
Abstract
Individuals with cervical spinal cord injury (SCI) have impaired thermoregulatory mechanisms attributed to interruption of motor, sensory, and autonomic neuropathways. To determine the effects of heat exposure on core body temperature (Tcore) and cognitive performance in persons with tetraplegia, 8 individuals with chronic tetraplegia (C3–C7, American Spinal Cord Injury Association Impairment Scale A–B) and 9 able-bodied controls were acclimated to 27°C at baseline (BL) before being exposed to 35°C for up to 120 min (Heat Challenge). Rectal temperature (Tcore), distal skin temperatures (Tskavg), sweat rate (QSavg), microvascular skin perfusion (LDFavg), and plasma norepinephrine (NE) were measured. Cognitive performance was assessed using Stroop Color and Word and Wechsler Adult Intelligence Scale-Fourth Edition Digit Span tests at BL and at the end of Heat Challenge. After Heat Challenge, Tcore increased 0.78 ± 0.18°C (p < 0.001) in tetraplegics after an average of 118 ± 5 min. Tcore did not change in controls after 120 min. The increase in QSavg was larger in controls than in tetraplegics (946 ± 672% vs. 51 ± 12%; p = 0.007, respectively). LDFavg increased only in controls (109 ± 93%; p = 0.008). Tskavg appeared to increase less in tetraplegics than in controls. Plasma NE levels remained lower in tetraplegics compared to controls after Heat Challenge (86 ± 64 vs. 297 ± 84 pg/mL, respectively; p < 0.001). Stroop Color, Interference, and WAIS-IV Sequence scores increased only in tetraplegics (19.4 ± 17.2%; p < 0.05, 8.3 ± 5.9%; p < 0.05, 29.1 ± 27.4%; p < 0.05, respectively). Dysfunctional thermoregulatory mechanisms in the tetraplegic group allowed Tcore to rise from subnormal levels to normothermia during heat exposure. Normothermia was associated with improvements in attention, working memory, and executive function.
Introduction
T
Spinal cord injury (SCI) impairs autonomic, sensory, and motor pathways, significantly impacting mobility, internal organ function, and metabolic homeostasis. In the United States alone, the estimated occurrence of new SCI is 17,000 cases each year with approximately 282,000 people currently living with SCI. 7 Average lifetime costs for medical care and living expenses for a person with incomplete tetraplegia, the most common neurological form of SCI, is approximately $3 million. 7
After SCI, central regulation of sympathetically mediated heat dissipating mechanisms is interrupted. 8 –10 The impaired abilities to sense changes in ambient temperature, effectively sweat, and vasodilate below the level of lesion in persons with tetraplegia allow even mildly hot ambient temperatures to cause Tcore to rise above normothermia. 9,11 –13 These impairments, combined with restricted mobility, create a vulnerability to hyperthermia, the risk of which is greater in persons with tetraplegia (cervical SCI) than persons with paraplegia (thoracic SCI) because of the more extensive interruption of autonomic thermoregulatory mechanisms.
Several studies have documented declines in various aspects of cognitive performance with passive heat exposure in able-bodied (AB) subjects. 14 –17 Simmons and colleagues raised Tcore of AB subjects to mild hyperthermia, an increase of ∼1°C, by passive exposure to ambient temperatures of 45°C. 16 Although response times increased, accuracy of responses declined secondary to decreased attention. Racinais and colleagues and Gaoua and colleagues demonstrated declines in working memory in AB subjects with hyperthermia induced by passive exposure to 50°C. 14,18 Sun and colleagues also exposed AB subjects to 50°C and demonstrated declines in executive function with the hyperthermia induced by this intense heat. 17
Cognition determines how we interact with other individuals and our surroundings. Cognitive performance refers to how quickly and accurately we can acquire, process, and utilize knowledge. It includes processes of attention, the ability to maintain awareness of specific stimuli, sensations, or thoughts while disregarding others 19,20 ; memory, processes of information registration, retention, and recognition, which may be divided into short-term or working memory and long-term memory 19 ; and executive function, the highest order of cognitive function, the ability to critically judge situations, manipulate abstract information to solve complex problems, and direct behavior. 21
Despite the prevalence of SCI, its associated thermoregulatory dysfunction, and the acknowledged sensitivity of the metabolism and synaptic transmission of the central nervous system to temperature change, 22 there are no studies that address the effect of heat exposure on Tcore and associated cognitive function in persons with SCI.
