
Abstract
A substantial minority of children experience post-traumatic stress symptoms (PTSS) following injury. Research indicates variation in the trajectory of PTSS following pediatric injury, but investigation of PTSS following concussion has assumed homogeneity. This study aimed to identify differential trajectories of PTSS following pediatric concussion and to investigate risk factors, including acute post-concussive symptoms (PCS), associated with these trajectories. A total of 120 children ages 8–18 years reported PTSS for 3 months following concussion diagnosis using the Child PTSD Symptom Scale, with a score of 16 or above indicating probable post-traumatic stress disorder diagnosis. Age, gender, injury mechanism, loss of consciousness, previous concussions, prior hospitalization, prior diagnosis of depression or anxiety, and acute PCS were assessed as risk factors. Data were analyzed using group-based trajectory modeling. Results revealed 16% of children had clinically significant PTSS 2 weeks post-concussion, declining to 10% at 1 month and 6% at 3 months post-injury. Group-based trajectory modeling identified three trajectories of PTSS post-concussion: “resilient” (70%); “recovering” (25%), in which children experienced elevated acute symptoms that declined over time; and “chronic symptomatology” (5%). Due to small size, the chronic group should be interpreted with caution. Higher acute PCS and prior diagnosis of depression or anxiety both significantly increased predicted probability of recovering trajectory group membership. These findings establish that most children are resilient to PTSS following concussion, but that PTSS do occur acutely in a substantial minority of children. The study indicates mental health factors, particularly PTSS, depression, and anxiety, should be considered integral to models of concussion management and treatment.
Introduction
C
Following injury, children may experience post-traumatic stress symptoms (PTSS), 15 or subthreshold post-traumatic stress disorder (PTSD). According to the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5), 16 PTSS occur in response to a traumatic experience and are grouped into four symptom clusters: intrusion, avoidance, altered cognition/mood, and arousal—some of which have unique presentations in children. Identification of subthreshold symptoms is important in child populations as research indicates the DSM criteria for PTSD may be overly restrictive in identifying clinically significant symptomatology in childhood. 17,18 In children and adolescents, PTSS have been associated with negative outcomes including disruption of important relationships, somatic symptoms, academic problems, and increased risk of psychiatric disorders and suicide. 19,20
Studies have identified objective predictors of PTSS following child injury, such as injury type and severity. 21,22 However, recent meta-analyses 15,23 and a systematic review 24 argue subjective factors—such as perceived life threat, appraisals of trauma severity, and beliefs about initial symptoms—and post-trauma variables (e.g., coping strategies, social support, the family environment) have greater influence. 15,23,24 Pre-morbid and co-morbid psychological problems, younger age, and female gender also are associated with greater risk of PTSS. 15,23,24
PCS have been associated with PTSS following mTBI in both adults 25 –27 and children. 28 However, heterogeneity in mTBI definitions 6,8 and symptom overlap between PTSS and PCS have complicated research with no reliable method of differentiation. 29,30 Additionally, existing studies tend to compare mean PTSS rates over time, based on an assumption children with concussion are a homogenous group. 13 Recent studies have highlighted individual differences in response to trauma in general and identified multiple trajectories of PTSS over time. 31 –34 For example, Le Brocque and colleagues 34 described three PTSS trajectories in a sample of injured children (excluding head injuries): resilient, recovery, and chronic. These trajectories, as well as a fourth group (delayed reactions) were replicated in a sample of uninjured children who witnessed a traumatic event. 32
Using group-based trajectory modeling and a longitudinal design, this study aimed to: 1) investigate the incidence and trajectories of PTSS in children and adolescents following concussion; 2) determine whether severity of acute PCS increases the risk of elevated PTSS; and 3) extend the exploration of risk factors associated with PTSS to a young concussion sample.
