
Abstract
Traumatic brain injury (TBI) is the leading cause of death and disability in people younger than 45 in Western countries. Despite many studies, no reliable biomarkers have been found to assess TBI severity and predict recovery. MicroRNA (miRNA) profiling has become widely used to identify biomarkers and therapeutic targets. Through use of the TaqMan Array Human MicroRNA A+B Cards, the expression of 754 miRNAs was analyzed in serum of five mild TBI (mTBI) patients with extra-cranial injury (EC), five severe TBI (sTBI) patients with EC, and five healthy volunteers (HV) at 1 day and 15 days post-injury. The aim was to find candidate biomarkers able to discriminate between mTBI and sTBI. Following this, it was possible to select 10 miRNAs for further study in an enlarged validation cohort of 120 patients by using single TaqMan assays at the following time-points: T0-1 h, T4-12 h, T48-72 h, and 15 days from the injury. Analysis revealed two miRNAs (miR-425-5p and miR-502) that were significantly downregulated (p < 0.05) in mTBI at early time-points and are ideal candidates for diagnosis of mTBI, and two miRNAs (miR-21 and miR-335) that were significantly upregulated (p < 0.01) and are valid biomarkers for the diagnosis of sTBI. In addition, miR-425-5p was a strong predictor of 6-month outcome at T0-1 h and T4-12 h, while miR-21 was predictive of the outcome at T4-12 h. The panel of selected miRNAs shows promise as biomarkers to discriminate mTBI from sTBI. In addition, the selected miRNAs represent new potential therapeutic targets.
Introduction
M
One of the main challenges of TBI at present is the lack of diagnostic biomarkers. This is especially true for mild TBI (mTBI), which remains currently difficult to assess in clinical practice. Although TBI patients are initially assessed by the Glasgow Coma Score (GCS) and neuroimaging techniques, which require costly equipment, the current diagnostic tools are lacking in the ability to precisely define and quantify the actual severity of the brain injury, thus leading to an easy detection of severe, but not mild TBI, which represents the vast majority of cases (75–90%). Moreover, the GCS score can be of limited use in mTBI diagnosis in the presence of polytrauma, alcohol abuse, use of sedatives, and psychological stress.
The majority of patients who suffer an mTBI tend to experience only transient effects and are left with no permanent deficits. About 15% of them experience prolonged disabling post-concussional symptoms. In addition, evidence suggests that although mTBI induces only limited clinical effects after injury, a wide range of metabolic changes occur that lead to a period of post-concussive vulnerability, during which an additional mild insult can lead to catastrophic injury. 16 –18 Repetitive mTBI also has been linked to neurodegenerative conditions, including chronic traumatic encephalopathy. 19 Therefore, the correct diagnosis of mTBI is particularly important in patients who are at greater risk of repetitive mTBI, such as sportspeople, 20 military personnel, and children. 21,22
Biomarkers offer many advantages for mTBI diagnosis since they can be measured from biofluids such as blood, urine, and saliva, and can be easily quantitated using standard biochemical and molecular methods. Early diagnosis and evaluation of the severity of TBI thus becomes crucial for patients' well-being and ultimately saving their lives. As miRNAs are emerging as promising biomarkers in a range of different pathologies, we sought to explore their role in TBI.
First, we determined the serum levels of 754 miRNAs in five mTBI patients with extra-cranial injury (EC), five severe TBI (sTBI) +EC injury patients, and healthy volunteers (HV) at 1 day and 15 days from injury. The aim of this initial study was to select specific candidate biomarkers that are able to discriminate mild from severe TBI, and follow their levels up to 15 days. Based on this information, it was then possible to select 10 miRNAs for further study in an enlarged cohort of 120 patients, which were grouped based on mTBI+EC, sTBI+EC, and EC by using single TaqMan assays. In this second data set population, the blood was taken at different time-points, with the aim to identify early biomarkers, in particular at “time zero,” where samples have been collected within 1 h from injury by the ambulance crew at the injury scene before patients were admitted to hospital. The early identification of these biomarkers allows clinicians to recognize and treat patients at risk of secondary brain injury and streamline early management pathways. The identification of “time zero” TBI biomarkers is particularly desirable, as this could potentially lead to the development of point-of-injury diagnostics that could provide clinical information in a pre-hospital environment before any radiological or specialist clinical information was available. Moreover, if the same biomarkers also held prognostic value, they could enhance the current predictive models 23,24 for outcome and patient stratification.