Methods
Subjects
Seven males and 1 female with chronic tetraplegia (International Standards for Classification of Spinal Cord Injury level of injury C3–C7, American Spinal Cord Injury Association Impairment Scale [AIS] A & B [A = 5, B = 3]) and 9 age- and sex-matched non-SCI controls were recruited for the study (Tables 1A and 1B). The study was approved by the institutional review board of the James J. Peters Veterans Affairs Medical Center (Bronx, NY). Written informed consent was obtained from each subject before study participation.
NLI, neurological level of injury; AIS, American Spinal Cord Injury Association Impairment Scale for eight subjects with tetraplegia.
Group averages (± standard deviations [SD]) for age (in years), height (in meters), and weight (in kilograms).
BMI, body mass index (in kg/meter2); DOI, duration of injury (in years) for 8 subjects with tetraplegia and 9 able-bodied control subjects; NS, not significant; NA, not applicable.
Subjects were excluded if they reported or had a history of heart, kidney, peripheral vascular, or cerebral vascular disease; traumatic brain injury; diagnosed cognitive impairment; color blindness; hypertension; untreated thyroid disease; diabetes mellitus; acute illness or infection; dehydration; and/or smoking.
Research design
A prospective, two-group comparative study was performed to determine the effect of a warm thermal challenge on Tcore and cognitive performance, our primary outcome measures. Secondary outcome measures included those of average distal skin temperature (Tskavg) and thermal sensitivity (TS) to assess the effects of interruption of vasomotor control and impairment of perception of heat, respectively. Upper extremity (UE) and lower extremity's (LE) average sweat rate (QSavg), distal UE and LE average microvascular perfusion (LDFavg), systolic blood pressure (SBP), and plasma norepinephrine levels (NE) were measured to assess sympathetic modulation of sweat production, cutaneous microvasculature, and the general integrity of the sympathetic nervous system.
Procedures
Subjects' responses to a thermoneutral environment (27°C, 35% relative humidity, air speed <0.1 m/s) were measured for 15 min at baseline (BL) before being exposed to the Heat Challenge (35°C) for up to 120 min. Duration of the Heat Challenge was reduced if subjects' Tcore reached 38°C and/or if subjects reported discomfort. Before baseline data collection, participants rested in the same thermoneutral environment for 30 min to allow for acclimation.
Subjects were seated for the duration of the study. Subjects with SCI used their own wheelchairs whereas non-SCI subjects were provided with a wheelchair. Wheelchairs were equipped with a Roho High-Profile dry flotation seat cushion (The Roho Group, Belleville, IL) for air circulation and prevention of skin breakdown. Male subjects wore only shorts and females wore a sports bra and shorts; the extremities were partially extended and positioned away from the body to allow for maximal skin exposure to the ambient temperature.
Tcore was measured by a rectal thermocouple (RET-1; Columbus Instruments, Columbus, OH) placed 10 cm beyond the anal sphincter. Tsk was measured with surface thermocouples (TX-4 Skin Surface Probes; Columbus Instruments) taped to 15 sites above and below the level of lesion: forehead; left axilla; right proximal triceps; dorsal surface of both hands; palmar surface of both middle fingers; upper and lower chest; proximal thighs; dorsal surface of both feet; and plantar aspect of both halluces (Fig. 1). Rectal and skin temperatures were continuously collected by the Iso-Thermex Multichannel Thermometer (Columbus Instruments). Distal vasculature flow was measured by laser Doppler flowmetry (LDF; Periflux System 5000; Perimed, Stockholm, Sweden) using laser probes taped to the dorsal surface of both hands and both feet. QS was measured by the Quantitative Sweat Measurement System (WR Medical Electronics, Stillwater, MN) with capsules secured to four sites: left upper arm, left forearm, left mid-thigh, and left mid-calf (C5, T1, L3, and L5 dermatomes, respectively). Blood pressure (BP) and heart rate were monitored using a GE Carescape V100 vital signs monitor (GE Healthcare, Buckinghamshire, UK). TS was assessed by asking the subject to grade their perception of heat on the Zhang rating scale of thermal comfort from −4 (very cold) to +4 (very hot). 23,24 Venous blood was drawn into heparinized tubes, centrifuged to separate formed blood cell elements from plasma, and assayed for NE concentrations by using high-performance liquid chromatography methodology.

