
Abstract
Efforts to validate novel therapies in acute clinical trials for spinal cord injury (SCI) are impeded by the lack of objective quantitative measures that reflect injury severity and accurately predict neurological recovery. Therefore, a strong rationale exists for establishing neurochemical biomarkers that objectively quantify injury severity and predict outcome. Here, we conducted a targeted proteomics analysis of cerebrospinal fluid (CSF) samples derived from 29 acute SCI patients (American Spinal Injury Association Impairment Scale [AIS] A, B, or C) acquired at 24, 48, and 72 h post-injury. From a total of 165 proteins, we identified 27 potential biomarkers of injury severity (baseline AIS A, B, or C), with triosephosphate isomerase having the strongest relationship to AIS grade. The majority of affected proteins (24 of 27) were more abundant in samples from AIS A patients than in those from AIS C patients, suggesting that for the most part, these proteins are released into the CSF more readily with more severe trauma to the spinal cord. We then analyzed the relationship between CSF protein abundance and neurological recovery. For AIS grade improvement over 6 months, we identified 34 proteins that were associated with AIS grade conversion (p < 0.05); however, these associations were not statistically significant after adjusting for multiple comparisons. For total motor score (TMS) recovery over 6 months, after adjusting for baseline neurological injury level, we identified 46 proteins with a statistically significant association with TMS recovery. Twenty-two of these proteins were among the 27 proteins that were related to baseline AIS grade, consistent with the notion that protein markers that reflect a more severe injury also appropriately predict a poorer recovery of motor function. In summary, this study provides a description of the CSF proteome changes that occur after acute human SCI, and reveals a number of protein candidates for further validation as potential biomarkers of injury severity.
Introduction
T
A number of clinical trials of novel interventions for acute SCI have been conducted 5 and an increasing number of trials are being initiated as promising interventions emerge from the laboratory setting and seek human translation. 6 Despite this, treatments that can significantly improve neurological recovery after acute SCI remain limited, in part because of inherent challenges of conducting clinical trials in acute SCI. 7,8 Fundamental to this challenge is the fact that currently (and historically), individuals with acute SCI who are eligible for clinical trials must be evaluated with a detailed neurological assessment and appropriately stratified according to baseline degree of neurological impairment. In its current format, the International Standards for Neurologic Classification of SCI (ISNCSCI) examination requires acute SCI patients to be conscious and cooperative enough to participate in a fairly detailed assessment of motor and sensory function. 9,10 However, many such patients cannot be examined reliably upon arrival in the emergency room because of concomitant injuries or pharmacological sedation/intoxication. 11,12 This renders many acute SCI patients ineligible for clinical trials and slows recruitment for these studies. Also, even when a baseline assessment can be performed, there is considerable variability in spontaneous neurological recovery among individuals stratified according to the American Spinal Injury Association Impairment Scale (AIS). 13 As a result, clinical trials with small numbers of patients are typically underpowered to establish efficacy, leading to uncertainty as to whether the treatment in question is having the intended biological effect, and thus stalling progression of potentially effective therapies along the clinical pipeline.
As an adjunct or alternative to the standard ISNCSCI neurological assessment, molecular biomarkers to objectively stratify injury severity, predict neurological recovery, and act as surrogate outcome measures would be extremely useful for the field, 14,15 and could have an important role in facilitating translation of novel SCI therapies. Interest in neurochemical biomarkers is particularly strong in other neurological conditions such as traumatic brain injury (TBI), Alzheimer's disease, and Parkinson's disease. 16 In general, all fields of neuroscience share similar goals and face comparable challenges in making appropriate diagnoses, stratifying disease severity in an objective manner, predicting outcome, and establishing biological measures of treatment outcome. Additionally, although those working toward such biomarker discovery efforts are eager to establish biomarkers within blood, it is intuitive that the analysis of cerebrospinal fluid (CSF) provides a more representative picture of the injured/diseased central nervous system.
We have been enrolling individuals with acute SCI into a prospective observational study in which CSF samples are accrued over 3–5 days through indwelling lumbar intrathecal catheters. In previous work, we identified a series of inflammatory markers (interleukin [IL]-6, IL-8, and monocyte chemoattractant protein [MCP]-1) and structural proteins (tau, S100β, and glial fibrillary acidic protein [GFAP]) that appeared promising as neurochemical biomarkers of injury severity. 17,18 Although we have continued to analyze inflammatory cytokines and structural proteins within the CSF, we acknowledge that this panel of proteins represents a very small subset of the proteomic responses to injury. Here, we describe a targeted proteomic analysis of CSF samples accrued serially over 72 h from 29 individuals with acute SCI. This represents, to our knowledge, the largest series of human patients in which CSF samples serially acquired during the acute injury phase have been subjected to proteomic analyses.
Methods
Clinical trial enrolment
Individuals sustaining an acute SCI (Table 1) were enrolled into this prospective observational study if they met the following inclusion criteria: 1) AIS grade A, B, or C SCI upon presentation; 2) spinal injury between C3 and T11 inclusive; 3) within 48 h of injury; and 4) the ability to provide a valid, reliable neurological examination. Patients were excluded if they had concomitant brain injuries or concomitant major trauma to the chest, pelvis, or extremities that required invasive intervention (e.g. chest tube, internal or external fixation), or were too sedated or intoxicated to provide a valid neurological examination. Although the inability to provide a neurological examination was a significant impediment to patient recruitment, having a valid baseline neurological assessment was felt to be critical for the establishment of a neurological “phenotype” to compare against the biomarkers. The clinical trial protocol for conducting this prospective observational study at this single institution was approved by our local institutional review board (IRB) (#H10-01091); a subsequent multi-center extension of this study is registered with
The non-SCI negative control group consisted of CSF samples collected from 1 male and 5 females who underwent surgical intervention not related to acute SCI. The average age of this group was 59.7 ± 8.3 years.
SCI, spinal cord injury; CSF, cerebrospinal fluid.
Neurological evaluation
The severity of neurological impairment was graded according to INSCSCI standards of neurological testing, with motor scores recorded separately in the upper and lower extremities. All baseline testing and the assigning of the baseline AIS grade (A, B, or C) was conducted by research study nurses to confirm the initial examination of the patients, which was often conducted by the spine surgery residents or fellows. The INSCSCI examination was conducted again at 6 months post-injury to determine whether AIS grade had improved (“AIS grade conversion”), and the extent of total motor score improvement.
CSF collection and processing
Once a patient was enrolled in the study, an intrathecal catheter (PERIFIX® Custom Epidural Anesthesia Kit, B. Braun Medical Inc. Bethlehem, PA) was inserted in the lumbar spine at L2/3 or L3/4 using a standard aseptic technique. The catheter was advanced 15–20 cm from the entry point on the skin surface and kept in place for 72–120 h. The catheters were inserted prior to surgery with the patient log-rolled to the right side, and the spinal column protected in a neutral position by a physician.
CSF samples of 3–4 mL were drawn at the time of catheter insertion, and then in the subsequent postoperative period approximately three times each day (discarding the first 1 mL of CSF aspirated from the line). Sample processing was performed immediately at the patient's bedside by the research study nursing team. The CSF sample was centrifuged at 1000 rcf for 10 min, and the supernatant was then dispersed into 200 μL aliquots and immediately frozen in an ethanol-dry ice bath and stored at −80°C.
