
Abstract
Autonomic dysfunction and diminished capacity for physical exercise are commonly implicated in the 3- to 4-fold increased risk of cerebrovascular disease after spinal cord injury (SCI). We assessed cerebrovascular function (transcranial Doppler; neurovascular coupling [NVC], and cerebral pressure-flow regulation) in elite national level wheelchair rugby players (n = 23), normally active SCI individuals (n = 12), and able-bodied controls (n = 13). Cognitive (Stroop test) and autonomic function (postural change) also were evaluated. SCI individuals demonstrated reduced posterior cerebral blood flow, as well as impaired cerebrovascular and cognitive function. Autonomic dysfunction but not physical activity was related to impaired NVC and cerebral pressure-flow regulation after SCI. Routine upper-body exercise, as utilized by elite wheelchair rugby athletes, may not elicit beneficial cerebrovascular effects. On the other hand, autonomic dysfunction needs to be considered a key culprit in cerebrovascular diseases after SCI.
Introduction
C
In non-SCI populations, greater participation in moderate- to-vigorous physical activity is associated with greater cerebrovascular health, reduced risk of stroke, 6 and improved cognition. 7 After SCI, physical activity is commonly markedly reduced, 1 and physical activity is primarily limited to the upper limbs. This is a crucial issue, as upper body exercise may not influence cardiovascular health to the same extent as exercise modalities using both upper and lower limbs. In support of this, recent work demonstrated that body exercise does not improve endothelial health or aortic stiffness after SCI. 8,9
Normal cerebrovascular function is critically dependent on the sympathetic division of the autonomic nervous system, through both providing sufficient blood pressure for the cerebrovasculature to be perfused with blood and directly regulating vascular tone. 10,11 As such, the disruption of sympathetic pathways after SCI is likely contributing to cerebrovascular dysfunction in this population. 1 We do not presently understand the roles of physical activity and the autonomic nervous system in cerebrovascular function after SCI. Using the largest sample to date, we examined the correlative role physical activity plays in cerebrovascular and cognitive function after SCI. To explore the hypothesis that physical activity would provide less benefit in SCI, we compared NVC and cerebral pressure-flow regulation between normally active and elite athletes with SCI. We also assessed the role autonomic injury plays in cerebrovascular function utilizing an orthostatic test to evaluate the extent of autonomic dysfunction. We reasoned that the degree of autonomic dysfunction would be correlated to the extent of cerebrovascular impairment.
Methods
The 23 individuals with SCI in the SCI athlete group were elite national-team wheelchair rugby athletes assessed at the 2015 ParaPan American Games. The age -matched SCI non-athletes (n = 12), and able-bodied individuals (n = 13) were assessed in Vancouver according to the identical procedure. All SCI participants with the exception of two had sustained motor-complete injuries, and all were injured at or above the 4th thoracic spinal segment. All participants were instructed to abstain from exercise and alcohol for 24 h before testing and caffeine on the day of testing, and to only have a small meal (e.g., a small yogurt) approximately 1 h before testing. Participants with any history of brain injury were excluded from participation. All participants provided written informed consent in accord with the Clinical Research Ethics Board at the University of British Columbia and the International Paralympic Committee, who approved this study. Participants were tested over a 1-h protocol that consisted of at least 15 min resting in the supine position while being outfitted with assessment equipment, followed by at least 10 min of supine rest, which proceeded to a 10-min duration sit-up test that we have previously described and shown to be a reliable test of orthostatic hypotension. 12 For each participant, brachial blood pressure (BP) was measured (Dinamap, General Electric Pro 300V2; Tampa, FL) on the left brachial artery each minute throughout the protocol.
