
Abstract
Traumatic brain injury (TBI) has been assessed with diffusion tensor imaging (DTI), a commonly used magnetic resonance imaging (MRI) marker for white matter integrity. However, given that the DTI model only fits a single fiber orientation, results can become confounded in regions of “crossing” white matter fibers. In contrast, constrained spherical deconvolution estimates a fiber orientation distribution directly from high angular resolution diffusion-weighted images. Consequently, constrained spherical deconvolution-based measures, such as apparent fiber density (AFD) and track-weighted imaging (TWI) metrics (including tract density imaging, average pathlength mapping, and mean curvature), may be more sensitive than DTI metrics to white matter injury post-TBI. As such, this study administered the lateral fluid percussion injury (FPI) model of TBI, assessed for changes in AFD and TWI metrics, and compared these results to the DTI metrics, fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD). Rats received either an FPI (n = 11) or sham injury (n = 9) and after a recovery period of 12 weeks underwent MRI. AFD was calculated as described previously and statistical testing was performed using connectivity-based fixel enhancement. TWI and DTI metrics were assessed using voxel-wise nonparametric permutation testing. We found that rats given an FPI had significantly reduced AFD, tract density, average pathlength, and mean curvature when compared to sham-injured rats and significant changes in DTI metrics, including reduced FA and increased MD, RD, and AD. However, the latter DTI metrics identified fewer voxels affected by TBI. Additionally, analysis of AFD with connectivity-based fixel enhancement was the only method that identified damage within the corticospinal tract of rats given an FPI. These results support the use of constrained spherical deconvolution, in conjunction with DTI metrics, to better assess disease progression and treatment post-TBI.
Introduction
T
Diffusion-weighted imaging (DWI) is an MRI technique that is sensitive to the hindrance and restriction of water molecules as they move and interact with cell membranes, neurites, and macromolecules. In typical diffusion measurement times, displacement of water molecules is short, on the order of 5–15 μm, and as such, DWI is sensitive to the underlying structure of the tissue of interest. 4,5 Introduced in 1994, diffusion tensor imaging (DTI) fits an ellipsoidal model (tensor) to a collection of image volumes with diffusion weighting applied in different directions, modeling the degree of anisotropy and diffusion of water molecules in the underlying tissue. 6 The resulting diffusion tensor eigenvalues and eigenvectors give rise to a number of markers, including fractional anisotropy (FA) and mean diffusivity (MD). DTI has become a common marker for white matter integrity in neurological conditions, and changes in DTI measures have been reported post-TBI. 7 –13
Since its introduction, new DWI acquisition methods and modeling techniques have emerged with the aim of developing markers with greater sensitivity to changes in white matter microstructure. Unlike the diffusion tensor model, which fits a single fiber orientation and is confounded in regions of “crossing” and “kissing” fibers, constrained spherical deconvolution estimates a fiber orientation distribution (FOD) directly from high angular resolution diffusion images without needing to make any a priori assumptions about the number of distinct fiber bundles or any dependence on a specific model of diffusion (Fig. 1). 14 Instead, the diffusion-weighted signal attenuation for a voxel containing multiple fiber bundles is modeled as a spherical convolution of the distribution of fiber orientations within the voxel (i.e., the FOD) and an axially symmetric response function representing the signal attenuation expected from a single fiber bundle. Because the response function can be directly estimated from voxels that are highly likely to contain a single fiber bundle, the FOD can be obtained for voxels with crossing fiber bundles by applying spherical deconvolution. 14 However, spherical deconvolution is susceptible to noise, which results in negative lobes in the FOD. By placing a non-negativity constraint on the FOD, more-reliable FOD estimates are obtained and it is possible to resolve fiber bundles orientated at more acute angles. 15
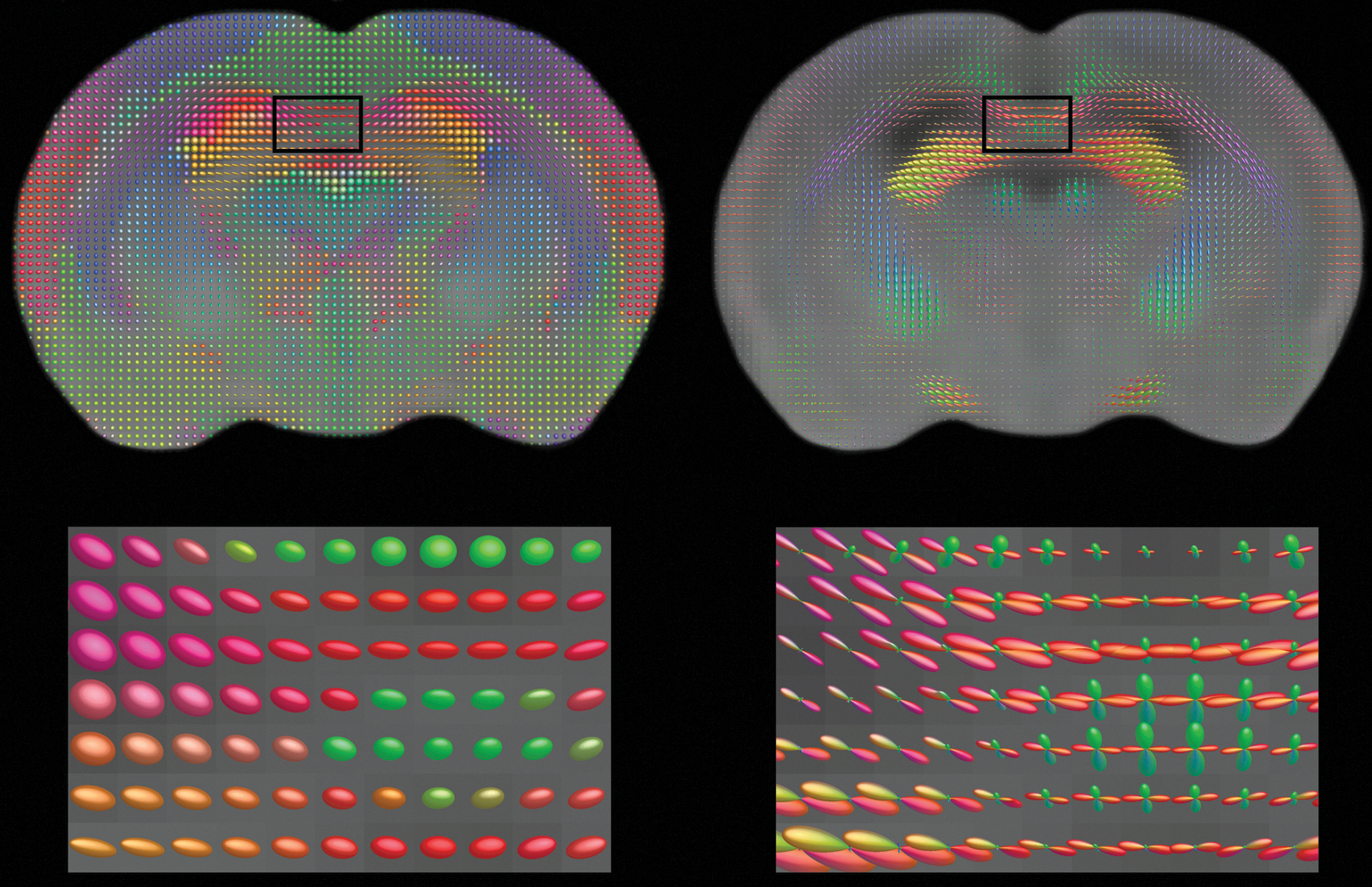
