
Abstract
The aim of this study was to provide accurate estimates and characterizations of children with spinal cord injuries (SCIs) and for the subset that are appropriate for inclusion in clinical trials. We identified children <18 years of age with SCI International Classifications of Diseases, Ninth Revision, Clinical Modification Codes (ICD-9-CM codes) from the 2006, 2009, and 2012 Kids' Inpatient Database. We excluded those with late effects, transfers to other hospitals, unspecified injury levels, and hospital stays <48 h. We then used conventional rationale to identify children who were eligible for SCI clinical trials. Over 3 years, 2484 children had SCI ICD-9-CM codes; 1342 had coding consistent with true SCI and 706 satisfied clinical trial inclusion criteria, yielding national estimates of 2013 and 1062, respectively. Of children with clinical trial eligible SCI, injuries were more common in the cervical region (66.1%), males (65.5%), older children (51.1% were 16–17 years old), and the South (49.8%). The majority were treated at urban teaching hospitals (84.6%); however, only 20.3% were treated at pediatric-specific centers. Of the 445 sample hospitals treating children with SCI, 66.3% treated just 1 child in the 3-year period. Children eligible for SCI clinical trials represented less than one third of children with SCI ICD-9-CM codes. These children were regionally localized to the South, with few receiving treatment at pediatric-specific centers or centers that frequently care for children with SCI. These findings highlight the importance of carefully assessing the national distribution of children with SCI, so that resources are appropriately allocated to optimize clinical care and research outcomes.
Introduction
S
There have been numerous studies characterizing the population of children with SCI using registries from individual trauma centers and national databases. 2,8 –13 These studies have provided important epidemiological information; however, to date, no study has characterized those children that would feasibly be eligible for clinical trials, a minority within the overall SCI population. Patients must fit within a stringent set of criteria to be eligible for a clinical trial; these criteria have previously been described for adult SCI patients. 14 An ideal SCI candidate for a phase 1 clinical trial possesses, in addition to other selection criteria, substantial neurological deficits from acute, blunt trauma to the spinal cord above the lumbar level, with attention to the presence of concomitant traumatic brain injury (TBI). 14 Previous pediatric SCI studies provide clinical trial investigators an unrealistic view of the demographic and geographical characteristics of their target population. A number of SCI trials have been terminated because of underenrollment, preventing investigators from determining the efficacy of interventional therapies in children. 15 –18 This is the first study to account for criteria relevant to pediatric SCI clinical trials. The specific aims of this study are to: 1) provide national estimates of the number of children eligible for SCI clinical trials; 2) describe the demographic and geographical distribution of these children in the United States; and 3) examine the implications of these findings for future clinical trial design. These findings hold important implications for both research and clinical care planning. The national distribution of children with true SCI should be carefully assessed so that resources are appropriately allocated to optimize research and clinical outcomes.
Methods
Data source
This project was considered exempt from review by our institutional review board (IRB). The data used in this study were obtained from a de-identified national public use data set, and, for this reason, it is not considered human subject research by our IRB. We analyzed the Kids' Inpatient Database (KID), the largest all-payer pediatric inpatient care database in the United States. The KID is part of the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality, which contains inpatient data from participating organizations across 48 states. The KID provides pediatric discharge data to allow health care usage to be tracked for patients 20 years of age or younger at the time of admission. The records include clinical and resource use information obtained through discharge abstracts, such as diagnosis codes, insurance type, and discharge status. The KID provides weights and sampling variables to generate national estimates. The data available in the KID were first collected in 1997 and is accessible for analysis every 3 years. Because of the rare nature of pediatric SCI, the 2006, 2009, and 2012 data sets were combined for this analysis.
The most recent 2006, 2009, and 2012 KID samples pediatric discharges from 3739, 4121, and 4179 hospitals, respectively, in the 48 states participating in the HCUP. The KID was chosen for this project because it has such a large stratified sample of inpatient discharges (over 3 million discharges representing more than 6.5 million nation-wide discharges), which allows researchers and policy makers to analyze hospital utilization, national trends, and the burden of uncommon conditions, such as SCI.