A total of 2 × 200 μL aliquots of CSF from patients was applied to an antibody-based protein depletion column (Agilent Human 14 Multiple-Affinity Removal Spin Cartridge) and 14 abundant proteins were removed from the sample. Flow-throughs from this step were concentrated and digested in-solution with trypsin, as previously described. 19 After the digestion was complete, samples were cleaned on C18 Stage Tips as described. 20
Multiple reaction monitoring (MRM) assay development
In this study, we decided to screen CSF for a total of 165 unique protein targets selected, based on existing studies of CSF-based protein markers in other neurological diseases (Table S1) (see online supplementary material at
A control sample of CSF pooled from patients without an SCI (Table 2) was depleted and digested (as will be discussed), and a mixture of all synthetic peptides was spiked in. Using the transitions selected, the retention time of each of the peptides was located in the liquid chromatography (LC)-MRM run, allowing the construction of a “dynamic MRM” experiment.
In summary, of the 29 patients, there were 10 AIS A, 12 AIS B, and 7 AIS C at baseline. There were 24 males and 5 females, and the average age was 45.8 ± 3.0 years. A total of 22 were cervical level injuries.
SCI, spinal cord injury; AIS, American Spinal Injury Association Impairment Scale; UEMS, Upper Extremity Motor Score; LEMS, Lower Extremity Motor Score; MS, Motor Score.
The panel of previously described MRMs for CSF proteins was analyzed as described. 21 The newly developed MRMs were also applied to the patient CSF in a multiplexed assay performed on an Agilent 6460 Triple Quadrupole mass spectrometer with an Agilent (1200) nanoflow high performance liquid chromatography (HPLC), and a chip cube ion source. A large-capacity C18 nanospray chip (Agilent, G4240-62010) was used for all analyses, employing 90 min water:acetonitrile gradients. Peak areas were integrated and manually extracted from the vendor's MassHunter data analysis software.
Samples (including the positive and negative control samples) were assigned to the 96 well plate using a randomization scheme that balanced AIS grade and sampling time (24, 48, and 72 h) across the rows of the plate. In this way, we ensured these key factors were not confounded with mass spectrometry processing time and sequencing.
Statistical analysis
As in previous work, we focused our attention on the CSF sample drawn at the 24 h post-injury time point. 17,18 We selected 24 h because this represents a time point at which most acute SCI patients would likely be admitted to a trauma center, and a CSF sample could be obtained for biomarker analysis. The 48 h and 72 h samples were plotted against time and AIS grade, but were not otherwise analyzed here.
Quality control
Prior to the statistical analysis, we took a number of steps to deal with measurements below the lower limit of quantitation (LLOQ) of the assay and variation associated with CSF sample size. In an initial blinded quality control (QC) review of the data, we dropped from our analysis any protein with more than two out of three values below the LLOQ among the 24 h samples from our 29 analyzable patients. For proteins with greater than two out of three values below LLOQ, we assessed whether any association existed between the proportions of values below LLOQ and SCI Severity or Total Motor Score (TMS) by logistical regression, and found no such association (not shown).
The abundance of many proteins was measured by more than one peptide. We chose to conduct our analysis using a representative peptide for each protein: the peptide most frequently found to be the most abundant of the set across all the 24 h patient samples. Next, we adjusted our abundance estimates to account for restricted volume of CSF available for the MS analysis. Each abundance value was adjusted for the volume of CSF to a standard 400 μL sample CSF. Finally, any remaining values below LLOQ were imputed to one half of the smallest observed volume-corrected abundance, after taking log-base 2 transformations.
Univariate analysis
To identify proteins whose abundance monotonically increased or decreased with baseline AIS grade, for each protein, we fit a linear regression model, with an empirical Bayes shrinkage of the protein-specific within-group variance, using the “limma” R package. 23 We report both unadjusted p values and Benjamini–Hochberg false discovery rates (adjusted p-values).
To identify proteins whose abundance was linearly associated with 6 month change from baseline in TMS we again employed the “limma” R package. Baseline neurological injury level was included as a covariate in the model.
Multivariate analysis
Multi-protein panels for discrimination between AIS grades were identified using sparse partial least-squares discriminant analysis (SPLS-DA) via the “mixOmics” R package. 24 Similarly, we used SPLS regression analysis to identify proteins predictive of the 6 month change from baseline in TMS. Both analysis methods perform variable reduction (i.e., protein selection). We used leave-one-out cross-validation of the error rate for the SPLS-DA and the R2 for the SPLS regression analysis to identify the optimal number of components and optimal number of proteins per component in each analysis and estimate out-of-sample performance. All analyses were conducted using R (ver. 3.3.0).
Results
Twenty-nine acute SCI patients were included for the final data analyses including: 10 AIS A, 12 AIS B, and 7 AIS C (the demographics and clinical data are shown in Table 1). The primary mechanism of injury among both men and women was sports accidents (41%) followed by falls (31%). The mean age of the cohort was 45.8 ± 3.0 years, with an age range of 19–74 years, and females representing 19% of the cohort. For the “negative,” non-SCI control group, CSF samples obtained from six adult subjects undergoing routine lumbar decompressions and/or fusions were pooled and then analyzed (Table 2). These negative control subjects were between 39 and 79 years old and had no current or past history of spinal cord injury. For the “positive” controls, we pooled CSF samples obtained at 24 h post-injury from 6 AIS A patients. These were distinct from the 29 patients included in the study (Table 3).
The positive control group consisted of CSF samples collected from 3 male and 2 female AIS A patients. The average age of this group was 37.5 ± 11.7 years with 2 cervical and 3 thoracic-level injuries.
AIS, American Spinal Injury Association Impairment Scale; UEMS, Upper Extremity Motor Score; LEMS, Lower Extremity Motor Score; MS, Motor Score.
Protein identification and abundance changes across injury severities
Similarly to our previous reports on the establishment of CSF biomarkers, 17,18 we focused the assessment of injury severity on the CSF samples collected 24 h post-injury. The entire set of proteins that were identified in this proteomics analysis did not change between AIS grade; however, the abundance levels varied among the three injury severities (AIS A, B, or C). From a total of 165 proteins interrogated at 24 h post-injury, we identified 27 proteins that revealed statistically significant differential abundance among AIS A, B, and C patients (adjusted p < 0.05; see Table 4). Proteomics data for the 27 differentially abundant proteins are shown in Table 4. The abundance profiles of the nine most significant proteins associated with injury grade at 24 h post-SCI are displayed in Figure 1, with triosephosphate isomerase (TPI) as the most statistically significant protein marker by nearly an order of magnitude (adjusted p < 0.0001). Further, apolipoprotein M (APOM), γ-enolase, IL-1 receptor-like 1, actin 3 α cardiac muscle 1, phosphatidylinositol-glycan-specific phospholipase D, peroxiredoxin 2, cystatin-B, and prostaglandin-H2 D isomerase were identified among the top nine proteins that differed among AIS grades. Figure 1 also illustrates that over the period of 3 days post-SCI, during which the secondary injury progresses, the levels of these proteins generally declined in the CSF of all three injury severities to levels comparable to those in the pooled negative control sample.
