
Abstract
The current study investigates whether repetitive subconcussive impacts cause changes in plasma S100β levels, and also tests the associations between S100β changes and frequency/magnitude of impacts sustained. This prospective study of 22 Division-I collegiate football players included baseline and pre-season practices (one helmet-only and four full-gear). Blood samples were obtained and assessed for S100β levels at baseline and pre- to post-practices; symptom scores were assessed at each time-point. An accelerometer-embedded mouthguard was employed to measure the number of impacts (hits), peak linear acceleration (PLA), and peak rotational acceleration (PRA). Because we observed a distinct gap in impact exposure (hits, PLA, and PRA), players were clustered into lower (n = 7) or higher (n = 15) impact groups based on the sum of impact kinematics from all five practices. S100β levels significantly changed across the study duration. Although S100β levels remained stable from baseline to all pre-practice values, statistically significant acute increases in S100β levels were observed in all post-practice measures compared with the respective pre-practice values (range: 133–246% in the overall sample). Greater number of hits, sum of PLA, and sum of PRA were significantly associated with greater acute increases in S100β levels. There were significant differences in head impact kinematics between lower and higher impact groups (hits, 6 vs. 43 [Mlower − Mhigher = 35, p < 0.001]; PLA, 99.4 vs. 1148.5 g [Mlower − Mhigher = 1049.1, p < 0.001]; PRA, 7589 vs. 68,259 rad/s2 [Mlower − Mhigher = 60,670, p < 0.001]). Players in the higher impact group showed consistently greater increases in plasma S100β levels, but not symptom scores, at each post-practice than the lower impact group. Collectively, these data suggest that although players continued to play without noticeable change in symptoms, a brain-enriched serological factor suggests an acute burden from head impacts. Assessing the effects of repetitive subconcussive head impacts on acute changes in S100β levels may be a clinically useful blood biomarker in tracking real-time acute brain damage in collegiate football players.
Introduction
A
Unlike subjective measurement, a blood biomarker is a powerful objective approach to detect subtle structural and metabolic changes after neural damage. 7 –9 One candidate blood biomarker that may provide clinical utility after a head impact is the astrocyte-enriched protein, S100β. S100β is a member of the S100 family and preferentially binds to calcium ions to regulate intracellular calcium levels. Low concentrations of intracellular S100β are beneficial, whereas high concentrations can trigger apoptotic cascades. 10 Following mechanical stress, astrocytes undergo excessive calcium influx, upregulation of S100β, and translocation of S100β into the extracellular space. 11 Extracellular S100β can be a ligand for the cell-surface receptor for advanced glycation end products (RAGE) in neurons and activate c-Jun N-terminal kinase (JNK) signal transduction, further leading to tau phosphorylation. 9,12 Extracellular S100β may reach the bloodstream either by crossing the disrupted blood–brain barrier or through the glymphatic system where the interstitial fluid drains into the lymphatic system then into the bloodstream. 9 Although effects of increased plasma S100β level on non-cerebral tissues remain elusive, some studies suggest that there is minimal need of neuroimaging referral if the plasma S100β level is below 0.1 ng/mL. 13 –15
In the healthy human, both plasma and serum S100β levels are approximately 0.05 ng/mL, 16,17 and some studies report that increased levels of S100β in blood are superior for predicting mortality and recovery outcome after severe traumatic brain injury (TBI) to other blood biomarkers including glial fibrillary acidic protein, neuron-specific enolase, and brain-derived neurotrophic factor. 18 Among contact sport athletes, significant elevations in S100β levels are detectable within 3 h post-concussion (0.10 ± 0.01 ng/mL) compared with baseline (0.06 ± 0.01 ng/mL). 8,19 Similarly, football players sustaining subconcussive head impacts also show increases in S100β levels 1 h post-game (0.11 ± 0.05 ng/mL) compared with pre-game levels (0.06 ± 0.02 ng/mL). 20,21 However, the contributions of subconcussive impact kinematics, such as frequency and magnitude of hits, on acute and cumulative changes in S100β levels in the blood have not been addressed.