The following were sampled at 1000 Hz using an analog-to-digital converter (Powerlab/16SP ML 795; ADInstruments, Colorado Springs, CO) interfaced with data acquisition software on a laptop computer (LabChart 8; ADInstruments): beat-by-beat blood pressure via finger photoplethysmography (Finometer PRO; Finapres Medicine Systems, Amsterdam, the Netherlands), and electrocardiogram. In order to ensure that hemispheric differences in velocity did not influence our results, which do occur in the posterior cerebral artery (PCA), 13 cerebral blood velocity was consistently recorded in the right middle cerebral artery (MCA) and the left PCA (P1 segment; ST3 Transcranial Doppler; Spencer Technologies, Redmond, WA). These arteries were insonated using a 2 Mhz probe mounted on the temporal bone and a fitted head-strap, according to detailed instructions published elsewhere by our group. 2,4 Systolic and diastolic BP (SBP, DBP), as well as peak MCA blood velocity and PCA blood velocity (MCAv, PCAv) and minimum MCAv/PCAv, were then extracted to generate mean steady-state values for the given stage (vmin). From these values, mean arterial pressure as (2*DBP+SBP)/3 and mean MCAv/PCAv as (2*MCAv/PCAv minimum+MCAv/PCAv maximum)/3 were calculated. This also allowed for the calculation of cerebrovascular conductance as mean MCAv/PCAv/mean arterial pressure on a beat-by-beat basis.
Orthostatic challenge test
To assess orthostatic tolerance, participants were passively raised to a seated position. Blood pressure was continuously monitored throughout. Using minute-by-minute blood pressure readings, the severity of orthostatic intolerance was calculated by subtracting the maximum decline in SBP from the 2 to 3 min average of supine blood pressure recordings collected just prior to assuming the seated position. Orthostatic hypotension was defined as a drop in SBP >20 mm Hg or a decrease in diastolic blood pressure >10 mm Hg. 1 We have previously shown the severity of orthostatic hypotension after SCI is related to disruption of descending sympatho-excitatory fibers in the spinal cord, 14 which is the primary cause of cardiovascular autonomic dysfunction in this population.
Physical activity levels
All participants completed the Godin–Shephard Leisure Time Physical Activity Questionnaire, which is reliable and valid for assessing physical activity, 15 and which we have previously utilized for comparison between SCI and able-bodied individuals. 9,16,17 As per Godin's guidelines, 18 only units of moderate and vigorous physical activity were evaluated in relationship to measures of arterial stiffness.
Cognitive function
Selective attention and conflict resolution was assessed by the Stroop test, 19 which was comprised of three conditions with 80 trials each. In the first condition, participants read our words printed in black ink (P1). Second, participants named the displayed color of colored X's printed over black ink (P2). Last, while participants were shown color-words printed in dissimilar colors as to what the letters spelled (e.g., the letters “r-e-d” printed in blue ink), they were asked to name the color the word appeared, and therefore avoid saying the word typed (P3). The P3-P2 time was calculated as a marker of attention and conflict resolution, where a smaller time difference indicates better cognitive performance. 20 Spanish (n = 8) and Portuguese (n = 9) Stroop tests were utilized to allow assessments in participants' native language.
Neurovascular coupling
While measuring beat-by-beat blood pressure, PCAv and MCAv, our standardized visualization task was employed was utilized to elicit activation of the visual cortex, 21 and therefore stimulated hyperemia throughout cerebrovasculature perfused by the PCA. 21 The protocol involved repeating five to seven cycles of 30-sec eyes closed rest, followed by 30 sec of eyes open while tracking the side to side hand motion of assessor, and was analyzed using our proprietary automated software. 21 The dynamic relationships between spontaneous oscillations in BP and MCAv/PCAv were evaluated using transfer function analysis as previously described. 4 Following the assessment of variance homogeneity (Shapiro-Wilk test), SCI athletes, non-athletes, and able-bodied controls were compared using one-way analysis of variance (ANOVA) with Tukey post hoc analysis. Where homogeneity of variances was violated, a Welch F-test was performed with Games-Howell post hoc analysis. SCI athletes and non-athletes were compared using parametric (i.e., independent samples t-tests) or non-parametric comparisons (i.e., related-samples Wilcoxon signed rank test, independent-samples Mann-Whitney U test). SCI and able-bodied individuals were compared using parametric (i.e., independent-samples t-tests) or nonparametric comparisons (i.e., related-samples Wilcoxon signed rank test, independent-samples Mann-Whitney U-test). A multiple regression analysis was completed with PCA phase and peak decline in SBP as the independent variables and NVC as the dependent variable. Significance was set a priori at p < 0.05.
