
Abstract
Accelerated long-term forgetting (ALF) is characterized by adequate recall after short, but not long delays. ALF is not detected by standardized neuropsychological memory tests. Currently, the prevailing conceptualization of ALF is of a temporal lobe seizure-related phenomenon. Nevertheless, Mayes and colleagues (2003) proposed that ALF may occur when any of the components of the brain network involved in long-term memory formation, or their interaction, is disrupted. This disruption does not have to be caused by temporal lobe seizures for ALF to occur. Here, we investigate this possibility in a group of school-age children who have sustained traumatic brain injury (TBI) (n = 28), as TBI typically disrupts the brain network that is important for long-term memory formation and recall. Healthy control children (n = 62) also participated. Contrary to the dominant conceptualization of ALF being a seizure-related phenomenon, children with TBI showed ALF. Sustaining a severe TBI and diffuse subcortical damage was related to ALF. Individually, 8 of the 13 children with severe TBI presented with ALF. ALF would remain undetected on standardized testing in six of these eight children. One child had the opposite pattern of dissociation, an impaired score on standardized testing, but an average long-term memory score. This is the first study, to our knowledge, to show ALF in patients with TBI, which has remained undiagnosed and untreated in this patient population. Our study also challenges the dominant hypothesis of ALF being a temporal lobe seizure-related phenomenon, and raises a possibility that short-term and long-term memory systems may be independent.
Introduction
A
ALF has been found in studies involving patients with epilepsy, with most studies involving adult patients with temporal lobe epilepsy (TLE) 6 –21 and transient epileptic amnesia (TEA), 22 –26 which is thought to represent a particular manifestation of TLE. ALF has also been found in children with TLE 27 and in patients with epilepsy whose seizures do not emanate from the temporal lobes: children with idiopathic generalised epilepsy (IGE) 28,29 and adults with extratemporal epilepsy. 20 Moreover, several group studies found associations between ALF and seizure variables: seizure frequency, 14,21 seizures that generalize, 18 and subclinical discharges. 30 Treatment with antiepileptic medication was also found to resolve ALF in some (but not all) patients with TEA. 24,31
In contrast to evidence of ALF being a seizure-related phenomenon, several lines of evidence suggest that ALF may not be seizure related. First, patients with TEA, who present with ALF, are often free of clinical seizures. 26,32 Second, some seizure-free patients with TLE also exhibit ALF. 18 Third, Muhlert and colleagues 17 did not find ALF in adults with IGE. Fourth, it has been proposed that in patients with epilepsy, ALF may be related not only to seizures and interictal encephalographic (EEG) abnormalities, but also to associated structural lesions. 33 Fifth, in a recent review, Geurts and colleagues 34 observed that evidence of accelerated forgetting (although originally not termed ALF) was found in 3 out of 11 studies that examined long-term forgetting in neurological patients (with Alzheimer's disease and mild cognitive impairment) with no history of epilepsy. It is possible that the discrepancies in findings may be, in part, the result of differences in methodology (see Elliott and colleagues 35 for a review) and developmental factors (i.e., ALF found in children with IGE, but not in adults with IGE). It is also possible that structural lesions to any of the components of the brain network involved in long-term memory formation, without seizures, could result in ALF.
Traumatic brain injury (TBI) provides an excellent model to test whether seizures are necessary for ALF, as severe closed TBI often results in contusions of the mesial temporal and frontal lobes and diffuse white matter (axonal) injuries. 36 White matter injuries are more common, and cortical contusions are less common in children than in adults, because of differences in biomechanical features of the developing brain. 37 As long-term memory formation is proposed to involve a process of consolidation that takes a long time (i.e., days or weeks) to complete and requires ongoing interaction between the mesial temporal and distributed neocortical networks, 4,38 this combination of diffuse subcortical and focal cortical injuries could disrupt long-term memory formation. In addition, injuries to the frontal lobe or disruption of interaction between frontal lobes and neocortical storage sites may result in deficits in retrieval of established memory stores, as the frontal cortex plays an increasingly important role 39 in effortful retrieval of information from long-term stores. 40 Formation and retrieval of long-term memory is critical for children, as it underpins development of knowledge and developmental progression. Retrieval of information from long-term memory stores at various delays (i.e., days, weeks, months) allows children to succeed academically and to utilize this information adaptively (i.e., in social interaction when required to recognize faces and recall of names or discuss events in which they participated).