Illustration of the sites used for placement of the 15 surface thermocouples: forehead; left axilla; right proximal triceps; dorsal surface of both hands; palmar surface of both middle fingers; upper and lower chest; proximal thighs; dorsal surface of both feet; and plantar aspect of both halluces.
BL data were collected for 15 min. During this period, Tcore, Tsk, and QS were collected continuously. LDF was measured in 5-min durations at 5-min intervals, at the beginning and end of BL. Heart rate, BP, and TS were measured at 10-min intervals. A venous blood sample for plasma NE concentrations was obtained once at BL. At the end of the BL period, all subjects were administered a neuropsychological battery to assess cognitive performance. The battery consisted of the Stroop Color and Word Test to assess attention, processing speed, and executive function and the Digit Span section of the Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV) to assess attention and working memory.
After completing the neuropsychological battery, subjects remained seated and were transported from the thermoneutral room to the adjacent pre-heated chamber (35°C, 35% relative humidity, air speed <0.1 m/s). Data collection resumed and was performed in an identical manner as during the BL period. Tcore and Tsk were collected continuously throughout the Heat Challenge. Heart rate, BP, and TS were measured at 10-min intervals; QS was measured in 15-min durations at 30-min intervals; LDF was measured in 5-min durations at 30-min intervals. Venous blood samples were drawn twice at 50-min intervals. At the end of the Heat Challenge, or if Tcore reached 38°C, subjects were administered the same neuropsychological battery that was administered during the BL period, except during heat exposure.
After the Heat Challenge, subjects were returned to the thermoneutral room (27°C) and provided with ice water. Subjects were monitored until their Tcore returned to BL values.
Statistical analysis
A two-group (tetra, AB) by two-condition (BL, Heat) mixed model analysis of variance was used to determine main and interaction effects for each of the physiological and cognitive outcome measures. If significant main or interaction effects were found, post-hoc analyses with paired and independent t-tests were used to determine within- and between-group differences, respectively.
To analyze the thermal sensitivity data, the Wilcoxon signed-rank test was used for within-group comparisons (BL to Heat Challenge) whereas the Mann-Whitney U test was used for between-group comparisons. The threshold for significance was set at p < 0.05 for all comparisons.
Results
Baseline (27°C)
The groups were not significantly different for age, height, weight, or body mass index (BMI; Table 1B). Baseline values were not significantly different between the tetraplegic and control groups for Tskavg, QSavg, LDFavg, or TS ratings. However, Tcore for the tetraplegic group was significantly lower than that of the control group (36.9 ± 0.3°C vs. 37.3 ± 0.3°C, respectively; p < 0.013; Table 2A). Additionally, plasma NE levels were significantly lower in the tetraplegic group than in the control group (83.5 ± 65.0 vs. 329.9 ± 98.2 pg/mL; p < 0.0001).
BL and Heat Challenge correspond to 27°C and 35°C temperature exposure, respectively. p values are a result of post-hoc between-group comparisons. Significance threshold was set at p < 0.05. Asterisks indicate statistically significant within-group post-hoc comparisons to the null hypothesis (* p < 0.01; ** p < 0.001; *** p < 0.0001).
BL, baseline; oC, degrees centigrade; Tskavg, average of distal skin temperatures; QSavg, quantitative sweat measurement of average upper and lower extremity sweat rate; LDFavg, laser Doppler flowmetry measurement of average distal upper and lower extremity microvascular perfusion; TS BL, 60, and 120, subjective rating of thermal sensitivity at baseline, 60, and 120 min of Heat Challenge; SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; HR, heart rate; Plasma NE, plasma norepinephrine; NA, not applicable; NS, not significant.