In this prospective longitudinal investigation of Division-I collegiate football players, we examined the acute and cumulative effects of repetitive subconcussive impacts on plasma S100β levels. Our first aim was to investigate the pattern of changes in S100β over the study duration. We hypothesized that acute increases in plasma S100β levels would be detected from pre- to post-practices—increases were expected due to exercise 22 and repetitive subconcussive head impacts. Our second aim was to examine the relationship of magnitude and frequency of repetitive subconcussive impacts, measured using head impact kinematics via an accelerometer-embedded mouthguard, on acute increases in S100β levels. We hypothesized that higher magnitudes and higher frequencies of repetitive subconcussive impacts would result in greater acute increases in S100β levels. This aim enables us to determine the additive effects of repetitive subconcussive impacts on S100β increases from pre- to post-practices to changes caused by exercise.
Methods
Participants
Twenty-two Division-I collegiate football players volunteered for study participation. The study was conducted at pre-season physical exams, during a series of helmet-only (no contact) and full-gear (full contact) training-camp practices. None of 22 players sustained a concussion during the study period, validated by team athletic trainers. Inclusion criteria included being a currently active collegiate football team member. Exclusion criteria were any history of head, neck, or face injury in the 6 months prior to study entry and/or any neurological disorders. Participants refrained from substances influencing the central nervous system (e.g., stimulants) and alcohol use was prohibited. The Temple University Institutional Review Board approved the study and participants gave written informed consent.
Study procedures
During pre-season physical examination, participants were fitted with the Vector™ mouthguard (i1Biometrics™, Inc., Kirkland, WA) to measure the frequency (number of hits) and magnitude of head accelerations. After a brief incubation in boiling water, the mouthguard was fitted to each participant's bite for a secure custom fit. Demographic information (e.g., age, body mass index) and blood samples were collected. Previous history of concussion and years of football experience were self-reported. During training-camp practices, head impact data were collected from five practices with intervals of 3 to 4 days between measures, starting from the first helmet-only (Pads-OFF, no contact), first full-gear (Pads-ON1, full contact), and three other full-gear practices (study flow chart, Supplementary Fig. 1; see online supplementary material at

S100β levels across study duration. Data points represent the actual mean and standard error at each time-point. **p < 0.0001 and *p < 0.001 compared with respective pre-practice value. p < 0.001 and  p < 0.01 compared with baseline.
p < 0.01 compared with baseline.
Head impact measurement
This study used an instrumented Vector mouthguard for measuring linear and rotational head kinematics during impact as previously described. 23 The mouthguard employs a triaxial accelerometer (ADXL377, Analog Devices, Norwood, MA) with 200 g maximum per axis to sense linear acceleration. For rotational kinematics, a triaxial rotational rate gyroscope (L3GD20H, ST Microelectrics, Geneva, Switzerland) was employed. 23,24 Accelerometer and gyroscope data were low-pass filtered at a 180 and 40 Hz cutoff, respectively. When a preset threshold for a peak linear acceleration (PLA) magnitude exceeded10.0 g, 16 pre-trigger and 80 post-trigger samples with a standard hit duration of 93.75 milliseconds of all impact data were transmitted wirelessly through the antenna transmitter to the sideline antenna and computer, then stored on a secure Internet database. The Vector mouthguard employs an in-mouth sensor to ensure that the data acquisition only occurs when the mouthguard is fitted in one's mouth. 23,24 From raw impact data extracted from the server, the number of hits, PLA, and peak rotational acceleration (PRA) were used for further analyses. Two observations were consistent outliers on the number of hits, sum of PLA, and sum of PRA; one observation was a consistent outlier on the average PLA and PRA. These observations were excluded from analysis (<2% of all data).