In children with TBI, a dose-response relationship between injury severity and memory deficits has been consistently found on standardized testing; children with more severe injuries had poorer memory outcomes. Studies involving children with severe TBI have repeatedly found that memory deficits involve different memory skills: working memory, 41 encoding/learning, and recall after short delays. 42 –46 Although not a universal finding, in a number of studies, memory skills of children with mild/moderate TBI were comparable to the norms/control groups; 42 –46 however, in one study, mild difficulties with retrieval were reported in children with mild/moderate TBI. 46 Further, children with TBI and their parents frequently report experiencing memory difficulties in everyday living. 47,48 Inspection of studies that used qualitative methodology to examine memory deficits in children with TBI 48 and children with epilepsy 49 suggests that the range of memory problems displayed in day-to-day life greatly exceeds memory skills measured by standardized tests. Among other deficits, difficulties in retaining information from one day to another have been reported, which cannot be captured by standardized testing that uses short delays (minutes) only.
The primary aim of this study was to determine whether children with TBI, who have never experienced overt seizures, had deficits in memory for verbal information on long delays that were greater than expected from their performance on standardized memory tests. We chose to study long-term verbal memory for two reasons. First, in studies that used both verbal and visual material to assess long-term memory formation, ALF was consistently found on verbal tasks, 6,11,14,17,18,21,27 –30,50 but only sometimes on visual tasks as well. 6,11,14,17,21,30 Second, the verbal memory task used in this study has been validated on typically developing children and children with epilepsy. 27,28 We also investigated the relationships between injury severity and memory for verbal information on long delays, and explored relationships between the site of lesions and long-term memory formation. We aimed to control for possible deficits in verbal working memory and encoding/learning, as these deficits were common in children with TBI and could impact long-term recall. Based on reviewed literature, we predicted that relative to controls, children with severe TBI, but not mild to moderate TBI, would have greater deficits in memory for new verbal information following a long delay (7 days) than was expected from their performance after short delays. We expected that injuries to the temporal lobe and frontal lobe and/or diffuse axonal injuries, which were all common post-TBI, would be associated with ALF. These long-term verbal memory deficits would not be (1) explained by impaired verbal working memory and encoding/learning or (2) evident on standardized memory tests that required recall of verbal information at short 20–30 min delays.
Methods
Subjects
Children with TBI were recruited from the Rehab2Kids ward at Sydney Children's Hospital (Randwick) between October 2013 and February 2016. Inclusion criteria were: (1) evidence of having sustained an accidental TBI of any severity (involving alteration of consciousness or significant neuroimaging findings) ≥12 months earlier, (2) being between 8 and 16 years of age, and (3) being fluent in English. Exclusion criteria were: (1) major pre-existing developmental/psychiatric/other neurological disorder (i.e., intellectual disability, autism, brain tumors), (2) significant sensory/motor impairments (i.e., cerebral palsy, significant visual or hearing impairments) that would interfere with task completion in the study, or (3) a history of seizures (in children with TBI: preceding the TBI as well as post- TBI).
A total of 93 participants were identified through searches of the database and review of clinical/medical records against the inclusion/exclusion criteria. Twenty-nine declined participation because of inconvenience of time and/or travel requirements (n = 8), lack of interest in the study (n = 4), lack of cognitive concerns (n = 1), denial of the reported TBI (n = 2), involvement in another study (n = 2), parent or caregiver not wishing to put the child through additional testing (n = 2), or reasons unknown (n = 10). A further 21 were unable to be contacted. Thirty-one children agreed to participate in the study and were tested. Three were not included in the final sample for the following reasons: becoming uncooperative on assessment (n = 1), coming under investigation for additional neurological illness unrelated to TBI (n = 1), and omission of the experimental verbal memory measure from the testing protocol (n = 1).
The final sample included 28 children whose injury severity was classified as (1) mild (n = 3) Glasgow Coma Score (GCS) of 13–15, post-traumatic amnesia (PTA) <24 h and no intracranial abnormality on CT or MRI scan, (2) moderate (GCS of 9–12, n = 12), PTA 1–7 days and/or evidence of abnormalities on CT/MRI, and (3) severe (n = 13) GCS of 3–8 and/or PTA >7 days and evidence of abnormality on CT/MRI. 42 Given the small number of children with mild TBI, and comparable memory outcomes being found in previous studies that included children with mild and moderate TBI, 42 –46 children with mild and moderate TBI were treated as one group (mild-moderate). GCS was taken on admission or at scene/during transfer by ambulance (when GSC on admission was not available), except in one patient who was <1 year of age at the time of injury and had no GCS recorded. In this case, TBI was classified by a treating medical specialist as severe based on imaging evidence (i.e., CT scan: minimally depressed right temporoparietal fracture, left frontal hemorrhagic cortical contusion, a falcine subdural hemorrhage, and predominantly right-sided subarachnoid blood) and clinical signs.