Patient selection
Patient inclusion parameters were based on previously described selection criteria for a SCI clinical trial. 14 We first captured all SCI in children <18 years of age with the following International Classification of Diseases, Ninth revision, Clinical Modification (ICD-9-CM) codes: fracture of the vertebral column with SCI (806.00–806.9) and SCI without evidence of spinal bone injury (952–952.9). To ensure capture of only acute events to the spinal cord, we excluded children who also had codes for late effects of SCI (905.1, 907.2). Because of the de-identified nature of the KID, a child transferred from one acute care facility to another would be listed as two separate admissions. Therefore, to avoid double counting patients, we excluded those with discharge dispositions of “transfer to other acute care facilities.” 13
We then identified children with true SCI by excluding those children with diagnostic coding and hospital lengths of stay that would be inconsistent with SCI. To ensure that all children had sustained neurological deficits attributable to an SCI, those with vertebral fractures limited to the lumbar, sacral, or coccyx regions (806.6 series, 806.7 series, and 806.4, 806.5) were excluded, because the spinal cord ends at the L1 level. Injuries sustained below this level represent cauda equina (952.4) and nerve root injuries, as opposed to true SCI. We also excluded children discharged in <48 h to somewhere other than a long-term facility, children without a discreet level of spinal cord injury (806.8, 806.9, 952, 952.0, 952.8, or 952.9), and those discharged home with a length of stay (LOS) <48 h. These children were unlikely to have sustained true SCI given that a level of injury was not assigned and children whose signs and symptoms were transient enough to allow discharge home within 48 h of injury.
After limiting the data set to children with evidence of a true SCI, children ineligible for a clinical trial were then excluded. Given that penetrating injuries (gunshot and knife wounds) have a pathophysiological process distinct from blunt trauma, children with penetrating injuries are typically excluded from clinical trials. Therefore, patients with only penetrating trauma codes were excluded, using ICD-9-CM External Cause of Injury codes (E-codes). Similarly, SCIs with open fractures (806.10–806.19, 806.30–806.39) were excluded. Codes for vertebral dislocations (839.0–839.5) were excluded, given that these injuries result in cord ischemia attributed to impingement of the vertebral arteries, as opposed to direct blunt trauma to the spinal cord. Children with cardiac arrest codes (427.5) were also excluded, given that cardiac arrest can cause neurological ischemia, resulting in an injury indistinguishable from blunt trauma SCI.
Vulnerable and unreliable patient populations were excluded: prisoners (312.9, V62.5); wards of the state (V61.29); child abuse victims (995.50–995.59; E967.0–E967.9); children with pregnancy codes (V22–V23, 640–649); children with codes for drug and/or alcohol abuse; and children with self-inflicted injuries. Children with mental illness diagnoses indicating a potential for spurious focal neurological findings were also excluded: conversion disorder (300.11); hypochondriasis (300.7); undifferentiated somatoform disorder (300.81, 300.82); and chronic factitious illness with physical symptoms (301.51).
Eligible children were then ranked according to the highest anatomical level of SCI based on their ICD-9-CM codes and separated into four groups: cervical injury without concurrent TBI; cervical injury with TBI; thoracic injury without TBI; and thoracic injury with TBI.
Statistical analysis
Patient demographics, geography, and hospital characteristics were analyzed, including: injury level, age, sex, race, mechanism of injury, residence, discharge status, payer information, region, hospital location, and hospital type (children's vs. nonchildren's, rural vs. urban nonteaching vs. urban teaching).
Children were separated into a 0- to 15-year-old age group and a 16- to 17-year-old age group, based on spinal maturation and the onset of driving at age 16, which marks a shift in the mechanism of injury in the pediatric population to motor vehicle accidents and a corresponding increase in the incidence of SCI. Data analyses were performed using SAS statistical software (version 9.3; SAS Institute Inc., Cary, NC).
All data were weighted to represent all U.S. pediatric SCI hospitalizations. The KID obtains discharge weights for national estimates using the American Hospital Association (AHA) universe of community, nonrehabilitation hospitals as the standard. 19 Hospitals are post-stratified by six characteristics: ownership/control; bed size; teaching status; rural/urban location; U.S. region; and a stratum for freestanding children's hospitals. Discharge weights are then created by stratum in proportion to the total number of non-newborn AHA discharges for non-newborn discharges and to the total number of AHA newborns for newborn discharges.
For patient demographic information and hospital information, we provide weighted estimates and percentages with 95% confidence intervals (CIs).