Heat challenge (35°C)
For Tcore, there was a significant main effect of Condition (p < 0.0001) and a significant interaction of Condition*Group (p < 0.0001). In the tetraplegic group, Tcore increased 0.78 ± 0.18°C (p < 0.001) after an average of 118 ± 5 min (range, 105–120 min) of Heat Challenge, whereas the control group demonstrated no significant change (−0.02 ± 0.22°C) after 120 min (Table 2A). The duration of exposure to the Heat Challenge did not significantly differ between groups; however, 87% of subjects with tetraplegia completed the entire 120 min of the Heat Challenge, whereas 100% of control subjects did. Despite the differences in Tcore at BL and the increase in Tcore in the tetraplegic group during the Heat Challenge, TS ratings were not different between the groups at any time during the Heat Challenge (Table 2A).
For Tskavg, there was a significant main effect of Condition (p < 0.0001), but no significant interaction of Condition*Group. Tskavg did not differ significantly between the tetraplegic and control groups at any time point, but did significantly increase within each group from BL to Heat Challenge (2.8 ± 1.2°C and 4.7 ± 3.0°C, respectively; Table 2A).
For QSavg, there was a significant main effect of Condition (p < 0.0001) and a significant interaction of Condition*Group (p < 0.0001). Both tetraplegic and control groups increased QSavg from BL to Heat Challenge (11.2 ± 3.9 to 17.1 ± 6.6 nL/min; p = 0.001 and 14.2 ± 3.5 to 131.1 ± 56.2 nL/min; p = 0.001, respectively). However, the percent increase of QSavg in the tetraplegic group (51 ± 12%) was significantly less (p = 0.007) compared to that in the control group (946 ± 672%; Table 2A).
For LDFavg, there was a significant main effect of Condition (p < 0.01) and a significant interaction of Condition*Group (p < 0.05). Only the control group demonstrated a significant increase in LDFavg from BL to post-Heat (109 ± 93%; p = 0.008), which was different between groups (p = 0.026; Table 2A).
There were no significant main effects of Condition or significant interaction effects of Condition*Group for either plasma NE or SBP. As expected, before and after Heat Challenge, plasma NE levels were lower in the tetraplegic group compared to the levels in the control group (p < 0.0001). SBP was significantly different between groups at all time points, but did not significantly increase in either group from BL to Heat Challenge (Table 2A).
For the Stroop Color and Word test, significant main effects of Condition were found for Stroop Color, Color-Word, and Interference (p = 0.008, p = 0.001, p = 0.011, respectively). Significant interaction effects (Group*Condition) were found for Stroop Color and Interference (p = 0.016, p = 0.011, respectively). After the Heat Challenge, the increases in Stroop Color and Interference scores were significant only in the tetraplegic group (p = 0.012 and p = 0.006, respectively), and the percent changes were different compared to controls (p = 0.021, p = 0.019, respectively; Table 2B).
BL and Heat Challenge correspond to 27°C and 35°C temperature exposure, respectively.
p values are a result of post-hoc within-group comparisons of Post-Heat to Baseline T-scores. Significance threshold was set at p < 0.05. Asterisks indicate significant post-hoc between-group comparisons of the percent change in T-scores (* p < 0.05; ** p < 0.01).
SD, standard deviation; BL, baseline; CI, confidence interval; NS, not significant.
For WAIS-IV Digit Span scores, a significant interaction effect (Group*Condition) was found in the Sequence subset (p = 0.025) with a trend toward significance for the WAIS-IV Total score (p = 0.073). After the Heat Challenge, the increase in WAIS-IV Sequence scores was significant in the tetraplegic group only (p = 0.022), and that change was different between groups (p = 0.009; Table 2B).
Discussion
Whereas previous studies have examined the effect of passive heat exposure on Tcore in persons with tetraplegia, 9 –12 this study is the first to explore the relationship of Tcore and cognitive performance during heat exposure in this population.