Sixty-two normal control (NC) children, who met the same inclusion criteria, but did not have a history of TBI, also participated. The NC group was recruited via passive snowballing. All children who contacted us were suitable for the study. Demographic and injury characteristics of the sample are provided in Table 1.
Cohen's d.
Phi coefficient.
Two patients with mild to moderate injuries did not have scans or reports on the scans in their files.
TBI, traumatic brain injury; SES, socioeconomic status; ADHD, attention- deficit/hyperactivity disorder; LD, learning difficulties; WASI, Wechsler Abbreviated Scale of Intelligence; FSIQ, full-scale intelligence quotient; WISC-IV, Wechsler Intelligence Scale for Children, 4th Edition; WRAML-2, Wide Ranging Assessment of Memory and Learning, 2nd Edition; GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia; MVA, motor vehicle accident.
Materials
Intelligence
Two subtests (Vocabulary and Matrix Reasoning) from the Wechsler Abbreviated Scale of Intelligence (WASI) 51 were used to estimate a Full-Scale IQ (FSIQ) (mean = 100, SD = 15).
Verbal working memory
The Digit Span subtest of the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV) 52 was employed. Scores obtained on the Digits Forward and Digits Backward components of this subtest were considered separately. Age scaled scores (mean = 10, SD = 3) were employed.
Verbal memory: learning and recall
Verbal learning (immediate recall) and retention after a standard short delay (20–30 min) was evaluated using the Story Memory subtest from the Wide Ranging Assessment of Memory and Learning, Second Edition (WRAML-2). 53 Age scaled scores (mean = 10, SD = 3) obtained on the immediate recall and 30 min delay were used in the study.
Experimental verbal memory task
An adapted version of the California Verbal Learning Test for Children (CVLTC) 54 developed by Gascoigne and colleagues 28 examined retention of verbal material over short and long delays. Instead of a 15 word list, which was found too demanding in our pilot study, children <9 and ≥9 years of age were presented with a 9 or 12 word list, respectively. The list was read to participants until all words were recalled on two consecutive learning trials or participants completed a maximum of 12 learning trials. Next, participants were read and asked to recall an interference list immediately following the presentation. A recall of the first list was requested after 2 min, 30 min, and 1 week, without forewarning. On completion of recall at 1 week only, a recognition list was presented to participants who were asked to indicate whether or not each of the words was included in the first list. One week recall and recognition were conducted via telephone. In the current study we employed the following scores: number of learning trials (learning efficiency), proportion of words recalled (maximum 100%) relative to last learning trial (recall), and d prime (d', a sensitive measure of recognition that considers correctly and incorrectly recognized words 55 ).
Site of brain injury
Two authors (S.L. and C.G.) independently reviewed reports of brain scans obtained for clinical purposes during acute admissions. Focal (frontal, temporal, extrafrontotemporal, and subcortical) and diffuse subcortical injuries were noted for each patient. When discrepancies in reviews of reports were found, the reports were reviewed jointly and discussed and discrepancies were resolved.
Procedure
The study was conducted in accordance with the approval granted by the Sydney Children's Hospitals Network Human Ethics Committee. Only children who agreed to participate and whose parents provided informed written consent were included in the study.
Parents of children with TBI who met our inclusion criteria on review of medical records were sent an invitation letter. To recruit control participants, we distributed the advertisement for the study through social networks of parents of children with TBI and researchers. In addition, we sent advertisements in local organizations (i.e., community halls, independent schools).
A semistructured interview was conducted over the telephone with parents of children interested in the study to provide further information about the study and confirm eligibility. For children who were included in the study, information about main caregiver's education was collected and used as a measure of socioeconomic status. All participants were assessed over two sessions. The first assessment was conducted in a quiet room in the hospital or in participants' homes. At the conclusion of the first session, a 7 day follow-up telephone call was scheduled with the parents of participants. Participants were told that the telephone call would allow them to provide feedback about the study and not to rehearse the content of any assessment materials. During the second session (i.e., the 7 day follow-up telephone call), participants were asked to recall previously learned words. A qualified psychologist administered all tests.