Methods
Study approval
Study participants were recruited from the Surgical Reconstruction and Microbiology Research Center at Queen Elizabeth Hospital of Birmingham (UK) as part of the SIR (Steroids and Immunity From Injury Through to Rehabilitation) study (Ethics Ref. 11/SW/0177), the ReCoS (Repetitive Concussion in Sport) study (Ethics Ref. 11-0429AP28), and the Golden Hour study (Ethics Ref. 13/WA/0399). Written informed consent was received from participants or valid proxy (family or a professional not directly involved in the study) prior to inclusion in the study.
The preliminary study used serum samples from a total of 15 patients: five HV, five mTBI+EC patients, and five sTBI+EC patients. Serum was taken at 1 day and 15 days from the injury. From these data, we calculated the sample size needed for validation in a larger cohort of patients with alpha = 0.05 and power = 0.8. The sample size required was 29 subjects in each category group based on the most variant miRNA identified (miR-335).
The second dataset of samples used serum samples from a total of 120 individuals grouped into four different categories: HV (n = 30), EC (n = 30), mTBI+EC (n = 30), and sTBI+EC (n = 30); blood was taken at different time-points (T0-1 h, T4-12 h, T48-72 h, 15 days) in each patient. Healthy volunteers were consented and enrolled in the ReCoS study. EC injury patients had radiographically confirmed orthopedic fractures, no head trauma, no infection, no history of neurological or psychiatric disorders, and no alcohol or drug dependency. Mild TBI with EC included those with a non-penetrating head trauma and a Glasgow Coma Scale (GCS) score ≥13. Severe TBI with EC included patients with a GCS score ≤8. Clinical, demographic, and imaging parameters were collected for each patient including, among others, duration of loss of consciousness, confusion, post-traumatic amnesia, neurological deficits, hypoxemia, systemic hypotension, Injury Severity Score (ISS), length of hospital and intensive care stay, seizures, sepsis, CT Marshall grade, age, pupillary reactivity, significant comorbidities and ethnicity (Table 1).
Mechanism of injury. bComputed tomography findings: −, no visual pathology; + visual pathology (swelling, contusion, mass lesion).
ISS, Injury Severity Score; GCS, Glasgow Coma Scale; GOSe, extended Glasgow Outcome Scale; SD, standard deviation; M, male; F, female; A, assault; F, fall; P, penetrating; RTC, road traffic accident; B, other blunt; HV, healthy volunteers; NA, not applicable; mTBI, mild traumatic brain injury; EC, extra-cranial injury; sTBI, severe traumatic brain injury.
Patients' outcome was evaluated by the extended Glasgow Outcome Scale (GOSe) at 6 months from the injury, which, for survivors, was collected by face-to-face follow up or telephone interview with the patient or carer in all cases. All patients were gender and age matched to HVs.
Sample processing
The blood samples were processed for serum isolation within 2 h after withdrawal. Whole blood was left to stand for about 30 min at room temperature before being centrifuged at 3000 rpm for 10 min at 4°C. Serum was divided into aliquots and stored at −80°C until analysis.
RNA isolation, reverse transcription, and miRNAs profiling by TaqMan Low Density Array
Initial screening (discovery set) was performed on five mTBI+EC and five sTBI+EC patients, which was compared with HV at the two different time-points (1 day and 15 days from the injury). The serum of these patients was used to profile the transcriptome of 754 miRNAs. Serum samples were centrifuged at 2000 rpm for 10 min to pellet and remove any circulating cell or debris. MiRNAs were extracted from 400 μL of serum samples by using Qiagen miRNeasy mini kit (Qiagen, GmbH, Hilden, Germany) according to Qiagen supplementary protocol for purification of small RNAs from serum and plasma and finally eluted in 30 μL volume of RNase-free water. 25 The concentration and purity of the resulting RNA was determined with a ND-1000 UV-Vis Spectrophotometer (NanoDrop). Twenty ng of serum RNAs were retrotranscribed and pre-amplified according to the manufacturer's instructions (Applied Biosystems, Life Technologies). Pre-amplified products were loaded onto TaqMan Low Density Arrays (TLDAs), TaqMan Human MicroRNA Array v3.0 A and B (Applied Biosystems, Life Technologies). Polymerase chain reaction (PCR) on TLDAs were performed on 7900HT Fast RealTime PCR System (Applied Biosystems, Life Technologies).