Baseline (27°C)
At baseline, the average Tcore of subjects with tetraplegia (36.9 ± 0.3°C) was significantly lower than that of AB controls (37.3 ± 0.3°C; Table 2A), which is supported by previous investigations. 11,12,25 Inpatients with chronic tetraplegia have presented with subnormal Tcore (35–36.5°C) 63% of the time despite relatively mild indoor temperatures (22.2–23.3°C). 26 The subnormal Tcore at BL was likely attributed to decreased thermogenesis secondary to the effects of skeletal muscle paralysis and atrophy on metabolic rate, and decreased heat conservation attributed to interruption of sympathetic vasomotor control.
Baseline measures of Tsk, QS, LDF, and TS did not differ between groups, demonstrating that the thermoneutral temperature (27°C) did not require hypothalamic activation of thermoregulatory mechanisms, that is, vasodilation of peripheral vasculature or sweating for heat dissipation, to maintain Tcore. 27,28 Investigations in AB subjects have shown that internal heat production and heat loss is balanced in ambient thermoneutral temperatures, allowing Tcore to be maintained passively. 29 –31
Heat challenge (35°C)
To effectively maintain Tcore during ambient heat exposure, peripheral thermosensors (transient receptor potential ion channels) relay hot temperature information from the skin to the preoptic-anterior hypothalamus. 32 The preoptic area integrates thermal information from both peripheral and central thermoreceptors and rapidly orchestrates the appropriate sympathetic-mediated thermoeffector responses of cutaneous vasodilation 33 and sweating 34 to dissipate heat while simultaneously withdrawing vasoconstrictor tone and inhibiting shivering for decreased insulation and thermogenesis, respectively. 35 –37
The control group demonstrated appropriate responses to the Heat Challenge. The significant increase in LDFavg of the distal extremities (109.6 ± 92.9%; p = 0.008) indicates increased blood flow to the periphery. The increased Tskavg of distal extremities (15.9 ± 10.9%; p = 0.002) reflects the convection of heat from central compartments to peripheral areas to increase radiant heat loss. Increases in evaporative heat loss were demonstrated by increased QSavg (946.3 ± 672.5%; p = 0.005). The effectiveness of these heat-dissipating responses in controls is evidenced by their stable Tcore during BL and Challenge conditions (37.3 ± 0.3°C vs. 37.3 ± 0.2°C, respectively; Table 2A).
Vasodilation of the peripheral vasculature increases convection of heat from the core to the skin. Blood flow to the skin is approximately 5% of cardiac output when resting in thermoneutral conditions. 38 Once Tcore exceeds 37°C, noradrenergic vasoconstrictor tone to the cutaneous vasculature is gradually withdrawn, whereas active cholinergic vasodilator tone to nonglaborous areas is increased. 4,39 During maximal heat stress, cardiac output may double with 60% of increased cardiac flow being redistributed to the skin. These adaptations allow the rate of skin blood flow to increase from approximately 300 mL/min to 8 L/min. 4, 39
The ability to increase sweat rate is vital to permit sufficient evaporative heat loss. 34 Eccrine sweat glands are responsible for the majority of evaporative heat loss. 40,41 During heat exposure, integration of peripheral and central afferent information by the preoptic hypothalamus results in increased sympathetic stimulation of postganglionic cholinergic sudomotor neurons to depolarize eccrine sweat gland receptors, increasing the number of active sweat glands and the rate of sweat production. 42 Under intense conditions, typical maximal sweat rates are 1.4 L/h, although sweat rates as high as 3 L/h have been reported in elite athletes. 43,44
Post-SCI, particularly after injuries resulting in sensory complete tetraplegia (AIS-A), the skin below the level of lesion (≈75% of the body) is insentient and information of hot ambient temperatures is not transmitted to the hypothalamus. 8,45 This interruption of sensory feedback, in conjunction with the decentralization of descending sympathetic pathways, impairs hypothalamic regulation of peripheral vasodilation 13 and sweating, 11 limiting the ability to increase peripheral heat loss through convection, radiation, and evaporation in persons with tetraplegia. Therefore, in hot environmental conditions, Tcore in persons with tetraplegia drifts toward hyperthermic values. 9,12,46
After 118 ± 5 min of Heat Challenge, the tetraplegic group had a significant increase in Tcore (2.1 ± 0.5%), compared to no change in the control group. Tcore at the end of Heat Challenge in the tetraplegic group (37.7 ± 0.4°C) was greater than that of controls, yet still within the euthermic range (Table 2A). This rise in Tcore is supported by previous investigations in persons with SCI when exposed to warm-hot ambient temperatures. 9,10,12,13,47
The rise in Tcore during the Heat Challenge in the tetraplegic group was attributed to ineffective responses of peripheral vasodilation and sweating. The increase in Tskavg in the tetraplegic group, although significant (8.4 ± 3.8%; p < 0.001), was only half that of the control group (15.9 ± 10.9%) and appeared to be lower as well (Table 2A). Although QSavg increased in the tetraplegic group (51.5 ± 12.3%; p < 0.0001), the increase was less robust compared to controls (p = 0.007), signifying lower rates of evaporative heat loss (Table 2A). LDF did not increase in the tetraplegic group, signifying an impaired ability to increase blood flow to the periphery for convection of heat to the skin (Table 2A).