Statistical analysis
IBM SPSS version 21 was used for the analyses. Two tailed tests were conducted (unless specified otherwise), with a standard α of 0.05. The expectation maximization algorithm 56 was employed to estimate missing values (two data points for TBI and three data points for NC participants for 7 days recall/recognition), which were missing at random (Little's Missing Completely at Random test χ2 (84) = 0.144, p = 0.93).
Between-group differences on all categorical variables were assessed with χ2 tests. For continuous cognitive and demographic variables (1) one way analyses of variance (ANOVAs) tested differences between the mild-moderate TBI, severe TBI, and control groups, and (2) t tests assessed differences between the two TBI groups. On the experimental verbal memory task, a repeated measure (group [mild-moderate, severe, control] × delay [2 min, 30 min, 7 days]) ANOVA and one way ANOVA assessed between group differences in recall and recognition, respectively. When significant findings were obtained, post-hoc contrasts were completed. Šidák corrections for multiple comparisons were used.
Given our a priori hypothesis that indices of injury severity and injuries to the consolidation network would be related to greater declines in recall of words over delays, one tailed Spearman's correlations were used to explore relations between injury variables and declines in recall of words over delays. As the declines were not normally distributed, Spearman's correlations were used. Only those injury variables on which TBI groups differed were used in this analysis to reduce the number of unnecessary correlations.
To examine whether background and cognitive variables on which control and TBI groups differed related to declines in recall of words and recognition accuracy, a two-step approach was used. First, Spearman's correlations were obtained. Second, cognitive and background variables that were related to recall and recognition accuracy were used as covariates in the analyses of covariance (ANCOVAs).
Finally, to further examine the frequency of ALF in children with TBI and whether participants with TBI who presented with ALF on the experimental verbal memory task would be identified as having memory deficits on the recall of the Story Memory-Delay, and vice versa, we scrutinized patterns of performance across these two tasks for each child. Scores that fell ≤ −1.35 SD below the mean were defined as impaired, and scores ≥ −0.67 SD from the mean were considered average. These cutoff scores represent the borderline range and below (z ≤ −1.35) and the average range and above (z ≥ −0.67) in the Wechsler classification of ranges of intellectual function. 52,57 The use of nonadjacent ranges to classify scores as either impaired or average avoided the issue of having scores very close in magnitude being classified as impaired or average. 58 The scores that fell in between these ranges were classified as neither. On the experimental verbal memory task, z scores were calculated using the mean and SD of a control group for a decline from 30 min (commonly used delay on the standardized tests) to 1 week (indicative of ALF). On this task (1) the borderline range and below was defined as z ≥ 1.35 (≥ 91%), as a greater decline indicated a worse score, and (2) the average range and above was defined as z ≤0.67 (≤ 75%), as a smaller decline indicated a better score. On the Story Memory-Delay, age-scaled scores of ≤6 (z ≤ −1.35, ≤ 9%) and ≥8 (z ≥ −0.67, ≥ 25%) were classified as borderline and average, respectively.
Results
Between-group comparison of background variables and scores obtained on standardized tests
The TBI and NC groups did not differ in age, family socioeconomic status, presence of learning disabilities, or sex distribution (see Table 1). Chi-square analysis, however, revealed that the groups differed significantly in the number of children diagnosed with attention-deficit/hyperactivity disorder (ADHD). The mild-moderate TBI group had significantly more children diagnosed with ADHD (n = 4, two diagnosed pre- and two post- TBI) relative to the severe TBI and NC (n = 0, in both) groups.
Table 1 shows scores obtained on standardized tests. ANOVA indicated that the between-group differences in FSIQ were significant. Post-hoc analyses showed that both TBI groups had significantly lower FSIQ than the NC group (mild-moderate, p = 0.03; severe, p = 0.002). The two TBI groups, however, did not differ in the FSIQ (p = 0.81). On standardized verbal memory tests, TBI and NC groups obtained comparable scores on measures of verbal working memory (Digits Forward and Digits Backward) and verbal learning (Story Memory-Immediate). In contrast, the groups differed in the recall of verbal information after a standard 30 min delay (Story Memory-Delay). Post-hoc analyses indicated that the severe TBI group received significantly lower scores than the NC group (p = 0.02). Other between- group differences were nonsignificant (severe TBI compared with mild-moderate TBI, p = 0.34; mild-moderate TBI compared with NC, p = 0.72).
T tests assessed differences between TBI groups on injury variables. Relative to the mild-moderate TBI group, the severe TBI group had significantly (1) lower GCS, (2) longer duration of PTA, and (3) higher proportion of children with frontal lobe and diffuse subcortical injuries. The two groups, however, did not differ in the age at injury and time since injury.
