
Abstract
Many patients do not return to work (RTW) after mild traumatic brain injury (mTBI) because of persistent complaints that are often resistant to therapy in the chronic phase. Recent studies suggest that psychological interventions should be implemented early post-injury to prevent patients from developing chronic complaints. This study is a randomized, controlled trial that examines the effectiveness of a newly developed cognitive behavioral therapy (CBT) intervention (CBTi) compared to telephonic counseling (TC) in at-risk mTBI patients (patients with high reports of early complaints). Patients underwent either five sessions of CBT treatment or five phone conversations starting 4–6 weeks post-trauma. The main outcome measure was RTW 6 and 12 months post-trauma. Secondary measures comprised functional outcome at 6 and 12 months, and depression, anxiety, and reported post-traumatic complaints at 3, 6, and 12 months post-injury. After excluding dropouts, CBTi consisted of 39 patients and TC of 45 patients. No significant differences were found with regard to RTW, with 65% of CBTi patients and 67% of TC patients reporting a RTW at previous level. However, TC patients reported fewer complaints at 3 (8 vs. 6; p = 0.010) and 12 months post-injury (9 vs. 5; p = 0.006), and more patients in the TC group showed a full recovery 12 months post-injury compared to the CBTi group (62% vs. 39%). The results of this study suggest that early follow-up of at-risk patients can have a positive influence on patients' well-being, and that a low-intensive, low-cost telephonic intervention might be more effective than a CBT intervention at improving outcome in at-risk patients.
Introduction
M
Although subject of much debate, there is growing evidence suggesting that early post-traumatic complaints that are caused by the direct effects of the brain injury may convert into chronic complaints because of psychological mechanisms, such as appraisal and coping style. 6,7 For example, it has been found that persistent post-traumatic complaints are unrelated to performance on neuropsychological tests, and severity of injury measures have been found to be poor predictors of outcome. 5 Apparently, some patients are better able to adapt and thus to cope with the injury and its initial consequences than others. 8,9 Coping refers to psychological adaptation to stressors and serious life events, such as sustaining mTBI. It is generally acknowledged that an active coping style with positive thinking will more frequently lead to a positive adaptation whereas a passive coping style with denial or avoidance of problems and focusing on negative feelings is considered to be maladaptive. 10 Coping strategy is closely related to appraisal, or patients' perceptions of their condition. Perceiving an event like mTBI as catastrophic is unrealistic and may lead to feelings of threat and loss of controllability. 11 An unrealistic illness perception combined with a maladaptive coping style may cause depression and anxiety, which, in turn, increases selective attention to symptoms. This can result in experiencing even more complaints, creating a vicious cycle. 7,12,13
Psychological treatments of mTBI patients have mostly focused on treating persistent complaints with cognitive behavioral therapy (CBT) in the chronic phase. Although some studies reported improvements regarding depression, anxiety, and stress-related complaints, improvements in daily life functioning have not been achieved. 14 –16 This is not surprising, given that post-traumatic complaints in the chronic phase are traditionally seen as resistant to therapy and very difficult to treat. 14 Recently, several studies suggested that psychological interventions might be effective in preventing the development of persistent post-traumatic complaints, rather than treating them in the chronic phase. 15 However, routine preventative CBT treatment of all mTBI patients offered no benefit, suggesting that for these interventions, only patients at risk of persistent complaints should be targeted. 17 In a study that investigated an early CBT intervention in at-risk mTBI patients, Silverberg and colleagues demonstrated a reduction of post-traumatic complaints and depression in mTBI patients at 3 months post-injury. 18 However, this and other studies are hampered by small numbers and short durations of follow-up, and well executed randomized, controlled trials (RCTs) are lacking.
Another psychological intervention that has been used to prevent long-term post-traumatic complaints is the provision of educational information only, early post-injury. 19 –21 Patients who received elaborate information regarding post-traumatic complaints early post-injury report overall fewer symptoms 3 months post-injury. 20 Moreover, in another RCT, it was found that patients that received telephone counseling (TC) had fewer chronic complaints when compared to care as usual. 22 However, receiving TC did not have an effect on general health outcome, which included health, emotional status, and productive activity. The latter might be an indication that providing information and coaching solely by telephone is not sufficient, and that a prevention combining education with CBT in the acute phase might be more valuable.
