
Abstract
Recovery from concussion in childhood is poorly understood, despite its importance in decisions regarding return to normal activity. Resolution of post-concussive symptoms (PCS) is widely employed as a marker of recovery in clinical practice; however, it is unclear whether subtle impairments persist only to re-emerge in the context of increased physical or cognitive demands. This study aimed to examine the effect of strenuous exercise on clinical symptom report and neurocognition in children and adolescents after PCS resolution after concussion. We recruited children and adolescents with concussion (n = 30) on presentation to an Emergency Department (ED). At Day 2 and Day 10 post–self-reported symptom resolution, participants completed a strenuous exercise protocol, and pre- and post-exercise assessment of PCS and neurocognition. Results demonstrated an overall reduction in PCS from Day 2 to Day 10 post-symptom resolution, with no evidence of symptom increase after strenuous exercise at either time point. Neurocognitive performance was linked to task complexity: on less cognitively demanding tasks, processing speed was slower post-exercise and, unexpectedly, slower on Day 10 than Day 2, while for more demanding tasks (new learning), Day 2 exercise resulted in faster responses, but Day 10 processing speed post-exercise was slower. In summary, we found the expected recovery pattern for PCS, regardless of exercise, while for neurocognition, recovery was dependent on the degree of cognitive demand, and there was an unexpected reduction in performance from Day 2 to Day 10. Findings provide some suggestion that premature return to normal activities (e.g., school) may slow neurocognitive recovery.
Introduction
M
While evidence is scarce, there are several consensus driven return-to-play (RTP) concussion guidelines for athletes, primarily adult-based, which recommend that post-concussive symptoms (PCS) are monitored, that the athlete is asymptomatic at rest before beginning to return to normal activities, and that a gradual return to play process is undertaken. 5 –9 These guidelines are derived from findings that premature return to active sport participation, before full symptom resolution, presents an increased risk of further injury and the potential for worse outcomes. 10
In child and adolescent concussion, there is evidence that recovery may be more protracted than the 7–10 days often quoted for adults. 11,12 If so, there are important implications for post-concussion management in these younger age groups, because current guidelines, informed primarily by adult recovery patterns, may lead to early return to normal activities and thus increased risk of further injury.
One means of reducing risk of premature return to normal activities is to base decisions on reliable measurement tools, rather than subjective clinical opinions. There are various methods for assessing PCS, including: (1) traditional severity indices (e.g., Glasgow Coma Score [GCS] 13 ), with limited sensitivity to concussive injuries; (2) sidelines tools (e.g., Sports Concussion Assessment Tool [SCAT], 8 which tap into orientation, attention, memory, balance, and co-ordination; (3) self- and parent-report questionnaires, rating presence and severity of symptoms (e.g., Health and Behavior Inventory, 14 Post-Concussion Symptom Index 15 ), which may not account for pre-existing symptoms, common in the general population 16 ; and (4) standard neuropsychological assessment tools, which can be both long and costly, and are often insensitive to change. 17 –19
Recently, research has explored the potential for controlled exercise to contribute to decisions regarding return to play and to quicker recovery. 20 –22 In the normal population, and in physically fit individuals, exercise has been shown to improve neurocognitive function, including reaction times (RTs). 23 In contrast, within the concussion literature, several adult studies have explored whether such activity post-concussion may actually unmask ongoing symptoms not evident on self-report or neurocognitive testing. 12,21,22 Preliminary findings suggest that post-concussion, asymptomatic adults exposed to intense physical and cognitive exertion show increases in PCS and processing speed, and subtle memory deficits. 12,21,22 Majerske and associates 12 have extended these findings, showing that athletes who engaged in intense activity demonstrated increased symptoms post-exercise. In contrast, moderate level exercise (i.e., school activity, slow jogging, or domestic chores) resulted in no such drop in performance. Others have reported that introduction of light exercise early in recovery may accelerate return to pre-concussion function. 21,23 –26
Given these conflicting findings and population findings that exercise improves neurocognition, we set out to examine the effect of strenuous exercise in children and adolescents with a recent concussive injury. We were particularly interested to identify whether strenuous exercise results in the re-emergence of previously resolved PCS or unmasks persisting neurocognitive inefficiencies, and thus may assist in more accurately determining full recovery and guide safe return to normal activity. No previous research has examined these relationships in children and adolescents, despite the high frequency of concussive injuries and the reported delayed recovery trajectories in these younger age groups.