The increase in distal Tskavg in the tetraplegic group may have been attributed to external factors, that is, increased skin temperature secondary to exposure to the warm ambient temperature, rather than from increased blood flow from central compartments, given that no increase in LDF was observed. Further, had the controls not exhibited such a robust rate of sweating (131.1 ± 56.6 nL/min), the cooling effect of evaporation would have been minimized and their rise in Tskavg would have most likely been even higher. We speculate that the increase in QSavg, albeit minimal in the tetraplegic group, may have been attributed to residual sympathetic pathways.
Plasma NE levels did not increase in the tetraplegic group during the Heat Challenge despite a significant rise in Tcore. We attribute the absence of change in circulating NE levels to interruption of sympathetic pathways, which is supported by their lower plasma NE levels compared to controls (p < 0.001) during both BL and after Heat Challenge conditions (Table 2A). 48,49
The absence of an increase in plasma NE levels in the control group was likely attributed to the Heat Challenge not being stressful enough to affect a rise in Tcore. Previous investigations in healthy controls used more intense heat challenges (up to 73°C) to cause a rise in Tcore and associated increases of up to 58% in plasma NE levels. 50 –52
Cognitive outcomes
When comparing cognitive performance at BL to post-Challenge, only the tetraplegic group demonstrated significant improvements in Stroop Color and Interference T-scores and in WAIS-IV Digit Span Sequencing T-scores. These improvements in cognitive performance were in contrast to the absence of change in controls to neuropsychological testing (Table 2B).
The improvements in the Stroop Color T-scores imply improved attention, which may be attributed to increases in arousal secondary to the increased Tcore in the tetraplegic group post-Challenge. The improvements in Stroop Interference scores imply improved response inhibition under a condition in which subjects must inhibit the reflex of reading the word and instead state the color of the font. Inhibiting a reflexive response in favor of a conscious decision is a measure of executive function. Increased control of attention can enhance focusing on selected stimuli and suppressing attention to distracting stimuli. 53
The improvement in the WAIS-IV Digit Span Sequencing scores implies enhanced working memory given that subjects must not only remember numbers, but also temporarily store them to rearrange those numbers and repeat them in the proper sequence.
The improvements in attention, executive functioning, and working memory in the tetraplegic group may be attributed to the higher Tcore post-Challenge increasing nerve conduction velocity, cerebral metabolism, and, possibly, brain neurotransmitter levels. Wright and colleagues demonstrated in AB controls that subtle increases in Tcore (∼0.5°C), a typical variability attributed to circadian rhythm, had a positive effect on working memory, alertness, and attention independent of circadian phase, 54 supporting the hypothesis that Tcore affects neurobehavioral processes. More specifically, tissue temperature changes have been shown to affect peripheral nerve conduction velocity increasing from 12 m/s at 21°C to 30 m/s at 35°C ambient temperature. 55,56 Cerebral metabolism has been reported to decline 6–8% for every 1°C decrease in Tcore, 57 and lower Tcore during cold exposure has been shown to decrease brain catecholamine levels, resulting in decreased attention and inhibition of distracting stimuli. 58 Although nerve conduction velocity, cerebral metabolism, or brain catecholamine levels were not measured, their combined effects in the tetraplegic group could have attributed to the observed improvements in attention and executive function with the increase of ∼0.8°C in Tcore attributed to heat exposure.
