
Abstract
The recent disappointing results of phase III trials for progesterone (PROG) in traumatic brain injury (TBI) have triggered speculation about reasons for the negative outcomes. One confounding factor may have been the vehicle used to administer PROG. Virtually all of the many pre-clinical experiments informing the clinical trials and reporting beneficial PROG effects used more soluble 2-hydroxypropyl-b-cyclodextrin as a vehicle given intraperitoneally or subcutaneously rather than a lipid formulation given intravenously (IV). The present investigation compared the effect of PROG infusion with that of lipid emulsion (Intralipid®) as a carrier/vehicle on edema following TBI in rats. Eight-mg/kg doses of PROG with 20% Intralipid were given IV via central venous catheter beginning 1 h post-injury over a 1 h duration (1.2 mL/h). Animals were killed and brains removed at 24 h post-injury. All the brain-injured groups showed more edema compared with the control group. However, PROG+Intralipid significantly attenuated cerebral swelling compared with Intralipid alone. No difference was observed between the TBI-alone and Intralipid groups. Although this study used much a smaller volume and shorter duration of Intralipid infusion than the clinical trials (up to 5 days of continuous infusion), our results suggest that the use of Intralipid in rats did not prevent or mask the beneficial effect of PROG.
Introduction
D
Another factor that could have confounded results is the intrinsic biological activity of the carrier chosen for the intravenous (IV) delivery of PROG. 29 In both phase III trials, the test drug was dissolved in a lipid emulsion. Patients enrolled in ProTECT III received IV PROG in 20% Intralipid® (974 mL) at a flow rate of 14 mL/h for 1 h and then 10 mL/h for a total infusion duration of 96 h. Patients in the SYNAPSE trial received either IV PROG in a proprietary lipid emulsion of 6% soybean oil and 1.2% egg lecithin, or just the emulsion within 8 h after injury and continued for 120 h.
It is questionable whether the choice of Intralipid as the carrier for PROG treatment in humans was justified. Most of the animal studies on PROG used more soluble 2-hydroxypropyl-β-cyclodextrin; none used Intralipid. Multiple studies have demonstrated that lipid carriers are not neutral. 30 –33 Lipids used as a vehicle for drug treatment can have important biological effects on physiology and may have confounded the interpretation of the data. Some of Intralipid's effects are beneficial, some are not. Lipid emulsions have been shown to reduce inflammatory reactions in endothelial cells by suppressing the expression of intercellular adhesion molecule (ICAM-1), an indicator of inflammation of endothelial cell, which affects modulating vascular repair in the damaged brain. 30 Continuous and rapid infusion of 10% Intralipid has been shown to reduce food intake and cause build-up of intracellular cholesterol in rats. 31 –33 A recent clinical study looking at the effect of Intralipid on dosing of a local anesthetic, ropivacaine, demonstrated that Intralipid might prevent the rapid increase in concentration of the drug after extravascular administration. 34
A meta-analysis of case reports found that Intralipid administration was effective in reversing multiple drug toxicities, 35 and Taftachi and colleagues 36 showed that IV lipid emulsions can be effective in the acute stages of drug intoxication, improving Glasgow Coma Scale (GCS) outcomes and reducing blood glucose levels up to 6 h after administration. However, Intralipid is also reported to increase insulin resistance in heart tissue. An experimental model of type II diabetes in rats indicated that the agent can interfere with glucose metabolism under certain conditions that also might affect the extent of brain injuries. 37
Thus, as a carrier, Intralipid may confound and/or mask the effects of PROG given to patients in the acute stage of the injury cascade. The present study was designed to test the effects of Intralipid infusion, given with PROG, on edema following TBI in rats. This is the first pre-clinical study to evaluate the efficacy of PROG administered IV with Intralipid.
Methods
Twenty-three male SD rats weighing 300–350 g at the time of injury were used. All experimental animal procedures were approved by the Emory University Institutional Animal Care and Use Committee (Protocol # 2002865). Controlled cortical impact (CCI) was induced as previously described. 38 Under aseptic conditions, a midline incision was made, the skin was retracted and a 5-mm diameter mid-sagittal bilateral craniotomy 3 mm anterior to bregma was created. The bone cap was carefully removed. CCI to the medial frontal cortex was induced as previously described 38 using a magnetic cortical pinpoint contusion impactor (4-mm diameter; PC1300; Hatteras Instruments, Cary, NC) to a depth of 2.5 mm at a pressure of 1.7 psi, impact time of 100 msec, and velocity of 2.26 m/sec. The incision was sutured after bleeding stopped. Animals were allowed to recover from the anesthesia before being returned to their home cages. Animals were randomly assigned to one of four groups: sham (n = 5), controlled TBI (n = 6), Intralipid (n = 6), and Intralipid+PROG (n = 6).