Using a standardized exercise regimen, with a test-re-test design, we assessed a sample of children and adolescents with concussion recruited on presentation to an Emergency Department (ED) and explored the effect of exercise on PCS and neurocognition once PCS had resolved. Specifically, we examined the impact of exercise on PCS and neurocognition at two time points—Days 2 and 10 post-symptom resolution. We predicted that, following self-reported PCS resolution: (1) exercise would result in increased PCS and reduced neurocognition; and (2) these effects would decrease from Day 2 to Day 10 post-symptom resolution.
Patients and Methods
Design
This study employed an experimental, repeated measures (test-exercise-test) design with three time points: Day 0, presentation to The Royal Children's Hospital (RCH) ED; Day 2, two days after self-reported full symptom resolution; Day 10, 10 days after self-reported full symptom resolution.
Participants
The study comprised 30 children and adolescents (25 males), aged between 10.0 to 17.1 years, presenting to the RCH ED, Melbourne, within 24 h of sustaining a concussive injury. The study investigator (VM) identified ED presentations with concussion through surveillance of the electronic visits database of the RCH ED. Eligibility was then verified with the treating clinician, before the research team approached the patient and family regarding the study.
Consistent with the Zurich Consensus statement, 8 concussion was defined as a blunt injury to the head associated with an altered mental state or any of the following symptoms: headache, dizziness, fatigue, drowsiness, nausea/vomiting, poor balance, memory or concentration problems. Participants were included if they presented with: (1) loss or altered consciousness; (2) post-impact confusion and disorientation; and (3) two or more acute concussion symptoms including headache, dizziness, gait unsteadiness, and blurred vision. These symptoms were assessed by ED staff as part of routine clinical assessment and management. Exclusion criteria were: intubated patients, need for neurosurgical operative intervention or general anesthesia for injury management, presence of structural/hemorrhagic intracranial injury on computed tomography (CT) scan, clinical evidence of cerebrospinal fluid leak, injury resulting from child abuse or assault, alcohol or drug intoxication at time of ED presentation, multiple trauma, GCS 13 below 13, pre-existing physical, neurological, or psychiatric disorder.
Once eligibility was confirmed, the researcher then approached potential participants and their families in the ED and provided detailed information on the study protocol. Of the 48 young persons approached, 30 agreed to participate (62.5% recruitment). Reasons for refusal included family time commitments, residing at a distance from the RCH, and lack of interest. Of those who agreed to participate, all completed all study requirements.
Measures
A. Screening and demographic information
Screening questionnaire
The young person (or parent) completed a questionnaire in the ED to determine study eligibility. Information collected included participant age, post-concussion symptoms, English proficiency, demographic characteristics, and developmental history.
Injury characteristics
GCS, injury details, and clinical symptoms were extracted from medical histories.
Sample descriptors: Intellectual ability (Day 10)
The Wechsler Abbreviated Scale of Intelligence (WASI), 27 two-subtest form provided a Full-Scale Intelligence Quotient (IQ) score estimate (M = 100, standard deviation [SD] = 15).
Everyday Executive Function (Day 10)
The Behavior Rating Inventory of Executive Function–Parent Form (BRIEF) 28 consists of 86 items and provided an overall score, the Global Executive Composite (GEC) (M = 50, SD = 10). A score of >60 is indicative of clinical level executive problems.
Quality of life (Days 0 and 10)
The Children's Health Questionnaire–Parent Form (CHQ) 29 was administered at Day 0 to determine any pre-injury health or psychosocial problems.
B. Outcome measures (pre-post exercise)
CogSport. 30 , 31
This is a computerized tool, commonly used to assess PCS and cognitive function post-concussion. The symptom scale (CogSport SS) comprises 24 items describing common PCS (e.g., headache), scored on a seven-point Likert scale from 0 (none) to six (severe) and divided into symptom clusters: arousal, somatic, cognitive, emotional, and sleep dysregulation. Based on International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) criteria, symptom resolution is defined as endorsement of ≤3 PCS with less than moderate intensity (rating 0–2). Participants completed the CogSport SS in the ED and then immediately before and after completing the exercise protocol on Days 2 and 10.
