
Abstract
The objective of this prospective cohort study was to evaluate the probability of employment and predictors of employment in patients with moderate- to- severe traumatic brain injury (TBI) over 10-year follow-up. One hundred nine patients (18–67 years) were included with follow-up measurements 3, 6, 12, 18, 24, and 36 months and 10 years post-TBI. Potential predictors of employment probability included patient characteristics, injury severity factors, functional outcome measured at discharge from the hospital with the Glasgow Outcome Scale (GOS), Barthel Index (BI), Functional Independence Measure (FIM), and the Functional Assessment Measure (FAM). Forty-eight patients (42%) completed the 10-year follow-up. Three months post-TBI, 12% were employed, which gradually, but significantly, increased to 57% after 2-years follow-up (p < 0.001), followed by a significant decrease to 43% (p = 0.041) after 10 years. Ten years post-TBI, we found that employed persons had less-severe TBI, shorter length of hospital stay (LOS), and higher scores on the GOS, BI, FIM, and FAM at hospital discharge than unemployed persons. No significant differences in age, sex, educational level, living with partner/family or not, pre-injury employment, professional category, psychiatric symptoms, or discharge destination were found. Longitudinal multivariable analysis showed that time, pre-injury employment, FAM, and LOS were independent predictors of employment probability. We concluded that employment probability 10 years after moderate or severe TBI is related to injury severity and pre-injury employment. Future studies on vocational rehabilitation should focus on modifiable factors and take into consideration the effects of national legislation and national labor market forces.
Introduction
W
The current study focuses on employment status 10 years after sustaining moderate or severe TBI. Many studies on employment post-TBI have been published with mixed results. Patient mix, definitions of outcome variables, assessment methods, and study design may differ substantially between studies, which may hinder comparing the outcomes. Several studies use a retrospective or cross- sectional design. 9 –11 Prospective studies often have a follow-up limited to 1 year post-TBI or sometimes to 3 or 5 years post-TBI. 12 –16 Prospective studies with a 10-year follow-up are scarce.
Cuthbert and colleagues prospectively followed 3618 moderate-to-severe TBI patients up to 10 years post-onset. 17 The patients in this study were not retired at injury, received inpatient rehabilitation at a Traumatic Brain Injury Model System center, were discharged between 1989 and 2009, and had at least three complete follow-up interviews at post-injury years 1, 2, 5, and 10. The researchers developed a model to predict individual employment outcome. 17 They describe an overall decline in trajectories of probability of employment between 5 and 10 years post-injury. 17 Age, sex, race/ethnicity, education, pre-injury substance abuse, pre-injury vocational status, and days of post-traumatic amnesia (PTA) were identified as predictors of being employed in the long term. 17 In Dahm and colleagues, shorter PTA and younger age were associated with higher employment rates in a prospectively followed cohort of 97 mild- to- severe TBI patients (who were compared with 91 patients with orthopedic injuries) over 10-year follow-up. 18 They reported a 10-year employment rate of 50.5%.
We previously reported the 3-year outcomes of the Rotterdam TBI study, a prospective cohort study of outcome after moderate and severe TBI. 7,16,19 We found that employment rate dropped from 80% pre-injury to 55% over 3-year follow-up and that unemployment could be predicted using the Functional Assessment Measure (FAM) at hospital discharge. 16 The aim of the present study was to evaluate employment outcome and its predictors up to 10 years post-injury.
Methods
Procedure
The design of the Rotterdam TBI study has been described before. 7,16,19 In short, after informed consent and with approval of the Medical Ethics Committee (MEC), patients with moderate or severe TBI were consecutively enrolled between January 1999 and April 2004 at three Dutch level 1 trauma centers and prospectively followed. Measurements were completed at hospital discharge and at 3, 6, 12, 18, 24, and 36 months post-TBI. In 2012, the Rotterdam TBI Study was extended with a 10-year follow-up visit, which was approved by the MEC. New informed consent was obtained from all participants.