Methods
Design
This study is part of a larger prospective, longitudinal study, TakeCARe (Concussion Assessment and Recovery Research), undertaken at a state-wide, tertiary pediatric hospital, which is the only pediatric trauma center in the area providing primary and secondary medical services to the local community. 35
Participants
Participants were a subsample (n = 120) of the TakeCARe study, 35 recruited between 2013–2015. Children ages 5–18 years presenting to the emergency department (ED) at the Royal Children's Hospital (RCH), Melbourne, Australia, within 48 h of sustaining a concussion were eligible to participate. Concussion was defined according to the Zurich Consensus Statement on Concussion in Sport 36 as having sustained a head injury with one or more symptoms in one or more of the following categories: somatic (headache, nausea, loss of balance, clumsiness, sensitivity to light or sound, dizziness); cognitive (feeling foggy, memory or concentration difficulties, confusion, slowed responses/reaction times); emotional/behavioral (lability, irritability, nervousness, sadness); physical signs (loss of consciousness, amnesia); or sleep disturbance (sleeping more, fatigue, insomnia). Children with Glasgow Coma Scale <13, abnormal CT scans, or multiple injuries, or those who required intubation, neurosurgical operative intervention, or general anesthesia were excluded. Other exclusions included injury due to abuse or assault, no clear history of trauma as the primary event (e.g., migraine, seizure), intoxication upon presentation, intellectual disability, or insufficient understanding of English.
Measures
PTSS were assessed using the Child PTSD Symptom Scale (CPSS), 37 a 17-item self-report measure of PTSD symptoms listed in the DSM-IV, 38 validated for children 8–18 years. Items are scored on a 4-point frequency scale and summed to calculate a continuous total severity score (range 0–51). A severity score of 16 or above indicates probable PTSD diagnosis. 39 The CPSS has shown good psychometric properties. 37,39
PCS were assessed using the parent report form of the Post Concussive Symptom Inventory (PCSI), 40 a developmentally appropriate and psychometrically robust 10 measure for assessing PCS in children and adolescents. Parents completed the form containing 20 items scored on a 7-point Gutman scale. The PCSI provides a total PCS severity score and sub-scale scores for physical, cognitive, emotional, and fatigue symptoms. 10
Treating doctors reported injury-related information, including details of concussion diagnosis, loss of consciousness, and injury mechanism. Parents completed pre-injury and demographic information forms reporting the child's age, sex, prior concussions and hospitalizations, and prior diagnosis of depression or anxiety.
Procedures
This study was approved by the RCH Human Research Ethics Committee. Eligible families were approached in the ED by trained research assistants and written informed consent gained from parents and children. Recruitment occurred between 9
Statistical analysis
Group-based trajectory modeling, a specialized form of finite mixture modeling that does not require complete data across all time-points, 41,42 was used to investigate trajectories of PTSS over time. For a hypothesized number of underlying latent groups, it uses maximum-likelihood estimation to identify distinctive clusters of individuals following similar trajectories for an outcome, outlines the shape (polynomial parameters) of each trajectory and size of each group, and profiles the characteristics of individuals within trajectory groups. 43,44 It allows analysis of risk factors for group membership through the inclusion of time-invariant predictors. 41 Analyses were conducted in Stata/ICv13.1 using the traj plugin. 43 Alpha was set to 0.05 for all analyses.
Model selection involved two-stages: 1) identification of optimal number of trajectory groups, and 2) determining preferred polynomial orders specifying the shape of the identified trajectories. 41 Assuming quadratic longitudinal profiles, models containing one to five groups were compared on the Bayesian Information Criterion (BIC), parsimony, and fit with prior theory. 41 Once the optimum number of groups was determined, non-significant polynomial orders were dropped individually and models again compared on BIC for final selection. Children were assigned to the group for which they held the highest posterior probability of membership.
Bivariate risk factor analysis was conducted to estimate the association between demographic, pre-injury, and injury-related characteristics, including acute PCSI scores, and the probability of trajectory group membership. Partial effects of significant predictors were then investigated using multiple risk factor analysis.