Results
Pediatric spinal cord injury population eligible for clinical trials
In the compiled sample data from the 2006, 2009, and 2012 KID, 2484 children had SCI codes (849 in 2006, 833 in 2009, and 802 in 2012; data not shown). Figure 1 shows the algorithm used to determine the sample of children with true SCI and those eligible for clinical trials. Transfers accounted for 8.6%, and a small portion had codes for late effects of SCI (1.0%). In the sample, 8.7% of children experienced isolated injuries to the lumbar, sacral, and/or coccyx spine or had cauda equina syndrome, and 13.9% had SCI codes without a specific level of injury. Another 13.8% of children were excluded because of an LOS ≤2 days without discharge to a long-term care facility. In total, 1342 children (54.0%) displayed evidence of a true SCI.
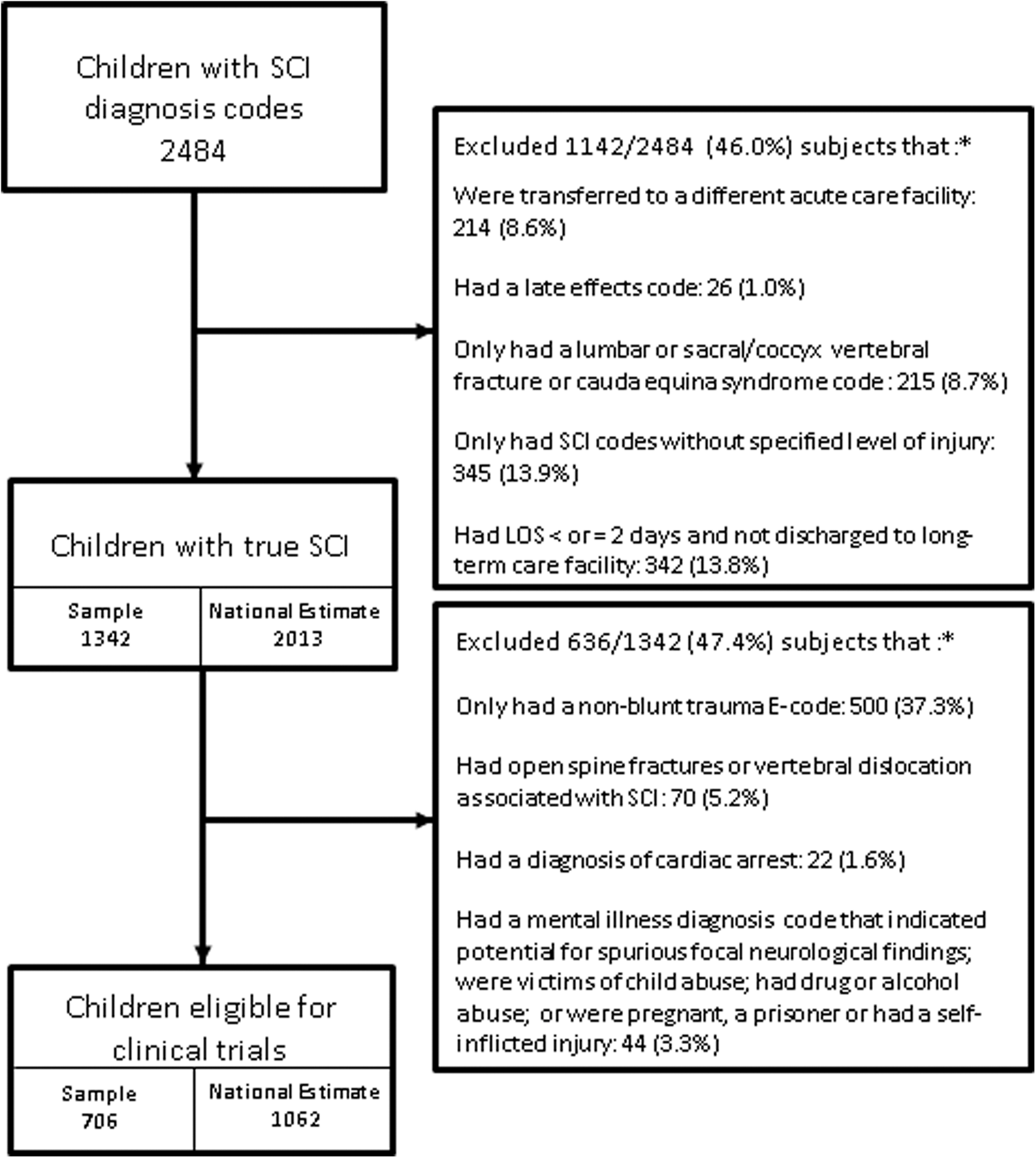
Reported patient counts for each exclusion criteria are based on the sample numbers rather than national estimates. KID, Kids' Inpatient Database; SCI, spinal cord injuries; LOS, length of stay; E-code, International Classifications of Diseases, Ninth Revision, Clinical Modification External Cause of Injury code.
