
Abstract
Cogniphobia refers to avoidance of mental exertion out of a fear of developing or exacerbating a headache. Headaches are very common after mild traumatic brain injury (mTBI) and often become chronic. Cogniphobia is hypothesized to contribute to poor cognitive test performance and persistent disability in some patients with mTBI. Eighty patients with mTBI and post-traumatic headaches were recruited from specialty outpatient clinics. They completed a battery of questionnaires (including a cogniphobia scale) and neuropsychological tests (the National Institutes of Health Toolbox Cognition Battery and the Medical Symptom Validity Test) at 2–3 months post injury, in a cross-sectional design. Participants with more severe headaches reported higher levels of cogniphobia. Cogniphobia was associated with lower performance on memory testing (but not other cognitive tests), independent of headache severity. Participants who avoided mental exertion also tended to avoid physical activity and traumatic stress triggers. The findings provide preliminary support for the role of cogniphobia in persistent cognitive difficulties after mTBI, and suggest that cogniphobia may reflect a broader avoidant coping style.
Introduction
F
Headache is among the most common symptoms after mild traumatic brain injury (mTBI). 10,11 One in three patients continue to experience headaches 12 months after an mTBI. 10 Cogniphobia may help explain why some patients with persistent headaches perform poorly on neuropsychological testing and in daily life long after an mTBI; 8,12 however, empirical evidence for this link is lacking. The present study investigates cogniphobia in a treatment-seeking mTBI sample. We hypothesized that cogniphobia will be associated with 1) greater headache severity, 2) lower cognitive performance, and 3) greater behavioral avoidance of other kinds. Evidence supporting these hypotheses would add further detail to an evolving biopsychosocial conceptualization of mTBI outcome and potentially help inform the design of novel interventions.
Methods
Participants were recruited from consecutive referrals to four outpatient concussion clinics in the greater Vancouver area from March 2015 to August 2016. The eligibility criteria were: 1) being 18–65 year of age, 2) having sustained an mTBI by the World Health Organization Neurotrauma Task Force operational definition 13 within the past 6 months, 3) being fluent in English, 4) having been employed prior to injury, because the current study was embedded in a larger research program investigating return to work following mTBI, and 5) reporting having experienced at least one headache during the week prior to assessment. The present study received approval from the University of British Columbia Behavioural Research Ethics Board, the Vancouver Coastal Health Research Institute, and the Fraser Health Research Institute. Participants completed a battery of tests in a single session at the time of their first clinic visit that included the following measures.
Cogniphobia Scale
The Cogniphobia Scale 9 was originally developed by Todd and coworkers 14 for post-traumatic headaches by adapting the widely used Tampa Scale for Kinesophobia, 15 a general measure of pain-related fear of movement. Suhr and Spickard 9 revised the cogniphobia scale (raising the item total to 19) and performed a factor analysis in a chronic headache sample, deriving two subscales that measure avoidance of mental exertion (Cogniphobia-Avoidance) and beliefs that mental effort is dangerous (Cogniphobia-Dangerousness). The internal consistency (Cronbach's α) of these subscales in the present sample was 0.79 and 0.80, respectively. Higher scores indicate stronger endorsement of avoidance behavior and dangerousness beliefs.
British Columbia Postconcussion Symptom Inventory (BC-PSI)
The BC-PSI 16 prompts respondents to rate the frequency and intensity with which they have experienced a range of physical, cognitive, and emotional symptoms over the previous week, including headaches. It is widely used in mTBI research. 17 –19 The headache item from this scale was used as a measure of headache intensity over the past week.
Brief pain questionnaire
Participants rated their current pain intensity (0/“none” to 3/“severe” pain “at this moment”) in multiple bodily regions, the head/skull, neck, chest/abdomen/back, arms/shoulders, and pelvis/legs. This measure has been shown to correlate with functional outcome from mTBI. 20 The head/skull item from this scale was used as measure of headache intensity at the time of the assessment.