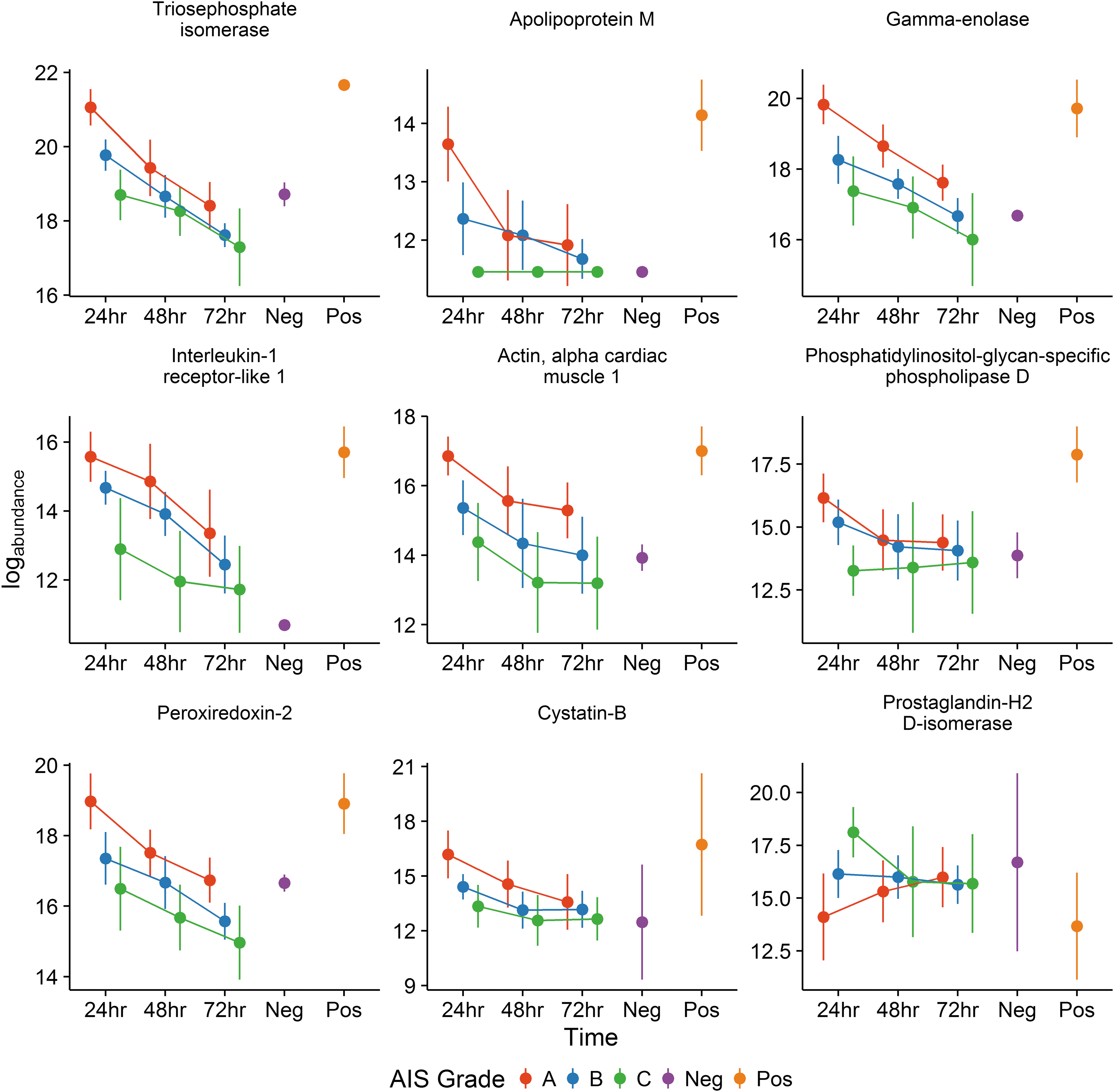
Time course of protein abundance in cerebrospinal fluid (CSF) for the top nine proteins associated with American Spinal Injury Association Impairment Scale (AIS) grade at 24 h after injury. Mean protein log concentration (± 2 standard deviations) for patients with injury severity AIS grade A (red, n = n1), B (blue, n = n2), or C (green, n = n3), are shown at 24, 48, and 72 h post-injury. Also shown the mean protein log concentration (± standard deviations) for negative (purple) and positive (orange) controls. Note that the data points for AIS A, B, and C at each time point (24, 48, 72 h) are offset slightly in the x-axis plane to increase clarity by avoiding overlap on the figure.
Included in the table are the protein and peptide IDs, log2 fold change (logFC), and p values for the comparison of AIS C versus AIS B versus AIS A (unadjusted and adjusted using the Benjamini–Hochberg procedure). A positive logFC value indicates highest to lowest concentration in the comparison AIS C-B-A, whereas a negative logFC indicates highest to lowest concentration in the comparision AIS A-B-C. There were 27 proteins that were significantly associated (adj. p value <0.05) with baseline AIS grade.
CSF, cerebrospinal fluid; AIS, American Spinal Injury Association Impairment Scale.
Most of the proteins (24/27) that were found to be significantly associated with AIS grade at the 24 h time point were elevated in the more severely injured patients (AIS A compared with AIS B and C). A heat map of protein abundance ratios is shown in Figure 2. Compared with the AIS C group, a total of 10 proteins were consistently upregulated or downregulated in all tested AIS A samples Figure 3. In the AIS A group, TPI, APOM, γ-enolase, IL-1 receptor-like 1, actin 3 α cardiac muscle 1, phosphatidylinositol-glycan-specific phospholipase D, peroxiredoxin 2, and cystatin-B were the most significantly upregulated proteins (each adjusted p < 0.01), whereas prostaglandin-H2 D isomerase and neural cell adhesion molecule 1 (NCAM1) were significantly downregulated in AIS A as compared with AIS C patients (each adjusted p < 0.01).