From this remaining sample, 47.4% of the children (n = 636) were ineligible for a clinical trial. We excluded 5.2% with open spine fractures or vertebral dislocations. Another 37.3% of children with SCI had non-blunt-trauma E-codes only. Codes for cardiac arrest were present in 1.6% of children. Just over 3% of children with SCI were excluded as vulnerable or unreliable patients; three quarters of these had codes for drug and alcohol use. The other vulnerable/unreliable populations, including those with potentially spurious findings, had <10 children per category (mental health diagnoses, pregnancy, juvenile delinquency/wards of the state, and self-inflicted injuries).
After taking into account relevant criteria for a clinical trial, there were 706 children with SCI remaining in the sample data (243 in 2006, 248 in 2009, and 215 in 2012). The proportion of children with SCI eligible for a clinical trial was fairly consistent in each year: 28.6% of all pediatric SCI patients in 2006; 29.8% in 2009; and 26.8% in 2012. Sample weighting was applied to the 706 children in the sample data, generating a national estimate of 1062 (95% CI, 910–1174) children for the years 2006, 2009, and 2012.
Demographic characteristics
Table 1 shows the demographic, geographical, and hospital characteristics for the national estimates. The population of children with pediatric SCI eligible for clinical trial was generally comparable to the total pediatric SCI population in the KID. Key differences included a larger proportion of white children and a smaller proportion of black children in the clinical trial eligible population. The clinical trial eligible group also had fewer missing E-codes (3.7% vs.17.7%) and more motor vehicle and traffic-related accidents (53.6% vs. 34.3%). The clinical trial eligible pediatric SCI population had a larger percentage with private insurance (61.3% vs. 53.3%). Nearly half of all trial eligible SCIs were cervical SCI without TBI (48.5%; 95% CI, 44.7–52.2), whereas nearly one quarter of injuries were thoracic SCI without TBI (23.7%; 95% CI, 20.3–27.1). Cervical and thoracic SCIs with TBI were less common, with 17.6% (95% CI, 14.4–20.7) and 7.8% (95% CI: 5.8–9.8), respectively.
Because of missing data, the total number may not add up to the sample size.
Cells with KID reported data are not able to be reported if they are less than or equal to 10; therefore, values that fit these criteria are expressed as ≤10.
KID, Kids' Inpatient Database; SCIs, spinal cord injuries; TBI, traumatic brain injury; MVT, motor vehicle traffic; HMO, health maintenance organization; CI, confidence interval.
A large proportion of clinical trial eligible injuries were observed in a small age bracket: children 16–17 years of age (51.1%; 95% CI, 45.9–56.3). Majorities were also noted in males (65.5%) and whites (63.2%). Children eligible for SCI clinical trials primarily resided in metropolitan areas, with 43.3% of children in metropolitan areas with population ≥1 million. The most common cause of injury was motor vehicle traffic (MVT) crashes, representing 53.6% of all SCI clinical trial eligible cases. Falls represented 21.3% of SCI, including 5.7% related to diving.
Most (48.5%) of the children eligible for an SCI clinical trial were discharged to a skilled nursing facility, intermediate care, or other long-term care facility, and 42.8% were routinely discharged. In total, 2.9% of children died in the hospital. The majority of children had private insurance (61.3%).
Geographical characteristics
Nearly half of all children eligible for an SCI clinical trial were admitted to hospitals in the South (49.8%). A much smaller proportion (11.4%) was admitted to hospitals in the Northeast. Figure 2 shows the 2012 population rates of pediatric SCI across the census regions of the United States. Pediatric SCIs were more prevalent in the South (5.5 per 1,000,000 children) and West North Central regions (5.5 per 1,000,000) and less prevalent in New England (1.3 per 1,000,000 children).