Since PROG is soluble only in alcohol, we used 95% ethanol to compound the PROG solution. Stock solutions of PROG (4 mg/mL) were made by diluting the ethanol stock solution (40 mg/ml; ethanol:Intralipid = 1:9). A dosing worksheet based on body weight and final PROG concentration (8 mg/kg) was used to determine the volume of stock solution required to be diluted in Intralipid for a standard infusion rate (1.2 mL/h). Following CCI, the rats' femoral vein was catheterized and Intralipid solution (Fresenius Kabi, Bad Homburg, Germany) with or without PROG was given via femoral vein with an injection pump over a period of 1 h.
Animals were euthanized at 24 h post-injury and their brains extracted and dissected into anterior and posterior sections. The anterior section contained the entire lesion area; the posterior distal section was taken remote from the injury. Sections were placed in a pre-labeled and pre-weighed tube that was immediately capped. Tubes were reweighed, opened, and placed in a 60°C oven with 15 mm Hg vacuum pressure for 48 h. Samples were reweighed after drying. All weighing was done on the same balance. The percent water content was calculated by [(wet wt - dry wt)/wet wt] *100. The percent difference in water content between the anterior peri-contusional and the posterior distal section was calculated for each sample by: [(anterior H2O% - posterior H2O%)/ (posterior H2O%)] *100.
Results
We evaluated the neuroprotective actions of PROG on edema attenuation following TBI when administered via Intralipid infusion. Intralipid did not change the level of TBI-induced edema at 1 h post-TBI. PROG treatment significantly (p < 0.05) attenuated edema level when infused with Intralipid (Fig. 1). We observed a significant (F [3,22] = 28.22; p < 0.01) increase in brain water content in all injured groups: controlled TBI alone (4.08 ± 0.38), Intralipid alone (3.69 ± 0.58), and Intralipid+PROG (2.28 ± 0.43), compared with uninjured untreated shams (−0.76 ± 0.20) at 24 h post-TBI. No significant difference was found between the TBI-alone and Intralipid groups.
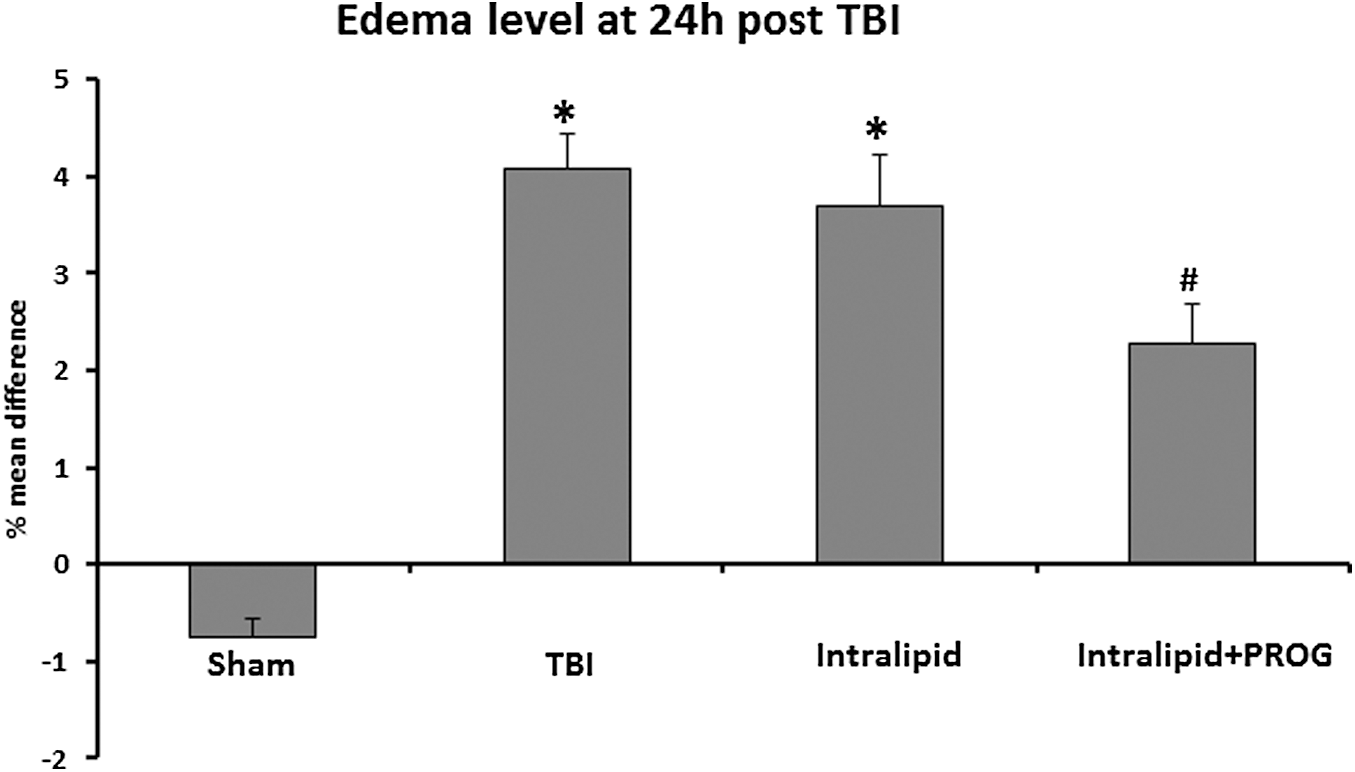
Effect of progesterone administered with Intralipid infusion on edema level at 24 h post–traumatic brain injury (TBI). Brains of all injured groups were higher in brain water content, compared with the sham group. Treatment with progesterone via Intralipid infusion significantly reduced edema. Values are expressed as mean ± standard error. *TBI and Intralipid vs. Sham; #TBI vs. Intralipid + progesterone (PROG).