Increased attention and processing speed in the post-Challenge condition would enhance the ability to concentrate on the information presented, thus increasing the ability to store and manipulate it. In summary, the ability to store and manipulate information quickly and accurately would favorably affect the routine activities that persons with tetraplegia encounter during routine shopping, banking, and adherence to complex medical routines whereas improved decision making can result in more attentive self-care and prudent lifestyle choices.
Measures of thermal sensitivity were not different between the groups at any time point despite significant differences in Tcore during both BL and Heat Challenge conditions. However, the relationship of TS to Tcore was different between groups (p = 0.012), with an increase of 1 point of TS rating for every 0.044°C increase in Tcore in the tetraplegic group. No relationship was evident in the control group, which had no change in Tcore to heat exposure (Fig. 2). This lack of increased sensitivity in the tetraplegic group raises clinical concerns that subjective ratings of neutral thermal comfort (0 of 4) at BL in persons with tetraplegia does not imply euthermia, whereas ratings of feeling hot (3 of 4) during Heat Challenge may imply that Tcore values are approaching hyperthermia (≥38°C). We speculate that the lack of afferent information from the majority of peripheral thermal receptors may have contributed to the similar ratings of TS despite significant differences in Tcore between the groups. 8
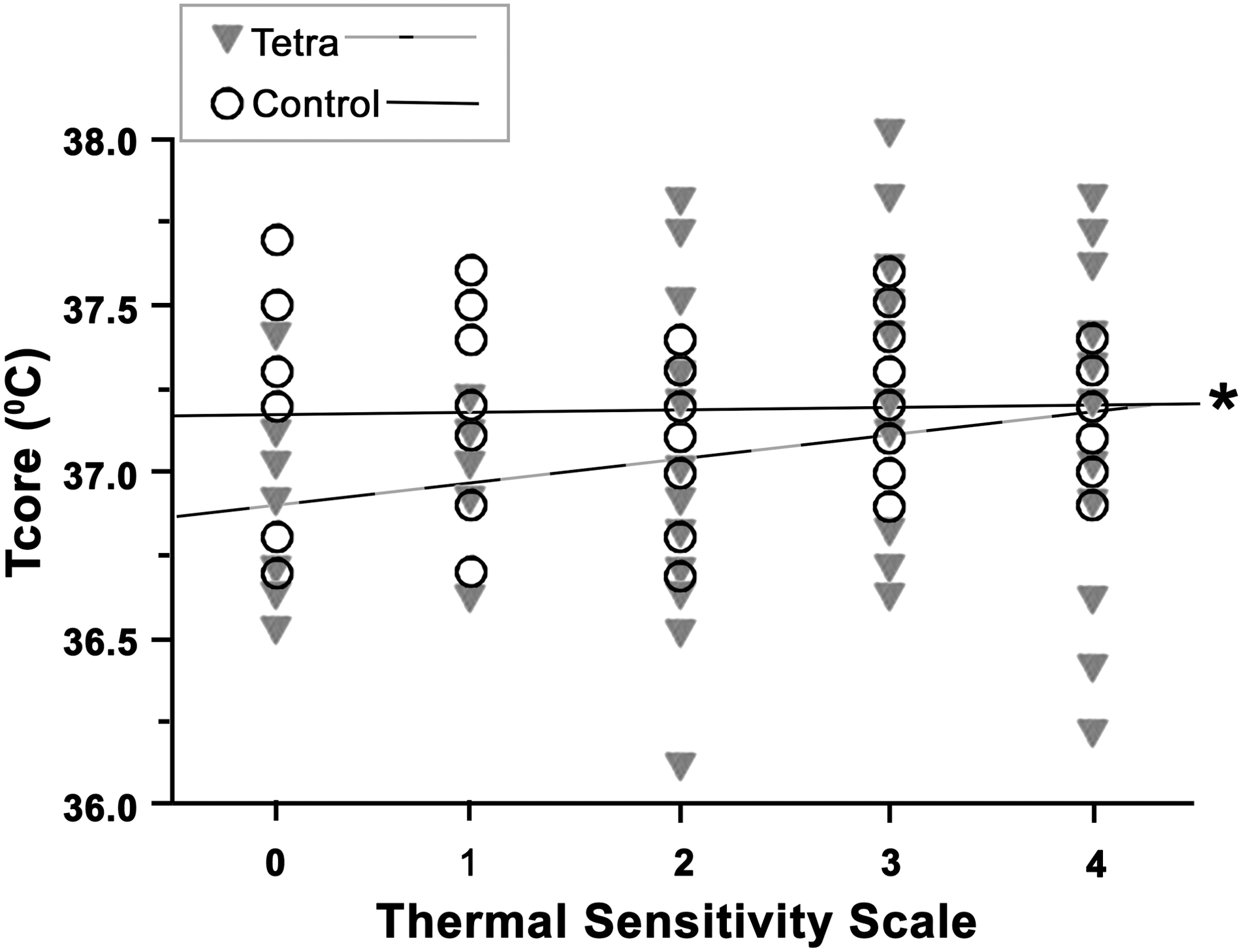
Relationship of thermal sensitivity to Tcore was different between groups (p = 0.011). Asterisk (*) indicates significant between-group comparison of regression lines (*p < 0.05).
Had the duration of the Heat Challenge extended past the average of 118 ± 5 min in the tetraplegic group, it is very likely that the majority of those subjects would have become hyperthermic. Given that exposure to hot ambient temperatures is quite common, especially during summer months, the development of convenient, user-friendly methods for more frequent objective monitoring of Tcore in persons with tetraplegia would be beneficial, particularly whenever they report feeling hot.
Implications
The clinical implications of these findings are that persons with tetraplegia have an increased vulnerability to hyperthermia during even limited heat exposure. However, subjective perception of heat post-SCI does not represent similar Tcore as it does in AB individuals. Therefore, more frequent monitoring of Tcore is recommended during heat exposure or when persons with tetraplegia report feeling hot. Second, these findings suggest that the typical resting Tcore of persons with tetraplegia may not be optimal for cognitive performance. Bringing Tcore into the euthermic range may optimize cognitive performance for such individuals, allowing for improved self-care and healthier lifestyle choices, resulting in improved overall quality of life.