Blood collection and S100β measurements
Venous blood samples were collected at each time-point into vacutainer sterile tubes with the anticoagulant acid-citrate-dextrose (BD Bioscience). Plasma was separated by centrifugation (1500 x g, 15 min) and stored at −80°C until analysis. S100β measurements were performed using sandwich-based enzyme-linked immunosorbent assay (ELISA) kits (EMD Millipore, Billerica, MA). The lowest detection limit of the assay is 0.0028 ng/mL and the assay covers a concentration range up to 2 ng/mL with a typical intra-assay precision of
Symptom checklist
Participants completed the Post Concussion Symptom Scale, a subset of the Sports Concussion Assessment Tool 3, 25 as a method of assessing the presence of symptoms at each time-point throughout the study duration.
Statistical analysis
A series of mixed effects regression models (MRM) with random intercept were used to examine changes and factors (e.g., frequency and magnitude of head impacts) that may influence changes in S100β expression over time. MRM uses all available data, accommodates repeated measurements across time-points correlated to different degrees, and handles missing data. The first MRM focused on the pattern of change in S100β levels across study duration–11 time-points. The primary predictor variable was time, treated categorically as the S100β levels were not expected to change linearly across study duration. Of particular interest were the comparisons of S100β levels from baseline with each time-point and comparisons between each pre- to post-practice assessment. Based on findings from the initial model, all subsequent models focused on the change in S100β level (post minus pre) across the study duration of five time-points. We first examined the magnitude of change in S100β levels across time, with time being the primary predictor variable. Next, we examined the impact of kinematics (e.g., hits) on changes in S100β levels. Predictors included time, kinematics (treated as time-varying), and time by kinematics interactions (retained if p < 0.05). The last series of models focused on group variables (e.g., impact, concussion history) and changes in S100β levels. Predictor variables included time, group, and the time by group interaction (retained if p < 0.05). All analyses were conducted with SAS (v.9.4 for Windows; SAS) and significance was set at p < 0.05.
Results
Demographic and head impact kinematics
A total of 721 head impacts were recorded from the 22 players during the five training camp practices. Demographics and kinematics are summarized in Table 1.
Based on the sum from five-practice impact kinematic data collections (see Methods section).
DB, defensive back; DL, defensive lineman; OL, offensive lineman; PLA, peak linear acceleration; PRA, peak rotational acceleration; QB, quarterback; RB, running back; SD, standard deviation; WR, wide receiver.
Pattern of S100β expression changes across study duration
Plasma S100β levels changed significantly across the study duration, F (10, 188) = 18.97, p < 0.001 (Fig. 1). S100β levels remained stable from baseline to all pre-practice time-points (p's > 0.14). Conversely, S100β levels increased from baseline to all post-practice time-points (p's < 0.01; Table 2). Notably, when comparing acute changes in S100β levels between pre- and post-practice for each practice, there were significant increases in S100β levels from all pre- to post-practices (p's < 0.001, Fig. 1; Table 2). The magnitude of these increases was similar across all practices, F (4, 73) = 1.31, p = 0.28 (Supplementary Fig. 2; see online supplementary material at

Association between kinematic variables and changes in S100β levels (post minus pre). Associations are depicted between change in S100β levels to total number of hits
p < 0.001; ** p < 0.01; * p < 0.05; ‡ p = 0.07; T p = 0.07; † p = 0.09.
Results reflect one model conducted in the overall sample and one model focusing on the differences between impact group.
Effect of subconcussive head impact kinematics on acute changes in plasma S100β
Kinematic variables were associated with pre-post practice changes in S100β levels. For hits, greater numbers were associated with greater pre-post practice increases in S100β levels, F (1, 70) = 11.54, p = 0.001 (Fig. 2A). For example, 4 hits predicted a 0.02ng/mL increase (SE = 0.003) and 10 hits a 0.025ng/mL increase (SE = 0.007) pre-post practice in S100β levels (Fig. 2F). Similar associations were apparent with SumPLA, F (1, 70) = 8.78, p = 0.004, SumPRA, F (1, 70) = 14.05, p < 0.001, AvgPLA, F (1, 71) = 2.92, p = 0.09, and AvgPRA, F (1, 71) = 5.95, p = 0.01 (Fig. 2B–E). The relationship between kinematics and pre- to post-practice changes in S100β levels were stable over time as indicated by no significant time by kinematic variable interactions (p's > 0.62).