Results
Sample attrition
Of eligible children, 221 were enrolled in the larger study (Fig. 1). Eighteen were excluded post-enrollment, 52 participants dropped out prior to first CPSS report (2 weeks post-injury), 30 were excluded due to CPSS age validity requirements (< 8 years), and one participant was excluded due to missing CPSS data, resulting in a sample of 120 children aged 8–18 years. (For further recruitment and attrition detail, see Supplementary Table 1.) All children with CPSS data for at least one time-point were included in analyses. CPSS scores across all time-points were available for 73% children: 95% of children completed the CPSS 2 weeks post-injury, 87% 1 month post-injury, and 86% 3 months post-injury. Statistical analysis indicated children who completed all time-points did not significantly differ from those who did not on CPSS scores or other relevant factors.
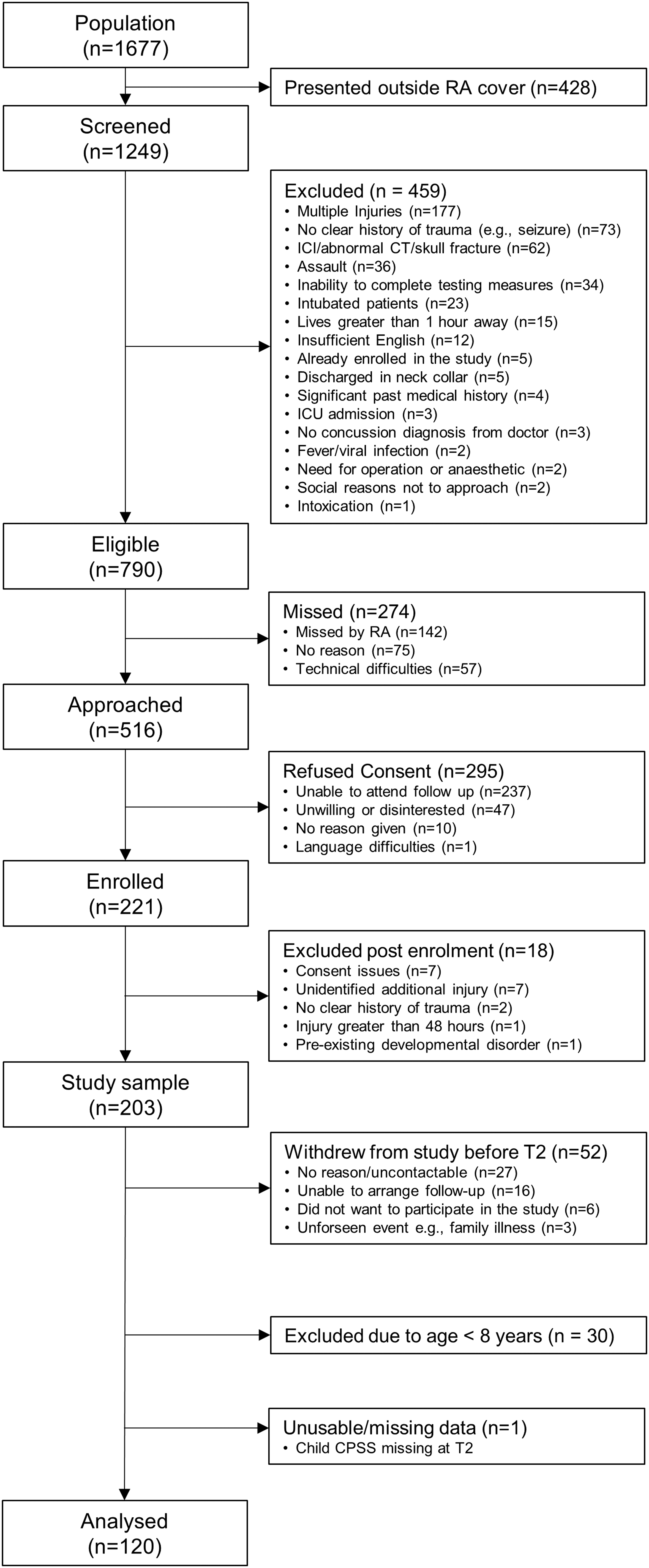
Recruitment and participation flow-chart for the TakeCARe study, October 26, 2013 to October 3, 2015.