Participants
Inclusion criteria were admission to a hospital for moderate (Glasgow Coma Scale [GCS] score of 9–12) or severe (GCS score of 3–8) TBI attributed to a nonpenetrating trauma and age at injury between 16 and 67 years. Exclusion criteria were inadequate knowledge of the Dutch language to participate in the study or important pre-traumatic neurological, oncological, or systemic impairments (e.g., spinal cord injury, psychiatric disorder, and cancer) that may interfere with TBI-related disability assessment. Follow-up measurements were excluded from patients who reached the age of 67 during follow-up.
Measurement instruments
Primary outcome
The primary outcome measure was status of employment. Data on employment outcome were collected at each visit by means of a structured interview by a trained research psychologist. This interview included questions on employment status (yes/no) and type of work. Employment included all payed vocational activities at the time of measurement. Unemployment was defined as any voluntary vocation without payment, including students, homemakers, early retirement, sick leave, and other. The type of work was classified into four categories: professional/managerial (executive, administrative, and managerial functions and professional specialties); skilled (technicians and administrative support, precision production, craft, and repair personnel); manual labor (machine operators, assemblers, transporters, and cleaners); and unemployed or student. 20
Covariates
Sociodemographic data were collected at enrollment in the study and during follow-up. Sociodemographic data included age at injury, sex, marital status (living together vs. alone), education (at least high school vs. less), and pre-injury employment status (employed vs. unemployed). Clinical data were collected from the medical records during hospitalization and at hospital discharge. Severity of TBI was based on the GCS, defining moderate TBI as a GCS of 9–12 and severe TBI as a score of 8 or less. The GCS was determined as the lowest score in the first 24 hours post-TBI measured in the hospital. Presence (yes/no) and type of psychiatric symptoms were observed during hospitalization by the medical staff and also recorded at each follow-up visit by the research psychologist in a structured interview, which included self-reported depression, anxiety, and other serious psychiatric symptoms.
Functional outcome was assessed with the Functional Independence Measure (FIM), FAM, Glasgow Outcome Scale (GOS) and the Barthel Index (BI) at hospital discharge. 21,22 The FIM and FAM have a good reliability and validity. 22,23 The FIM evaluates motor functioning with respect to self-care, sphincter control, transfers, and locomotion, whereas FAM evaluates cognitive and communication functioning and psychosocial adjustment. Together, they consist of 30 items, 18 of the FIM and 12 of the FAM, that are evaluated on a 7-point scale. The FIM score ranges from 18 (totally dependent) to 126 (totally independent), and the FAM score ranges from 12 (totally dependent) to 84 (totally independent). The research psychologists were qualified FIM/FAM assessors. The GOS measures general outcome post-TBI and consists of five categories: death, vegetative state, severe disability, moderate disability, and good recovery. 23,24 The BI also has a good reliability and validity. 25 It consists of 10 items on activities of daily living (e.g., making transfers, dressing, bathing, and bowel and bladder status), each with two, three, or four response categories (0–3 points). Total scores range from 0 (severely restricted) to 20 (no restrictions). Finally, the hospital discharge destination (home, rehabilitation institute, or nursery home) was recorded.
Statistical analysis
Descriptive data are presented as the means and standard deviations (SDs) of interval variables and the numbers and proportions of categorical variables. Variables of interest included patient characteristics (age, sex, partner, educational level, and injury severity variables: length of hospital stay [LOS], TBI severity [moderate {GCS 9–12} or severe {GCS 3–8}], presence of psychiatric symptoms [yes/no], and employment variables [pre-injury employment, occupational category]) and functional outcomes at hospital discharge (GOS, BI, FIM, and FAM). Differences between patients that were included and patients that were lost to follow-up were analysed using χ2 or exact tests for categorical data and independent-samples t-tests for interval variables. The same statistical tests were used to compare the two subgroups of persons who were employed and those who were unemployed in a cross-sectional analysis at 10 years post-injury.
The longitudinal pattern of the probability of employment over 10-year follow-up time was estimated using generalized estimating equations (GEEs) to fit a logistic regression analysis with repeated measurements. This analysis takes into account that multiple measurements within subjects are correlated using an unstructured covariance structure. This method is very flexible in handling missing values. Thus, all available measurements of the total cohort (N = 109) were included in this GEE analysis, in which employment status depended on the measurement time post-TBI in years (0.25, 0.5, 1, 1.5, 2, 3, and 10 years, respectively). In post-hoc analyses, the differences between measurements were evaluated using pair-wise comparisons.