Data analysis
To obtain an accurate miRNA profiling, we used the global median normalization method. Similar to microarray analysis, Ct values from each sample were normalized to the median Ct of the array.
26
Moreover, by computing the Pearson correlation among the Ct medians and means of each array and Ct of each miRNA, we identified two miRNAs that showed an expression profile close to the median and mean of TLDAs (i.e., miR-331 and miR-223*). These miRNAs also were confirmed to be among the most stable in TLDAs by applying two different methods: DataAssistv.3 software (Applied Biosystems, Life Technologies) and geNorm Algorithm (
Single TaqMan assays
Ten differentially expressed miRNAs were chosen from the arrays as potential candidate biomarkers with the aim to discriminate mTBI from sTBI at early time-points. These candidates were used to validate the data in an enlarged cohort of 120 patients (validation set) grouped into three different categories (mTBI+EC, sTBI+EC, and EC only) and controls (HV) at different time-points (T0-1 h, T4-12 h, T48-72 h, and 15 days from injury) by single TaqMan assays (Applied Biosystems, Life Technologies). Samples were extracted and retrotranscribed as described above and real-time quantitative polymerase chain reaction analysis was performed in Bio-Rad iQ5 Real-time PCR Detection System (Bio-Rad, CA). Expression fold changes were calculated by the 2−ΔΔCT method.
Statistical analysis
The data were checked for normal distribution and transformed to perform parametric tests. Comparisons across groups at each time and within groups over time were performed by the one-way analysis of variance and Tukey's post hoc test on transformed data. A receiver operating characteristic analysis was utilized to calculate sensitivity and specificity of each biomarker in diagnosing either mTBI or sTBI at T0-1 h and T4-12 h, expressed as area under the curve (AUC). All analyses were carried on SPSS v.22 (IBM).
Using a Spearman correlation analysis the miRNAs levels also were correlated with age, Marshall grade, and ISS. Mann Whitney was used to analyze gender differences in miRNA levels.
An ordinal regression analysis (proportional odds model) was carried out in order to analyze the predictive value of miRNAs with regard to 6-month outcome. The predictors were selected based on the variables of the CRASH Head Injury Prognosis model (
miRNA targets
To infer biological meaning of data obtained, targets for DE miRNA were retrieved from Tarbase V7, a database cataloguing published experimentally validated miRNA:gene interactions (REF: PMID:25416803). The identification of statistically significant biological functions associated to miRNA targets was obtained by using FatiGo from Babelomics 4.3 server (
Results
Patient characteristics and demographics are shown in Table 1. Of the mTBI patients, 20 (66.7%) experienced loss of consciousness and 10 did not (33.3%); 17 (56.7%) experienced mild post-traumatic amnesia (PTA) (< 24 h), nine (30%) moderate PTA ( > 24 h but <7 days), and four (13.3%) were not assessed for PTA. No seizures were recorded in mTBI patients.
Expression profiles by TaqMan Low Density Arrays
From 754 screenable miRNAs of TLDA, we identified 10 circulating miRNAs at 1 day and 13 at 15 days in mTBI+EC, 19 at 1 day, and 22 at 15 days in sTBI+EC differentially expressed (Table 2). From this list, hsa-miR-126*, miR-139a-5p, miR-144*, miR-190, miR-194, miR-365, miR-590-3p, miR-624, miR-625*, and miR-671-3p were excluded for further analysis because they were expressed across all the categories, hence not suitable candidate biomarkers for mild or severe trauma only. On the other hand, miR-184, miR-502, miR-505, and miR-301b, uniquely and differentially expressed in mTBI+EC at 1 day, were selected as early candidate biomarkers of mTBI. In addition, miR-203, miR-654-3p, and miR-655 differentially expressed at 15 days post–mTBI+EC were selected as later candidate biomarkers of mTBI. MiR-425-5p also was selected because its peculiar trend—downregulated at 1 day and upregulated at 15 days in mildly injured patients only.
In bold, microRNAs selected for analysis in the validation cohort.
mTBI, mild traumatic brain injury; EC, extra-cranial injury; sTBI, severe traumatic brain injury; HV, healthy volunteers; TLDA, TaqMan Low Density Array.
Finally, two miRNAs (miR-21 and miR-335) of the 19 and 22 DE miRNAs at 1 day and 15 days respectively were selected in sTBI+EC for further studies because they were consistently expressed at both time-points.