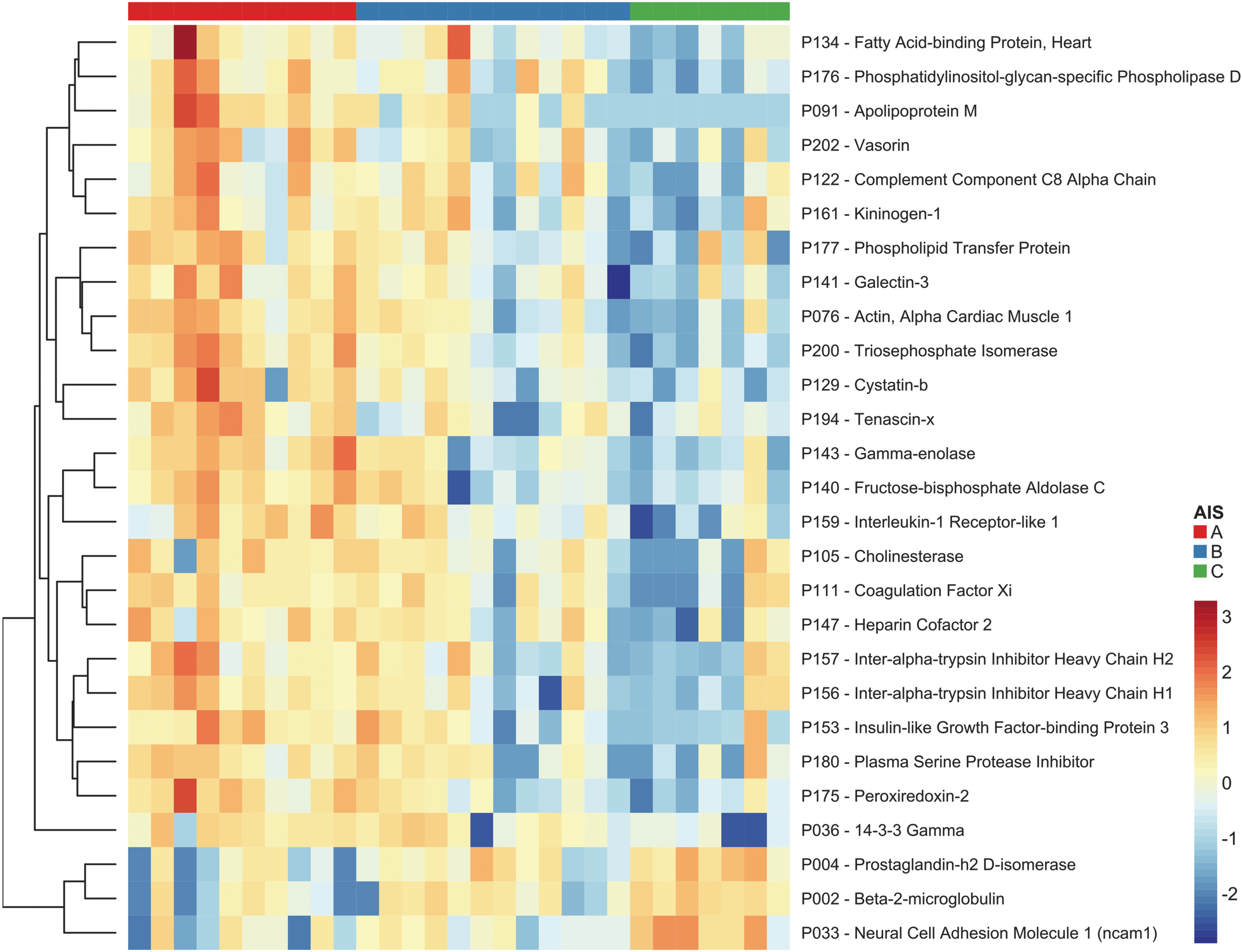
Proteins found to be associated with baseline American Spinal Injury Association Impairment Scale (AIS) grade. Each cell of the heat map represents the abundance of one protein (rows) in one sample (columns). The colored band at the top indicates baseline AIS grade (red = AIS A, blue = AIS B, green = AIS C). Most of the proteins that were found to be significantly associated with AIS grade at this time point were elevated in the more severely injured patients (AIS A). Only three proteins were significantly elevated in less severe injury (AIS C): prostaglandin-H2 D-isomerase, β-2-microglobulin, and neural cell adhesion molecule 1 (bottom).
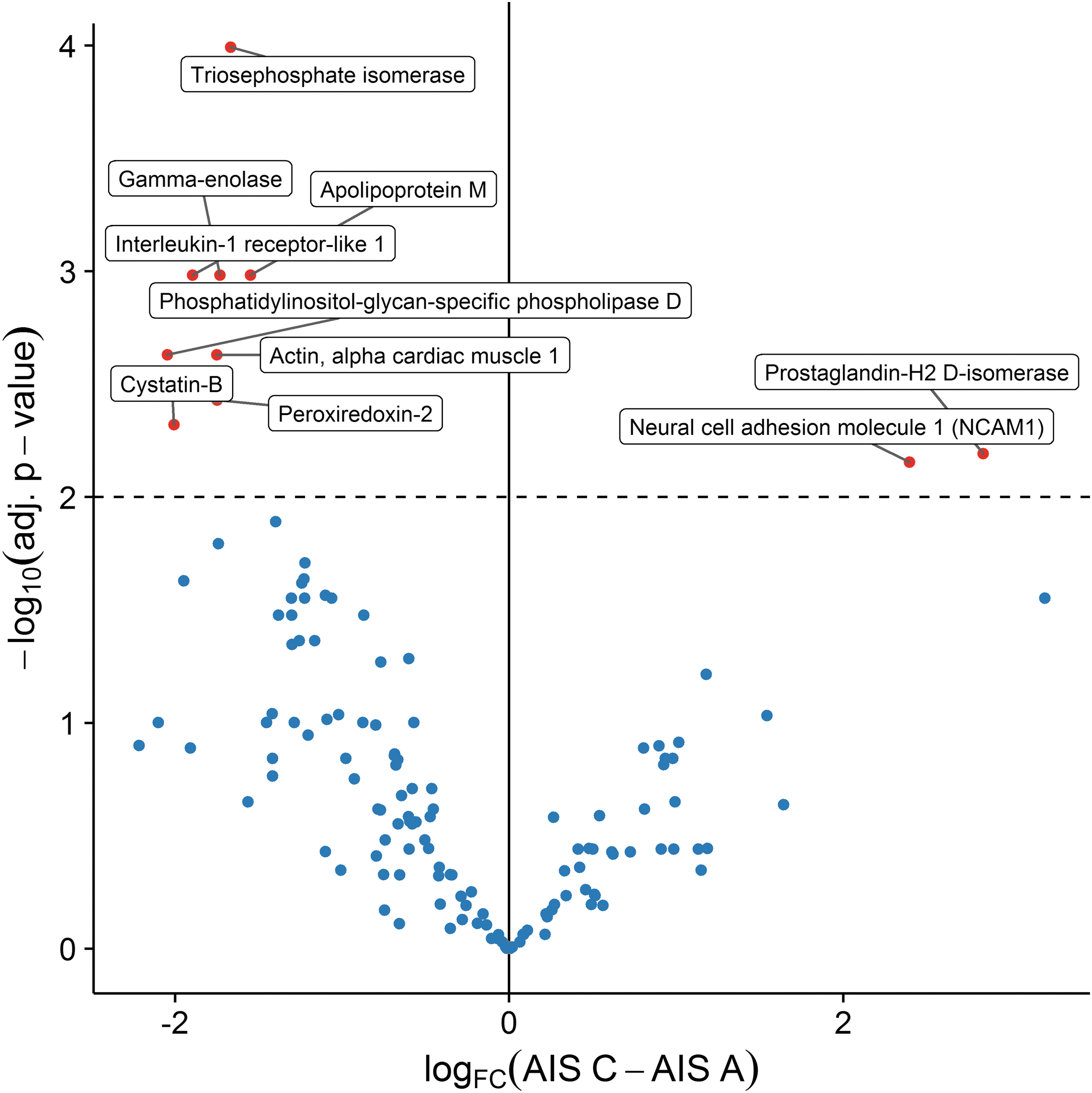
Visualization of log2 of fold-changes (logFC) versus log10 of the adjusted p values for the comparison of baseline American Spinal Injury Association Impairment Scale (AIS) Grade A versus Grade C for all proteins. Proteins above the dashed line have adjusted p values <0.01. Proteins to the left of the 0 logFC have higher abundance in AIS Grade A than in AIS Grade C; those to the right have higher abundance in Grade C than in Grade A.
Classifying baseline AIS grade using 24 h post-injury CSF protein markers
The close relationship of the CSF compartment to the injured spinal cord provides an opportunity to monitor, at the molecular level, physiological responses to mechanical spinal cord trauma. Because the baseline severity of neurological impairment (as judged by AIS grade) is currently the strongest predictor of neurological outcome, the primary goal of this analysis was to evaluate whether proteins identified in our proteomic analyses could differentiate among AIS A, B, and C severities of injury.