Discussion
Our result is consistent with previous studies that reported edema-attenuating effects of PROG in a number of animal models of brain injury. 6,39 An inverse correlation between serum PROG level and degree of edema also has been reported. 40 In previous studies evaluating edema by measuring brain water content after CCI in rats, a number of PROG analogs showed efficacy in reducing edema. 38,41,42
The extent, time course of drug action, and distribution pattern of a drug can be markedly affected by the route of administration. Two small single-center clinical studies have shown positive outcomes with oil-based intramuscularly administered low-dose PROG, 43 –45 but large phase III clinical trials using IV administration at much higher doses in lipid carriers had negative results. 22,23 The first trial using intramuscular (IM) injection was a phase II, single-center, 1:1 randomized trial conducted in Hangzhou, China, 43 which enrolled 159 male and female adult patients with severe TBI (GCS 3–8) who received blinded treatment with PROG or vehicle (1 mg/kg). PROG was given by IM injection in camellia oil vehicle within 8 h after injury and then once every 12 h for 5 days at 2 mg/kg/day. Primary neurological outcomes were Glasgow Outcome Scale (GOS) scores dichotomized into favorable or unfavorable outcomes. At both 3- and 6-month follow-ups, the patients treated with PROG had significantly better GOS and Functional Independence Measure scores and mortality. The second prospective, single-blinded trial using the IM route was done in Iran. Forty-eight males, 18–60 years of age, with diffuse axonal injury (DAI), GCS scores ≤12, and admission within 4 h of injury were randomly assigned to PROG or control groups. The protocol followed the same treatment schedule of PROG (1 mg/kg) every 12 h for 5 days. The results of the study showed that the neurologic outcome improved in PROG-administered DAI patients, probably through modulation in cytokine levels.
Chronic administration of Intralipid can elevate lipoproteins and may affect the pharmacological behavior of drugs given to patients. Given its lipid-based composition and its effect on build-up of intracellular cholesterol, 33 the use of Intralipid vehicle in relatively large volume for a condition like stroke should be undertaken with caution. Monitoring of lipoprotein levels in patients during treatment for TBI or stroke also may be important for evaluating drug efficacy.
In this study, we used a much smaller volume and duration of Intralipid+PROG infusion compared with that used in the clinical trials, a limitation which precludes drawing definite conclusions about the possible effect of lipid infusion on PROG's efficacy. However, our results can be taken to suggest that an Intralipid infusion of short duration and low volume did not confound or mask the beneficial effect of PROG on edema reduction in the TBI model we used. Although measurement of edema is useful in evaluation of acute efficacy, it alone cannot provide a prognosis concerning the extent of, and recovery from, cognitive, sensory, and motor deficits. It will be important also to evaluate the effects of Intralipid infusion given with PROG on molecular and long-term behavioral outcome measures previously used to show PROG effectiveness.
Much has been learned from the large but problematic trials besides the fact that more comprehensive and quantitative assessments are needed. If PROG is to be conclusively tested as a treatment for TBI, a carefully selected and targeted population must be tested in a phase IIB trial for dose and duration optimization with a suitable vehicle control to determine optimal treatment parameters for any future phase III trials. If at all possible it would be even better to include or stratify for sex and age differences as separate categories for patient selection.
Footnotes
Acknowledgments
The authors would like to thank Leslie McCann for editorial suggestions.
Author Disclosure Statement
DGS and IS, along with Emory University, retain patents related to the use of progesterone and its uses but they have no financial gains, royalties or licensing agreements from research on progesterone. BW reports no competing financial interests.