National Institutes of Health Toolbox Cognition Battery (NIHTB-CB)
The NIHTB-CB 21 is a brief neuropsychological test battery that was developed to by National Institutes of Health Blueprint for Neuroscience Research platform to serve as a cognition outcome measure across neurological conditions. It consists of two tests measuring crystallized cognitive ability (Picture Vocabulary and Oral Reading Recognition) and five tests of fluid cognitive abilities including processing speed, attention, episodic memory, and executive functioning (Flanker Inhibitory Control and Attention, Dimensional Change Card Sort, Picture Sequence Memory, Pattern Comparison Processing Speed, and List Sorting Working Memory). 21 Initial validation studies suggest that these tests have strong convergent validity with legacy neuropsychological instruments, strong test–retest reliability, and minimal ceiling or floor effects. 22 Age-adjusted standard scores based on the revised norming system described by Casaletto and coworkers 23 were used in the present analyses.
Medical Symptom Validity Test (MSVT)
The MSVT 24 is a purpose-built “effort,” or performance validity test that is sensitive to motivational factors, but insensitive to the effects of TBI or genuine memory impairment. 25 –27 The “easy” subtests (Immediate Recognition, Delayed Recognition, and Consistency) have evidenced-based cutoffs for identifying cases with probable below-capacity performance. Higher scores on the MSVT indicate better performance; 100 is the maximum possible score.
Secondary measures
The assessment battery also included measures of avoidance of physical activities (Fear Avoidance Beliefs Questionnaire-Physical Activity) 28 avoidance of traumatic stress (items 6 and 7 from the PTSD Checklist-5), 29 and self-imposed general activity restrictions following injury (Behavioral Response to Illness Questionnaire-Limiting scale). 30
Analyses
The primary hypothesis that avoidance of mental exertion (Cogniphobia-Avoidance) would be associated with lower cognitive effort (MSVT “easy” subtests) and cognitive performance (five fluid cognition subtests of the NIHTB-CB) was tested with Pearson correlations, using complete case analysis (actual sample size of 57–60 depending on which