We also used GEE analyses to evaluate the effect of potential predictors, that were measured at baseline, on the probability of employment over 10-year follow-up. We first fitted a quadratic unconditional model to the data by adding time and time squared as predictors of employment status to the model. Next, we evaluated the effects of the covariates that differed significantly between the employed and unemployed subgroups on employment outcome over time. Because of missing values in some of the covariates at hospital discharge, the first follow-up outcomes of the FIM, FAM, BI, and GOS were used instead in some cases. Variables that were not significant were removed from the multivariable model one by one. The final multivariable model included all significant predictors. Statistical analyses were performed using SPSS for Windows software (version 21.0; SPSS, Inc., Chicago, IL). A significance level of 0.05 was used in all analyses.
Results
Study population
Of 549 patients screened, 153 patients died and 229 were excluded (Fig. 1), which left 167 eligible patients, from which 113 were willing to take part in the Rotterdam TBI study. 16 Four patients (4%) were excluded because they reached the age of retirement during follow-up. Thus, 109 patients remained in the cohort. After 3 years, 19 patients were lost to follow-up (17%). Between 3- and 10-year follow-up, 7 patients died (7%), 20 were no longer willing to participate (21%), and 15 could not be traced (16%). Thus, 48 patients participated in 10-year follow up. Patients who were lost to follow-up (n = 61) did not differ significantly from patients with complete follow-up in baseline characteristics, except for pre-injury employment status (Table 1). Patients with complete follow-up were more often employed pre-injury than those who were lost to follow-up (90% vs. 75%; p < 0.048). Baseline characteristics, hospital discharge outcomes, and discharge destinations are presented in Table 1.
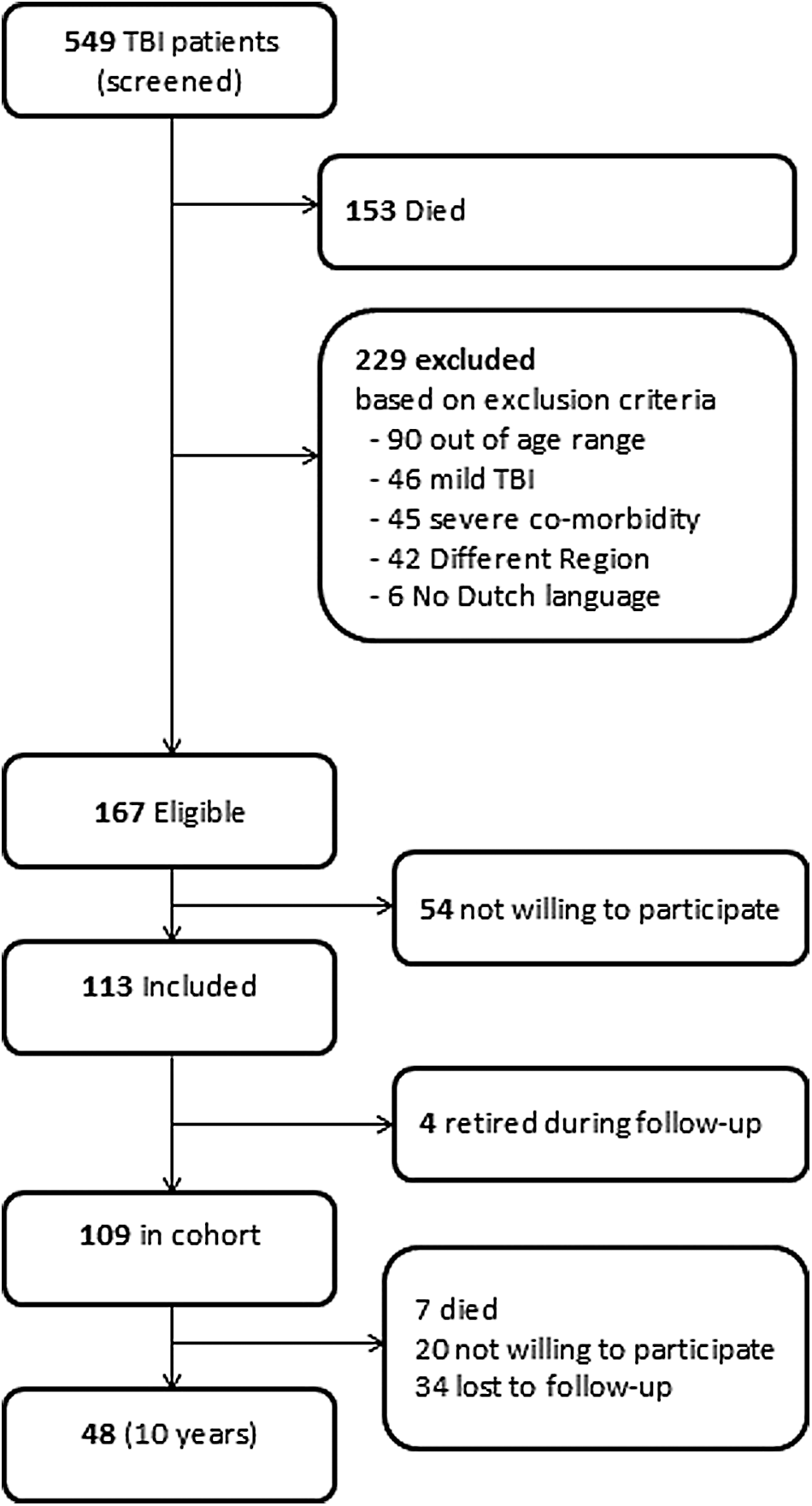
Flow chart of patient inclusion and participation. TBI, traumatic brain injury.
Number of missings in included and lost patients, respectively: employed pre-injury: 0, 2; occupational category pre-injury: 0, 3; FIM: 7, 11; FAM: 8, 11; BI: 11, 13; GOS score: 8, 13.
p < 0.048 included versus lost.