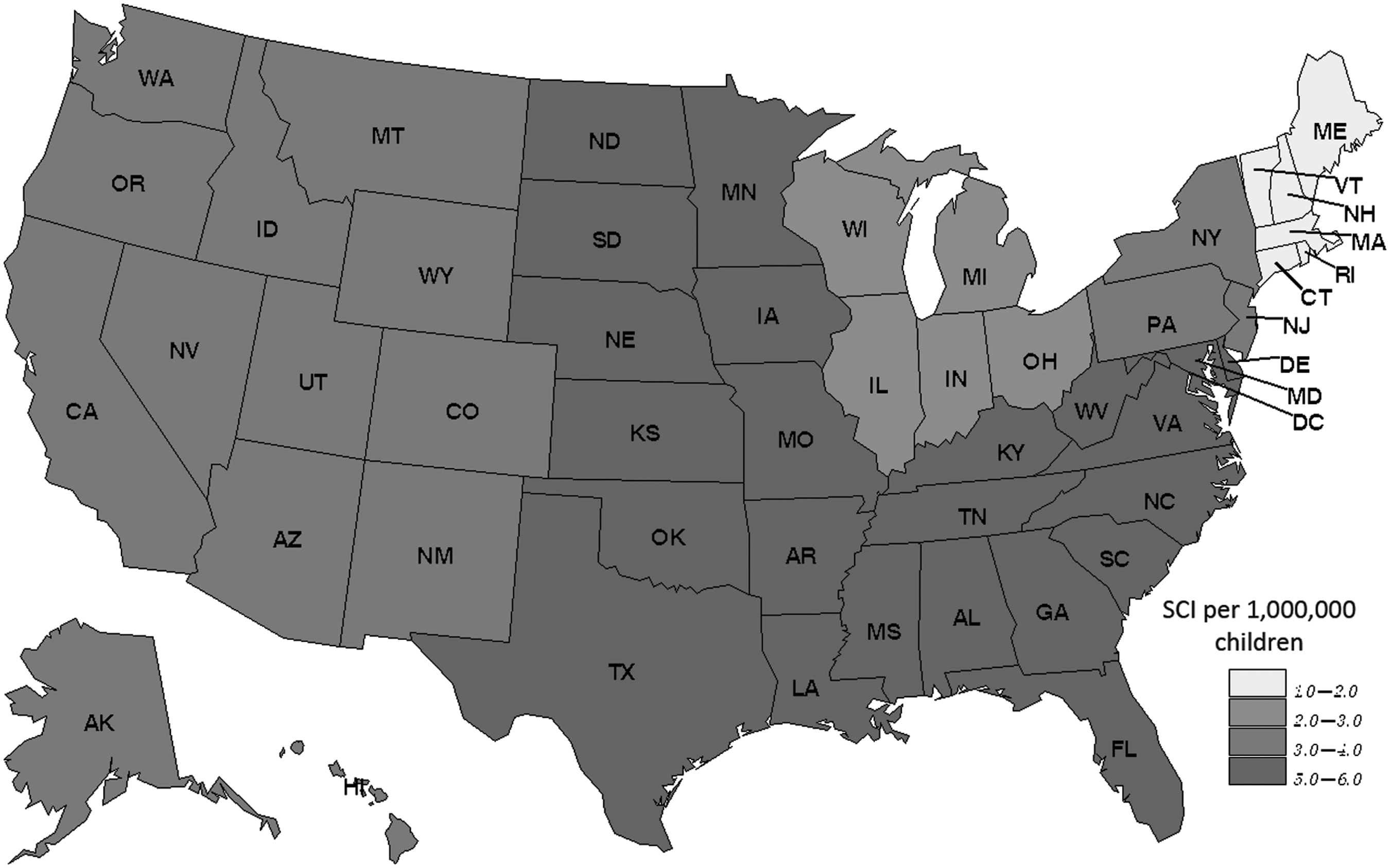
The Kids' Inpatient Database (KID) divides U.S. hospitals into nine divisions: New England; Middle Atlantic; East North Central; West North Central; South Atlantic; East South Central; West South Central; Mountain; or Pacific. Based on discharge weights provided by the KID, national estimates were calculated for the number of children with an SCI in each division. SCI, spinal cord injury.