combinations of variables were used) with a Bonferroni-corrected α level of 0.01. All variables were continuous. Supplementary analyses involved linear regression and relative risk. The relative risk ratio is the probability of impaired cognitive test performance in individuals with high avoidance of mental exertion divided by the probability of impaired cognitive test performance in individuals with low avoidance of mental exertion.
Results
Of 200 consecutively screened referrals, 80 met the eligibility criteria and consented. Figure 1 displays reasons for non-enrollment in a flow diagram. The demographic and clinical characteristics of the final sample are shown in Table 1.
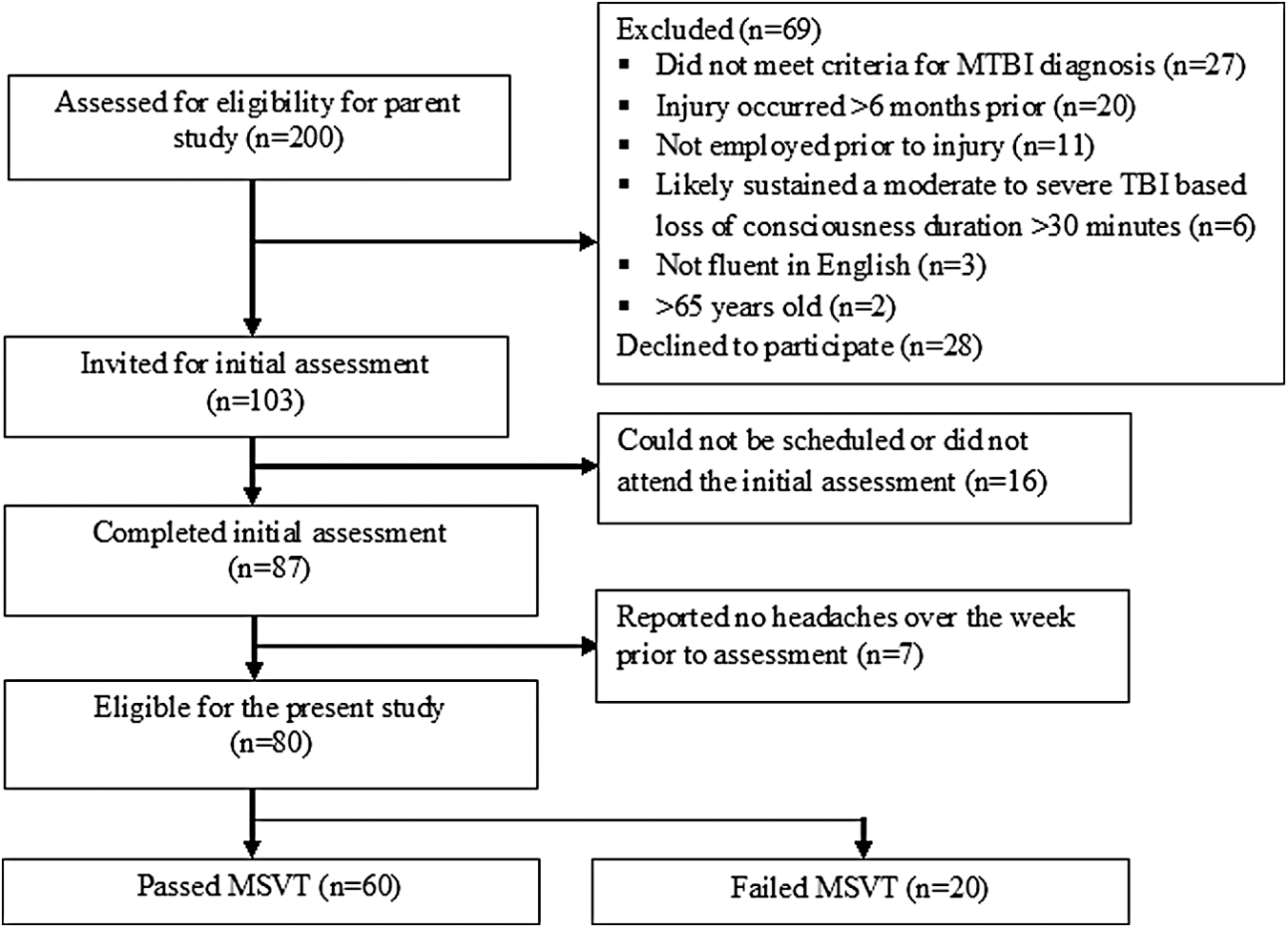
Flow diagram. MSVT, Medical Symptom Validity Test.
^Sample stratified based on Cogniphobia-Avoidance raw scores ≤ 36 or >36.
p value for independent samples t test (for continuous variables) or χ2 test (for proportions).
MSVT. Medical Symptom Validity Test; NIHTB-CB, National Institutes of Health Toolbox Cognition Battery.
Cogniphobia-Avoidance and Cogniphobia-Dangerousness were correlated (r[60] = 0.649, p < 0.001). Neither Cogniphobia-Avoidance or Cogniphobia-Dangerousness were associated with age (r[58] = 0.004, p = 974; r[58] = −0.116, p = 0.386) or time since injury (r[60] = −0.081, p = 0.538; r[60] = −0.119, p = 0.366). Men and women reported similar levels of Cogniphobia-Avoidance (mean = 33.48, SD = 4.83 vs. mean = 35.27, SD = 5.39) and Cogniphobia-Dangerousness (mean = 18.00, SD = 3.22 vs. mean = 18.12, SD = 3.89).
The main analyses are presented in Table 2. Cogniphobia-Avoidance, and to a lesser extent, Cogniphobia-Dangerousness, correlated significantly with headache severity and other measures of avoidance (of physical movement and traumatic stress). Despite a severely restricted range on the MSVT (i.e., 61.7%, 60%, and 51.7% of sample achieved the ceiling score on the Immediate Recognition, Delayed Recognition, and Consistency subtests, respectively), there were significant correlations between Cogniphobia-Avoidance and the MSVT subtests. Cogniphobia-Avoidance correlated with only one NIHTB-CB fluid cognition test at p < 0.01, the Picture Sequence Memory test.
p < 0.05; ** p < 0.01; *** p < 0.001.