Fiber orientation distribution (FOD) estimated using constrained spherical deconvolution. A coronal section of the rat brain showing diffusion tensor (left column) and FOD (right column) estimations determined from high angular resolution diffusion images. In contrast to diffusion tensor imaging, which fits an ellipsoid representing only a single fiber orientation, constrained spherical deconvolution estimates an FOD and is able to resolve multiple fiber bundles in single voxels (see zoomed sections below). Tensor ellipsoids and FODs are color encoded according to direction: medial/lateral is mapped to red, rostral/caudal to green, and dorsal/ventral to blue.
When the extracellular water signal is attenuated by high b-values (≥3000 s/mm2), the FOD amplitude in a particular direction is approximately proportional to the total intra-axonal volume of the corresponding fiber bundle oriented in that direction. This allows the concept of apparent fiber density (AFD) to be defined as the fraction of space occupied by a fiber bundle. 16 Given that each voxel may contain multiple fiber bundles, and therefore multiple AFDs, it is referred to as a fixel-based measure, where the term fixel refers to a specific population of fibers that pass through the voxel. 17 Recently, Raffelt and colleagues introduced a new statistical framework, called connectivity-based fixel enhancement, to analyze fixel-based measures such as AFD. 17 Connectivity-based fixel enhancement uses probabilistic tractography to identify fixels that are structurally connected by specific fiber populations and therefore more likely to share underlying pathology. It has been shown that whole-brain analysis of AFD using connectivity-based fixel enhancement was more sensitive than analysis of FA with tract-based spatial statistics (TBSS), a common method for voxel-based analysis of diffusion metrics. 17 Of particular relevance here, significant decreases in AFD were observed in the corticospinal tract and corpus callosum of motor neuron disease patients, two white matter bundles that are commonly affected post-TBI. 11 –13,18 –23 As such, connectivity-based fixel analysis of AFD may also be a sensitive marker of axonal injury post-TBI.
Constrained spherical deconvolution–derived FODs can also be used for tractography, a DWI post-processing technique that connects voxels based on their FODs, to guide streamlines along continuous fiber bundles in the brain. Unlike seed/target tractography, where streamlines are seeded from a known region of interest (ROI) and retained if they intersect with a target ROI, whole-brain tractography seeds streamlines from everywhere within the brain parenchyma to form a tractogram. This allows the entire white matter to be investigated without any user input on factors, such as past knowledge of which bundles are likely to be affected. One technique for assessing the tractogram is track-weighted imaging (TWI), which uses properties of the tractogram streamlines, such as streamline density, length, and curvature, to potentially reveal additional insights into white matter pathology. 24 –26 In the present study, rats were given either a lateral fluid percussion injury (FPI) or sham injury and white matter was assessed using AFD, TWI, and traditional DTI metrics. The lateral FPI model localizes injury to one hemisphere and is one of the most widely used, well-characterized models of TBI. 3 At moderate-to-severe levels, the lateral FPI results in a focal contusion and widespread diffuse axonal injury that can lead to progressive neurodegeneration and persisting neurological deficits. 3,23 As such, both distinct and more-subtle changes to diffusion metrics are expected throughout the brain following a lateral FPI. Here, it was hypothesized that the lateral FPI would result in significant changes in AFD- and TWI-derived metrics, and that these markers would be more sensitive than DTI metrics, detecting a wider pattern of diffusion changes throughout the brain of TBI rats compared to sham-injured rats.
Methods
Subjects
Twenty male Long-Evans hooded rats were purchased from Monash animal research services (Melbourne, Australia). Rats were 12 weeks of age and weighed 250–300 g at the time of injury. Rats were housed individually under a 12-h light/dark cycle and given access to food and water ad libitum for the duration of the experiment. All experimental procedures were approved by the Melbourne Health and The Florey Institute of Neuroscience and Mental Health Animal Ethics Committees (AEC#1112173, 12-100-FNI).