Sample characteristics and descriptive statistics
Demographic, pre-injury, and injury-related data are shown in Table 1. Descriptive univariate statistics for PTSS and PCS are shown in Table 2. PTSS were present across all time-points. Mean CPSS scores were generally low, well below the clinical cut-off score of 16, and declined over time. However, 16% of children scored at or above the clinical cut-off score for probable PTSD diagnosis 2 weeks post-concussion, 10% 1 month post-concussion, and 6% 3 months post-concussion.
Injury mechanism % does not sum to 100 because some sport-related injuries also involved falls. Higher proportion of males in the sample is common in concussion studies, consistent with higher prevalence of traumatic brain injury in males.55
SD, standard deviation; MVA, motor vehicle accident.
Trajectory analysis
Group-based trajectory modeling of CPSS scores identified the best-fit solution with the highest BIC value contained three optimal trajectory groups (Fig. 2): 1) “resilient” (n = 85), with CPSS scores well below clinical levels for the entire study period; 2) “recovering” (n = 29), with CPSS scores initially at clinical levels but declining to below clinical significance within 1 month; and 3) “chronic” (n = 6), where CPSS scores remained high throughout. The resilient trajectory was quadratic, demonstrating a fast decline of initially low levels of distress, and largest in size, containing a population estimate of 70% of children. The recovering group was linear, indicating consistent decline in elevated symptoms, and contained a population estimate of 25% of children. The chronic group was constant, describing little change in levels of symptomatology, and contained a population estimate of 5% of children. Descriptive statistics for each trajectory group are shown in Table 3.
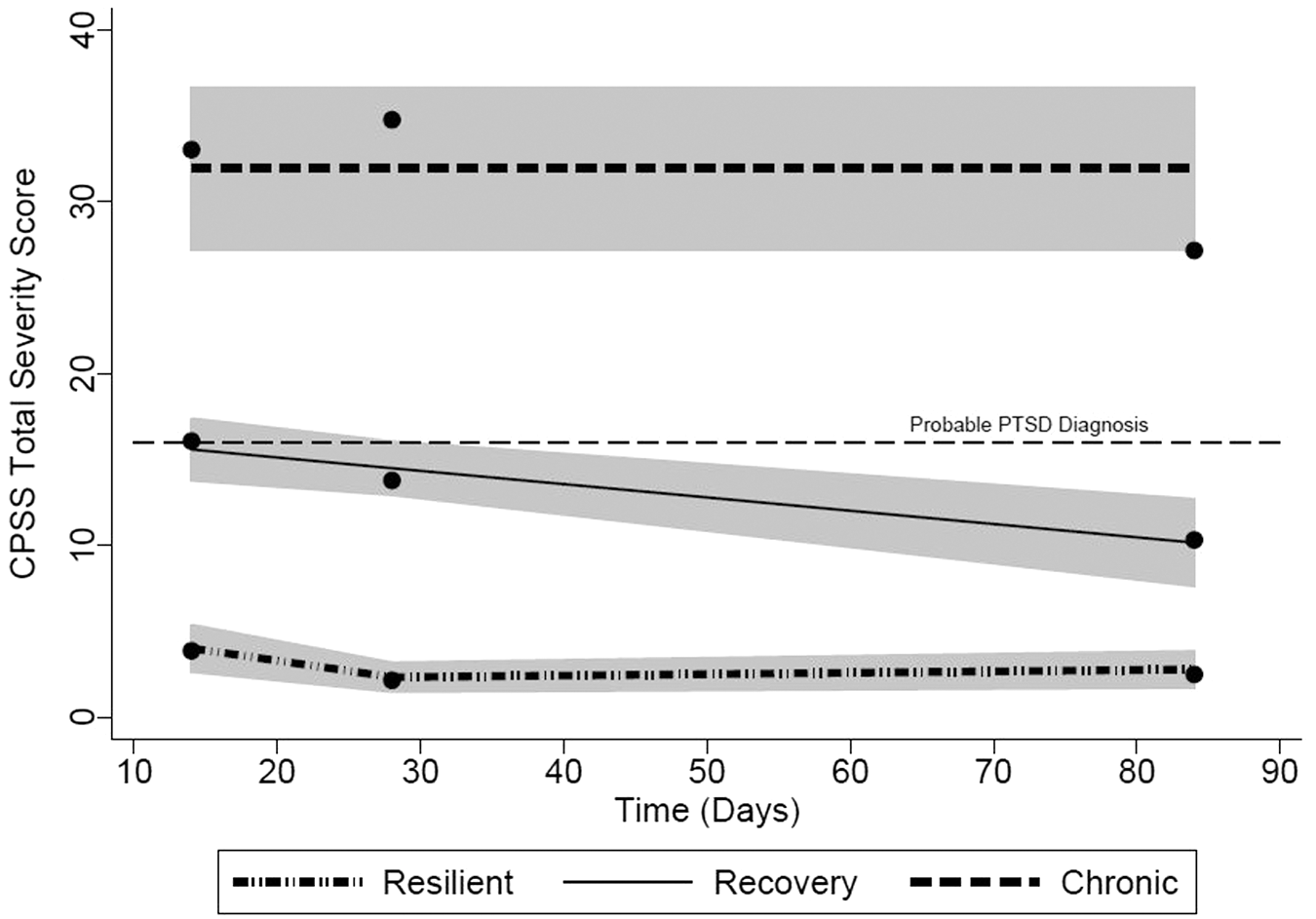
Lines of best fit and 95% confidence intervals for the three trajectories of post-traumatic stress symptoms over 3 months following pediatric concussion.