^Correlations were not computed because of a profoundly restricted range on the MSVT variables, with 62.3–78.7% achieving the ceiling score.
BC-PSI, British Columbia Postconcussion Symptom Inventory; FABQ, Fear Avoidance Beliefs Questionnaire; PCL, PTSD Checklist; BRIQ. Behavioral Response to Illness Questionnaire; MSVT, Medical Symptom Validity Test; NIHTB-CB, National Institutes of Health Toolbox Cognition Battery.
Low scores on the MSVT may reflect avoidance of mental effort caused by headache fear and/or unmeasured confounds, such as intentional below-capacity performance for secondary gain (malingering). To investigate whether the relationship between Cogniphobia-Avoidance and the NIHTB-CB fluid cognition tests held in participants without performance validity concerns, we reran the correlations after excluding participants who failed the MSVT (performed below established cutoffs for credible performance; n = 20). These results are also reported in Table 2. The correlation between Cogniphobia-Avoidance and Picture Sequence Memory was very modestly attenuated.
To better appreciate the clinical significance of the Picture Sequence Memory finding, we dichotomized the outcome as impaired (Picture Sequence Memory Test age-adjusted standard score <85) versus not, and calculated the risk associated with scoring above the cutoff on the Cogniphobia-Avoidance (raw score >36) that optimally discriminated impaired versus normal Picture Sequence Memory Test performance in this sample. In the full sample, the risk ratio for low memory test performance associated with high avoidance of mental exertion was 3.71 (95% confidence interval = 1.76–7.80). In the sample who passed the MSVT, the risk ratio was 3.39 (95% confidence interval = 1.16–9.91).
Migraine headaches are classically worsened by activity 31,32 and can cause reversible cognitive dysfunction. 33 To explore the possibility that the link among cogniphobia, headache pain, and reduced cognitive performance was restricted to migraine-type headache, we performed a supplementary analysis limited to only selected participants (n = 32) who probably did not have migraine-type headaches based on their reporting no more than mild nausea and sensitivity to noise on the BC-PSI (both item scores = 0–2; note that photobobia is not measured by the BC-PSI). As in the primary analyses, Cogniphobia-Avoidance correlated with MSVT Delayed Recognition (r[32] = −0.529, p = 0.002), MSVT Consistency (r[32] = −0.461, p = 0.007), and Picture Sequence Memory Test (r[32] = −0.540, p = 0.001] in the subgroup without migraine features. The correlation with Dimensional Change Card Sort was r(32) = −0.283, p = 0.117. Cogniphobia-Dangerousness did not significantly correlate with any NIHTB-CB fluid cognition test (p > 0.05). After removing participants who failed the MSVT from this subgroup, the correlation with the Picture Sequence Memory Test held (r[28] = −0.386, p = 0.042) and a correlation between Cogniphobia-Avoidance and the Dimensional Change Card Sort test emerged (r[24] = −0.386, p = 0.042).
Further supplementary analyses aimed to determine if the relationship between avoidance of mental exertion and performance on the Picture Sequence Memory Test would remain after adjusting for headache severity. In linear regression modeling with the sample who passed the MSVT, Cogniphobia-Avoidance significantly predicted Picture Sequence Memory Test performance when it was the only predictor (β = −0.335, t = −2.632, p = 0.011). When headache intensity during the assessment (β = −0.241, t = −1.571, p = 0.122) and headache severity (frequency × intensity) over the past week (β = 0.023, t = 0.151, p = 0.880) were added to the model as covariates, the coefficient for Cogniphobia-Avoidance remained significant (β = −0.384, t = −2.13, p = 0.043).