Based on the differential protein concentrations among AIS groups, a partial least squares discriminative analysis (PLS-DA) was performed to determine whether the protein abundance data at 24 h post-injury could distinguish the baseline AIS grade groups. As presented in Figure 4, each of the three AIS groups differs significantly from the others along the first component identified by the PLS-DA (p < 0.01, using Tukey's Honest Significant Difference test to control for multiple inference). For the cohort of 29 patients analyzed in this study, a PLS-DA model including 10 proteins across two components resulted in the best observed classification accuracy in leave-one-out cross-validation of 76% overall. Specifically, this model had cross-validated classification accuracy of 80% for AIS As, 58% for AIS Bs, and 100% for AIS Cs. When fit on all available samples, this model included: actin α cardiac muscle 1, APOM, γ-enolase, peroxiredoxin-2, TPI (first PLS-DA component), and angiotensinogen, complement factor I, CD44 antigen, gelsolin, mannan-binding lectin serine protease 2 (second PLS-DA component).
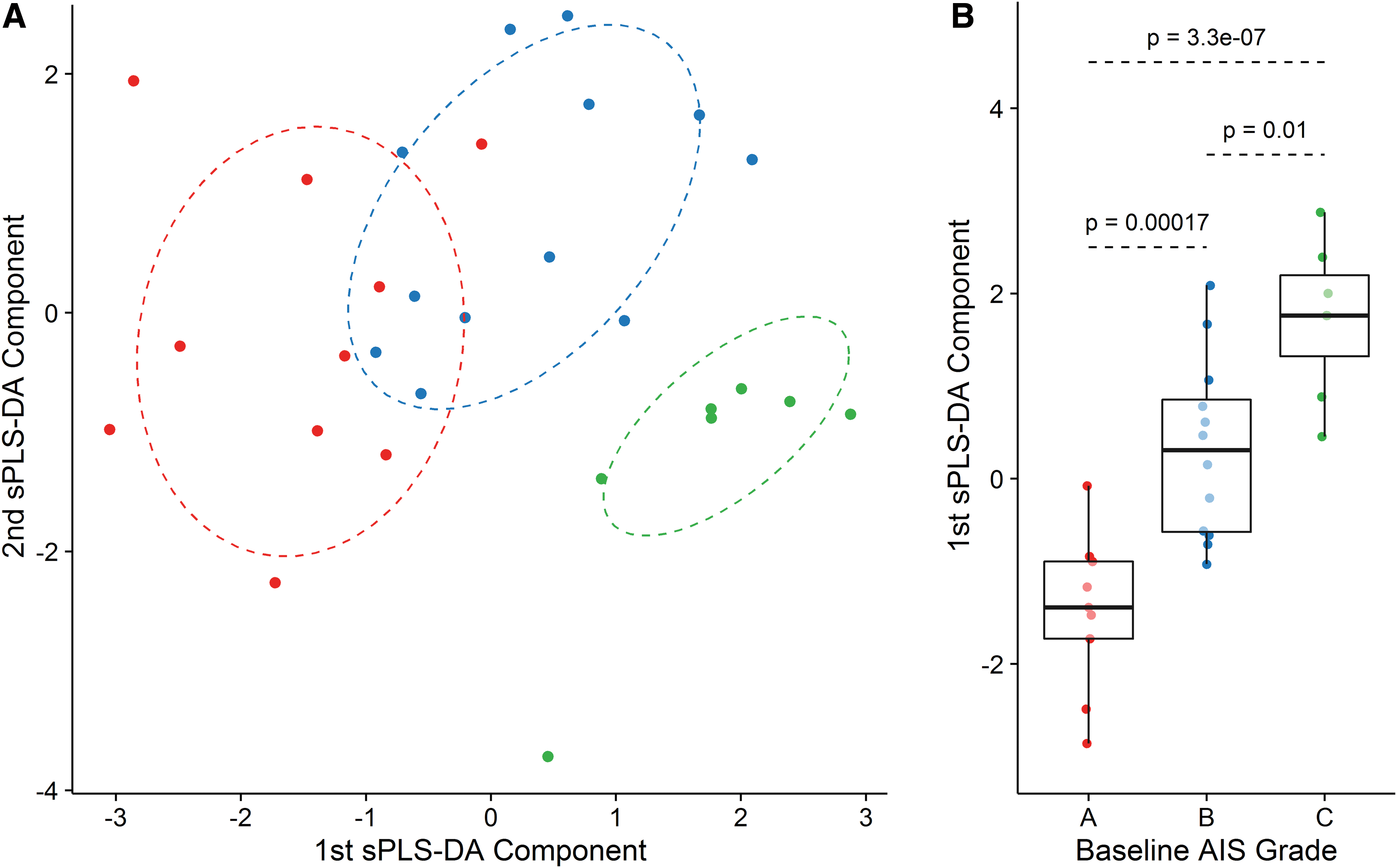
Using cerebrospinal fluid (CSF) biomarkers to discriminate between baseline American Spinal Injury Association Impairment Scale (AIS) grades. The first and second components from the sparse partial least-squares discriminant analysis (SPLS-DA) model are plotted for all 24 h sample data in 27 patients
Predicting AIS grade conversion and TMS improvement 6 months post-injury using CSF protein marker abundance at 24 h post-injury
Next, we determined whether AIS grade improvement at 6 months post-injury could be predicted using CSF protein abundances at 24 h post-injury. Two of the initial patients (1 AIS A, 1 AIS B) were lost to follow-up, and, therefore, this question was addressed with the data from 27 patients. Ultimately, an improvement of at least one AIS grade by 6 months post-injury was demonstrated in 14 patients out of the 27 (1 AIS A, 7 AIS B, 6 AIS C; see Table 1). No deterioration in AIS grade was observed at 6 months. Our analysis revealed that although the abundance of 33 proteins at 24 h post-injury was associated with AIS grade conversion (p < 0.05) (Table S4) (see online supplementary material at
We then evaluated whether TMS improvement at 6 months post-injury could be predicted using CSF protein abundances at 24 h post-injury. As expected, a higher abundance of a specific protein generally reflected a more severe injury and a lesser chance of TMS improvement. After adjusting for baseline level of neurological injury (e.g., C6 versus T6), we found that 46 proteins were significantly related to the 6 month TMS improvement (adjusted p < 0.05; see Table 5). Again, TPI had the strongest individual association to TMS recovery; however, strong associations (adjusted p < 0.01) were also found for other markers including γ-enolase, galectin, and coagulation factor XII (FXII) (Fig. 5). As might be anticipated, 22 of these proteins were among the 27 proteins that were significantly associated with baseline AIS grade (Table 5 highlighted in bold). The consistent relationship between AIS grade (baseline injury severity) and TMS improvement over 6 months (neurological recovery) for these protein candidates certainly highlights their potential utility as biomarkers for acute SCI.

Proteins found to be associated with total motor score (TMS) improvement over 6 months after adjusting for baseline neurological level (adjusted p < 0.01) Each cell of the heat map represents the abundance of one protein (rows) in one sample (columns). The colored bands at the top of the heat map indicate (from top to bottom): baseline neurological level (C3 through T11) and change in total motor score over 6 months (0 through 80).
Included in the table are the protein and peptide IDs, log2 fold change (logFC), and p values (unadjusted and adjusted using the Benjamini–Hochberg procedure). A positive logFC value indicates that the highest protein concentration was observed in subjects with the highest recovery, whereas a negative logFC indicates that the highest protein concentration was observed in subjects with the lowest recovery, on average. There were 46 proteins that were significantly associated (adj. p value <0.05) with TMS recovery over 6 months; A total of 22 of these were in the list of 27 proteins that were significantly associated with baseline AIS Grade (bold).