Resilient group n = 85. Recovering group n = 29. Chronic group n = 6. Injury mechanism % does not sum to 100 because some sport-related injuries also involved falls.
PTSS, post-traumatic stress symptoms; SD, standard deviation; MVA, motor vehicle accident; PCSI, Post Concussion Symptom Inventory.
Risk factor analyses
Bivariate risk factor analysis estimated the odds ratio of PTSS trajectory group membership, relative to the resilient group, based on demographic, pre-injury, and injury-related factors, including acute PCS. As the chronic trajectory group was small (n = 6), at times perfect prediction excluded this group from analysis. Only previous diagnosis of depression or anxiety and acute PCS were significant risk factors for PTSS (Table 4). Previous diagnosis of depression or anxiety increased the probability of recovering group membership, relative to the resilient group. No children in the chronic group had pre-injury depression or anxiety, prohibiting analysis of this group. Total PCSI score 1–4 days post-injury also was a significant risk factor, with higher total PCSI scores increasing the predicted probability of recovering group membership, relative to the resilient group. This result was not consistent for the chronic group.
N = 120; PCSI, n = 115.
Statistically significant at the 0.05 level.
-Omitted from analysis due to perfect prediction.
PTSS, post-traumatic stress symptoms; CI, confidence interval.; MVA, Motor vehicle accident; PCSI, Post Concussion Symptom Inventory.
As PCS was a significant risk factor for PTSS, post hoc analysis investigated if this was specific to a particular subset of PCS through analysis of PCSI subscales. Physical, cognitive, and emotional PCS all significantly increased the risk of recovering group membership relative to the resilient group (Table 4), while fatigue symptoms approached significance.
Significant risk factors were entered into a final model to investigate partial effects, with the effect of prior diagnosis of depression or anxiety on recovering group membership increasing and remaining significant (OR = 32.03 [3.26–314.47]; p = < 0.001). Effects of PCSI total severity score were unchanged.