Finally, to appreciate the relative contribution of cogniphobia to cognitive test performance (Picture Sequence Memory Test), we ran a linear regression that included other candidate predictors of MTBI outcome. 34,35 In this model, Cogniphobia-Avoidance (β = −0.322, t = −2.821, p = 0.006) and performance validity (MSVT) failure (β = −.384, t = −3.281, p = 0.002) independently predicted Picture Sequence Memory performance, but a history of mental health treatment, history of prior mTBI(s), presence of loss of consciousness with the index mTBI, time since index mTBI, and current post-concussion symptom severity (BC-PSI Total Score) did not significantly contribute to the prediction model.
Discussion
A number of factors other than brain injury may influence neuropsychological test performance and daily functioning in post-acute mTBI. Intentional underperformance for secondary gain is one well-established example. 36 Other examples may include performance anxiety induced by creating an expectation of low performance by drawing attention to the subjects' mTBI diagnosis (“diagnosis threat”), 37,38 or exerting extra effort by deploying top-down control over automatic skills, as when a golfer “chokes” on a high-stakes short putt. 12,39 The present study suggests that cogniphobia may also be relevant to understanding chronic problems after mTBI. Given that fear-avoidance is common in various pain and headache disorders, 1,9,32 it can also be expected in people with post-traumatic headaches following mTBI. Theoretically, phobic anticipation of headache pain may motivate some patients to withhold mental effort and restrict their participation in mentally taxing activities, contributing not only to reduced neuropsychological test performance but potentially to functional disability, above and beyond the headache pain itself.
Patients with more severe post-traumatic headaches reported greater avoidance of mental exertion so as to not elicit or worsen a headache, confirming that the phenomenon of cogniphobia applies to mTBI in a clinic sample. The origin of beliefs regarding the dangerousness of mental exertion after MTBI may come from early experiences with activity-related symptom exacerbations, 1,40 –42 inappropriate application of the “rest until asymptomatic” maxim by health professionals, 43 or media misinformation. Although likely adaptive in the acute phase of recovery, avoiding mental exertion is not necessary to achieve a good clinical outcome from mTBI. 40,44 It may be reinforced by relief from pain and/or other symptoms, and come to unduly restrict a patient's return to pre-injury activities and exacerbate their emotional distress. Also, avoiding activity and other headache triggers can over time make those triggers more potent. 45
Our primary hypothesis was that cogniphobia would be associated with lower cognitive performance. We found that avoidance of mental exertion was associated with objectively assessed cognitive effort (performance on the “easy” subtests of the MSVT), despite a severely restricted range on these variables. It is possible that withholding effort motivated by cogniphobia accounted for reduced effort test performance, but it is also possible that other factors (e.g., compensation seeking) explained both reduced effort test performance and high scores across questionnaires, including the cogniphobia scale. Of the five NIHTB-CB fluid cognition tests, avoidance of mental exertion was significantly related to one (the Picture Sequence Memory Test), even after removing participants who failed the MSVT and adjusting for multiple testing. A supplementary analysis also found that this relationship held after controlling for headache severity (current and over the past week). Participants who reported high avoidance of mental exertion were two to four times more likely to have a low score (< 1 SD) on the Picture Sequence Memory Test than those reporting low avoidance. It is unclear why avoidance of mental exertion correlated less strongly (and nonsignificantly) with other measures of fluid cognition. The Picture Sequence Memory test requires examinees to reproduce the sequential order of 15–18 pictures. Because a high information load (intended to exceed the capacity of working memory) is presented on the first trial, this task may be perceived as especially taxing and therefore sensitive to cogniphobia. Future research demonstrating that examinees rate their perceived exertion as higher during the Picture Sequence Memory test relative to the other NIHTB-CB tests would support the theory that subjective effort mediates the effects of fear-avoidance beliefs on cognitive performance. 9
The present study demonstrated that avoidance of mental exertion was associated with other forms of avoidance in mTBI, including avoidance of physical activity and traumatic stress. Cogniphobia may be a specific manifestation of avoidant coping, a broader psychological construct that negatively influences behavioral engagement in daily activities. Exposure-based treatments have been shown to successfully target avoidance in other health conditions, 1,2 and even to decrease sensitivity to headache triggers, 46 and, therefore, should be considered for chronic mTBI. It is also shown in Table 1 that participants with high scores on the Cogniphobia-Avoidance scale were somewhat less likely to have a college degree. Low education and health literacy might also contribute to cogniphobia.