CSF, cerebrospinal fluid; TMS, total motor score; AIS, AIS, American Spinal Injury Association Impairment Scale.
We also considered whether there might be protein markers that can predict TMS recovery even after controlling for baseline AIS grade, baseline neurological level, and baseline TMS. In this analysis, we found 47 individual proteins whose higher abundance levels were each significantly associated with lower improvement in TMS over 6 months (i.e., each p < 0.05). However, after adjusting for multiple testing, only FXII (P112) remained statistically significant (adjusted p = 0.0079). In other words, when comparing two patients with the same baseline AIS grade, baseline neurological level, and baseline TMS, higher levels of FXII predict less improvement in TMS over the first 6 months post-injury. Other nominally significant proteins (i.e., each p < 0.05) included 14-3-3 beta/alpha, complement factor 1, galactine-3, protein α-1-microglobulin/bikunin precursor (AMBP), vitamin D-binding protein, plasminogen, leucine-rich α-2-glycoprotein, plasma protease C1 inhibitor, 72 kDa type IV collagenase, α-2-antiplasmin, and vitamin-K-dependent protein 3 (Table S5) (see online supplementary material at
In our final analysis, a PLS regression model established using CSF protein marker abundance at 24 h post-injury was very good at predicting TMS recovery in patients with “incomplete” injuries, AIS B and C (correlations of r = 0.94 and r = 0.87, respectively), but was less so for complete AIS A injuries (r = 0.01) (Fig. 6). In this model, the first component consisted of actin α cardiac muscle 1, FXII, galectin-3, γ-enolase, and TPI; the second component included 14-3-3 beta/alpha, 14-3-3 gamma, collagenase 3, complement factor D, and vitamin K-dependent protein C. The performance at predicting TMS recovery in new samples was estimated with the leave-one-out cross-validation approach. The best overall out-of-sample R2 = 0.52, corresponding to a mean squared prediction error of 0.50, was obtained with a model retaining five proteins across three components, for a total of 14 unique features.
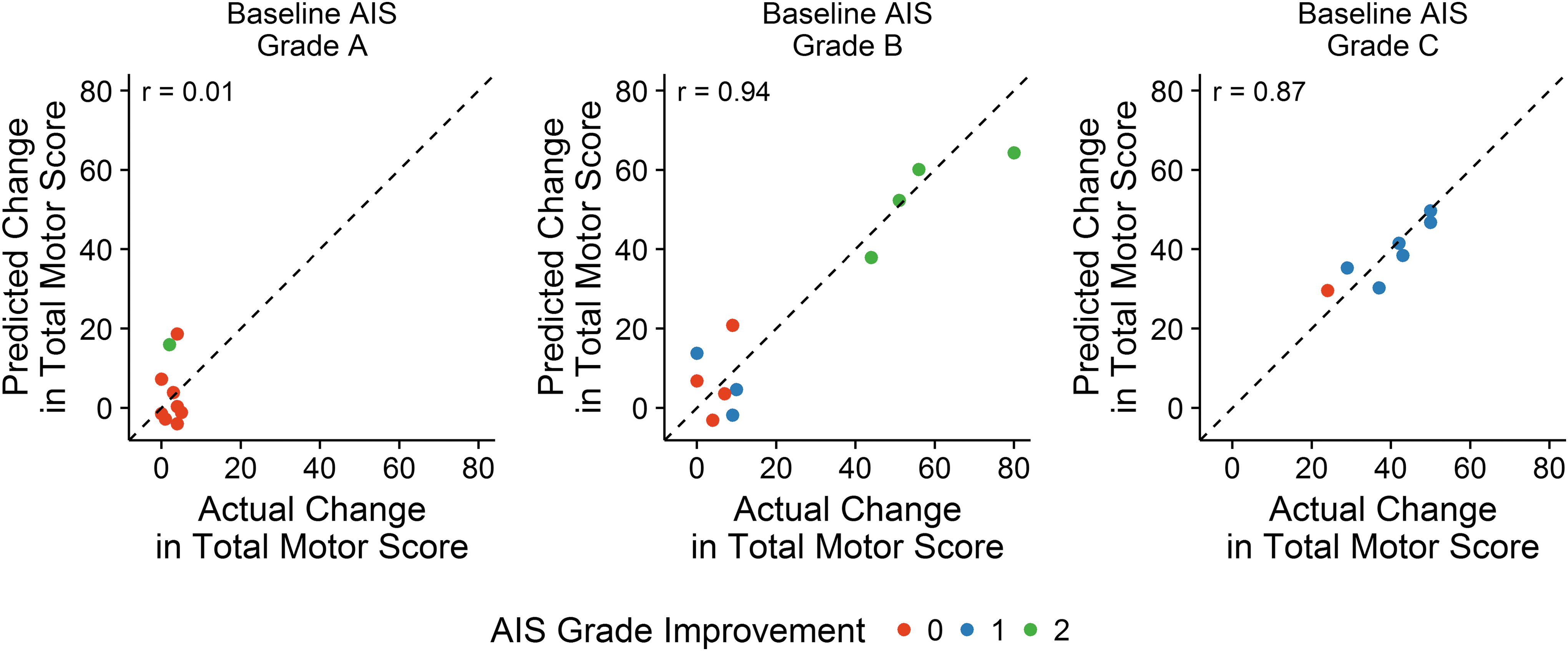
Correlation between improvement in American Spinal Injury Association Impairment Scale (AIS) grade and change in total motor score (TMS) score. The partial least squares (PLS) regression analysis model can predict 6 month changes in TMS, particularly for patients who have a baseline AIS grade of B or C. As expected, patients who improve in TMS also tend to improve in AIS grade by one or two grades.
Discussion
In the initial management of acute traumatic SCI, the baseline classification of neurological impairment as AIS A, B, C, or D is a fundamental component of the early assessment. Clinicians instinctively prognosticate the neurological outcome of the acute SCI patient after this initial assignment of neurological impairment. This prognostication is obviously important in the early communication with patients and their families, and can influence management decisions such as the urgency of surgical decompression. 25 Aside from the clinical utility of this neurological assessment, the conduct of clinical trials in acute SCI is highly dependent upon the ability to evaluate and then appropriately stratify potential subjects based on the severity of their neurological impairment. Currently, the development of novel therapies for acute SCI is severely hindered by the inability to clinically evaluate acute SCI patients in the acute injury period in a reliable fashion, the difficulty in accurately predicting neurological outcome based on this early evaluation, and the lack of objective molecular measures of outcome for monitoring treatment efficacy. In addition to these very practical issues, the paucity of molecular-level observation and description of human pathophysiology after acute SCI is a broad limitation for translational research in a field that relies heavily on experimental rodent models. 26
In this study, we utilized a targeted mass spectrometry-based proteomics approach to identify CSF proteins that could potentially serve as biomarkers of injury severity in patients with baseline AIS A, B, or C grades of neurological impairment. Additionally, we explored whether the specific proteins were associated with neurological recovery as judged by improvement (“conversion”) of the patient's AIS grade or improvement in the patient's motor score over 6 months. We compared abundances of 206 proteins in CSF from 29 acute SCI patients. We identified 27 specific proteins that were significantly different among AIS A, B, and C patients at 24 h post-injury. We found that TPI, APOM, γ-enolase, interleukin-1 receptor-like 1, actin 3 α cardiac muscle 1, phosphatidylinositol-glycan-specific phospholipase D, peroxiredoxin 2, cystatin-B, and prostaglandin-H2 D isomerase were particularly strong biomarkers of injury severity. Far fewer proteins were strongly associated with improvement in motor score, with only one protein (FXII) out of 47 proteins identified initially being statistically significant after adjusting for multiple comparisons. In our cohort of 29 patients, >50% experienced some improvement in AIS grade over the 6 months. Although a number of proteins had some association with this change, the analysis did not reveal any specific protein whose association with this neurological change was statistically significant after adjusting for multiple comparisons.