Lateral fluid percussion injury
The FPI has been described in detail elsewhere. 21,22,27,28 In brief, anesthetized rats underwent a craniotomy, creating a 3-mm-diameter window centered 3 mm posterior to bregma and 6 mm laterally, to expose the intact dura. An injury cap was then affixed to the skull over the window using cyanoacrylate and dental cement, filled with sterile silicon oil, and connected to the fluid percussion device. Anesthesia was then withdrawn, and at the first sign of hindpaw withdrawal to a pinch test, rats received a fluid percussion pulse of 3 atmospheres (n = 11). Three of these rats died immediately post-injury (27% mortality); thus, the total number of fluid-percussion–injured rats included was 8. Acute injury measures were monitored and included: duration of apnea, defined as the time from injury to the return of spontaneous breathing (sham/FPI, 0/43.5 ± 6.4 sec; p < 0.001); loss of consciousness (LOC), defined as the time to hindlimb withdrawal to a pinch test (sham/FPI, 0/310.2 ± 28.6 sec; p < 0.001); and time to self-righting, defined as the time from injury to return of an upright position (sham/FPI, 158.1 ± 15.4/511.3 ± 34.8 sec; p < 0.001). Upon resumption of spontaneous breathing, the injury cap was removed and the incision sutured. The protocol was identical for sham injuries, but no fluid percussion pulse was given (n = 9). A previous study conducted by our group revealed significant changes to DTI metrics following lateral FPI in 8 rats when compared to 10 shams. 28 Because AFD and TWI were hypothesized to be more-sensitive markers of injury, a similar number of animals per group was used here.
Magnetic resonance imaging acquisition
MRI was performed 12 weeks post-injury using a 4.7-Tesla Bruker Avance III scanner fitted with a BGA12S2 gradient set (Bruker BioSpin, Ettlingen, Germany) and running ParaVision 5.1. Actively decoupled volume transmit (internal diameter, 86 mm) and four-channel surface receive coils (Bruker) were used for imaging. Rats were anesthetized in a clear plastic box with 5% isoflurane in a 1:1 mixture of medical-grade air and oxygen. After LOC, rats were laid supinely on a purpose-built animal bed with ear and bite bars for stereotactic fixation and a hot-water circulation system for maintaining body temperature. During imaging, anesthesia was maintained with 2% isoflurane delivered through a nose cone in a 1:1 mixture of medical grade air (500 mL/min) and oxygen (500 mL/min).
After scouting scans to determine the orientation of the rat brain, a single-shot echo planar image was acquired with 126 diffusion gradient directions with diffusion duration (δ) = 5 ms, diffusion gradient separation (Δ) = 14 ms, and b-value = 3,000 s/mm2. Ten nondiffusion images (b0) were also acquired. Imaging parameters included: repetition time = 9 sec, echo time = 37 ms, field of view = 38.4 × 38.4 mm2, partial parallel imaging acceleration = 2, matrix size = 128 × 128, slices = 36, isotropic spatial resolution = 3003 μm3, and total imaging time = 20 min 24 sec. Processing of high angular resolution diffusion images is outlined in Figure 2 and described in more detail below.
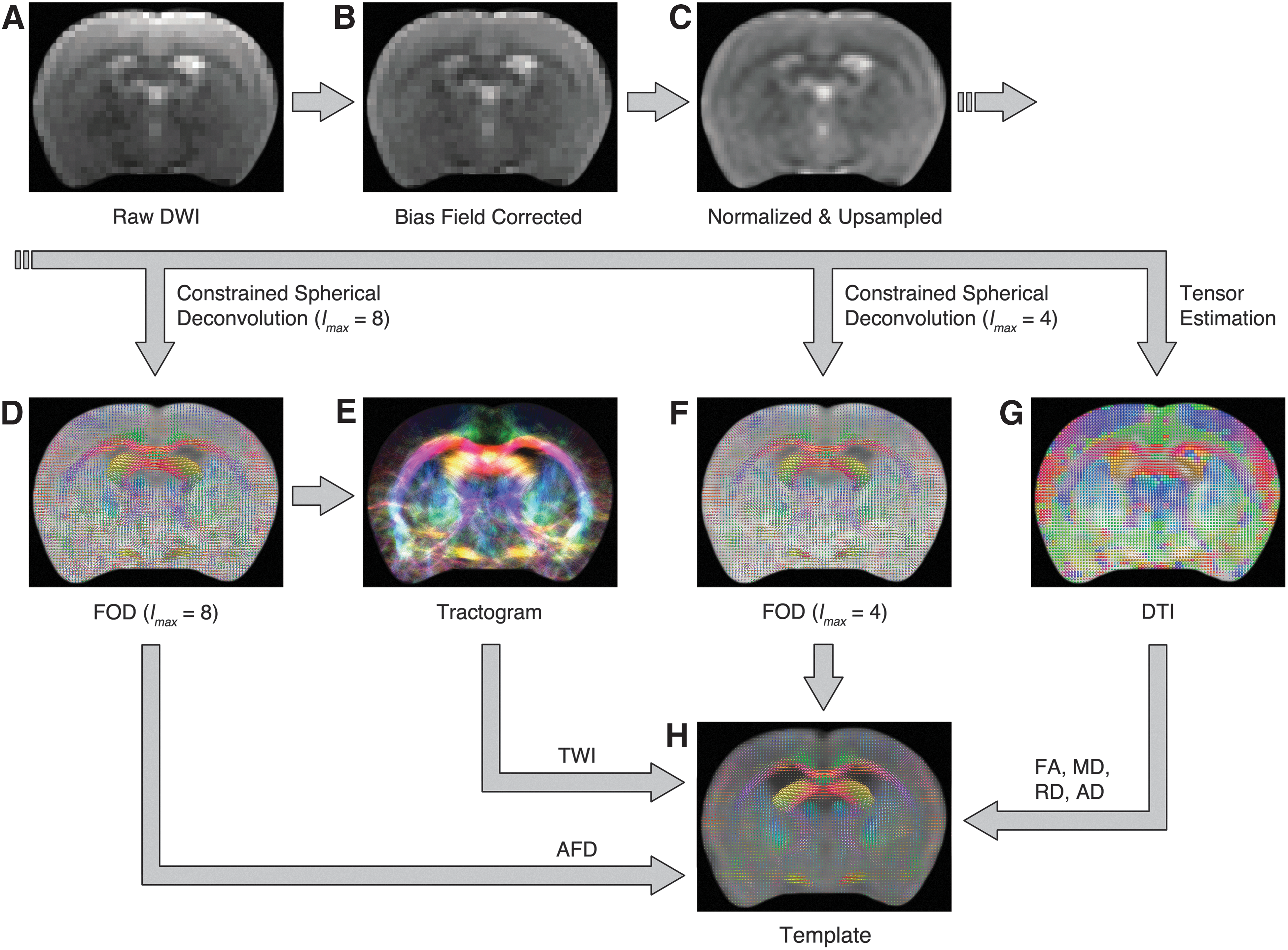
Image processing pipeline. (
Apparent fiber density
AFD computation and analysis was performed as outlined previously.