As PCS and PTSS share some symptoms, correlations between the two measures were conducted. Correlations between acute PCSI (1–4 days) and the CPSS at 2 weeks (r = 0.25; p = < 0.001), 1 month (r = 0.22; p = 0.03), and 3 months (r = 0.16; p = 0.11) were small to moderate. 45
Discussion
Results indicate the presence of clinically significant PTSS acutely post-concussion, with 16% of children at or above clinical levels 2 weeks after diagnosis. Three recovery trajectories were identified for PTSS following child concussion: resilient, recovering, and chronic. Of the risk factors examined, pre-injury diagnosis of depression or anxiety and elevated acute PCS were significantly associated with greater likelihood of membership in the recovering trajectory group, characterized by initially elevated PTSS.
The identified trajectories are consistent with those described in general child trauma research, 34 which excluded children with head injuries. Analyses demonstrated the majority of children (70%) did not experience elevated PTSS post-concussion, reflecting findings that most children are resilient to psychological trauma. 31 A small but substantial number (25%) experienced clinical levels of PTSS 2 weeks post-injury but recovered within 1 month, indicating acute stress. Although falling below the clinical cut-off for a probable PTSD diagnosis by 1 month, these children continued to report elevated levels of PTSS, compared with the resilient group, throughout the study period. Given PTSD diagnostic criteria may be too restrictive in identifying clinically significant symptomatology in child populations, 17,18 these elevated but subthreshold symptoms may indicate important impairment or distress. Subthreshold acute stress symptoms also have been found to be a more effective predictor of PTSD diagnosis in children more than 3 months after accidental injury than diagnosis of acute stress disorder. 18
A minority of children (5%) in this sample demonstrated chronic PTSS symptomatology above clinical levels for the entire study period. While confidence intervals for this group were quite wide, inspections of CPSS means and standard deviations indicated this was likely due to sample size rather than variation. Of note, the existence of a chronic group is consistent with prior research 32,34 and its omission would likely result in the loss of clinically important information about PTSS, which is itself relatively rare. Therefore, the three group model was accepted, highlighting the possibility that a minority of children do develop prolonged PTSS acutely post-concussion. Given the small group size (n = 6), findings related to this group should be interpreted with caution and are in need of replication. This study found no evidence of the delayed-onset PTSS noted in other studies, 32,46,47 likely due to the study duration.
Elevated acute PCS increased the predicted probability of recovering trajectory group membership, relative to the resilient group, indicating clinically significant PCS is a risk factor for the acute development of PTSS. Compared with the predicted probability of recovering group membership for an average child (0.24), a PCSI total score 2 standard deviations above the mean (72.43), indicating severe symptoms, 48 increased the predicted probability of recovering group membership substantially to 0.47.
The relation between PCS and PTSS is consistent with prior studies documenting the association in adults 25,26 and children. 28 Moreover, this study identifies the relation in concussion specifically, indicating this is not limited to injuries on the more severe end of the TBI spectrum. The weak-to-moderate correlations between measures of PTSS and PCS identified in this study indicate the effect also is unlikely due solely to symptom overlap. Recent research found deficits in sustained attention following mTBI predict the development of PTSS, which may point to a mechanism behind the relation between PCS and PTSS following concussion. 49
Although results of the current study suggest acute PCS increases the risk of PTSS, assumptions of causation should be tempered. While previous studies using control groups have suggested PCS may contribute to acute PTSS in children following mTBI, 28,47 others have suggested instead that PTSS predicts persistent PCS. 3 Regardless of direction of effect, the association has clear clinical implications, discussed below.