Therefore, we conducted an RCT that compared two preventative interventions administered early post-injury: a CBT-based intervention (CBTi) and TC. The interventions were offered to patients at risk of suffering from persistent post-traumatic complaints, and patients were followed-up for 1 year. The primary aim of this study was to examine the additional effectiveness of a newly developed CBTi early post-injury on RTW in comparison to TC, which was already found to be effective in lowering post-traumatic complaints. Secondary aims were to improve functional outcome and lowering the number of post-traumatic complaints. Moreover, because CBT aims to identify and replace dysfunctional beliefs about mTBI with functional beliefs and enhancing effective coping, potential changes in coping styles and levels of anxiety and depression will be also investigated.
Methods
Design and setting
This RCT (trial number: ISRCTN86191894) is part of a larger observational cohort study on outcome in mTBI, the UPFRONT study. It was conducted between January 2013 and January 2016 in three level I trauma centers: University Medical Center Groningen, St. Elisabeth Hospital Tilburg, and Medical Spectrum Twente in the Netherlands. Patients included in the study filled out questionnaires at 2 weeks and 3, 6, and 12 months post-injury. Demographic variables, injury characteristics, and psychiatric history were obtained from the hospital records. The Injury Severity Score (ISS) was determined based on these records. 23 On admission, Glasgow Coma Scale (GCS) scores were determined as part of the neurological examination. A computed tomography (CT) scan of the brain was performed on admission and CT abnormalities were defined by the Marshall score (category 1 = no abnormalities; categories 2–6 = abnormalities). 24
Participants
The general UPFRONT study population consists of 1151 mTBI patients with age ≥16 years admitted to the emergency departments of the participating centers. In accord with the recommended guidelines of the American Congress of Rehabilitation Medicine, 25 mTBI was defined as an impact to the head resulting in a GCS score of 13–15 with: post-traumatic amnesia of ≤24 h and/or loss of consciousness of ≤30 min. Patients suffering from chronic alcohol and/or drug abuse and major psychiatric or neurological disorders were excluded. Patients without comprehension of the Dutch language or without a permanent home address were excluded because of anticipated follow-up difficulties.
For the subsequent enrollment in the intervention study, additional inclusion criteria were used: age from 18 to 65 years and normal admission CT. Further, patients eligible for the intervention must have paid work or be studying at the time of injury and had to be at risk for persistent post-traumatic complaints. Based on previous studies, patients reporting three or more complaints 2 –4 with at least one complaint in the cognitive or in the emotional domain were considered to be at risk.
Interventions
Cognitive behavioral therapy intervention
The CBTi was primarily aimed at the prevention of chronic complaints and to facilitate successful RTW. Emphasis was on providing psychoeducation on mTBI, identifying and replacing dysfunctional beliefs about mTBI with realistic beliefs, and enhancing effective coping and sense of self-control. Patients received a copy of “Recovery after mild TBI: a guide for patients and their families” 26 translated in Dutch and adjusted in consonance with the latest scientific knowledge. This guide informed patients on expected symptoms and strategies to cope with these symptoms and manage stress in order to facilitate a gradual increase of activities toward previous level of participation. 21
In total five sessions of 1-h treatment were given within a time period between 4 and 10 weeks post-trauma. The intervention was given in small groups of 2–4 patients by one of three experienced CBT-certified psychologist of the three participating trauma centers. The design of the CBTi protocol was partly based on the Cognitive and Graded Activity Training 27 protocol for dealing with fatigue after a cerebrovascular accident and was adjusted to fit the specific needs and characteristics of the mTBI group. The content of each session was structured and the same for all groups. Cognitive restructuring was used to train patients to identify their automatic negative thoughts and misattributions concerning the symptoms (e.g., “this will never go away”) and aid them to form constructive thoughts instead. Moreover, it was expected that by providing insight into their own coping style and promoting an active and assertive approach, patients' sense of self-control would grow, enabling them to develop more adaptive responses. 6 By scheduling activities in a way that allowed patients to perform them better (e.g., difficult tasks in the morning when a patient feels rested), rewarding activities were gradually increased. This, in turn, provided the patient with behavioral evidence of their intact abilities. 14 A detailed description of the CBTi with the content per session and case examples is available. 28