16,17
Diffusion data sets were corrected for spatial intensity inhomogeneity using N4 bias field correction
29
and normalized to the signal intensity of cerebrospinal fluid on the b0 images. The data sets were upsampled by a factor of 2 because this has been suggested to improve image registration and statistical analysis in subsequent cluster-based statistical methods.
16
FODs were computed by constrained spherical deconvolution using the MRtrix software package (
Track-weighted imaging
Tractograms with 2 million streamlines were generated in native space for each rat using the same parameters outlined above and registered to the study-specific FOD template, ensuring that both the length and spatial location of the streamlines were normalized. 25 The registered tractograms were then used to generate three TWIs: track density imaging (TDI), which sums the number of streamlines passing through each voxel; average pathlength mapping (APM), which maps the mean length of each streamline traversing the voxel; and mean curvature, which maps the mean curvature of each streamline traversing the voxel. Group differences were assessed using nonparametric permutation testing with 5000 permutations and threshold-free cluster enhancement. 32 An FWE-corrected p value <0.005 was considered significant.
Diffusion tensor imaging
TBSS is currently the most commonly used method for voxel-wise analysis of DTI metrics. 33 However, TBSS only assesses DTI metrics on a tract skeleton calculated from voxels with high FA and therefore excludes voxels with low FA, including voxels in regions of crossing fibers. Because both AFD and TWIs were assessed over the whole brain, here we used a whole-brain, voxel-wise analysis instead of TBSS to assess each of the DTI metrics. FA, MD, radial diffusivity (RD), and axial diffusivity (AD) were reconstructed and transformed into the study-specific template space using MRtrix. Voxel-wise cross-subject statistical analysis was performed with 5000 permutations and threshold-free cluster enhancement. 32 An FWE-corrected p value <0.005 was considered significant.
Comparison of diffusion metrics
Each of the aforementioned nonparametric permutation tests resulted in an image where each voxel's value was the FWE-corrected p value reflecting the likelihood that the TBI and sham groups were significantly different. The total number of voxels with p < 0.005 were calculated and graphed as an indication of each method's sensitivity to diffusion changes post-TBI.
Results
Apparent fiber density
As shown in Figure 3, a significant decrease in AFD was observed in TBI rats compared to sham-injured rats (FWE corrected, p < 0.005). Regions affected were predominantly ipsilateral to the injury and included the corticospinal tract, external capsule, fimbria, and corpus callosum. Reduced AFD extended along the corpus callosum from the ipsilateral to contralateral hemisphere.
Traumatic brain injury (TBI) results in significantly reduced apparent fiber density (AFD). Rats given a TBI had significantly reduced AFD (family-wise error corrected, p < 0.005, blue/red color scale) when compared to sham-injured rats. Affected regions included the ipsilateral corticospinal tract, external capsule, fimbria of the hippocampus, and bilaterally in the corpus callosum. AFD results are shown overlaid on the sham-injured fractional anisotropy template image (gray scale).
Track-weighted imaging
TBI resulted in significant changes to TWI measures when compared to sham-injured rats. Nonparametric permutation testing of whole-brain TDI revealed that rats given a TBI had significantly fewer streamlines in the ipsilateral corpus callosum, fimbria, and internal capsule when compared to sham-injured rats (Fig. 4A; FWE corrected, p < 0.005). TBI rat streamlines were also significantly shorter as shown by a similar pattern of reduced average pathlengths that also included the contralateral corpus callosum (Fig. 4B; FWE corrected, p < 0.005). Additionally, analysis of mean curvature revealed that TBI rat streamlines were also significantly straighter than sham-injured rats within the corpus callosum bilaterally, as well as the ipsilateral fimbria, internal capsule, and further anterior in the medial forebrain bundle (Fig. 4C; FWE corrected, p < 0.005).