Between-group comparisons on the experimental verbal memory task
An ANOVA showed a significant effect of group on the number of trials to reach the criterion for the experimental verbal memory task (F[2,87] = 17.68, p < 0.001, d = 1.28). Compared with the NC children (mean = 6.24, SD = 2.39), children with mild-moderate TBI (mean = 9.27, SD = 3.03) and severe TBI (mean = 10.15, SD = 2.82) required a greater number of trials to reach criterion (p < 0.001, d = 0.88 and p < 0.001, d = 1.07 respectively). The number of trials to reach criterion did not differ between the TBI groups (p = 0.74, d = 0.19). Additionally, there was a significant difference in the distribution of children who did not meet the learning criterion; with four children in each of the TBI groups not meeting the criterion as compared with none from the NC group (χ2 = 19.59, p ≤ 0.001, Φ = 0.47).
A two way repeated-measure ANOVA found a significant interaction between group and delay (F[4,174] = 6.93, p < 0.001, d = 0.80; See Fig. 1). Planned contrasts revealed that compared with the NC group, the severe TBI group had significantly greater declines in the proportion of words recalled from both short delays to the long delay: 2 min to 7 days (F[1,87] = 12.07, p = 0.008, d = 0.75) and 30 min to 7 days (F[1,87] = 19.13, p < 0.001, d = 0.93), but not from 2 min to 30 min (F[1,87] = 0.52, p = 0.99, d = 0.26). The declines in the proportion of words recalled by the mild-moderate TBI group did not differ from the NC group either at short or at long delays: 2 min to 30 min (F[1,87] = 0.66, p = 0.99, d = 0.18), 2 min to 7 days (F[1,87] = 1.96, p = 0.81, d = 0. 30) and 30 min to 7 days (F[1,87] = 1.32, p = 0.92, d = 0.25). When the two TBI groups were compared, declines in the proportion of words recalled were not significant {2 min to 30 min (F[1,87] = 0.24, p = 0.92, d = 0.26); 2 min to 7 days (F[1,87] = 3.01, p = 0.48, d = 0.35); 30 min to 7 days (F[1,87] = 7.02, p = 0.09, d = 0.57)}. A main effect of delay (F[2,174] = 105.04, p ≤ 001, d = 2.5), but not group (F[2,87] = 1.65, p = 0.20, d = 0.39), was found. Post-hoc analyses showed that across groups a decline in the proportion of words recalled was significant from both 2 min and 30 min to 7 days (ps < 0.001), but not from 2 min to 30 min (p = 1.0).
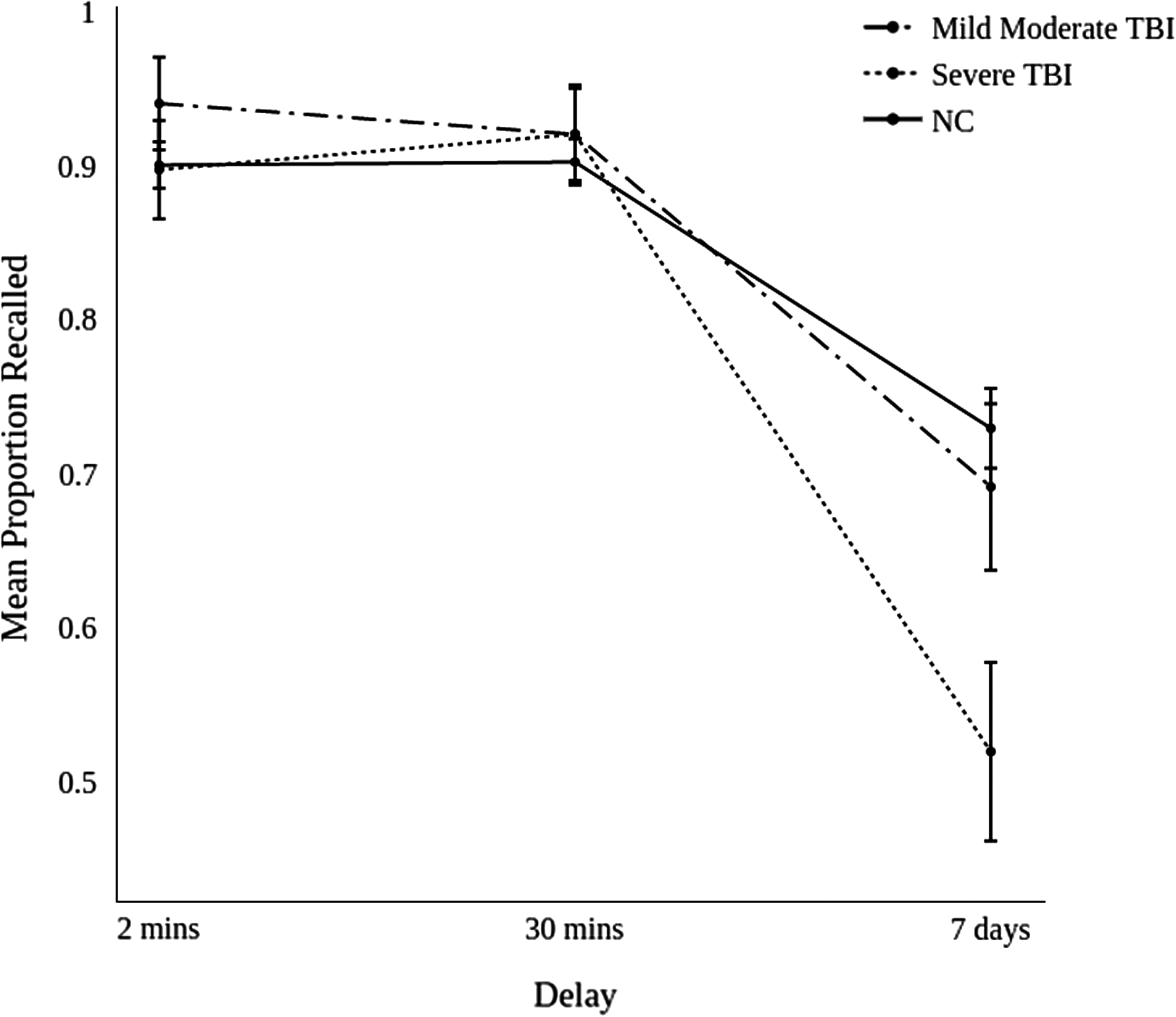
Mean (standard error) proportion of words recalled relative to the last learning trial on the experimental verbal memory task across delays by mild/moderate traumatic brain injury (TBI), severe TBI, and normal control (NC) groups.