Telephonic counseling
The design of the TC intervention was to provide follow-up of patients in five sessions/conversations by phone comprising information and reassurance. At regular intervals after randomization, between 4 and 8 weeks after discharge, patients were contacted by phone weekly by two professionals (psychologist and a physician) from one of the participating trauma centers to monitor the course of eventual complaints or to answer questions regarding their recovery process. The TC sessions followed a protocol in which the first session contained psychoeducation, in the form of verbal information on common cognitive complaints and its usual course of recovery. In the subsequent sessions, recovery was monitored and patients had the opportunity to ask questions. The duration of the TC sessions varied strongly between patients and could last for a few minutes to an hour, depending on the patients need. Patients in the TC intervention did not receive any written information. With the exception of discouraging health endangering behavior (e.g., resuming boxing shortly post-injury), the content of provided information was restricted to explanation/reassurance of the nature of complaints without giving instructions to the patient concerning modification of behavior or exercise in the home situation.
Measures
Primary outcome measure
Return to work (or study)
The level of RTW or study was determined by self-report and was included in all intervals after injury (2 weeks and 3, 6, and 12 months). Patients could indicate whether they had a full RTW at the previous level, partial RTW or RTW at a lower level, or whether they had no RTW. For analysis of RTW, we made a dichotomization between 1) a successful return to work (i.e., full RTW) and 2) an unsuccessful return to work (i.e., partial/lower level or no RTW)).
Secondary outcome measures
Functional outcome
The extended version of the Glasgow Outcome Scale-Extended (GOSE) 29 is a structured questionnaire with an 8-point scale ranging from good recovery (8) to death (1). The GOSE was used for outcome measurement at 6 and 12 months and was dichotomized into favorable outcome (GOSE 8) and unfavorable outcome (GOSE ≤7).
Post-traumatic complaints
The Head Injury Symptom Checklist (HISC) 30 is derived from the Rivermead Post-concussion Symptoms Questionnaire (RPQ) 31 and has been used in clinical and research setting for many years. 30,32,33 The HISC describes 21 complaints commonly described post-TBI, and although derived from the RPQ, there are some differences with some questions being added or left out. Like the RPQ, the HISC comprises questions on headache, dizziness, fatigue, forgetfulness, concentration problems, slowness, irritability, and noise sensitivity. Questions on light sensitivity, blurred vision, and depressed mood were left out in the HISC. The HISC also contains questions that are not present in the RPQ, like questions on hearing loss, sleeping problems, neck pain, and anxiety. Also, two non-post-traumatic complaints (itchiness and dry mouth) are assessed as an indicator of a tendency to complain. For all 21 complaints, a pre-injury and a current symptom level were indicated by the patient. Values range from 0 to 2 (0 = never, 1 = sometimes, and 2 = often). The total amount of complaints (from 0 to 21) and the severity of complaints (0 to 42) can be determined. The total number of complaints (adding up from 0 to 21) was used to determine at risk status, of which three or more complaints has been used previously.
Coping style
The Utrechtse Coping List (UCL) was used to measure coping style, which refers to the efforts made to minimize the impact of stressful events. 34 The UCL consists of 47 items divided into seven subscales that represent different coping styles, of which only the scores on the active and the passive coping style were analyzed. Scores on these subscales are summed up to a total score for each subscale. Based on norm scores, these sum scores are labeled on a 5-point scale, from a very low use (1) of that coping style to very high use (5).