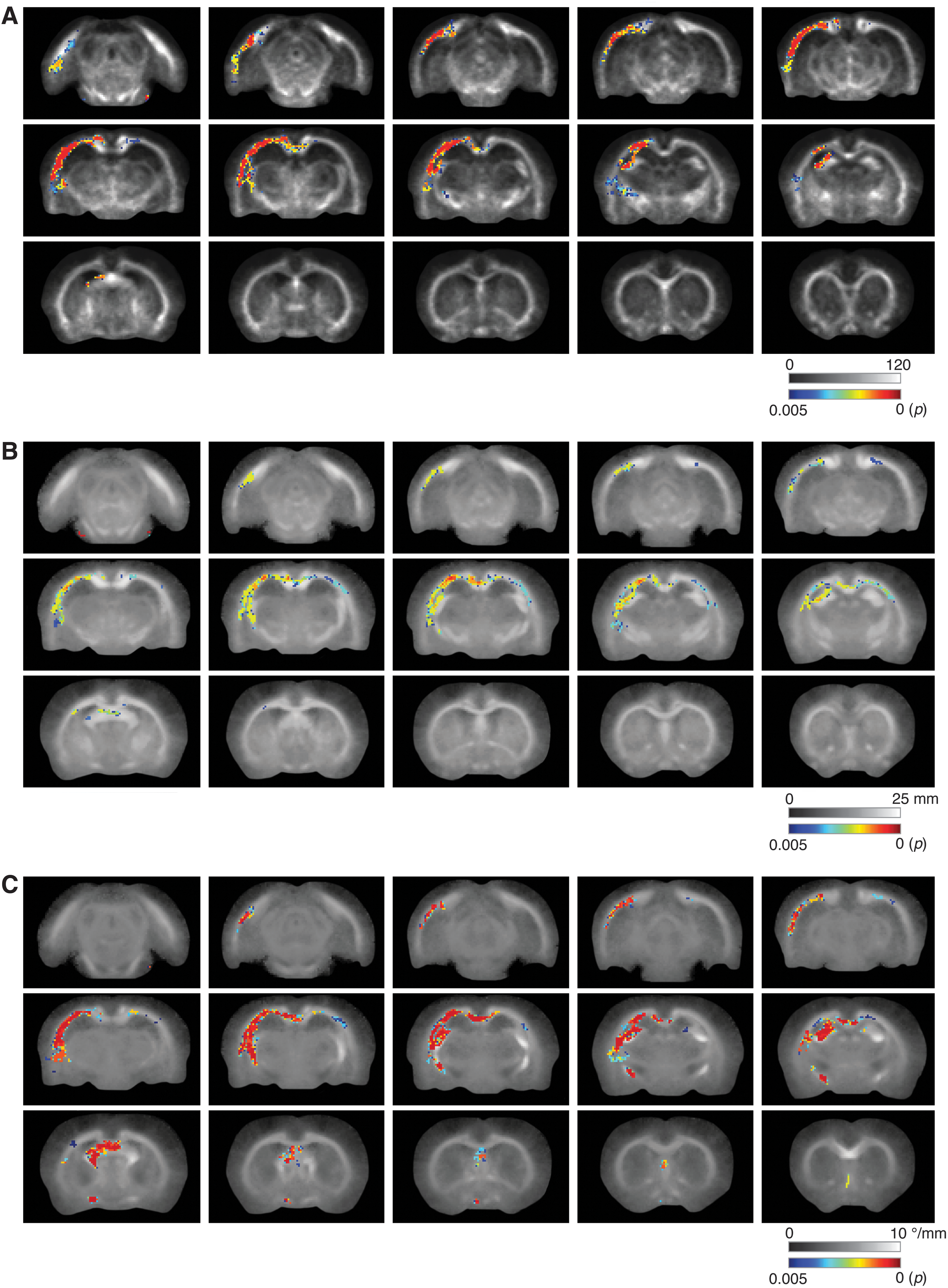
Traumatic brain injury (TBI) results in significant changes in track-weighted image measures. (
Diffusion tensor imaging
Nonparametric permutation testing of whole-brain DTI metrics also revealed significant changes post-TBI. Of these, significantly decreased FA was the most widespread, following a similar pattern to the changes observed in average pathlength (Fig. 5A; FWE corrected, p < 0.005). MD (Fig. 5B) and RD (Fig. 5C) exhibited a similar pattern of increased diffusivity, but over a less-extensive region than FA (FWE corrected, p < 0.005). AD was also significantly increased in a small region of the posterior ipsilateral corpus callosum and fimbria; however the changes were much more focused than the other DTI metrics (Fig. 6; FWE corrected, p < 0.005).
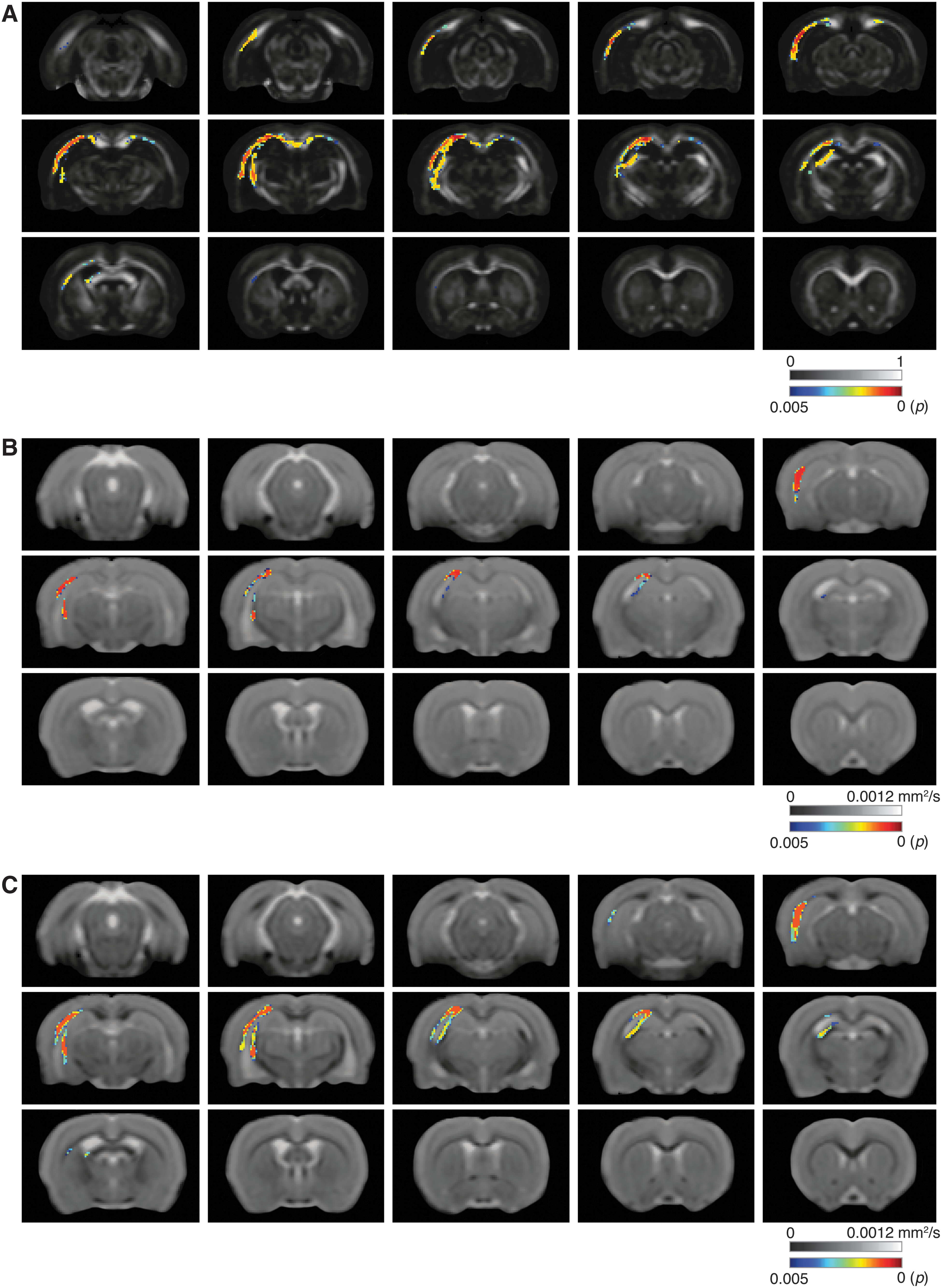
Traumatic brain injury (TBI) results in significant changes in diffusion tensor metrics. (
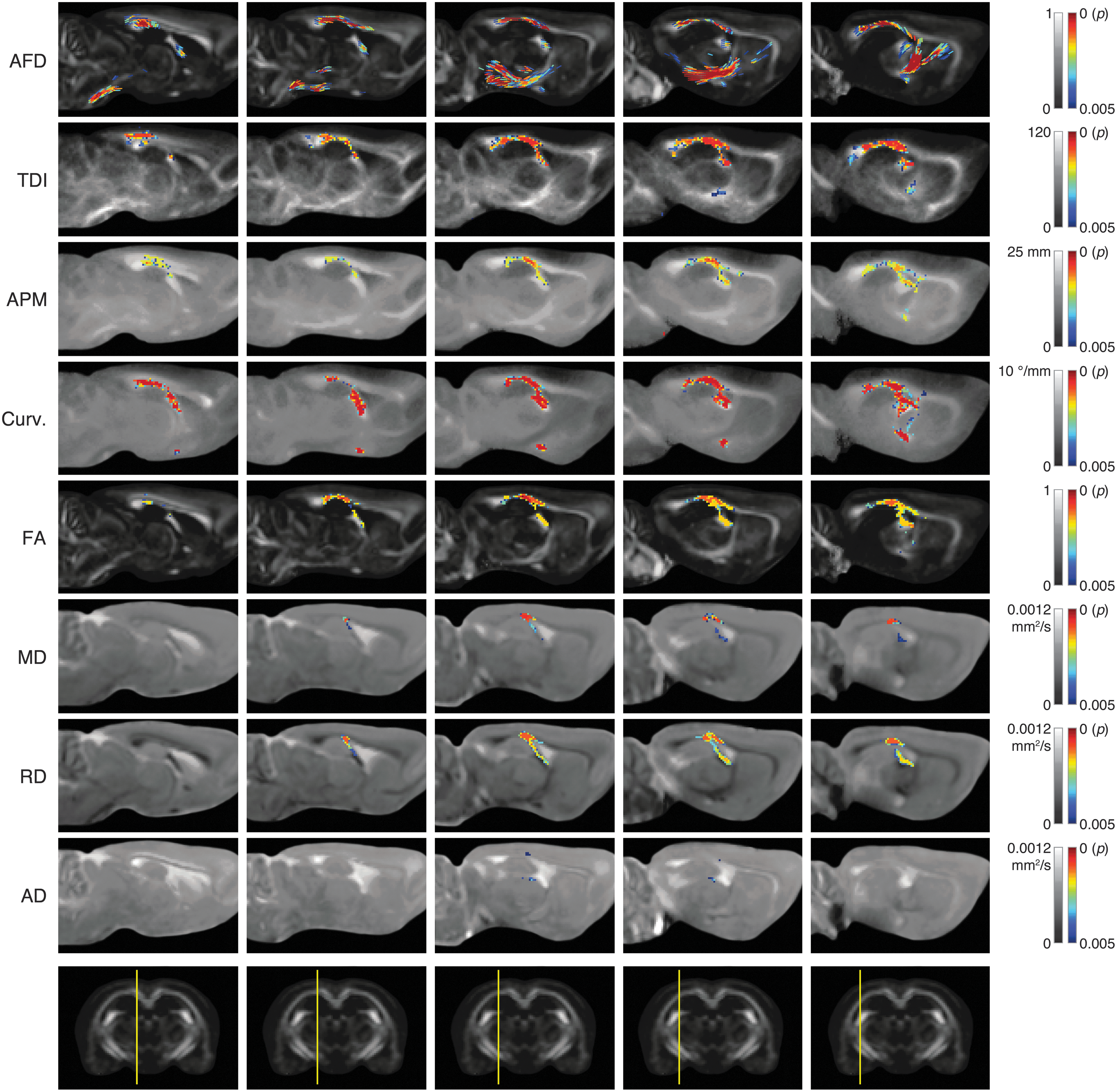
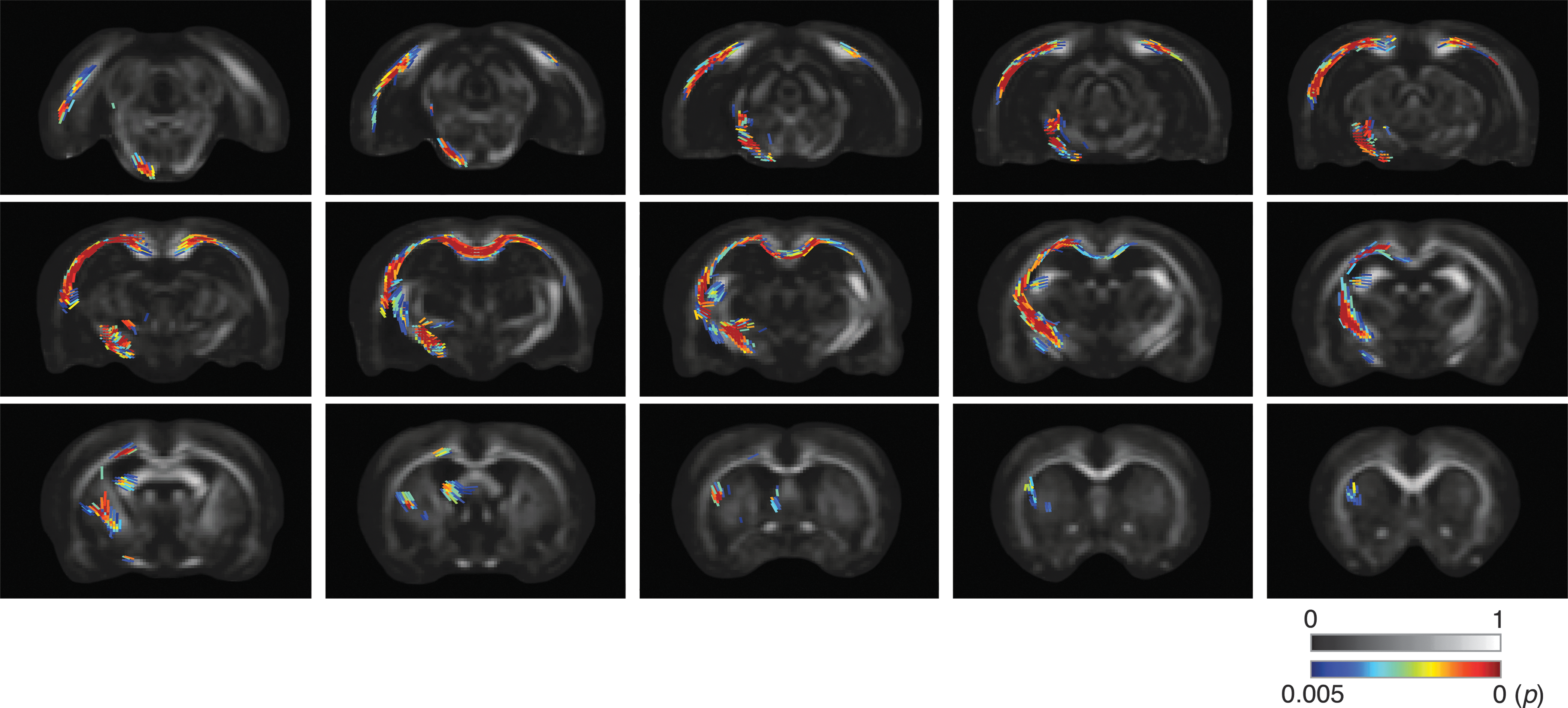
Ipsilateral corticospinal tract degeneration after traumatic brain injury. Analysis of apparent fiber density (AFD) with connectivity-based fixel enhancement revealed significantly reduced AFD in the ipsilateral corticospinal tract of rats given a fluid percussion injury (top row). Both AFD and the track-weighted imaging metrics: track density imaging (TDI), average pathlength mapping (APM), and mean curvature (Curv.) detected a more widespread pattern of diffusion changes than traditional diffusion tensor markers (family-wise error corrected, p < 0.005, blue/red color scales). Gray scale bars correspond to the underlying image value and the sagittal slice position is indicated on the coronal section at bottom. FA, fractional anisotropy; MD, mean diffusivity; RD, radial diffusivity; AD, axial diffusivity.