Single TaqMan assay for candidate biomarkers of mTBI
To validate these findings, we subsequently tested the expression of selected miRNAs in three separate and independent groups (30 mTBI + EC, 30 sTBI + EC, and 30 EC) at different time-points (T0, T4-12 h, T48-72 h, and 15 days from the injury) by using single TaqMan assays. The results were compared with 30 HV. The fold changes were calculated by the 2−ΔΔCT method, using miR-331 and miR-223* as reference.
Among the candidate biomarkers of mTBI at both time-points (miR-184, miR-502, miR-505, miR-301b, miR-203, miR-425-5p, miR-654-3p, and miR-655), only two showed interesting results and were significantly and differentially expressed in the three different categories, compared with HV. Specifically, miR-425-5p and miR-502 showed a similar trend (Fig. 1). They were both significantly downregulated in mTBI+EC, miR-425-5p at T0-1h (p = 0.01845), and at T4-12 h (p = 0.01962), respectively, compared with HV, or EC and sTBI+EC (p < 0.05), and miR-502 at T0-1 h and at T4-12 h, compared with HV (p = 0.02538 and p = 0.03718 respectively), or EC and sTBI+EC (p < 0.01). After 48 h from mild injury, miR-425-5p and miR-502 returned to normal levels. The expression of miR-425-5p and miR-502 also was found in the EC group at a comparable level to HV, thus suggesting that these two biomarkers are downregulated in brain injury patients only. Moreover, neither of them showed any significant downregulation in sTBI+EC, compared with HV, at all time-points. Therefore, miR-425-5p and miR-502 could be considered the most promising candidate biomarkers for the early diagnosis and monitoring of mTBI. AUCs for these biomarkers at the most relevant time-points are shown in Table 3.
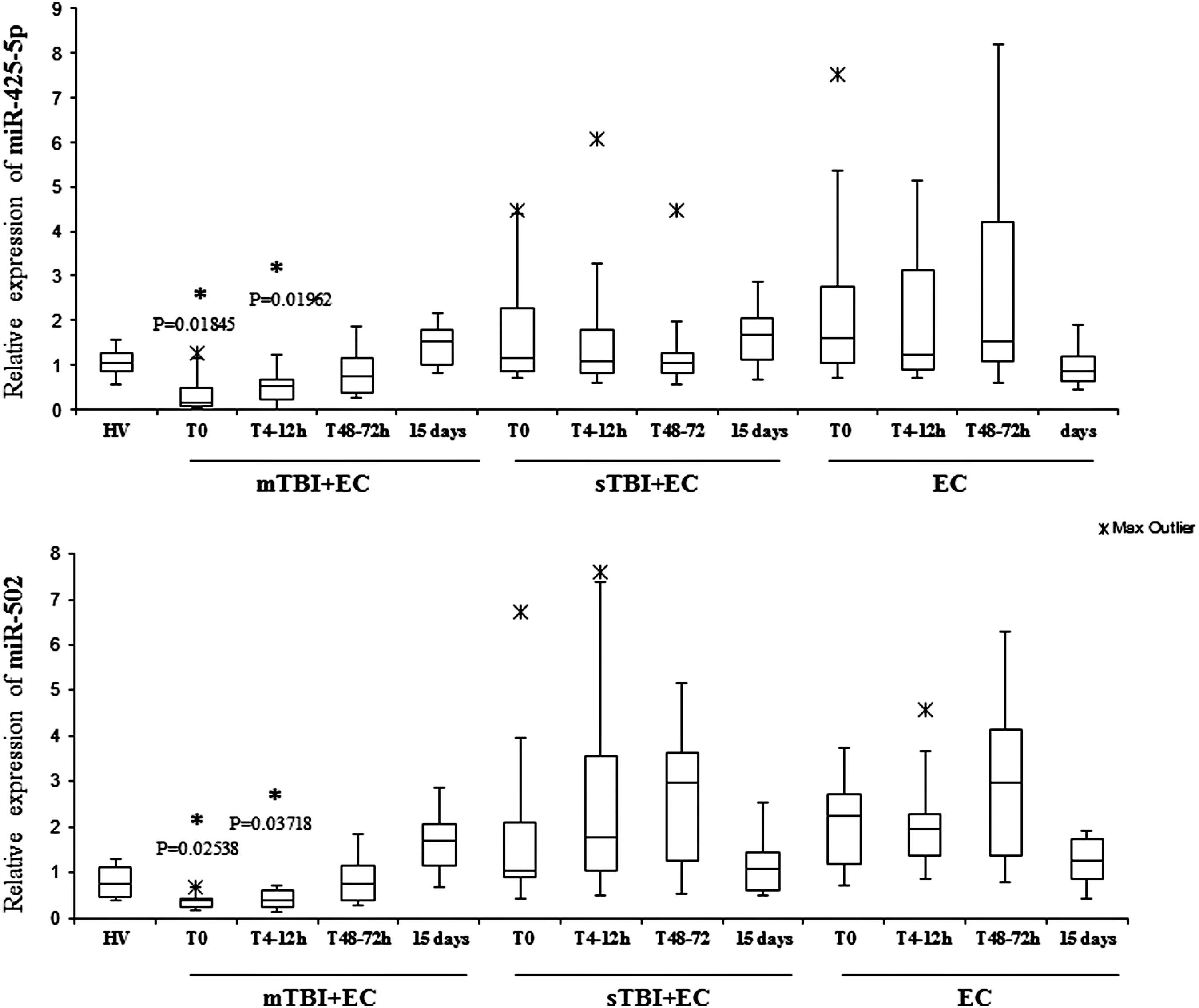