When examining grouping variables, only head impact (computed using impact kinematics across practices,
23
F (10, 188) = 18.96, p < 0.001, but not concussion history or years of football experience (p's
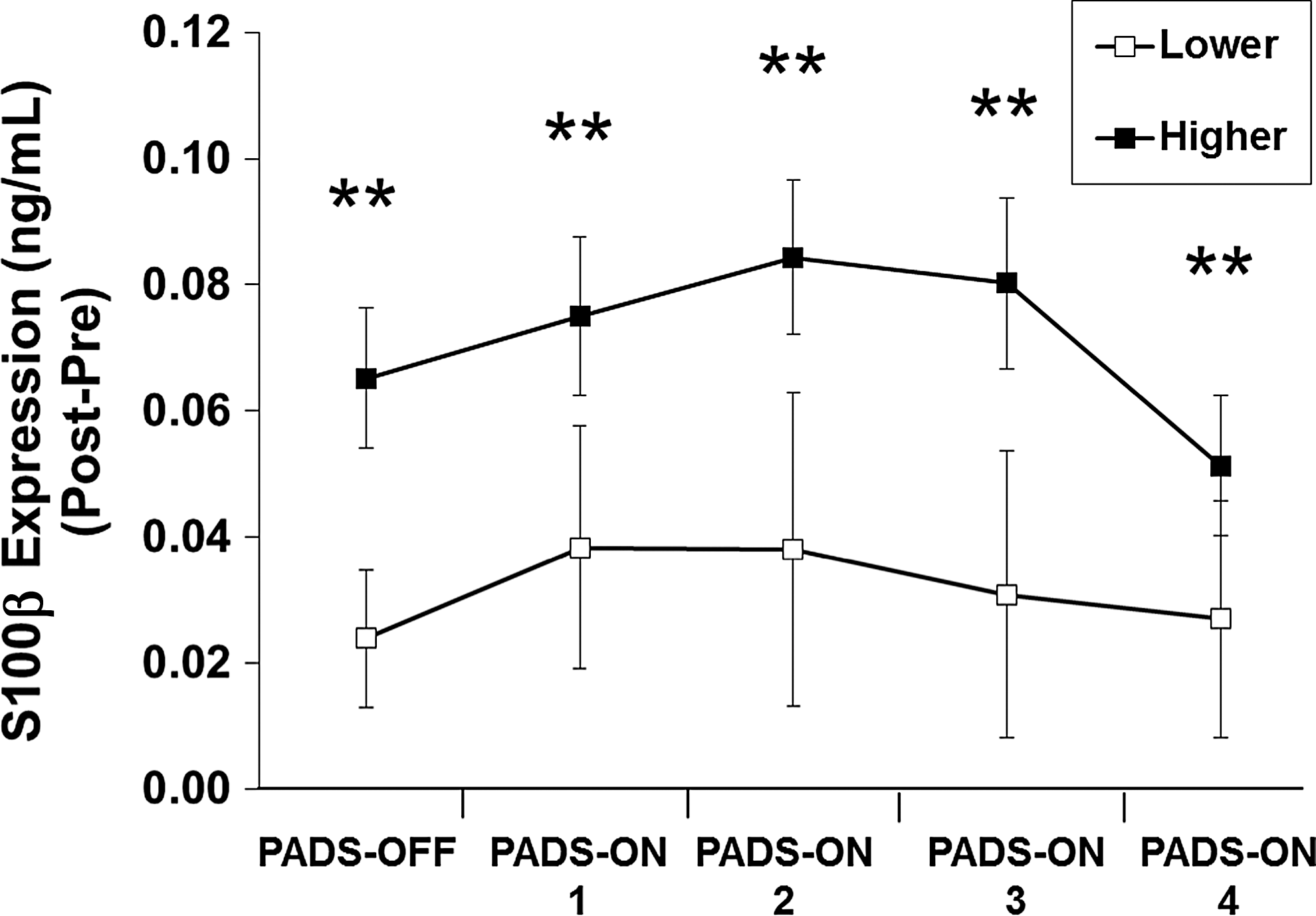
Group comparison: changes in S100β levels (post minus pre). The higher impact group showed greater changes in S100β levels compared with the lower impact group (**p < 0.001). The group by time interaction was not significant (p = 0.93).