Of the other factors examined, only pre-injury diagnosis of depression or anxiety predicted PTSS trajectories post-injury, and then only for the recovering group, possibly due to the small size of the chronic group. Of note, no effect was found for age, gender, or injury mechanism. The effect of pre-injury diagnosis of depression or anxiety is consistent with meta-analytical and systematic review findings that pre-morbid and co-morbid psychological problems predict the development of PTSD following other forms of trauma, 23 pediatric injury, 15,24 and TBI. 50 Similarly, Le Brocque and colleagues 34 found pre-injury internalizing behaviors significantly increased the risk of both recovery and chronic PTSS trajectory groups following pediatric injury in general. Co-morbid anxiety acutely post-trauma also has been found to predict recovery PTSS trajectory group membership and acute co-morbid depression to increase the risk of chronic-dysfunction group membership. 32 The current findings extend these effects to children with concussion.
This study indicates a substantial minority of children develop PTSS following concussion. This has important clinical implications, as research has shown the majority of pediatric emergency physicians largely underestimate the likelihood that children may develop PTSS following injury and are unaware of factors associated with PTSS development. 51 Relatedly, models of concussion management often exclude the influence of mental health factors. This study indicates psychopathology, particularly PTSS, depression, and anxiety, should be considered important elements in the study and treatment of pediatric concussion. Screening for pre-morbid internalizing disorders and elevated PCS acutely after concussion may help identify children who are at risk of PTSS and allow for early targeted intervention.
While pre-morbid depression or anxiety and elevated acute PCS have been found to increase the risk of children developing PTSS, identification of factors that predict chronic symptomatology are still lacking. It is possible effects were not observed in this study due to the small size of the chronic group. A larger sample may reveal risk factors that successfully discriminate between all trajectory groups. This study also combined depression and anxiety into one parent-report item, though Hong and colleagues 32 suggest comorbid anxiety predicts the recovering course while depression predicts chronic symptomatology. Larger studies should explore these factors independently to determine if they discriminate between PTSS trajectories following concussion. Other factors, such as children's and families' beliefs about the trauma and their initial concussion symptoms and acute stress symptoms, should be investigated. Physiological indicators, such as initial heart rate, also have been suggested to predict children who will develop chronic PTSD 52 and may differentiate between trajectory groups.
This study has a number of limitations. The study relied on self- and parent-reported symptoms rather than more objective measures. However, the measures used in this study have the benefits of clinical utility, being feasible for use as screening measures within the ED. The study also did not include a control group. Inclusion of orthopedic-injured controls would enable consideration of general injury effects and different PTSS presentations between groups, 50 and better inform the relationship between PCS and PTSS. Finally, the number of possible participants missed and declining to participate in the study highlights the possibility of selection bias and may limit the generalizability of results. Representative pediatric concussion samples are difficult to obtain because many individuals do not present for treatment. As many existing studies recruit participants attending follow-up clinics, which are likely to be biased towards those experiencing more severe or persisting symptoms, this study has the advantage of recruiting a more general sample than most. Acknowledging sampling limitations, this study presents detailed recruitment data (Fig. 1) to allow readers to determine generalizability.
To the authors' knowledge, this study is the first to investigate trajectories of PTSS following child concussion. This study demonstrates that while most children are resilient, PTSS develop in a substantial minority of children following concussion, are most common acutely post-injury, and vary in course following three identified trajectories: resilient, recovering, and chronic. While many demographic and injury-related variables did not predict PTSS trajectory group membership, prior diagnosis of depression or anxiety was a significant risk factor for recovering group membership. Important to concussion specifically, elevated PCS were also a significant predictor of recovering group membership. Although confirmation of the chronic trajectory and risk factors that discriminate between recovering and chronic trajectories require further research, the current findings indicate screening for pre-morbid depression and anxiety and elevated PCS acutely after concussion may allow for early intervention and the prevention of negative outcomes for children.
Footnotes
Acknowledgments
This study was funded by the Royal Children's Hospital Research Foundation and the Victorian Government Operational Infrastructure Scheme. SH was funded by an Australian National Health and Medical Research Council (NHMRC) Development grant, FEB was funded by the Royal Children's Hospital Research Foundation, and VA by an NHMRC Senior Practitioner Fellowship. The funding organizations did not have a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.