A one way ANOVA did not find a significant difference between the groups (NC [mean = 3.25, SD = 0.57], mild-moderate TBI [mean = 2.98, SD = 0.5], severe TBI [mean = 2.87, SD = 0.64]) in recognition accuracy (F[2,87] = 2.93, p = 0.06, d = 0.52).
Relationship between injury variables and declines in recall on the experimental verbal memory task
Spearmen correlations between a decline in the proportion of words recalled on the experimental verbal memory task and injury variables on which the two TBI groups differed were shown in Table 2. Lower GCS score and having sustained a diffuse subcortical injury were associated with greater declines in the proportion of words recalled from 30 min to 7 days. No other correlations were significant.
GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia.
Relationship between ALF and between-group differences on background and cognitive variables
To examine this question, we correlated declines in the proportion of words recalled from 2 min to 30 min, 2 min to 7 days, and 30 min to 7 days on the experimental verbal memory task with variables on which significant between-group differences were found: ADHD diagnosis, FSIQ estimate, 30 min recall of the Story Memory, and learning efficacy on the experimental verbal memory task (reaching learning criteria and trials taken to reach learning criteria). All correlations were small and nonsignificant (see Table 3). Therefore, further planned ANCOVAs were not performed.
WASI, Wechsler Abbreviated Scale of Intelligence; FSIQ, full-scale intelligence quotient; ADHD, attention-deficit/hyperactivity disorder; WRAML-2, Wide Ranging Assessment of Memory and Learning, 2nd Edition.
The frequency of ALF in children with TBI and possible detection of ALF in individual children with TBI on 30 min delays used on standardized verbal memory tests
To answer these questions, we examined the pattern of performance of each child with TBI and classified their scores as average, impaired, or neither on the experimental verbal memory task (the decline from 30 min to 7 days) and the standardized verbal memory test (Story Memory-Delay). The patterns of performance in individual TBI participants are presented in Table 4.
Neither indicates that the scores fell between the cutoff criteria for impaired and intact performance
Designates a number of cases with a dissociation in performance between verbal memory measure (children who had impaired performance on one measure but average performance on another measure).
TBI, traumatic brain injury; WRAML-2, Wide Ranging Assessment of Memory and Learning, 2nd Edition; ALF, accelerated long-term forgetting.