Depression and anxiety
The presence or absence of depression and/or anxiety was assessed by means of the Hospital Anxiety and Depression Scale (HADS). 35 The HADS is a 14-item questionnaire with two subscales, the depression scale (HADS-D) and anxiety scale (HADS-A) of seven items each. Items are rated on a scale from 0 to 3. In our analyses, we use the recommended cut-off score of ≥8 for establishing the presence of both depression and anxiety. 36
Statistical analyses
Data were analyzed with SPSS software (version 22.0; IBM Corp. Armonk, NY). 37 Differences in demographics and injury-related characteristics between the included group and the total mTBI group were tested using the chi-square test (categorical data) and two-sample Student's t-test (parametric data). Where appropriate, other nonparametric tests were used. To investigate the effects of the intervention, group differences in rate of full RTW and outcome scores (dichotomous variables) on different time intervals were analyzed using chi-square. A two-way repeated-measures mixed analysis of variance (ANOVA) was used on coping styles, the number of reported complaints, anxiety, and depression to investigate the effect of the two interventions over time. Where the assumption of sphericity was violated, the Greenhouse and Geisser 38 column was used to correct the repeated-measures ANOVA. Post-hoc mean comparisons were performed using univariate tests under the Bonferroni criterion. Alpha was set at 0.05, two-sided.
Results
Inclusion procedure and population
Figure 1 shows the flow chart of included mTBI patients. Of the 1151 mTBI patients, 91 were randomized into one of the interventions. The CBTi group consisted of 44 patients (with 5 drop-outs) and the TC group consisted of 47 patients (with two drop-outs) with 84 patients remaining for analysis. Response rates for the follow-up measurements (6 and 12 months) were 75% and 84% for the CBT group and 79% and 91% for the TC group.
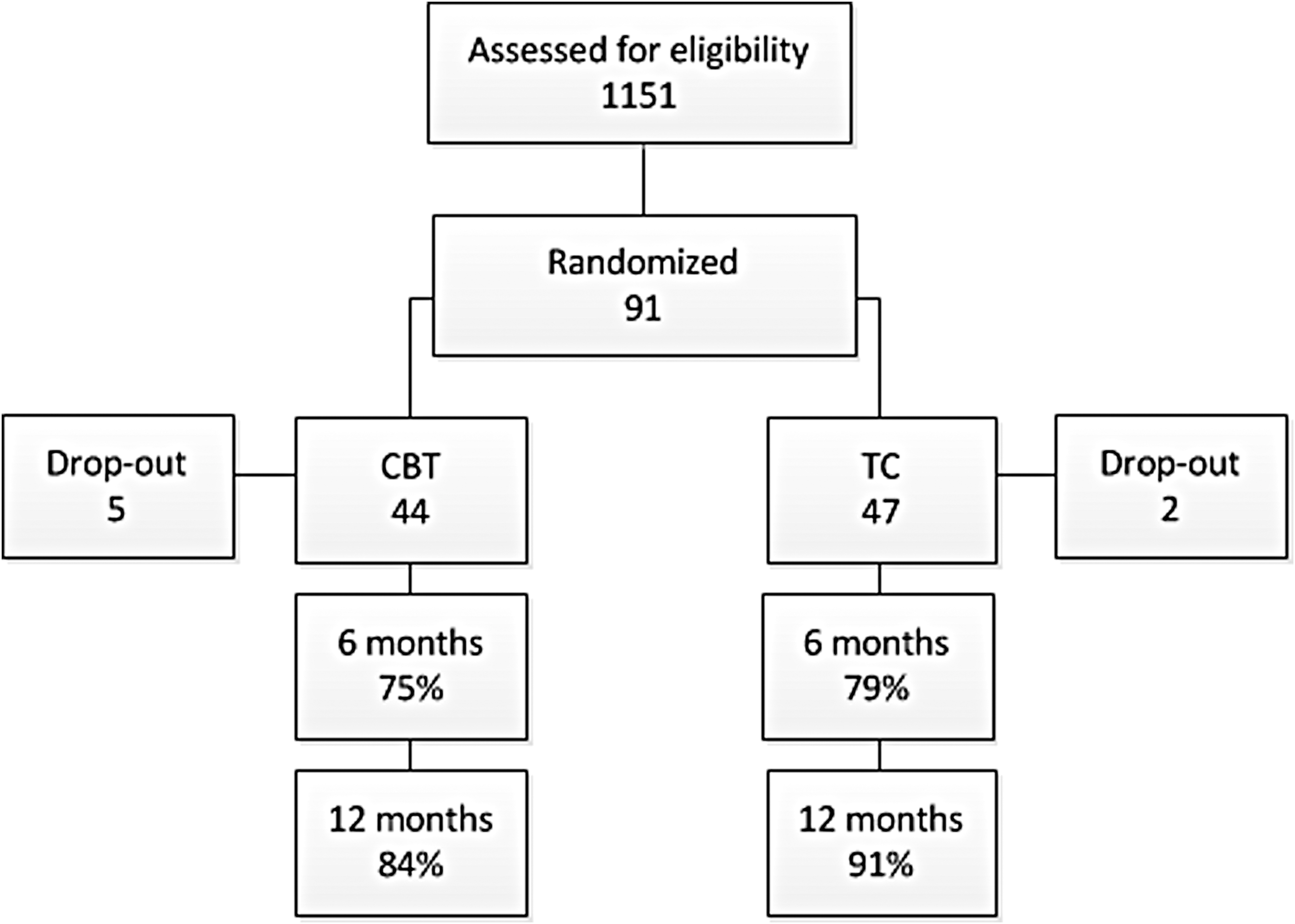
Flow chart of inclusion procedures. CBT, cognitive behavioral therapy; TC, telephonic counseling.
Table 1 shows a comparison of the CBTi group and the TC group on demographics, injury characteristics, and post-injury care. The CBTi group did not differ significantly from the TC group with regard to age, sex, educational level, GCS score, hospital admission, ISS, and the presence of CT abnormalities. No group differences were found with regard to use of medication, post-injury interventions, and the presence of a psychiatric history.