TBI, traumatic brain injury; SD, standard deviation; GCS, Glasgow Coma Scale; FIM, Functional Independence Measure; FAM, Functional Assessment Measure; BI, Barthel Index; GOS, Glasgow Outcome Scale; FU, follow-up.
Cross-sectional employment outcome 10 years after traumatic brain injury
In the cross-sectional analysis of the 10-year follow-up data, we found that 26 persons of 48 (55%) were employed. Further, we found that patients who were employed 10 years post-TBI differed significantly from those who were unemployed regarding severity of TBI and hospital discharge outcomes (Table 2). Employed persons had significantly less-severe TBI, a shorter LOS, and higher scores on the GOS, BI, FIM, and FAM at hospital discharge than persons without employment in the long term. Cross-sectionally, there were no significant differences between the groups in age, sex, educational level (high school or not), living with partner or family or not, pre-injury employment, professional category, psychiatric symptoms, or the different hospital discharge destinations (home, rehabilitation center, or nursing home).
Number of missings in employed and unemployed respectively: FIM: 4, 3; FAM: 5, 3; BI: 6, 5; GOS score: 4, 4.
p value <0.05.
SD, standard deviation; TBI, traumatic brain injury; GCS, Glasgow Coma Scale; FIM, Functional Independence Measure; FAM, Functional Assessment Measure; BI, Barthel Index; GOS, Glasgow Outcome Scale.
Longitudinal analysis of employment status and its predictors
In the longitudinal GEE analysis with repeated measurements, taking into account all available data of the cohort (N = 109) and the covariance between measurements, we found that the estimated employment probability at 10-year follow-up was 43%. The estimated employment probabilities at each follow-up time are presented in Figure 2. This figure shows that the probability of employment dropped from 80% pre-injury to 12% at 3-month follow-up and gradually increased to 57% at 2-year follow-up, after which it decreased to 43% at 10 years post-TBI. The employment probability significantly increased between 3 months and 1 year (mean difference, 0.34; p < 0.001) and decreased significantly between 2 and 10 years post- injury (mean difference, 0.14; p = 0.041). In Figure 2, also the quadratic model without covariates is presented.