On the experimental verbal memory task, the decline in scores from 30 min to 7 days were average for 13 (11 mild-moderate, 2 severe), impaired for 10 (2 mild-moderate, 8 severe) and neither for 5 (2 mild-moderate, 3 severe) out of 28 children with TBI. Hence 10 children with TBI showed ALF.
To determine whether ALF would be detected by the standardized verbal memory test the two tests were considered concurrently. The patterns were: (1) scores falling in the average range on both tasks (n = 12; 11 mild-moderate,1 severe), (2) impaired retention (decline) from 30 min to 7 days on the experimental verbal memory task, but average score on the standardized verbal memory test (n = 8; two mild-moderate, six severe), effectively showing ALF that would not be detected by the standardized test, (3) impaired on both tasks (n = 2; both severe) and (4) average retention (decline) from 30 min to 7 days on the experimental task, but impaired score (30 min recall) on the standardized test (n = 1; severe).
Discussion
Our study provides several novel findings. First, the study reveals ALF for verbal materials in some children who have sustained severe TBI. Lower GCS and diffuse subcortical injuries were associated with a greater decline from the standard short (30 min) to a long (7 days) delay. Second, the study shows that ALF is not related to scores obtained on standardized memory tests, such as those that involve recall of stories after short delays. Although our participants with severe TBI were impaired on the delayed story recall relative to the control participants, correlations between the delayed story recall and ALF were small and nonsignificant. This finding is critical for clinical work, as many patients with ALF are likely to remain undiagnosed on standardized memory tests. Third, our study provides further evidence of a single dissociation between short-term and long-term memory (average short-term, but impaired long-term memory score). Moreover, our study raises a possibility of a double dissociation between short-term and long-term memory systems (as one child showed the opposite pattern of dissociation: impaired short-term, but average long-term memory scores), which warrants further investigations because of potential theoretical and clinical implications.
Our study confirms that standardized memory tests are not sensitive to ALF, which is of clinical significance. In our study, children with severe TBI were impaired on the standardized memory test that required the delayed recall of stories. Nevertheless, the scores obtained on the delayed recall of stories were not related to ALF. In addition, in our study, ALF could not be explained by either reduced working memory or poor encoding/learning, as children with severe TBI and control participants performed comparably on the standardized tests of working memory and verbal learning. Hence ALF is likely to remain undetected and undiagnosed in clinical practice because of the lack of standardized instruments that are sensitive to this recently discovered memory disorder. It is of interest to compare our findings with purported brain correlates of ALF put forward by Mayes and colleagues. 6 We found that ALF was related to the presence of diffuse subcortical injuries in children with TBI. In our sample, ALF was not related to frontal lobe injuries, and temporal lobe injuries were infrequent. Our findings are consistent with the proposal of Mayes et al. 6 that ALF may arise not only from the focal cortical damage, but also from the disruption of the interactions between the cortical regions involved in the process of long-term memory formation. Hence diffuse subcortical injuries could have disrupted interaction between cortical sites involved in long-term memory consolidation. Nevertheless, whereas the findings of the brain scans considered in the current study were performed during acute hospital admission, assessment took place 4–5 years post-injury. However, child neuroimaging research has shown that reductions in brain volumes may present many years post-injury, suggesting that TBI may adversely impact and perturb subsequent brain growth and development. 10 Therefore, although our findings suggest that children with evidence of diffuse subcortical injuries in the acute stage of recovery from TBI may be at risk of ALF, determining structural correlates of ALF in children with TBI requires that cognitive testing and brain scans be performed simultaneously.
Although our study provides evidence of ALF in children with TBI who were free of epilepsy, ALF was apparent on recall. The between-group differences did not reach significance on recognition. In part, this pattern of ALF may be because of the distribution of brain injuries in our sample. In our study, focal temporal lobe injuries were less frequent than diffuse subcortical injuries and frontal injuries, especially in children who sustained severe TBI. This relative sparing of temporal lobes and other neocortical regions in our study may explain the lack of between-group differences in recognition, as neocortical sites are proposed to play an important role in long-term storage. As memories mature, recall of information becomes more effortful and the frontal cortex plays an increasingly important role, 39 especially in the effortful retrieval of information from long-term stores. 40 Although the relationship between a decline in recall from a standard delay to a long delay and frontal injuries has not reached significance in the current study, a trend was found, with a tendency for children with frontal injuries to have a greater decline. In the current study, the decline in the proportion of words recalled from the standard to the long delay is related to the presence of diffuse subcortical injuries, which could have hindered the interaction between the retrieval critical frontal lobes and distributed neocortical storage sites. Taken together, our findings suggest that children with TBI might have stored information into long-term memory stores, but had difficulties retrieving this information on long delays. As noted in a previous study, 48 one parent reported that “It's all in there but she can't pull it out.” Further inspection of our findings, however, suggests that the long-term storage of information may not be quite as robust in children with TBI as it is in typically developing children. We notice that the between-group difference just failed to reach significance (p = 0.06) on recognition, which was only administered on a long delay. Moreover, our analysis revealed a strong effect size (d = 0.52) with the mean recognition accuracy of children with TBI being lower than the mean recognition accuracy of the control children. These findings are consistent with the extended statement of the same parent whose report indicated that the child had difficulties with retrieval. The parent went on to say that “Some things she can't recall, even with lots of reminders.” 48 Overall, our study provides evidence of significant deficits in retrieval of information at long delays, but also raises a possibility that recognition may not be intact, and that long-term memory stores of children with TBI may be somewhat dilapidated.