Glycolytic pathway
In this study, three of the 27 identified potential biomarkers of injury severity were glycolytic enzymes, with the most significant (by nearly an order of magnitude) being TPI. Several pre-clinical proteomic studies have also reported the presence or upregulation of TPI in the injured spinal cord. 2,27 –30 Similar to our clinical data, Moghieb and colleagues 29 showed that TPI was readily detectable and elevated in CSF samples from moderate-severe SCI patients (AIS A n = 9 and AIS B n = 6) recruited at the University of Miami Hospital. 29 In this important study, serial human CSF samples were collected from the 1st day of injury up to 6 days from injury every 6 h, and compared with commercially available human CSF sample of uninjured controls (Bioreclamation Inc.). The authors also indicated that the temporal profile of the proposed biomarkers of SCI, including TPI, appeared to vary depending on the differences in severity (AIS scale), lesion level (e.g., cervical vs. lumbar), patient improvement over time, and/or presence of secondary insults at later time points. Because of the limited patient sample size, the authors stated that they did not have sufficient statistical power to examine these potential correlations systematically. 29 Nonetheless, our data regarding TPI and its relationship to injury severity are very much in support of the findings of this article.
The glycolytic enzymes γ-enolase (ENO2, also known as NSE) and fructose-bisphosphate aldolase C (ALDOC) were similarly altered in a SCI severity-dependent fashion. Levels of TPI, 27 –32 ENO2, 29,30 and ALDOC 33,34 are increased in the spinal cord, CSF, and serum after experimental SCI; however, only ENO levels correlate with injury severity or functional outcome, albeit with conflicting results in different studies. 35 –37 We observed that levels of these three enzymes at 24 h post-SCI were considerably elevated in AIS A patients compared with those with less severe injury (AIS B or C). Notably, the SCI severity-dependent pattern of ENO2 abundance we observed here is consistent with the findings of a previous report by Pouw and colleagues, 35 which used enzyme-linked immunosorbent assay (ELISA) methodology to measure ENO2 levels in CSF samples from motor complete (AIS A and B) and motor incomplete SCI patients (AIS C and D). Similar results were obtained by Cao and colleagues 36 using a contusive-induced rat model of SCI. However, one pre-clinical study failed to observe such injury-severity-dependent pattern of ENO2 abundance. 37
Several proteomic studies using animal models of SCI have found elevated levels of glycolytic pathway enzymes after injury, including phosphoglycerate mutase, 34,38 glyceraldehyde-3-phosphate dehydrogenase, 29,30 and pyruvate kinase. 34,38 It has been suggested that ischemia resulting from SCI results in lactate accumulation, and, consequently, the upregulation of glycolytic enzymes, to provide energy necessary for cellular homeostasis. 28 Moreover, mitochondrial dysfunction is known to contribute to the pathophysiology of secondary injury, in particular in neuronal damage secondary to free radical degeneration. 39 In our study TPI, ENO2, and ALDOC protein levels were increased in the AIS A group compared with those with less severe injury (AIS B or C). This is consistent with augmented glycolytic enzyme dependency in more severe injury, and is in good agreement with the model in which a more severe injury places higher energy demands on neuronal tissue, compounded by greater mitochondrial respiration deficits, as demonstrated by others. 40,41
Transport and metabolism of lipids and lipoproteins
We observed increased abundance of several proteins involved in the transport and metabolism of lipids and lipoproteins, including lipid phospholipid transfer protein (PLTP), APOM, fatty acid binding protein heart (FABP3), and prostaglandin-H2 D-isomerase (PTGDS) in AIS A CSF compared with others. Although one study has suggested APOH as a biomarker of injury severity in human SCI, 42 the biological role of APOM in SCI remains to be determined. It is of interest that the increased levels of APOM may be related to its lipocalin-like properties. 43 The identification of C8α, a covalent partner of the complement lipocalin C8γ, is noteworthy in this respect.
Immune and coagulation system
Several immune and complement response proteins including β-2-microglobulin (B2M) IL receptor-like 1 (IL1RL1), and complement protein C8α (C8α) were also identified among the potential biomarkers of injury severity in our study. Although the observation that the increased levels of B2M are associated with less severe injury seems somewhat counterintuitive, it can be contextualized by the fact that B2M is a negative regulator of the immune response. 44 Apart from the immune and complement proteins, we also observed altered CSF abundances of several proteins involved in the coagulation system. Kininogen-1 (KNG1) (high molecular weight kininogen [HMWK]) and coagulation factor XI (FXI), a serine protease, were both elevated in the CSF of AIS A patients compared with those who had sustained an AIS B and C injury. Consistent with our data, elevated KNG1 and kininogen precursor have also been found in rat CSF and parenchyma following injury. 30,45 Both KNG1 and FXI have a key role in the intrinsic coagulation pathway leading to fibrin formation. The traditional view of the coagulation cascade is linked to thrombotic diseases; however, there is increasing evidence that the coagulation cascade is an important player in inflammation and various inflammatory disorders of the nervous system, such as multiple sclerosis, 46,47 and Alzheimer's and Parkinson's diseases. 48
In addition to being a part of the intrinsic coagulation pathway, KNG1 is a precursor for the pro-inflammatory bioactive peptide and vasodilator bradykinin, which is proteolytically released from KNG1 by kallikrein. The kallikrein-kininogen system has been implicated in various brain diseases such as stroke, 49 multiple sclerosis, 50 and Alzheimer's disease. 51 Lastly, this system has also been explored as a therapeutic target in TBI, 52 –54 as bradykinin increases vascular permeability and promotes inflammation and edema formation, 55 which are likely important secondary mechanisms of injury following SCI as well.
Other biomarkers
In addition to glycolytic enzymes, we also identified several other proteins to be differentially expressed between baseline AIS grades at 24 h post-injury, although most did not survive the correction for multiple hypothesis testing. Other groups have also found several of the proteins identified in our study as being differentially regulated. Galectin-3, recently shown to act in most cases as a “pro-inflammatory cytokine,” 56 was identified as being more significantly upregulated among AIS A patients, and was found to be a marker of SCI in several proteomics studies of rat spinal cord injured tissue. 30 –32,34 Peroxiredoxin-2, an antioxidant enzyme, 57 was found in the spinal cord 29,58 and CSF 45 of rodents subjected to an experimental SCI. In our study, this protein was considerably higher in the CSF of AIS A patients than in those who had had a less severe injury (AIS B and C). Increased CSF concentrations of the 14-3-3 protein, involved in many processes including signal transduction, cell cycle regulation, and apoptosis, 59 have been described in patients with Creutzfeld–Jacob disease, 60,61 dementia, 62 acute brain injury, 63 and motor neuron injury. 64 Additionally, 14-3-3 was found in rat CSF and spinal cord following SCI. 30,34,45 Further, we found two inter-α-trypsin inhibitor heavy chains (inter-α -trypsin inhibitor heavy chain [ITIH]1 and ITIH2) in our list of candidate biomarkers of injury severity. The ITIs are a family of structurally related plasma serine protease inhibitors that are involved in extracellular matrix stabilization and the inflammatory response. 65 It is of interest that ITIH4 has previously been identified as a potential biomarker for the severity of SCI. 45
At the same time we also identified proteins that have not yet been evaluated as possible biomarkers in SCI, including vasorin, tenascin-X, neural cell adhesion molecule, heparin cofactor 2, IL-1-receptor-like 1, biotinidase, cholinesterase, PLTP, and insulin-like growth factor-binding protein 1. The significance of these findings requires further study.