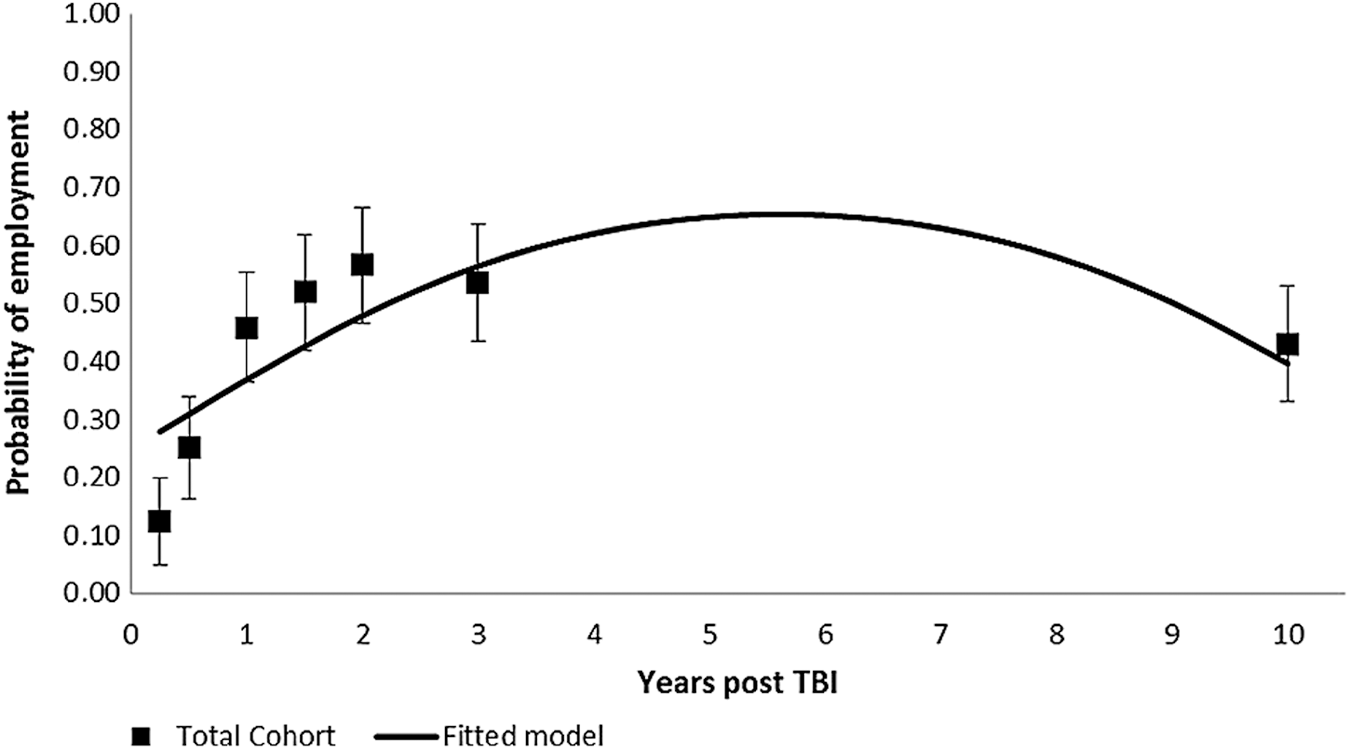
Probability of employment (estimated means and 95% confidence intervals) over 10-year follow-up and fitted model for the total cohort. TBI, traumatic brain injury.
Table 3 presents the parameters of the final multivariable GEE model. Time post-TBI, pre-injury employment, the FAM and LOS were found to be independent predictors of the probability of employment 10 years post-TBI. The model shows that the probability of being employed was significantly better for patients with pre-injury employment, higher cognitive functioning score at hospital discharge, or shorter LOS (Table 3). In Figure 3, the trajectories for two subgroups of pre-injury employment are presented, in which the solid line presents a subgroup of persons who were employed pre-injury, with a mean FAM score of 68.4 and a mean LOS of 30.9 days, whereas the dotted line presents a subgroup of unemployed persons pre-injury with a mean FAM score of 57.0 and a mean LOS of 45.6 days.