Analysis of individual data provides further support of ALF being frequently present in children with TBI, and highlights the importance of the findings for clinical (individual) work. Using current standardized instruments, 8 out of 28 children with TBI would be informed that they have no difficulties in recall of new verbal information, based on the average score on the standardized tests that requires recall of story details after a short, 20–30 min delay. However, these same eight children had marked impairment in recall of verbal information after 7 days. Moreover, if deficits were found in visual memory on standardized testing, these children and their parents would typically be advised to use intact verbal memory skills to compensate for their visual memory deficits. Our findings underscore the urgent need for the development of standardized procedures that will increase the scope and accuracy of memory assessments, and adequately inform treatment of memory deficits in clinical settings.
Our analysis of individual data identified one child with TBI who presented with the opposite pattern of impaired and preserved skills to ALF: impaired recall after a short delay, but adequate recall after a long delay. Such a pattern of performance is of further theoretical and clinical interest. Theoretically, it supports a possibility that the system involved in long-term memory consolidation may operate somewhat independently of the system involved in recall of information after short delays. It is possible, however, that this child (1) had initially learned and stored more information than suspected on the basis of his recall after a short delay, which could be investigated by administration of a recognition condition at short delay, or (2) has fluctuations in his performance caused by other cognitive deficits, such as problems with attention, which are very common following severe child TBI. 59 –62 Moreover, it is possible that this is a testing artefact and/or a chance finding, as only one child showed this opposite pattern of dissociation in our study. Clinically, if the findings are valid, this child would not require intervention to support his retention of information over time, which might have seemed warranted from the standardized testing.
Our study has some limitations. Although the study employed a method that has been previously used in studies that found evidence of ALF in children and adults with epilepsy – a learning to criterion approach 8,13,15,17,27 28,63 – it has been argued that such an approach could limit the sensitivity of the test to detect forgetting over short (30 min) delays because of the ceiling effect. 35 However, it is important to note that we concurrently employed a standardized verbal memory test that included a single presentation of prose passages that were recalled immediately and 30 min following the presentation. Moreover, recall of prose passages at 30 min and a decline in recall on the experimental task at 7 days were not correlated. Taken together with the findings of the individual analysis, these findings suggest that ALF may not be an artefact of a methodology, although further studies addressing this issue are warranted. Moreover, although children who participated in this study have not experienced overt seizures, we cannot exclude the possibility of subclinical epileptiform discharges, as we did not use concurrent EEG. In addition, our study included a convenience sample rather than a randomly selected sample or a sample of consecutively admitted children. Finally, as this is the first study to find evidence of ALF in children who do not have epilepsy, replications are needed.
Conclusion
In summary, even though children with TBI included in this study were free of a history of epilepsy, they were found to be at risk of ALF. Our findings suggest that ALF may be present in patients with neurological conditions other than epilepsy, which alerts to an urgent need to study neurological patients with structural lesions in the network involved with long-term memory formation and retrieval. The finding of a double dissociation in retrieval from the short-term and long-term memory storage is intriguing, but requires replication. The development and standardization of clinical tools that would enable the reliable assessment of memory beyond short delays is urgently needed.
Footnotes
Acknowledgments
This work was in part supported by the Memory Node of the ARC Centre of Excellence in Cognition and its Disorders and by The University of Sydney Thompson Fellowship awarded to S.L. We thank the staff from the brain injury programs at Sydney Children's Hospital (Randwick) who assisted with recruitment. We also express our gratitude to the families who participated in this study.
Author Disclosure Statement
No competing financial interests exist.