Hospital characteristics
Most children eligible for an SCI clinical trial were treated in urban teaching hospitals (84.6%); however, just 20.3% were treated in children's hospitals (Table 1). Admission to children's hospitals decreased with increasing age; 30% of children ages 0–15 years were admitted to children's hospitals versus 8% of children ages 16–17 years (data not shown). Hospital volumes for children with clinical trial SCI are shown in Table 2 (sample hospitals only). Of the 445 hospitals treating pediatric SCI patients, the majority (n = 295; 66.3%) cared for only 1 child with trial eligible SCI over the 3 KID years.
For the 3 years of KID data, there are between 3739 and 4179 hospitals in the sample each year.
KID, Kids' Inpatient Database.
Discussion
In this study, we provide accurate estimates of children who were eligible for SCI clinical trials within the United States using 3 years of KID data. This clinical trial eligible population was approximately one third of all children with SCI ICD-9-CM codes and approximately one half of all children with presumed true SCI. The rare nature of pediatric SCI and the unique distribution of trial eligible children across the United States hold important implications for clinical trial design and regionalized SCI care.
Our study estimated that an average of 235 children would be eligible for SCI clinical trials per year. Previous epidemiology literature has reported SCI estimates of 1308 and 1455 pediatric SCI patients per year. 2,10 Patient characteristics, mechanism of injury, payer status, and hospital type reported here are consistent with findings from other studies using national data sets. A majority of SCI occurs at the cervical level with injuries increasing with age. 2,8,13 In our study, 51.1% of injuries in clinical trial eligible children occurred at 16–17 years of age. Selvarajah and colleagues showed a smaller majority in this age group (41.0%). 8 Similar to Piatt and colleagues, injuries were more commonly observed in white children, representing over half of the sample. 13 Pediatric patients with SCI were also more likely to be male, insured, and treated in an urban teaching hospital. The most frequent injury mechanism for those children that were clinical trial eligible was MVT crashes, accounting for over half of the clinical trial eligible national estimate.
In contrast to other studies, we found differences in the frequency of associated TBI and in the geographical distribution of children with SCI. Our study found only 25.4% of the clinical trial eligible pediatric SCI population suffered concurrent TBI, whereas Selvarajah and colleagues reported 86.0%. 8 Last, we found that 49.8% of children with SCI eligible for a clinical trial were from the South, a considerable majority over other regions, whereas previous studies reported that Southern children constituted one third of the samples, a negligible increase over other regions. 2,8,13
Differences between our study and other characterizations of pediatric SCI from national data sets are accounted for by our strict definition of true SCI and our clinical trial exclusion algorithm. Phase 1 clinical trials for SCI require isolated injuries to determine the true effects of a therapy. Therefore, nerve root and cauda equina injuries are typically ineligible, resulting in exclusion of injuries below the termination of the spinal cord (L1 level). 14,20,21 Previous studies have described injuries below the thoracic region, thereby including injuries without direct trauma to the spinal cord. Previous epidemiological studies have also failed to exclude children with injuries to an unspecified level of the spinal cord, though many of these children were discharged to home in <2 days or represented SCI without radiographic abnormality (SCIWORA) in our study. 2,3,8 –14,22,23 Children with SCIWORA codes have previously been shown to have no evidence of injury on magnetic resonance imaging, and these children frequently regain considerable neurologic function. 24 Consequently, these children do not have injuries severe enough for a clinical trial. It is difficult to determine true SCI cases from a national data set, so we chose to apply stringent exclusion criteria to remove children with less-severe injuries and spontaneous recovery. A merit of this study was the careful review of individual patients suspected to have ineligible injuries by a physician reviewer (J.C.L.). Our sample contains fewer children with TBI, given that many of these patients were likely excluded because of penetrating injury, cervical dislocation, and other exclusion criteria. Excluding etiologies such as penetrating injury may have contributed to differences between the clinically relevant and the general pediatric SCI populations, given that African American children, who are associated with a disproportionate number of gunshot wounds, were less prevalent in the group of children eligible for clinical trial. 21
The geographical distribution of children with clinical trial eligible SCI demonstrates the need to better understand this population in order to adequately plan clinical trials. Whereas nearly 60% of clinical trial eligible children were from the South and West North Central regions, these areas are under-represented in pediatric clinical trial networks, such as the Pediatric Emergency Care Applied Research Network, the Neurologic Emergency Treatment Trials, the Collaborative Pediatric Critical Care Research Network, and the Spinal Cord Injury Model Systems. 25 –28 Only 28% of centers participating in these research networks are located in the regions with the highest rates of pediatric SCI, given that most study sites are in the Northeast and East North Central regions. Thus, states with the lowest rates of pediatric SCI have the most representation in clinical trials and in databases created by these networks.