CogSport also includes a computerized assessment tool, commonly used to examine multiple aspects of information processing and new learning. Four CogSport subtests were administered in this study: (1) detection (DET): simple RT/processing speed; (2) identification (ID): simple decision-making; (3) One Back (OB): working memory; and (4) One Card Learning (OCL): learning/memory. After an initial practice session on Day 2, to control for practice effects, CogSport was completed immediately before and after the exercise protocol on Days 2 and 10. Each administration took approximately 8 min. The RT scores were used in analyses.
C. Exercise protocol
Participants completed an adapted version of the McMaster All-Out Progressive Continuous Cycling Test, 32 which has been shown to be suitable for children. The protocol required participants to exercise at a submaximal level for 8 min. During this assessment, heart rate was monitored on a portable device (Polar FS1 Heart Rate Monitor–Model: 7258822716).
Warm-up
The protocol began with a 2 min warm up on a stationary exercise bicycle. In stages 1–3 (submaximal exercise routine) after the 2-min warm-up, the bicycle's resistance level was increased by 25 or 50 W, based on participant height (Table 1). Participants were instructed to keep rotations per minute constant. Throughout a 6-min exercise period, the researcher monitored participants' heart rate every 2 min, and participants were asked to rate their level of exertion using the Children's Effort Rating Scale (CERS), 32 which has a 10 point scale where 1 = very, very easy and 10 is so hard I'm going to stop.
Procedure
This study was approved by the RCH Human Research Ethics Committee. Participants were initially identified via ED database surveillance and approached, in the RCH ED, by the primary researcher (VM), at which time the project was explained in detail. Consenting participants/parents completed a screening questionnaire while under observation in the ED (Day 0). In the following days, the research team made phone contact with participants each morning until they reported being asymptomatic at rest. Once two consecutive asymptomatic days had passed (Day 2), participants then attended morning appointments at an outpatient clinic and again eight days later (Day 10).
On presenting to the exercise laboratory on Day 2 and Day 10, participants completed the CogSport SS and CogSport, followed by the exercise protocol and a second administration of the CogSport SS and CogSport (Fig. 1). Testing was completed within 45 min in total.