Corticospinal tract degeneration
Figure 6 shows five sagittal slices through the ipsilateral corticospinal tract, a white matter bundle known to be affected post-TBI. Significant differences between sham and TBI rats are shown overlaid in blue/red color maps for each of the diffusion measures investigated (FWE corrected, p < 0.005). Only analysis of AFD with connectivity-based fixel enhancement revealed significant differences along the length of the corticospinal tract post-TBI (Fig. 6, top row).
Diffusion marker sensitivity
As outlined above, nonparametric permutation testing of group differences revealed significant differences (FWE corrected, p < 0.005) in each of the diffusion markers post-TBI. The number of significant voxels was counted for each metric, and the total is graphed in Figure 7 as a measure of each marker's sensitivity to change post-TBI. As predicted by Figures 3 and 6, nonparametric permutation testing of group differences in AFD revealed the greatest number of significant voxels post-TBI, suggesting that this was the most sensitive diffusion marker assessed. Tract density imaging and mean curvature also revealed a more-widespread pattern of diffusion changes (i.e., a greater number of voxels with p < 0.005 following permutation testing of TBI and sham group differences) than average pathlength mapping, FA, and the less-sensitive diffusivity measures, MD, RD, and AD.

Analysis of apparent fiber density (AFD) with connectivity-based fixel enhancement identified the greatest volume of significant change after traumatic brain injury (TBI). Total number of significant voxels (family-wise error corrected, p < 0.005) detected by nonparametric permutation testing for group differences in each diffusion marker. AFD (black) and track-weighted imaging (TWI; dark gray) measures were more sensitive than traditional diffusion tensor image (DTI; light gray) metrics, with a greater number of voxels exhibiting significant differences between TBI and sham groups. Curv., mean curvature; TDI, track density imaging; APM, average pathlength mapping; FA, fractional anisotropy; RD, radial diffusivity; MD, mean diffusivity; AD, axial diffusivity.
Discussion
TBI commonly results in changes to white matter, 1 which can affect the diffusion of water molecules within the brain. Consequently, DWI methods have the potential to provide serial and in vivo markers of these changes. Here, we assessed the ability of constrained spherical deconvolution– and DTI-based metrics in detecting diffusion changes in white matter 12 weeks after an experimental TBI in rats. We found that rats given an FPI had reduced AFD, track density, average pathlength, and mean curvature when compared to sham-injured rats, as well as significant changes in DTI metrics, including reduced FA and increased MD, RD, and AD. However, as hypothesized, and consistent with earlier work, 17 the latter metrics identified fewer voxels affected by TBI. These results support the use of constrained spherical deconvolution, in conjunction with DTI metrics, to more comprehensively assess diffusion changes post-TBI.