The cross-sectional design limits us from drawing conclusions about the causal nature of the relationship between cogniphobia and neuropsychological performance. Patients may perform poorly on cognitive testing because they are avoiding mental exertion and/or they may avoid mental exertion because they accurately perceive having limited cognitive capacity (or other reasons). Further research is required to better understand the clinical implications of our findings. Patients with greater cogniphobia were more likely to produce an impaired score on one test in a five test battery. This effect may not be sufficient to significantly alter treatment recommendations. The present study was also limited by not having medical records available to document the mTBI in many cases. We relied on a structured interview of the injury event, signs of altered mental status, and potential confounds of altered mental status to determine whether participants met mTBI diagnostic criteria. The optimal cutoff score for the Cogniphobia-Avoidance scale used in the relative risk analyses and for stratification in Table 1 may be specific to the present sample and might not replicate in future studies. It should be cross-validated before it is applied clinically. Fear of headache may motivate other maladaptive behaviors not measured in the present study, such as analgesic overuse 3 and restricted head movement. 32 Another limitation of the present study is that participants were not medically evaluated for specific headache disorders common after mTBI, such as migraine versus tension type. We did, however, find an effect of cogniphobia in a subgroup that probably did not have migraine-type headache based on their reporting relatively mild or absent nausea and phonophobia, suggesting that cogniphobia is not restricted to the migraine phenotype of post-traumatic headache. Finally, our findings should generalize to patients who are seeking treatment for persistent problems related to mTBI, but not to those seen in other settings.
The risk for false negative and false positive findings should be considered. Our sample may have been too small to detect true differences in cognitive domains other than memory. With effect size estimates derived from the present work, future studies on cogniphobia can prospectively calculate sample size requirements necessary to achieve adequate power. We conducted a number of supplementary (post-hoc) analyses to explore the robustness of the cogniphobia–memory performance relationship. Given the purpose of these supplementary analyses and the modest sample size, we did not further adjust for multiple testing, which could have resulted in spurious findings. These novel findings require replication.
Conclusion
In conclusion, patients who reported avoiding mental exertion because of concerns about headache performed worse on memory testing, but not on other cognitive tests. They also reported worse headaches and greater avoidance of physical activity and psychological trauma. The results partially support our hypothesis that cogniphobia contributes to cognitive difficulties in some patients with chronic symptoms after mTBI. Future research is warranted on cogniphobia and its potential role in a biopsychosocial model of poor outcome from mTBI.
Footnotes
Acknowledgments
The authors thank research assistants Mary Ellen Johnson and Sabrina Khan as well as the clinical staff at our recruitment sites, including Kelsey Davies, Jennifer Loffree, and Grace Boutilier (GF Strong Rehab Centre); Deanna Yells, Heather MacNeil, and Rod Macdonald (Fraser Health Concussion Clinic); Denise Silva and Lesley Norris (Back in Motion); and Karilyn Lao, Wayne Tang, and Cyrus Huang (LifeMark). This study was funded by a Specific Priorities Research Grant from WorkSafeBC (#RS2014-SP03). N.D.S. receives salary support from a Clinician-Scientist Career Development Award from the Vancouver Coastal Health Research Institute.
Author Disclosure Statement
G.L.I. has been reimbursed by the government, professional scientific bodies, and commercial organizations for discussing or presenting research relating to mTBI and sport-related concussion at meetings, scientific conferences, and symposiums. He has a clinical practice in forensic neuropsychology involving individuals who have sustained mTBIs. He has received honorariums for serving on research panels that provide scientific peer review of programs. He is a co-investigator, collaborator, or consultant on grants relating to mTBI funded by several organizations. N.D.S. has a clinical practice in forensic neuropsychology and W.P. has a clinical practice in forensic neuropsychiatry involving individuals who have sustained mTBIs.