Biomarkers to predict neurological outcome
As was pointed out in the introduction, being able to stratify an acute SCI patient's injury severity with objectively measured biomarkers as described would certainly facilitate the conducting of clinical trials. However, arguably the greatest utility of biomarkers in acute clinical trials would be in the improved prediction of neurological recovery. The early assignment of neurological impairment as AIS A, B, or C unfortunately leaves much uncertainty about the final neurological outcome, because of variability in spontaneous neurological outcome and limitations of the initial clinical aseessment. 13 In this regard, biomarkers may play an important role in facilitating clinical trials. From our list of 206 interrogated proteins, we found that only one protein, FXII, associated with change in total motor score at 6 months post-injury. Whereas this protein is part of the same intrinsic pathway as KNG1 and FXI, identified here as potential markers of injury severity, FXII had no predictive value for baseline classification. This implies that although the proteomics approach we employed can identify protein candidates that are associated with baseline injury severity, it is a more challenging task to establish those that are truly predictive of spontaneous neurological recovery.
FXII is at the interface between inflammation and coagulation (two systems central to host survival in the face of tissue damage), and has previously been identified as a major driving force during ischemic neurodegeneration. 50,66 Previous studies have demonstrated that genetic deficiency of FXII or its pharmacological inhibition is therapeutic in animal models of ischemic stroke, 67 –69 multiple sclerosis, 50 focal brain trauma, 52 and TBI, 70 –72 as well as traumatic SCI. 73 Mechanistically, it has been suggested that FXII inhibition not only attenuates invasion of inflammatory immune cells but also stabilizes the blood–brain barrier and decreased secondary edema. 52,67 Such benefits of reduced FXII activity may underlie the inverse correlation of this protein to motor function recovery post-SCI, as was observed in this study.
Limitations
There are a number of limitations that warrant consideration. First, although our cohort of 29 acute SCI patients divided among AIS A, B, and C injury severities represents, to our knowledge, the largest series to undergo this type of proteomic analysis of CSF, it remains a relatively small cohort, and further testing of a larger cohort is warranted. Our “negative control” non-SCI group consisted of mainly female patients who were older than our predominantly male SCI patients. With the small size of the entire cohort, it is unknown whether there were gender or age-related differences in the proteomic responses to injury. We also acknowledge that the relationship between very early protein changes and functional outcome at 6 months post-injury may be clouded by variability in terms of the type, duration, and intensity of rehabilitation programs. However, in the search for useful biomarkers, we are definitely seeking biochemical changes that are so pronounced in the early stages of injury so as to overcome the effect size of this inevitable variability in post-injury rehabilitation. Along the same lines, our analysis focused on the relationship between acute proteomic changes and neurological impairment, and we did not investigate other meaningful health-related quality of life measures (e.g., spinal cord independence measure).
Conclusion
This targeted mass spectrometry study was undertaken as a logical extension of our previous work in which we employed Luminex and ELISA methodologies to identify a series of inflammatory and structural biomarkers within the CSF of acute SCI patients. 17,18 We recently reported that the level of IL-6, IL-8, MCP-1, tau, S100β, and GFAP in CSF samples collected from 50 acute SCI patients (29 AIS A, 9 AIS B, 12 AIS C; 32 cervical, 18 thoracic) exhibited a positive prognostic value of 83% to predict AIS conversion, and strongly correlated with the extent of upper extremity motor score recovery 6 months after SCI. 17,18,74 In the current study of 29 patients, we quantified the proteomic changes that occur in human CSF after acute SCI, and identified 27 statistically significant protein candidates (p < 0.05 after adjusting for multiple comparisons) that are encouraging for further study and validation, to determine their utility as potential biomarkers. These studies are ongoing.
Although the MRM mass spectrometry approach is technically as quantitative and precise as ELISA-based approaches, their sensitivities for specific targets such as low abundance cytokines do differ. It is, therefore, not surprising that our mass spectrometry analysis in this relatively small cohort of 29 acute SCI patients did not result in the same predictors of neurological recovery as our ELISA-based work, which focused on three inflammatory cytokines and three structural proteins in 50 acute SCI patients. 17 However, by casting a broader net with this more expansive proteomic interrogation of these valuable CSF samples, it is possible to better characterize the biological responses to human SCI, and identify interesting biomarker candidates that can be used for injury stratification, outcome prognostication, and surrogate outcome measures.
Further work in this area will focus on validating these findings in acute SCI patients who have been subsequently enrolled in our clinical initiative, and exploring reasons for discrepancies between our findings and others. For example, in this study, we identified both neurofilament heavy and light chains (NFH and NFL, respectively) in the CSF of our patients, although neither was significantly associated with injury severity or motor score improvement. This is contrary to the findings of Pouw and colleagues 75 who reported on the relationship between NFH and injury severity in the CSF of acute SCI patients, and of Kuhle and colleagues 76 who more recently reported that NFL in the serum of acute SCI patients showed a close correlation with the neurological outcome. The cause of this discrepancy is unknown, although we will be evaluating NFL in the serum of our patients as well, to more directly confirm the findings of Kuhle and colleagues.
Ultimately, our goal is to establish a panel of biomarkers that can be utilized as a tool for early injury severity stratification in clinical trials (to enhance patient recruitment) and for better prognostication of neurological outcome (to reduce the variability in spontaneous recovery and thus lower the numbers of patients required for clinical trials to be completed). Future studies that are currently ongoing will follow up on our findings and explore additional proteins in both CSF and blood samples collected from acute SCI patients. By characterizing the acute pathophysiological responses to traumatic SCI in humans, and establishing biomarkers for better injury stratification and improved prognostication of neurological recovery, we hope to provide the field with tools that can facilitate our collective efforts to improve the lives of those with SCI.
Footnotes
Acknowledgments
The authors gratefully acknowledge the assistance of Allan Aludino and Leilani Reichl of the Vancouver Spine Research Program for support of the clinical trial, Daniel Rogers of the Rick Hansen Institute for managing the Canadian Multicentre CSF Monitoring and Biomarker (CAMPER) study, and Sara Assadian for managing the Brain Canada Multi-Investigator Research Initiative (MIRI). The clinical trial and proteomics analysis were generously supported by the Rick Hansen Institute, Paralyzed Veterans of America, Craig Neilsen Foundation, Brain Canada, and the VGH & UBC Hospital Foundation. The mass spectrometry infrastructure used here was supported by the Canada Foundation for Innovation, the BC Knowledge Development Fund and the BC Proteomics Network. M.F.D. is the Paetzold Chair in Spinal Cord Injury, and B.K.K. is the Canada Research Chair in Spinal Cord Injury and the VGH & UBC Hospital Foundation Dvorak Chair of Spinal Trauma.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.