Subconcussive head impact kinematics and changes in levels of plasma S100β relative to baseline
To allow for comparisons with previous studies, 20,21 we examined changes in S100β expression levels across the entire study duration as a function of impact group (higher vs. lower). Whereas the groups showed similar S100β levels at baseline (B = −0.005, SE = 0.02, p = 0.80), each group showed a different pattern of increase in S100β levels from baseline to each time-point. Consistent with the overall sample, S100β levels remained stable in the higher impact group from baseline to all pre-practice time-points (p's > 0.10; Table 2). However, S100β levels increased from baseline to all post-practice time-points (p's < 0.001; Fig. 4; Table 2). Conversely, there was no significant increase in S100β levels in the lower impact group from baseline to all pre- (except fourth Pads-ON practice levels declined, p = 0.02) and post-practice time-points (p's > 0.06; Table 2).

Group comparison: changes in S100β across study duration. Significant changes compared with the baseline were predominately observed only in the higher impact group. ** p < 0.0001 compared with baseline. *The lower impact group showed no changes except from baseline to fourth Pads-ON practice.
Symptoms
Consistent with our previous study, 23 symptom scores did not change across the study duration, F (10, 195) = 1.38, p = 0.19, and there were no differences in symptom scores between the higher and lower impact group over time, F (10, 185) = 0.60, p = 0.81.
Discussion
To our knowledge, this is the first prospective longitudinal cohort study in collegiate football players examining the relationship between subconcussive head impact kinematics and changes in plasma S100β levels. The first notable finding was that plasma S100β levels were acutely increased after football training-camp practices. Second, consistent with previous reports that the S100β half-life in the blood is short (approximately 97 min), 16,26 we showed no evidence of cumulative burden from repetitive subconcussive impacts. Third, we report a significant positive relationship between head impact kinematics and acute increases in plasma S100β levels. Specifically, increases in the frequency and magnitude of impact regardless of practice day were strong predictors of the degree of acute change in S100β levels.
Findings from the study are clinically relevant, as plasma S100β may be useful in discerning different severities of brain injury. The average plasma concentration of S100β in healthy individuals is 0.05 ng/mL, 16,17 and similar levels were observed at the pre-season baseline time-point in our study (mean ± SD; 0.04 ± 0.04 ng/mL). In line with previous football subconcussion studies, 20 our data show that although the lower impact group showed similar S100β levels at all pre- and post-practice time-points relative to baseline (range of means 0.01 to 0.06 ng/mL), the higher impact group showed significantly higher plasma S100β levels at all post-practice time-points relative to baseline (range of means 0.09 to 0.13 ng/mL). Comparatively, in other studies examining the effects of mild TBI (mTBI) on serum S100β levels, individuals with mTBI showed higher levels (mean, 0.31 ng/mL) within 6 h post-injury compared with healthy controls (mean, 0.05 ng/mL). 27 Similarly, in a subsequent study examining the relationship between blood S100β levels and intracranial injury using computed tomography (CT) scanning in individuals with mTBI within 12 h post-injury, mTBI patients with a positive CT scan showed higher S100β levels (mean, 0.36 ng/mL) than mTBI patients without intracranial injury (mean, 0.18 ng/mL). 28 Further, studies in individuals with severe TBI consistently demonstrate that S100β levels correlate well with primary damage, secondary deterioration, and with outcomes after a head injury such as 1-month survival, recovery rate, and prolonged coma. For example, average serum S100β levels ranging between 0.3 and 1.6 ng/mL are associated with more favorable outcomes, whereas levels ranging between 1.1 and 4.9 ng/mL are associated with less favorable outcomes. 29,30 Although study procedures and S100β measurements varied across studies, there is a clear trend in severity-dependent levels of S100β increasing after TBI (e.g., subconcussion, mild and severe TBI).