Time course of miR-425-5p and miR-502 expression in three different categories of trauma and healthy volunteers (HV). MiR-425-5p and miR-502 expression in 30 HV, 30 mild traumatic brain injury (mTBI)+extra-cranial injury (EC) patients, 30 EC patients, and 30 severe traumatic brain injury (sTBI)+EC patients at different time-points from injury (T0, T4-12 h, T48-72 h, 15 days) detected by real-time quantitative polymerase chain reaction analysis. MiR-425-5p expression was found to be remarkably decreased in mTBI+EC patients at T0 and T4-12 h, compared with HV, sTBI+EC patients, and EC patients (p < 0.05). MiR-502 expression was found to be remarkably decreased in mTBI+EC patients at T0 and T4-12 h, compared with HV, sTBI+EC patients, and EC patients (p < 0.05). The p values were determined by Tukey's post hoc test. *Significantly different from HV.
Only most relevant time-points are shown.
TBI, traumatic brain injury; mTBI, mild traumatic brain injury; HV, healthy volunteers; sTBI, severe traumatic brain injury; EC, extra-cranial injury.
Single TaqMan assay for candidate biomarkers of sTBI
MiR-21 and miR-335 were analyzed as potential biomarkers of sTBI since they both appeared upregulated at both time-points of sTBI+EC in the initial screening. They showed to be strong candidates in the second dataset of patients, as well (Fig. 2). Mir-21 was significantly upregulated in sTBI with EC at all time-points after 4 h from injury with respect to HV, EC, and mTBI+EC (p = 0.00306 at T4-12 h, p = 0.00844 at T48-72 h, and p = 0.00077 at 15 days). No significant differences were found in the remaining categories, compared with HV. MiR-335 showed upregulation in sTBI+EC and at all time-points, compared with HV (p = 0.00109 at T0-1 h, p = 0.00284 at T4-12 h, p = 0.00012 T48-72 h, and p = 0.01284 at 15 days) and mTBI+EC, but no significant upregulation was found compared with EC. AUCs for these biomarkers at the most relevant time-points also are shown in Table 3.