Results
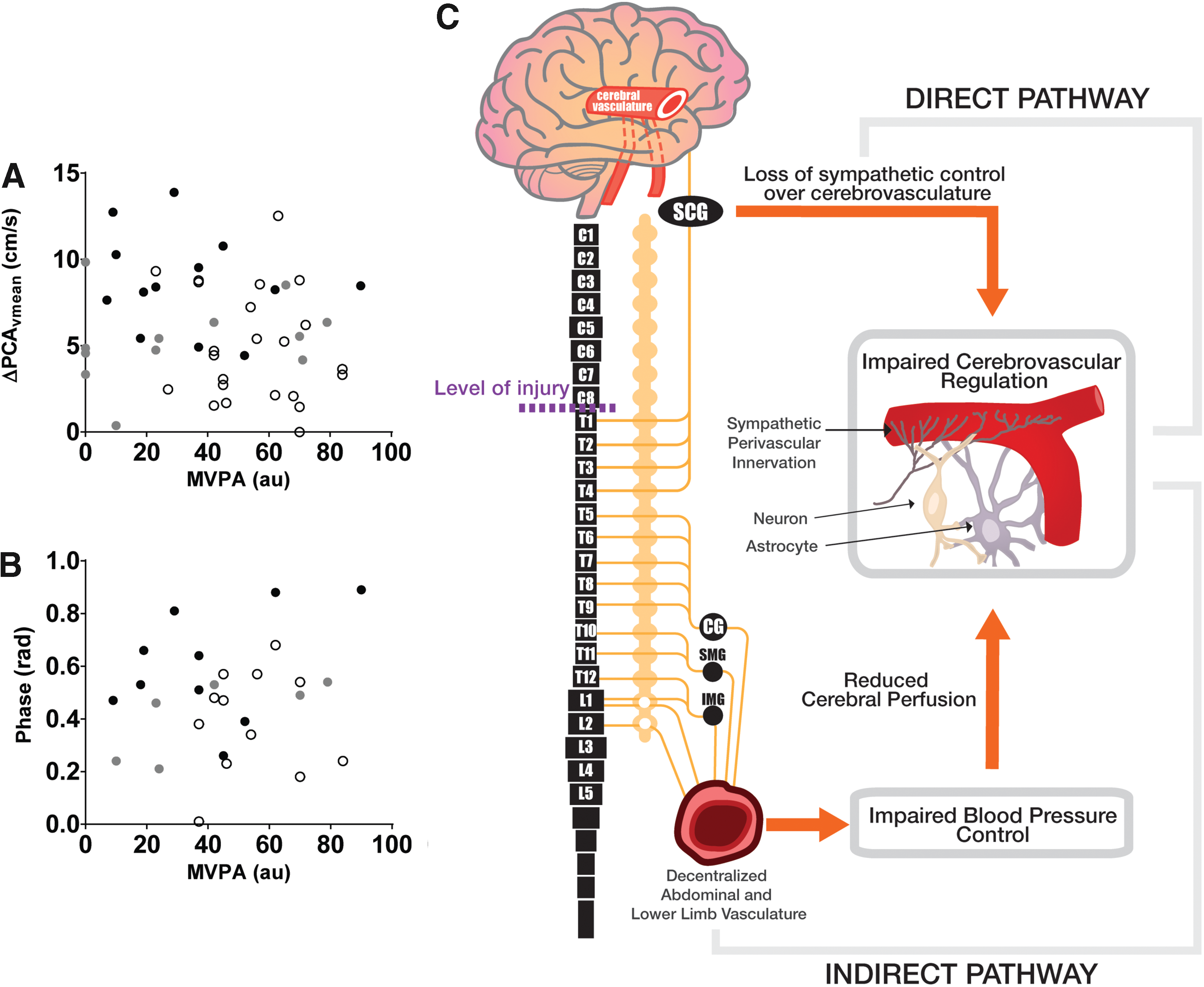
By design, SCI athletes participated in almost 2-fold more moderate-to-vigorous physical activity compared to SCI non-athletes, who were similar to able-bodied controls (Table 1). Resting BP and PCA blood flow was reduced in both SCI groups, compared with able-bodied individuals but not different between athlete and non-athlete SCI, while MCA flow was similar between all groups (Table 1). Both NVC and cerebral pressure-flow regulation were similar between SCI athletes and non-athletes (Fig. 1 and Fig. 2; Table 2). Impaired NVC (i.e., smaller PCA flow increases when eyes open) was apparent in both SCI groups, compared with able-bodied (Fig. 1A). Indicative of impairment in cerebral pressure-flow regulation, low-frequency transfer function phase was lower in both SCI groups, compared with able-bodied (Fig. 1D). No metrics of NVC or cerebral pressure-flow regulation were related to moderate-to-vigorous physical activity (Fig. 2). The severity of autonomic dysfunction (i.e., Δdecrease in SBP in seated position) was related to reduced NVC (Fig. 1B) and phase (Fig. 1E). Stroop performance (P3-P2 time) was impaired in SCI versus able-bodied (34 ± 2 sec vs. 26 ± 3 sec; p = 0.02); however, the ANOVA interaction was not significant (p = 0.08; Table 1). Reduced NVC was related to poorer Stroop performance (Fig. 1C). Cerebral pressure-flow regulation (PCA phase) and autonomic dysfunction severity predicted 30% of the variability in NVC (multiple regression; R2 = 0.3; p = 0.005).