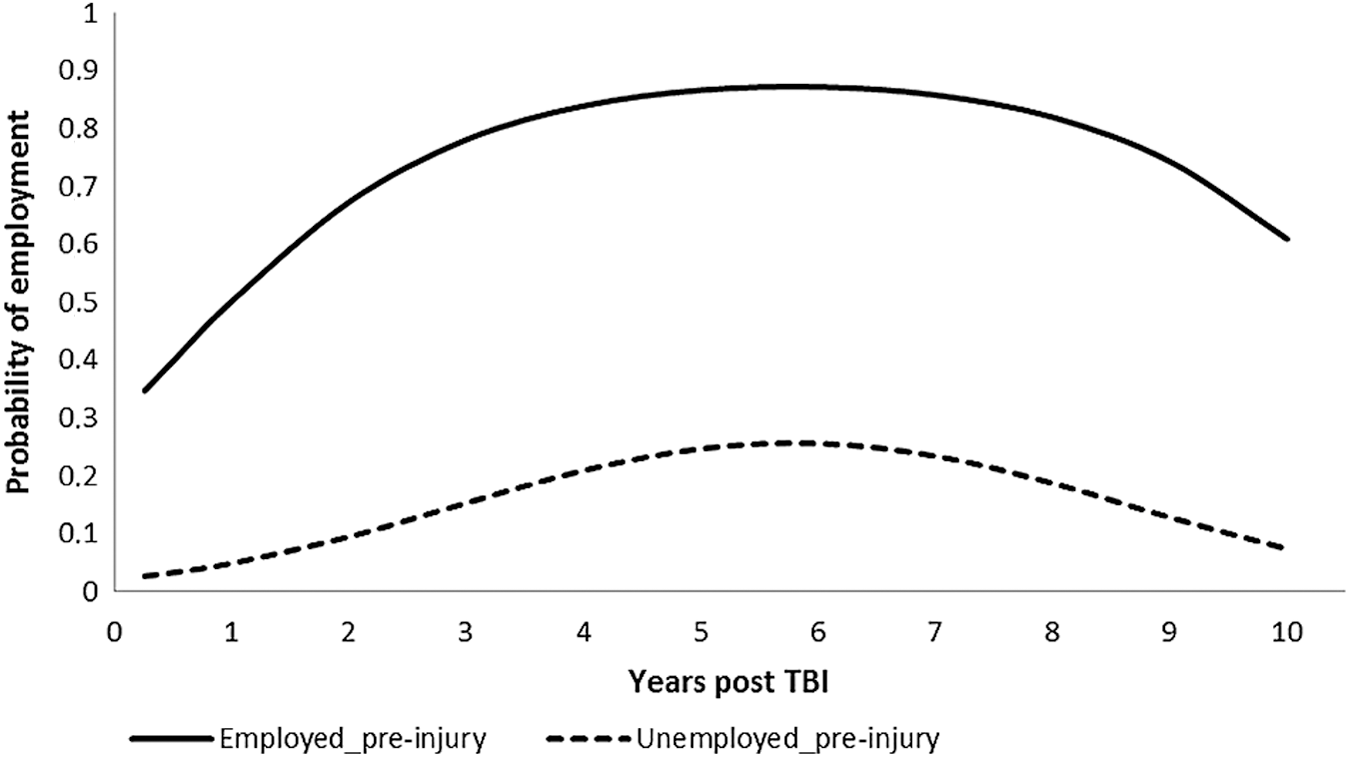
Probability of employment for persons who were employed pre-injury (solid line) and unemployed pre-injury (dotted line). TBI, traumatic brain injury.
Discussion
In this prospective 10-year follow-up study on patients with moderate and severe TBI, we found that, after an initial increase in the first 2 years post-TBI, the probability of employment stabilizes and decreases in the long term. The current study is unique for the fact that it contains many measurements in the first 3 years, in which most recovery takes place. These early extensive measurements enabled us to accurately predict outcome over 10 years despite the inevitable loss to follow-up in a 10-year follow-up study. Taking into account all measurements of the initial cohort, we estimated the 10-year probability of employment to be 43%, which is lower than the employment probability we found in cross-sectional analysis (55%). This study shows that the 10-year employment rate in a cross-sectional analysis will be overestimated if more persons who were unemployed pre-injury dropped out.