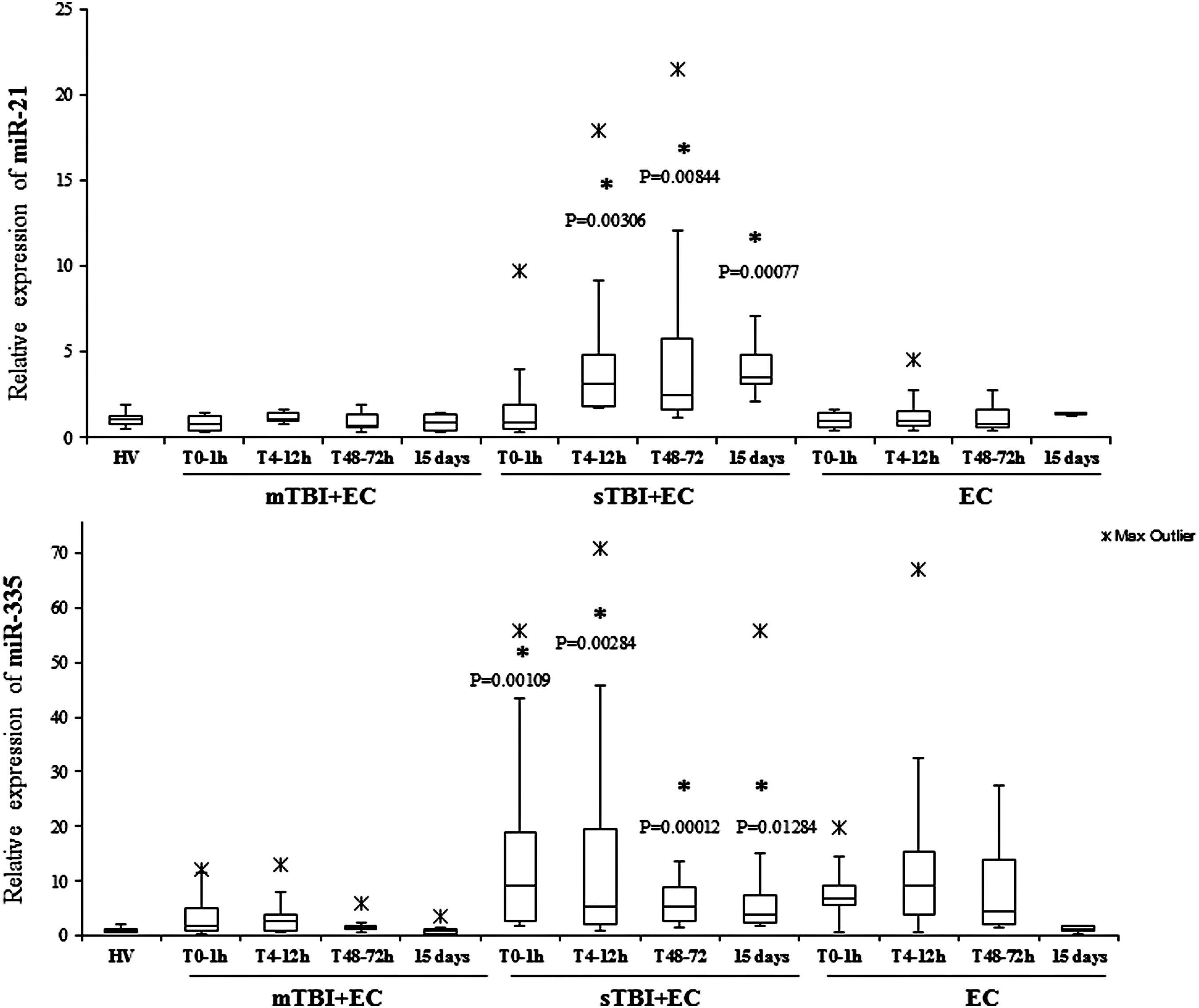
Time course of miR-21 and miR-335 expression in three different categories of trauma and healthy volunteers (HV). MiR-21 and miR-335 expression in 30 HV, 30 mild traumatic brain injury (mTBI)+extra-cranial injury (EC) patients, 30 EC patients, and 30 severe traumatic brain injury (sTBI)+EC patients at different time-points from injury (T0, T4-12 h, T48-72 h, 15 days) detected by real-time quantitative polymerase chain reaction analysis. MiR-21 expression was found to be significantly up-regulated in sTBI+EC patients at T4-12 h, T48-72 h, and 15 days, compared with HV (p < 0.01). MiR-335 expression was found to be remarkably up-regulated in sTBI+EC patients at T0, T4-12 h, T48-72 h and 15 days, compared with HV and mTBI+EC patients (p < 0.001) but not EC only patients. The p values were determined by Tukey's post hoc test.*Significantly different from HV.
In addition, miR-21 correlates with age (R = 0.43; p = 0.03) and Marshall grade (R = 0.58 p = 0.002) at T4-12 h. No other significant correlations were found between miRNAs and age, Marshall grade, and ISS. There were no differences in gender distribution of the microRNAs.
TBI patients outcome at 6 months
In our model, the ordinal regression analysis confirmed the predictive value of all known TBI outcome predictors, including age, GCS, radiological abnormalities, hypoxia, hypotension, pupillary reactivity, and major extracranial trauma. In addition, miR-425-5p at T0-1 h was strongly predictive of 6-month outcome when included in the model (both p < 0.0001; Table 4, Panel A). However, miR-502, miR-21, and miR-335 did not show any prognostic value at this time-point. When measured at a later time-point, T4-12 h, miR425-5p retained prognostic value; in addition, miR-21 also became highly predictive (p < 0.0001), while miR-502 and miR-335 remained non-significant (Table 4, Panel B).