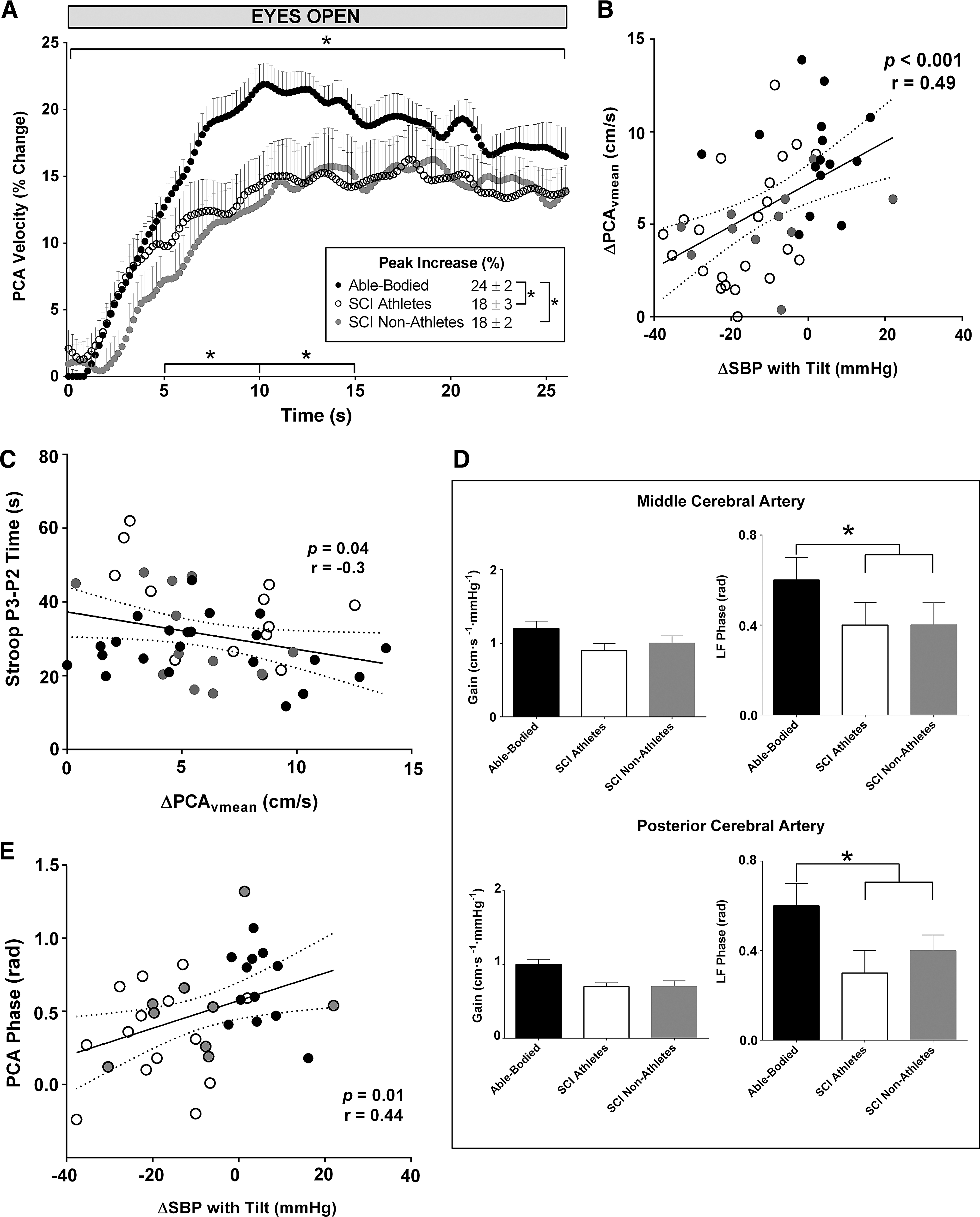
Neurovascular coupling was significantly impaired in both spinal cord injury (SCI) athletes (n = 23) and non-athletes (n = 12), compared with able-bodies (n = 13;
Neither neurovascular coupling
Denotes significantly different from able-bodied (p < 0.05).
