to administer and interpret, can reliably predict exercise cardiovascular capacity in those with autonomic dysfunction (Fig. 2). 28 As such, it is our recommendation to include this assessment into classification in order to ensure a level playing field between athletes with and without autonomic dysfunction. We believe that an added benefit of incorporating the assessment of autonomic function into classification may be that it will eliminate the need for boosting, as reduced cardiovascular capacity during exercise would already be accounted for in the scoring and therefore would potentially obviate the need to dangerously augment blood pressure in an attempt to mitigate the advance of athletes without autonomic dysfunction.

Geographical representation of the major knowledge translation that has occurred over the past 10 years of our team's involvement in International Paralympic Committee (IPC)–sanctioned events. Black stars represent IPC events and orange dots represent international conferences where we have delivered presentations critical for raising awareness regarding autonomic issues in Paralympic athletes. Color image is available online at
Promotion and Benefits of Physical Activity
Our participation in IPC-sanctioned events has provided deep insight into the role that regular training can play in cardiovascular and cerebrovascular health. Physical inactivity is one of the most powerful modifiable risk factors capable of improving both psychological and physical health, and certainly the IPC plays a major role in the promotion of healthy physical activity in those living with disabilities such as SCI who are at 3- to 4-fold increased risk of cardiovascular and cerebrovascular disease. 28,29 Unfortunately, those living with SCI have additional health issues other than the lack of mobility and capacity for exercise participation, such as autonomic dysfunctions, that contribute to this vascular decline. Further, we have shown in numerous studies that athletes who routinely participate in upper-body cardiovascular exercise (i.e., wheeling) have the similar cardiac and cerebrovascular decline seen in inactive individuals, 3,30 despite our pre-clinical data showing that passive lower-limb exercise can alleviate this risk. 31,32 Considering this, and largely due to the data we have been fortunate to collect through IPC events (Fig. 2), we are now becoming aware of the need to mobilize the large muscles of the lower-limbs in order to elicit the powerful positive cardiovascular effects of exercise.
Doping
Identifying individuals with autonomic dysfunction is a critical step in promoting both optimal exercise and competition performance, as well as ensuring athlete health. We know that low BP is a limiting factor for performance in those with SCI, 19 which has led to the practice of boosting, where individuals knowingly elicit autonomic dysreflexia in order to increase their blood pressure, which is considered a banned practice (i.e., doping) by the IPC. 10,33,34 Previously, this practice was defined as having a BP of more than 180 mm Hg 33 ; however, recently this has been revised to a threshold of 160 mm Hg in order to more conservatively protect these athletes.
Previous evidence indicates that up to 20% of Paralympic athletes with SCI boost during competition and 75% of surveyed individuals believe that 100% of those with cervical SCI boost. 34 Based on our data collected over the past decade, we estimate that approximately 50% of the individuals participating in IPC events demonstrate impaired autonomic control, suggesting they may attempt to boost during competition in order to increase their BP. Thus, we strongly recommend the incorporation of out-of-competition autonomic assessments (i.e., sit-up test and biological BP passport) for classification and doping prevention. We have strong evidence that in Wheelchair Rugby, the addition of these assessments into sport classification could help to balance teams in terms of cardiovascular capacity, and logically prevent the need for boosting.
It is reasonable to suggest that autonomic assessments, which can be reliably performed in a timely manner, be incorporated into standardized sport classification, as it may help balance the field in terms in cardiovascular limitations and mitigate the benefit gained from inducing potentially life-threatening episodes of autonomic dysreflexia. Considering the labile and unpredictable BP in many individuals with autonomic conditions, moving forward it is our recommendation to incorporate a biological passport into athlete screening, where BPs are collected over several days to allow assessors to better identify which pre-competition values fall within each individual athlete's normal range.
Conclusion
Our team's participation in IPC events over the past decade has truly been an honor and privilege. Through our work, we feel we have been able to contribute to the Paralympic Movement, vision, and mission, which encompasses “contribution to a better world for all people with a disability.” During this time, we have had the opportunity to better understand the specific pathophysiology of autonomic dysfunctions in athletes and non-athletes living with SCI and improve their care. Further, in collaboration with the IPC and sport governing bodies, we may refine sport classification to ensure a level playing field between SCI and non-SCI athletes, promote engagement in physical activity among those with disability, assess factors involved in the elevated risk of cardiovascular disease in this population, and raise awareness about boosting as a life-threatening practice that should be avoided. It is our goal to continue to contribute to the Paralympic Movement through further refining of classification, and incorporating a “Biological Passport” into athlete screening.
Footnotes
Acknowledgments
A.A. Phillips is supported by postdoctoral fellowships from the Craig H. Neilsen Foundation, the Heart and Stroke Foundation of Canada—Focus on Stroke, as well as the Michael Smith Foundation for Health Research. J.W. Squair is supported by a Frederick Banting and Charles Best Canada Graduate Scholarship and a Vancouver Coastal Health-University of British Columbia MD/PhD Studentship from the Canadian Institutes of Health Research, as well as a Killam Doctoral Scholarship and a four-year fellowship from the University of British Columbia. We acknowledge Cheryl Niamath for their artistic expertise. This work was supported by funding to the lab of A.V.K. from the Canadian Foundation for Innovation, BC Knowledge Translation Foundation, the Canadian Institute for Health Research, the Craig H. Neilsen Foundation, and the Martin Shkreli Foundation.
Author Disclosure Statement
No competing financial interests exist.