Dependent variable: Glasgow Outcome Scale Extended. Model: Marshall grade, hypoxia (oxygen saturation <90%), hypotension (systolic blood pressure <90 mm Hg), pupillary reactivity (PupilReact; both pupils reacting, one reacting, neither reacting), presence of traumatic subarachnoid hemorrhage (tSAH), major extracranial trauma (Polytrauma), Glasgow Coma Scale (GCS), age, miR-21, miR-335, miR-425-5p, miR-502. Only significant predictors are shown.
miRNA targets and gene ontology analysis
The different distribution of these miRNAs in serum of mTBI and sTBI patients is most likely a systemic consequence of the different physiopathology of these two types of trauma. To evaluate the biological functions of DE miRNAs, we computationally searched their validated or predicted targets. Gene ontologies of miRNA targets were analyzed by FatiGo. This analysis showed that they are involved in such important biological processes as inflammation, metabolism, proliferation/apoptosis, cell adhesion, and interestingly, in long-term depression (Supplementary Fig. 1; see online supplementary material at
Discussion
Efficiently identifying biomarkers for TBI is crucial, especially for mTBI patients, in order to prevent any potential further injury and to plan the appropriate care for the subset of patients who experience prolonged symptoms. For example, much effort is currently devoted to the identification of suitable pitch-side biomarkers for the management of sport concussion. The development of objective molecular markers for TBI would be of great use in this regard, particularly as existing tools such as the GCS scale do not fully capture the wide range of heterogeneity of patients with a score of 15. Some advancement has been made in the development of biomarkers for TBI in recent years, particularly concerning N-acetyl-aspartate (NAA). Reduced levels of NAA may reflect the severity and the recovery of trauma. 18,27 Some progress has also been made in biomarkers such as S100B, neuron-specific enolase, and glial fibrillary acidic protein; however, insufficient sensitivity and specificity 28 call for more research to identify other biomarkers specific to mTBI.
In the present study, we investigated if changes in the levels of serum miRNAs can be applied to evaluate the severity of TBI. In our study, we focused on serum, not only because it has practical advantages, but also because it is free of anticoagulants such as heparin, a potential inhibitor of PCR reactions. 29 It is also important to note that serum may be less affected by hemolysis, compared with plasma. A recent study suggests a contribution by blood cell–specific and platelet-specific miRNAs deriving from plasma haemolysis and resulting in significant variation of miRNAs expression. 30
The discovery of miRNAs as TBI biomarkers at such an early time-point (T0-1 h) is of paramount importance, as this could guide clinical decision-making in the pre-hospital environment at a time when no radiological or detailed clinical information is available. This may be particularly helpful in the work-up of mTBI, which is easy to miss and remains one of the most difficult diagnoses to make at the pitch side or in austere environments such as during military operations. The reproducibility of the mTBI findings across two independent cohorts of National Health Service patients (the Golden Hour study) and concussed professional athletes (the ReCoS study) increases the confidence in our results.
In the initial screening from the TLDAs, eight miRNAs were selected to be studied as candidate biomarkers for early detection and recovery of mTBI. MiR-425-5p and miR-502 showed a similar trend and a significant downregulation at T0-1 h and T4-12 h in mTBI+EC patients, compared with HV, EC patients, and sTBI+EC patients. This early downregulation, makes both miRs suitable candidate biomarkers of mild brain trauma.
Following sTBI, two miRNAs (miR-21, miR-335) were noted to be expressed at both 1 day and 15 days and were thus selected as potential biomarkers for sTBI. MiR-21 and miR-335 were significantly upregulated at most of the time-points in sTBI+EC patients when compared with controls. Therefore, the overexpression confirmed the results of the array and showed the potential of these molecules as biomarkers of sTBI. While miR-21 showed significant upregulation in brain injured patients only, miR-335 was significantly upregulated in EC patients, too, but it returned to normal in this cohort at 15 days from injury. This suggests that miR-335 is a suitable biomarker for trauma in general at early time-points but it may remain elevated in a sustained fashion in severe TBI patients only.