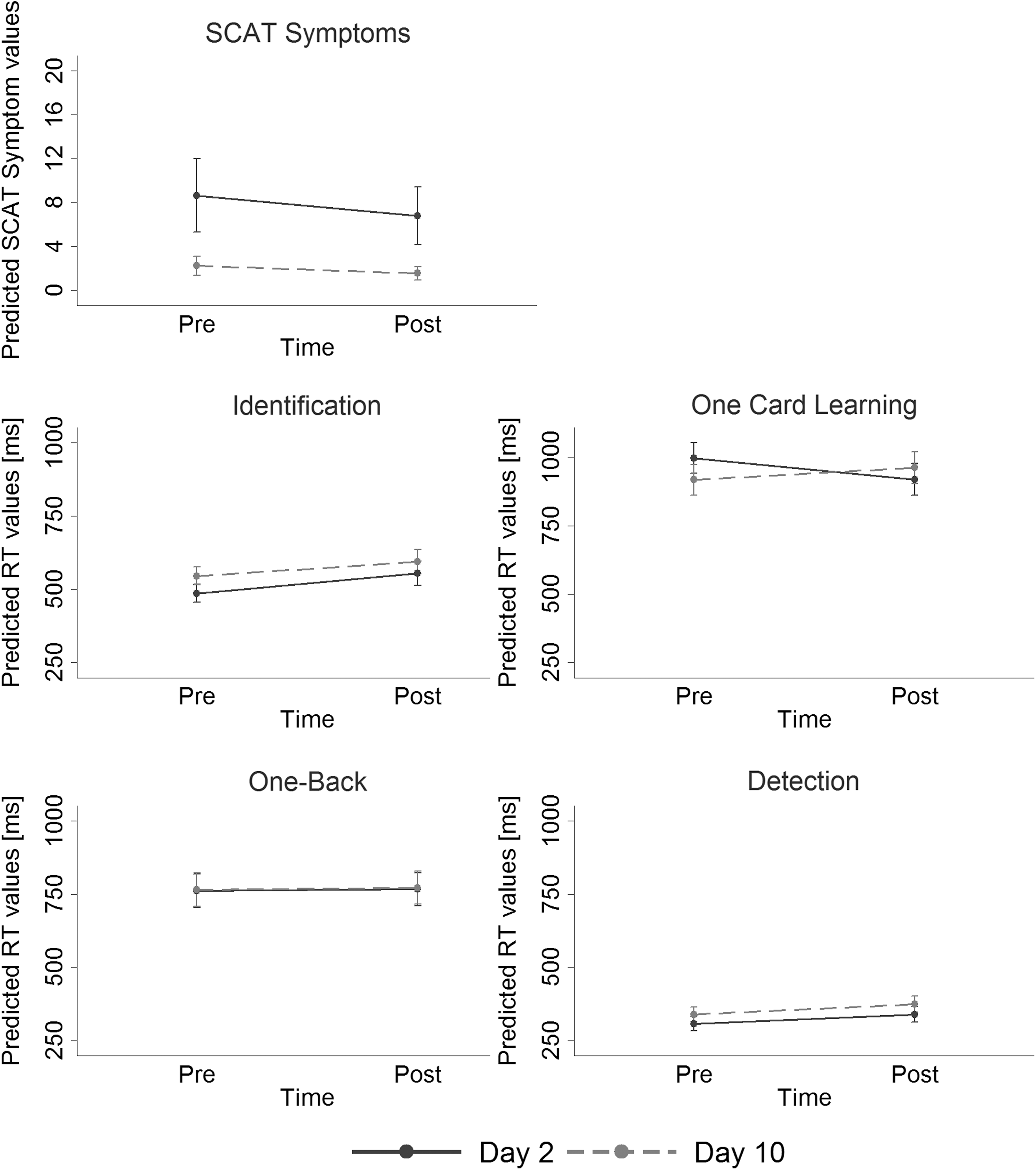
Linear Mixed Model estimates on Day 2 and Day 10 post-concussion pre- and post-exercise of (1) Sports Concussion Assessment Tool (SCAT) severity; (2) CogSport reaction times (RT) for detection, identification, One Card Learning, and One Back.
Statistical analysis
Summary statistics were initially calculated for demographic and injury-related variables. Repeated mixed models were then conducted to examine the effects of pre-/post-exercise and days post-concussion (measured at Days 2 and 10), and the interaction of these two variables on the CogSport four subtasks. Because of its distribution (heavy positive skew), CogSport SS data were modeled using a Poisson repeated mixed model. Repeated observations were clustered on the individual random variable, and day post-concussion was entered as a random slope.
Estimated model RT means were plotted to illustrate the effect of pre-/post-exercise at Days 2 and 10. The RT is often (log10) transformed to better satisfy the assumption of normality. 33 For these data, however, a sensitivity analysis between log10 and raw RT models did not yield differing results, model fit was not improved, and there was no noteworthy change to regression diagnostics. As such, raw RT outcomes were modeled and presented to aid estimate interpretation. Model effect sizes (Cohen f2) were also reported, with 0.10 representing a small, 0.25 a medium, and 0.40 a large effect size. 34
All analyses were conducted using Stata SE v14.0, and employed a significance level of α = 0.05.
Results
Demographic and medical characteristics
Participants comprised 25 males and five females, with a mean age at injury of 14.0 years (SD = 2.1, range: 10.1–17.7 years). Concussions were primarily as a result of sporting injuries (n = 27, 90.0%), and seven (23.3%) participants reported a history of previous concussion. No participant presented with abnormal neurological signs, 28 reported normal early development, and 6 (20%) noted school/learning problems (Table 2).
SD, standard deviation; CHQ, Child Health Questionnaire; PCS, post-concussive symptoms; SS, symptom scale; IQ, intelligence quotient; WASI, Wechsler Abbreviated Scale of Intelligence; BRIEF, Behavioral Rating Inventory of Executive Function; GEC, Global Executive Composite.
Days to resolution of post-concussive symptoms varied across the sample (M = 5.4 days, SD = 4.3, range = 0–24 days). On presentation at Day 2 post-symptom resolution, CogSport SS scores for the group had a mean of 7.7 (SD = 8.1) and a range of 0–43.