Limitations
This study did not assess cognitive performance a third time, after Tcore had returned to BL values, in order to more conclusively demonstrate a causal relationship between Tcore and cognitive performance. However, recent evidence of decreased cognitive performance with a decrease in Tcore in persons with tetraplegia supports the association of improved performance with increased Tcore, as was presented in our study. 59
The relatively small sample size, with the majority of subjects being men, limits the ability to extrapolate our findings to the general SCI population. However, a sample of predominantly men is representative of the sex bias in the incidence of SCI.
Conclusions
This study demonstrated that less than 2 h of exposure to ambient heat (35°C) resulted in a ∼0.8°C increase in Tcore. This is likely a result of thermoregulatory dysfunction post-SCI. The increase in Tcore, from subnormal levels to the euthermic range, was unexpectedly associated with an improvement in cognitive performance in the areas of attention, working memory, and executive functioning.
Increased awareness of the vulnerability of persons with tetraplegia to hyperthermia and more frequent monitoring during exposure to hot conditions would be expected to protect against the development of hyperthermia and its associated deleterious consequences. The finding of improved cognitive performance with a rise in Tcore warrants further study of safe and effective interventions to raise the apparently chronically depressed Tcore in persons with tetraplegia to within the euthermic range, which will allow for more optimal cognitive performance for self-care, compliance with medical advice, and healthy lifestyle decisions.
Footnotes
Acknowledgments
Support for this work was provided by the Department of Veterans Affairs, Veterans Health Administration, Rehabilitation Research and Development Service National Center for the Medical Consequences of Spinal Cord Injury (#B2020-C, #B9212-C), and the James J. Peters Veterans Affairs Medical Center. Clinical Trial Registration Number: NCT01890915.
We would also like to acknowledge the Roho Group (Belleville, IL) for their donations of Roho High-Profile dry flotation seat cushions.
Author Disclosure Statement
No competing financial interests exist.