Regardless of the method used, the observed diffusion changes in this study were predominantly found within the corpus callosum, external capsule, and fimbria, all of which are white matter bundles commonly damaged post-FPI in the rat. 21 –23,34 –37 Notably, fixel-based analysis of AFD was the only method that identified damage within the corticospinal tract of rats given an FPI, which emphasizes the potential sensitivity of this method. Our results showing reduced AFD in these tracts concurs with the work of Raffelt and colleagues, who reported reduced AFD in both the corpus callosum and corticospinal tracts of motor neuron disease patients compared to healthy controls. 17 Of interest, TBI has been proposed as a risk factor for the latter onset of motor neuron disease, and, recently, we showed that rats given an FPI develop pathophysiology consistent with a motor neuron disease–like process. 23
TWI utilizes properties of the tractogram streamlines, such as length and curvature, to provide additional forms of contrast. We assessed TDI, APM, and mean curvature and found significant reductions in each post-FPI in rats. Consistent with our results here, Pannek and colleagues showed that average pathlength was significantly reduced in the corpus callosum of a single TBI patient compared to a cohort of normal controls. 25 Recently, our group showed that mean curvature was more sensitive than APM in detecting injury following experimental mild TBI, 22 and our results here in a moderate TBI model further highlight the potential of mean curvature as a marker of white matter abnormalities induced by TBI. Whereas TDI has been suggested to be less reliable than other track-weighted images, and more suited to a qualitative assessment of the brain anatomy, 24 our results here also support its use as a marker sensitive to axonal injury post-TBI. These results also concur with earlier work showing reduced track density in the corpus callosum of rats given repeated mild TBI. 35 Although not as robust as the AFD and TWI findings, analysis of DTI metrics still revealed reduced FA and increased MD, RD, and AD in white matter of rats given an FPI, concurring with earlier FPI studies from our group. 21,22,35,38 However, both decreases and increases in FA, as well as opposing changes in diffusivity measures, have been reported in clinical studies of TBI. 7 –13 There are a number of possible reasons for such discrepancies, including the heterogeneous injuries, patient populations, and injury-to-imaging intervals observed in studies of clinical TBI. Another possibility is the limitations of the diffusion tensor in regions of crossing fibers. 5 For example, although a voxel containing a single fiber bundle will have a high FA, a voxel containing crossing (i.e., perpendicular) fiber bundles will have a low FA value. In this case, it is plausible that degeneration of a single fiber bundle will increase FA, whereas FA will remain low if both bundles are affected. Given the high number of voxels that contain multiple fiber populations within a typical diffusion data set, 39 this may explain why, in contrast to AFD, DTI-based metrics showed no difference between TBI- and sham-injured rats in the corticospinal tract and were also less sensitive than APM, TDI, and mean curvature, in detecting injury post-FPI.
There are limitations with this study that should be considered. Here, we focused on diffusion abnormalities in white matter 12 weeks post-injury. Although chronic diffuse axonal injury is a common feature of TBI, 40 it is important to acknowledge that TBI is a complex and progressive condition that involves a wide range of pathophysiological mechanisms. These may include neuroinflammation, gliosis, edema, excitotoxicity, and oxidative stress. 37 Notably, some of these pathologies are capable of influencing diffusion in gray and white matter. For example, rats given an experimental TBI had a persisting increase in FA in the injured cortex that was associated with gliosis and not axons. 41 Increased FA and decreased MD have also been used as markers of cytotoxic edema in injured gray matter structures (e.g., hippocampus) in the acute stages of experimental TBI. 42 Another limitation with the current study is that it did not incorporate direct measures of white matter pathology that would have elucidated the mechanisms underlying the diffusion measures observed. However, some insight into this question is provided by previous studies. For example, Laitinen and colleagues reported a loss of myelinated axons post-FPI that resulted in a thinning of the corpus callosum, which is consistent with our observation of reduced AFD in these areas. 34 Another study reported edema, myelin debris associated with macrophage infiltration, and increased microglia within the external capsule, as well as a loss of myelinated axons 3 months post-FPI in the rat. 37 Nonetheless, future studies making direct comparisons between diffusion measures and pathology will be important to improve the specificity of diffusion markers in TBI.
Finally, our findings support the incorporation of AFD and TWI into TBI studies. Currently, an appropriate diffusion-weighted data set with approximately 60 diffusion directions and b-value of 3000 s/mm2 can be acquired in less than 10 min using a 3T clinical scanner and standard diffusion sequence, making it feasible for use in clinical studies. However, it is also possible to perform constrained spherical deconvolution using diffusion data acquired with as few as 20 directions and a b-value of only 1000 s/mm2, 15 which opens the possibility of performing retrospective analyses on earlier tensor-based studies of TBI.
In conclusion, this study investigated the use of AFD and TWI markers in an experimental model of TBI and found reduced AFD bilaterally in the corpus callosum and in the ipsilateral corticospinal tract of rats given a TBI. Additionally, these rats also had reduced average pathlength, track density, and mean curvature when compared to sham-injured rats as well as significant changes in DTI metrics, including reduced FA and increased MD, RD, and AD. Although future studies are required to investigate the specificity of AFD and TWI measures, our findings that they are both more sensitive than traditional DTI in detecting diffusion changes post-TBI support their integration into TBI research and may prove useful in improving our understanding of disease progression and treatment.
Footnotes
Acknowledgments
This work was supported by funding to S.S. and T.O. from the Australian National Health and Medical Research Council, the Canadian Institute of Health Research, and Victorian Neurotrauma Initiative project. The authors acknowledge the facilities, and the scientific and technical assistance, of the National Imaging Facility at the Florey Institute of Neuroscience and Mental Health (Parkville, VIC, Australia).
Author Disclosure Statement
No competing financial interests exist.