The IQ scores were within the average range for all participants (M = 107.1, SD = 14.2) as were everyday executive skills (BRIEF GEC: M = 52.5, SD = 10.1) and pre-injury quality of life: CHQ physical (M = 46.5, SD = 8.9) and psychosocial (M = 54.6, SD = 8.2).
Post-concussive symptoms
CogSport SS
Results for the CogSport SS are provided in Table 3. Overall, a significant model was found for PCS on the CogSport SS, Wald χ2(3) = 131.55, p < 0.001, Cohen f2 = 0.33. This appeared to be driven by a significant main effect of time from post-symptom resolution (Day 2 vs. 10) (Poisson beta coefficient [βP] = −1.03, p < 0.001). No significant effect of exercise (βP = −0.31, p = 0.06), or interaction effect (βP = −0.17, p = 0.39) was found (Fig. 1).
M, mean; SD, standard deviation; SS, CogSport Symptom Scale (mean symptoms); DET, detection; ID, identification: OCL, One Card Learning; OB; One Back; COMP, Composite Score (all in milliseconds).
+ <0.05, *< 0.01, ** <0.001,
Time effect (Day 2 vs Day 10); bexercise effect (pre- vs. post-exercise); cinteraction (time × exercise).
Neurocognitive performance. (Results for the CogSport measures are provided in Table 3)
Detection
A significant model was found for Detection RT, Wald χ2(3) = 45.97, p < 0.001, f2 = 0.43. Both exercise and time effects were significant. Effects of exercise indicated that participants performed worse after completing the exercise routine (unstandardized beta coefficient [β] = 31.45, p = 0.001). For time post-symptoms, there was a decline in performance from Day 2 to 10; that is, increased RTs (β = 31.53, p = 0.001). A non-significant interaction term (β = 2.90, p = 0.82) suggested parallel lines of change between the two observation days (Fig. 1).
Identification
A similar pattern was found in Identification RT as was seen in Detection (Fig. 4). Overall, the model was significant, Wald χ2(3) = 45.97, p < 0.001, and significant main effects for exercise (β = 68.90, p < 0.001), and time-post symptoms (β = 59.10, p < 0.001). Again, the interaction was not significant (β = −20.10, p = 0.32).
One-Back
No significant main effect of exercise (β = 5.47, p = 0.82), or time post-symptoms (β = 4.45, p = 0.86), was found (Fig. 1). There was no observed interaction effect (β = 0.55, p = 0.99), and the overall model was not significant (Wald χ2(3) = 0.18, p = 0.98, f2 = 0.002).
One Card Learning
For One Card Learning, all terms were significant (model Wald χ2(3) = 8.56, p = 0.04): exercise β = −78.00, p = 0.02; time-post symptoms β = −79.07, p = 0.01; and interaction effect β = 121.87, p = 0.01. There was a decrease in RT from pre- to post-exercise on Day 2, but an increase in RT from pre- to post-Exercise on Day 10 (Fig. 1).
Effort ratings
Participant effort ratings suggest that the routine was challenging, with Children's Effort Rating Scale scores at Level 3, “getting quite hard” (mean = 5.57, median 6) at Day 2 and “starting to get hard” (mean = 4.97, Median = 5) at Day 10.
Discussion
The aim of this study was to examine the effect of exercise on PCS and neurocognitive function in children and adolescents with a recent concussive injury to determine whether additional stress post-symptom resolution could result in re-emergence of symptoms. Specifically, we investigated whether strenuous exercise precipitated recurrence of PCS and neurocognitive impairment in the 10 days after self-report of symptom resolution.
PCS
Despite participants reporting resolution of PCS for two days before testing, on formal measures of PCS they continued to rate themselves as experiencing symptoms on symptom inventories at rates higher than those reported in healthy samples. 16 Consistent with previous literature, 1,14,17 however, we did identify a significant reduction in PCS from Day 2 to Day 10, supporting the presence of subtle ongoing recovery. In contrast, the predicted re-emergence of self-reported PCS post-exercise was not evident on either Day 2 or Day 10. Rather, we found a small, non-significant decrease in PCS after exercise.