Single assays in the validation set of patients did not show significant results for miR-184, miR-505, miR-301b, miR-203, miR-654-3p, and miR-655 (data not shown). Thus, their potential use of biomarkers cannot be supported. This result may be attributable to the small sample size in the initial assay and to the variability of individuals.
Among the described miRNAs, only miR-21 has been already described in literature 31 as a candidate of severe brain injury in animals. The rest of the selected miRNAs are described for the first time in this paper as biomarkers of TBI.
One important point is that the initial downregulation of miRNAs in the array of mTBI+EC was in the early time-points from the injury. This result mirrors the general mRNA downregulation found at the beginning of mTBI, 32 and can be compared with a state of “hibernation” described after mTBI 33 and used as strategy of neuroprotection. 33,34 Therefore, it is not surprising to see a differential expression of miRNAs between mTBI and sTBI. In addition, considering the general mechanism of regulation of miRNAs, where downregulation allows a further upregulation of targets, it could be hypothesized that this initial downregulation leads to an increment of synthesis of proteins involved in recovery processes.
Moreover, our results correlate with patients' outcome. In particular, the expression at T0-1 h and T4-12 h of miR-425-5p, and at T4-12 h miR-21 contribute to the predictive model of outcome at 6 months, thus showing potential to support early clinical decision-making and patient stratification for treatment or research.
Finally, gene ontologies analysis showed the different mechanisms in which targets are involved in two pathologies. Our results show that miRNA targets are mainly involved in functional processes as metabolism, inflammation, and apoptosis in sTBI. Targets of mTBI instead induce signaling systems and regulation of apoptosis and cell adhesion. Importantly, in both cases, these targets are involved in long-term depression. As expected, target genes were found expressed mainly in brain (Supplementary Fig. 2) in both trauma severities, thus corroborating the plausibility of these miRNAs as biomarkers of brain trauma.
However, there are some limitations to this study that are important to address. First, while comparable in size to many similar studies, our sample is still relatively small and undoubtedly, further evaluation of the biomarkers will come from future studies. Second, the microRNAs analyzed in the validation set have been selected entirely on the results obtained in the discovery set, which consists of a small population and does not include isolated TBI or EC patients only. Third, the GCS was used to categorize injury severity; however, this score alone does not completely encapsulate the severity or complexity of injury. Other approaches could have been used—for example, models including multiple injury and demographic parameters—but we have chosen to follow a pragmatic classification tool that is used in the field by rescue services and non-expert clinicians. Some mTBI subjects included in this investigation experienced PTA > 24 h and <7 days, which is considered to be a moderate injury depending on the classification, and some have visible abnormalities on structural neuroimaging that has been defined as a “complicated mTBI.” Therefore, some mTBI cases would have been classified as more severe using a different taxonomy and it is also clear that some of the multi-dimensionality of TBI is lost by using GCS alone. Undoubtedly, it would be useful to investigate whether miRNA biomarkers might also be able to predict radiological abnormalities and duration of PTA, particularly at the early time-point of 0–1 h. However, a larger sample size would be needed to specify a more complex predictive tool in order to avoid the risk of overfitting the model.
Fourth, the GOSe, although widely utilized in TBI practice and research, is not particularly sensitive to mild injuries and may not sufficiently capture the discriminatory power of miRNAs in prognostication. We initially attempted to include a more comprehensive battery of self-reported outcomes, such as the Quality of Life after Brain Injury, Patient Health Questionnaire (PHQ) and the Post-Traumatic Stress Disorder (PTSD—civilian version), but this strategy was abandoned early on due to poor compliance. On the other hand, we were able to obtain GOSe scores on all subjects. Finally, the ordinal regression analysis, although commonly used in the TBI literature, has limitations derived from the fact that clinical data are differently recorded in mTBI and sTBI. This could result in an oversimplified model.
In conclusion, four candidate biomarkers were selected from a panel of 754 microRNAs, with both miR-425-5p and miR-502 being identified as valid candidates to assess the mTBI+EC. Both biomarkers are specific for brain-injured patients only. Mir-21 and miR-335 are promising candidates for sTBI+EC, with the former being specific for brain injury and the latter as a potential biomarker for sTBI associated with polytrauma.
Footnotes
Acknowledgments
This study was funded by the National Institute for Health Research (NIHR) and by the Midlands Neuroscience Training and Research Fund. The views expressed are those of the authors and not necessarily those of the National Heath Service, the NIHR or the Department of Health.
Author Disclosure Statement
The University of Birmingham has filed a patent on the microRNAs here described.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.