Similarly, a majority of children received treatment at nonchildren's hospitals, even though better outcomes are observed for children treated at children's hospitals and adult trauma centers with added resources for the care of children. 29,30 Most strikingly, only 445 hospitals treated children with trial eligible SCI, and a majority of those hospitals (66.3%) treated only 1 child with SCI over the 3-year KID period. Hospitals receiving so few pediatric SCI patients are likely to lack specialized resources for this population and may not be equipped to provide optimal care for debilitating injuries. Outcomes for children with SCI may be improved by regionalizing care to centers of excellence to not only ensure that these children receive optimal care, but to also generate sample sizes large enough to determine effective treatment guidelines. This may be crucial for children ages 16–17 years. This large population of children with SCI is treated in nonchildren's hospitals, making them inaccessible to pediatric clinical trial networks, while at the same time excluded from adult SCI trials. Few studies have investigated the benefit older children receive from treatment in children's hospitals. Pracht and colleagues found an additional reduction in mortality for children treated at pediatric designated trauma centers, as compared to centers without pediatric designation when children ages 16–19 years were included in their study sample. 31 McCarthy and colleagues noted the psychological benefits older children receive in a children's hospital. 32 Attributable to their overall healthy pre-morbid condition and their distinct needs when compared to adults, teenagers are likely to benefit from the more-extensive occupational therapy, physical therapy, art therapy, social interactions, and tutoring services provided at children's hospitals.
Several limitations exist in this study. By using an administrative data set, values such as the American Spinal Injury Association Impairment Scale, which grades patients for injury severity, could not be assessed, though they are important to clinical trial recruitment. 21 Because of this, and other exclusion criteria specific to an individual study, the values provided here still overestimate the true potential number of clinical trial eligible SCI patients. Differences in ICD-9-CM recording methods between different years and different hospitals may bias the information presented. Though transfers to acute care facilities were excluded, there is still the risk that children may have been double counted. Limiting the LOS to <48 h was an arbitrary cut-off point based on previous clinical trials for SCI, which used 48-h treatment regimens and with the assumption that it would take longer than 48 h to complete an evaluation and management plan for children with true SCI. A higher threshold LOS was not selected in order to avoid a spectrum bias that would be introduced by excluding children that have transient and self-limiting SCI, such as spinal cord concussion. Although we attempted to consider each patient individually, the de-identified nature of the KID prevents a true examination of each patient's chart, creating a risk for bias in the interpretation of injuries. The HCUP Data Use Agreement prevents reporting cell sizes ≤10.
Our study is the first to estimate the pediatric SCI population eligible for clinical trials in the United States by utilizing a stringent set of exclusion criteria to ensure that patients sustained true SCI with sufficient neurological deficit to warrant trial enrollment. We found that children eligible for SCI trials represented less than one third of all pediatric patients with SCI diagnostic codes. A majority of these children were treated in the South and West North Central areas, which are areas that are under-represented in clinical trial networks. Many children receive treatment in nonchildren's hospitals and in hospitals that treat few children with SCI per year, indicating they may lack sufficient institutional experience and resources. These findings hold important implications for future steps in clinical care and clinical trial planning.
Footnotes
Acknowledgments
Jaspreet Dhillon was awarded the Roessler Research Scholarship for $3,000 from The Ohio State University College of Medicine. This allows medical students to conduct medical research performed under the guidance of a faculty member of The Ohio State University College of Medicine (J.C.L). The purpose of this scholarship is to engage medical students in biomedical discovery and scholarly inquiry and to encourage students to consider a future academic career in biomedical research. A poster presentation was conducted at The Ohio State University College of Medicine Summer Scholars Research Symposium on October 2, 2015, and at the 2016 Pediatric Academic Societies Meeting, April 30–May 3, 2016.
Author Disclosure Statement
No competing financial interests exist.