Using statistical modeling, we found that a quadratic model best fitted these data, indicating an increase of the probability of employment in the first 2 years, which levels off and is followed by a decrease later in time. Forslund and colleagues found no relationship between employment probability and time in a similar cohort in Norway with measurements at 1, 2, and 5 years post-TBI. 15 This is not in conflict with our results, because most of the improvement over time was found in the first year in our study, when no measurements were done in the Norwegian study. Our long-term results are in accord with the large American cohort study described by Cuthbert and colleagues, who demonstrated a decline in trajectories of employment between 5 and 10 years post-injury. 17
Comparing our study with the results by Cuthbert and colleagues, we provide more-detailed information and more-extensive measurements in the first 3 years, which is important for long-term statistical modeling. This study concerns Dutch/European patients and confirms the results found in the American population investigated by Cuthbert and colleagues.
Comparing those who were employed 10 years post-injury with those who were unemployed in a cross-sectional analysis, we found that the latter group had more-severe TBI, a longer LOS, and worse functional outcomes at hospital discharge, as measured by the FIM, FAM, BI, and GOS. We did not find significant differences in age, sex, partner status, educational level, or type of occupation. A higher injury severity and poorer outcome in terms of impairments were predictive of long-term unemployment. This is in line with earlier findings that identified low GCS scores and longer PTA as predictors of employment probability. 15,17,18 In longitudinal analyses, we demonstrated that from the functional outcome measures, the FAM, measuring cognitive functioning, was the best predictor of long-term probability of employment, in addition to LOS and pre-injury employment status, which confirms the findings of our previous study. 16 Based on these predictors, two different scenarios illustrated how these variables impact the probability of employment in the long term. In other long-term follow-up studies, functional outcomes at hospital discharge are not often used as potential predictors of employment outcome. In a recent systematic review, there was weak evidence that the Disability Rating Scale has predictive value for RTW. 26
The current study shows that injury severity and functional factors, rather than personal and contextual factors (such as age, sex, being single, type of occupation, and education level), independently predicted employment status over 10 years follow up. Previous studies did show that contextual factors, such as type of medical insurance, may be associated with long-term employment status. 15,17 Cuthbert and colleagues suggest that employment status after moderate and severe TBI is also influenced by national labor market forces, which may explain different outcomes between countries. 17 Age (older than 40 years) has been shown to be a significant predictor of unemployment. 18,27,28 Age may both be related to a poorer outcome post-TBI, in terms of survival and disability, and may be considered a contextual determinant given that employment rates may also drop with increasing age for healthy persons. 29,30 The employment rate in the general Dutch population is lower for those between 55–65, compared to 45–55, years of age. The difference varies from 25–40% over the study years, with a consistently lower employment rate for the eldest group. 31
National regulations and labor market forces have to be taken into account in planning vocational rehabilitation programs and should also be considered in interpreting the employment rate in nationally oriented research/literature. Global, but also local, economic factors might influence the employment rate, especially if a longer time period is being investigated. To rule out national regulations, labor market forces, and local economic factors as much as possible, internationally oriented TBI research on employment outcome is needed.
The prospective study design and long-term follow up are a strength of this study. However, in cross-sectional analyses, selection bias may be a limitation. Of 167 eligible patients, 113 agreed to participate with a loss to follow-up of 17% after 3 years and 56% after 10 years. Patients who were lost to follow-up were more often unemployed pre-injury. Taking into account the within-person correlations between measurements, we found that the estimated 10-year employment probability was overestimated in the cross-sectional analysis. Although we adjusted our longitudinal analyses for pre-injury employment status and covariance between measurements, the 10-year employment rates may still be optimistic. Further, the data did not allow for detailed conclusions, such as whether a patient returned to his previous work, whether the level and extent of preinjury employment differed from follow-up, and whether there was a change in income over the years.
Conclusion
A dose-response relationship between TBI severity and mortality or long-term disability has been described before. 15 –17,27,29,30 The results of our study underscore that this relation also accounts for employment outcome 10 years after sustaining a moderate or severe TBI. Employment probability over a long follow-up time may be influenced by national regulations, labor market forces, and local, but also global, economic factors, which pleads for internationally oriented TBI research on employment outcome. Future studies on vocational rehabilitation should focus on modifiable factors and take into consideration the effects of national legislation and national labor market forces.
Footnotes
Acknowledgments
This study was financially supported by the Netherlands Organization for Health Research and Development (project no.: 1435.0020). We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated.
Author Disclosure Statement
No competing financial interests exist.