Denotes significantly different from SCI athletes (p < 0.05).
SCI, spinal cord injury; ANOVA, analysis of variance; BMI, body mass index; MVPA, moderate-to-vigorous physical activity; TBI, traumatic brain injury; SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; MCA, middle cerebral artery; vmean, mean flow velocity; cvc, cerebrovascular conductance; PCA, posterior cerebral artery.
Denotes a significant interaction between groups (p < 0.05).
Denotes significant different from AB group (p < 0.05).
denotes trend of significant difference from AB group (p = 0.06). Both MCA and PCA consistent showed a significant group interaction of phase, where those with SCI had reduced phase lag between MAP and cerebral blood flow indicating impaired cerebral blood flow regulation. SCI athletes and non-athletes were not different between groups for any metrics.
SCI, spinal cord injury; MAP, mean arterial pressure; MCA, middle cerebral artery; n-gain, normalized gain; PCA, posterior cerebral artery.
Discussion
This study represents the largest assessment of cerebrovascular health after SCI to date, and is the first to evaluate the putative role physical activity plays in cerebrovascular and cognitive impairment after SCI. The major findings are: 1) significant cerebrovascular dysfunction occurs after SCI, demonstrated by cerebral hypoperfusion, as well as impaired NVC and cerebral blood flow regulation; and 2) cerebrovascular dysfunction was related to the degree of autonomic dysfunction but not routine physical activity levels. These findings highlight at least two critical clinical issues: 1) standard recommendations of increasing upper-body exercise after SCI may not be sufficient to improve cerebrovascular and cognitive function, and new exercise modalities must be explored, and 2) autonomic dysfunction needs to be considered a primary factor in cerebrovascular and cognitive impairment after SCI. Disruption of descending sympathetic pathways after SCI may impair NVC and cerebral pressure-flow regulation (i.e., phase lag) both directly and indirectly. 1 Directly, the loss of sympathetic control over the cerebrovasculature can impact cerebrovascular regulation (as sympathetic influences do directly affect cerebrovascular tone), 10,11 while indirectly, reduced cerebral perfusion pressure due to hypotension (that results from loss of sympathetic control over systemic vasculature) 1 also reduces the capacity for cerebrovascular function 2,22 (See Fig. 2C for further explanation). Further, roughly one third of the NVC response was predicted by autonomic dysfunction and pressure-flow regulation (i.e., PCA phase), providing novel insight into the major factors/mechanisms underlying NVC in vivo, which is considerably divergent from ex vivo models. 21 Some studies have reported normal MCA flow, while others have shown a reduction after SCI. 1 Small sample sizes (i.e., n < 10) in previous studies may explain these differences. For the first time, our findings clearly indicate that while MCA flow is preserved, there is selective reduction in posterior cerebral perfusion (as indicated by reduced PCA flow) after SCI. It is known that cerebral hypoperfusion contributes to white matter damage, 23 and hypoperfusion of the brainstem (where autonomic control centers and regions for consciousness are located) likely underlies the high incidence of presyncope/syncope in this population. 1 These data, and our work demonstrating posterior reversible encephalopathy syndrome after SCI, illustrate susceptibility of posterior cerebrovasculature to hyperperfusion and hypoperfusion. 24
Footnotes
Acknowledgments
This project was funded by the Craig H. Neilsen Foundation, Canadian Institutes of Health Research, Michael Smith Foundation for Health Research, Heart and Stroke Foundation of Canada.
Author Disclosure Statement
No competing financial interests exist.