Although changes were not significant, exercise effects may have contributed to pre- to post-practice increases in S100β levels. Similar to previous subconcussion studies, recordings of exercise intensity and running distance remain a limitation in the current study. 20,21,31 The lower impact group comprised wide receivers, a defensive back, and special team players, which are speculatively running intensive positions. Evidently, regardless of type of practice (Pads-OFF or Pads-ON), each player in the lower impact group experienced an average 1.29 head hits per practice. These players showed on average 0.036 ng/mL increases in S100β levels from pre- to post-practice. Existing evidence indicates that individuals engaging in exhaustive exercise activities including swimming, soccer, and intensive running in a hot environment show on average a range of 0.03 to 0.05 ng/mL increases in S100β levels. 32 –34 In comparison, players in the higher impact group experienced 2 to 11 impacts on the Pads-OFF practice with an average increase in S100β level of 0.06 ng/mL, whereas the players experienced 4 to 25 hits per Pads-ON practice with an average increase in S100β level of 0.09ng/mL. Taken together, subconcussive head impacts may cause acute increases in S100β levels above and beyond the increases expected from exercise alone.
One explanation for pre- to post-practice increases in S100β levels among the higher impact group is that head insults concurrent with high intensity exercise further compromise the integrity of the blood–brain barrier. 22 Because astrocytes regulate the blood–brain barrier, additional S100β may be released into peripheral circulation due to minor head insults. 35 Another possible explanation is that greater increases among the higher impact players may be due to cerebrovascular damage and acute hypertensive effects on the blood–brain barrier. Associations between high blood pressure and blood–brain barrier disruption is well documented. 36 Further, players in football front-line positions such as lineman and tight ends tend to develop hypertensive characteristics, independent from their fat mass, 37 as their play style is obligated to perform repetitive concentric and isometric contraction. Additional large-scale studies are needed to draw more definitive conclusions regarding both of these explanations.
The Vector mouthguard contains an in-mouth sensor that only detects impacts when it is fitted in the mouth, mitigating a risk of false recording. Kinematic accuracy of the instrumented mouthguard 23 showed an excellent correlation with the matched data from an anthropomorphic testing device (crash test dummy). 24,38 Higgins and colleagues acquired impact kinematic data from a sensor-embedded football helmet and mouthguard after subjecting participants to a controlled weight-dropping intervention, and compared the acceleration data with head-form center of gravity acceleration. Their results suggest that mouthguard acceleration showed more accurate representation of head acceleration than helmet. 39 Further, when headgear-mounted, mouthguard, and skin-patch sensors were compared with high-speed video during soccer headings, the mouthguard showed a superior accuracy in displacement value less than 1 mm; whereas, headgear and skin patch displaced as much as 13 mm and 4 mm from the ear canal reference points, respectively. 40
In summary, there is growing concern that even low magnitude head impacts, if sustained repetitively, can result in significant long-term neurological deficits. Whereas numerous studies focus on concussions, limited information is available on the effects of subconcussive impacts, injury triage, and effective management of subconcussions. Our data provide initial evidence that plasma S100β levels acutely increase from pre- to post-football practice and that increases in the frequency and magnitude of head impacts result in the greatest acute change in plasma S100β levels. These findings have vast clinical implications not only in sports-related brain trauma, but also to blast-induced and industrial TBI. Future studies using larger scale prospective approaches are warranted to investigate the potential threshold between repetitive subconcussive impacts and concussion, by tracking within-subject changes in plasma S100β levels and exercise after subconcussion and concussion.
Footnotes
Acknowledgments
This work was supported by the Pennsylvania Athletic Trainers' Society research grant (to K. Kawata), generous support from Athole G. Jacobi, MD, and from the Marianne Garman Burton Foundation for Caregivers (to D. Langford), and a seed grant from Temple University Office of the Vice Provost for Research (to D. Langford). Sponsors had no role in the design or execution of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.