Neurocognition
For neurocognitive measures, Figure 1 and Table 3 illustrate the expected relationship between RTs and task complexity, with RTs shorter for less cognitively demanding tasks (Detection, Identification) compared with more demanding tasks (One Back, One Card Learning). Further, on both Detection (simple RT) and Identification (simple decision making), the predicted slower responses were found post-exercise at both Days two and 10 post-symptom resolution. Contrary to what we would expect in terms of recovery, RTs were also slower at Day 10 than Day 2. On One Card Learning (memory/learning), a more cognitively demanding task, exercise differentially impacted performance, depending on time post-symptom resolution. Contrary to expectations, slowest RTs were recorded pre-exercise on Day 2 with better performance post-exercise, and somewhat surprisingly, at Day 10 RTs post-exercise were slower than those recorded pre-exercise, and slower than those for Day 2.
Our overall finding, that while exercise did not impact PCS, it had a significant negative impact on more simple neurocognitive functions (simple decision making, RTs) at both Day 2 and Day 10, is in contrast to research with healthy persons, which suggests that exercise has a positive effect on processing speed 16 and increases the ability to inhibit responses and reduce the time required to make decisions.35 Rather, our findings suggest that, in the presence of a concussive injury, this normal response is not evident. Further, the continued decline in post-exercise neurocognitive performance (but not PCS) at Day 10 was unexpected. Interestingly, similar results have also been reported in other studies of child and adolescent concussion. 17
One explanation for these unexpected findings is that reduced neurocognitive performance is related to return to school and other normal activities. While no participant in our study had returned to school at Day 2 assessment, most were involved in regular pre-injury school and normal routines by Day 10 testing (n = 28, 93%), arguably before full recovery, which may have led to an increase in physical and mental fatigue and thus poorer test performances. This suggests that, for children and adolescents, self-reported resolution of PCS may not be an accurate index of full recovery, and neurocognitive inefficiencies may persist. This has important implications for return to cognitively demanding activities, such as school. To facilitate full neurocognitive recovery, a longer recovery period may be beneficial.
Results from our study must be considered in the context of some methodological limitations. While we report unique longitudinal data, which incorporated an experimental design, the study sample was relatively small. Despite this, large effect sizes were found. With respect to generalizability of results, mean time to symptom resolution is less than has been reported in the previous literature, although more in keeping with recent ED-recruited samples than those reporting on patients attending follow-up clinics. We do note that follow-up demonstrated that mean group IQs were within the normal range, as were parent ratings of executive abilities and quality of life.
Primary outcome measures were limited to self-reported clinical symptoms and computer-based testing of neurocognitive skills, and may not be sufficiently sensitive to detect functional difficulties. The subjectivity of self-report of clinical symptoms and whether they accurately represent PCS is a common issue in concussion research. Further, the recommended cut-off for symptom resolution (that is ≤3PCS, ICD-10), while supported by population studies, 16 is yet to be validated against robust outcome measures, and so may incorrectly classify some concussed persons. Finally, the exercise protocol used a submaximal exercise routine, and it may be that more strenuous exercise is necessary to illicit neurocognitive and clinical symptoms. Participant ratings, however, indicate that the routine was challenging, with Children's Effort Rating Scale scores for Level 3 of “getting quite hard” at Day 2 and “starting to get hard” at Day 10.
Conclusions
Study results suggest different recovery trajectories for PCS and neurocognition after child and adolescent concussion. PCS appeared unaffected by exercise and demonstrated the expected reduction in symptoms with time post-injury. In contrast, neurocognitive function was more susceptible to strenuous exercise and, contrary to our predictions, poorer neurocognitive performances were recorded at Day 10, when most participants had returned to normal activities. Our results provide preliminary evidence that subtle neurocognitive impairments may be present even once PCS have resolved, and support the need for ongoing monitoring in the weeks after symptom resolution.
Footnotes
Acknowledgments
This study was supported by the Victorian Government Operational Infrastructure grant to the Murdoch Childrens Research Institute. Dr. Anderson is supported by an NHMRC Senior Practitioner Fellowship. Dr. Babl is part funded by a grant from the Royal Children's Hospital Foundation.
Author Disclosure Statement
No competing financial interests exist.