Mean (±SD), range; all others = number (%).
Pearson's chi-square tests, Mann-Whitney U tests, and independent t-tests.
CBTi, cognitive behavioral therapy intervention; TC, telephonic counseling; GCS, Glasgow Coma Cslae; ISS, Injury Severity Score; CT, computed tomography; SD, standard deviation.
Table 2 shows a comparison between the patient group included for intervention and the rest of the total mTBI study population. The intervention group comprised significantly more females and had a lower age and a slightly higher educational level. The included intervention group reported significantly more complaints on average than the total mTBI group with significantly higher anxiety and depression scores.
Mean (±SD), range; all others = number (%).
Pearson's chi-square tests, Mann-Whitney U tests, and independent t-tests with Cohen's d effect sizes.
GCS, Glasgow Coma Scale; ISS, Injury Severity Score; HISC, Head Injury Symptom Checklist; HADS-A, Hospital Anxiety and Depression Scale–Anxiety subscale; HADS-D, Hospital Anxiety and Depression Scale–Depression subscale; NS, not significant.
Effect of the intervention: level of return to work
Figure 2 shows an overview of the percentage of patients that had a full RTW at 2 weeks (pre-intervention), 3 months (post-intervention), and at 6 (follow-up 1) and 12 months (follow-up 2). No significant differences in percentages with full RTW were found between CBTi and TC pre-intervention. No differences between groups were found post-intervention, at follow-up 1, or follow-up 2.

Percentage of patients with a full RTW over a 1-year time period. CBT, cognitive behavioral therapy; RTW, return to work; TC, telephonic counseling.
Functional outcome
Table 3 shows a comparison of the two intervention groups with regard to the rate of favorable outcome. No significant differences were found between groups on the 6-month measurement. At 12 months post-injury, the TC group had significantly more patients with a favorable outcome than the CBTi group.
Number (%).
GOSE, Glasgow Outcome Scale-Extended; CBTi, cognitive behavioral therapy intervention; TC, telephonic counseling; NS, not significant.
Post-traumatic complaints, anxiety, and depression
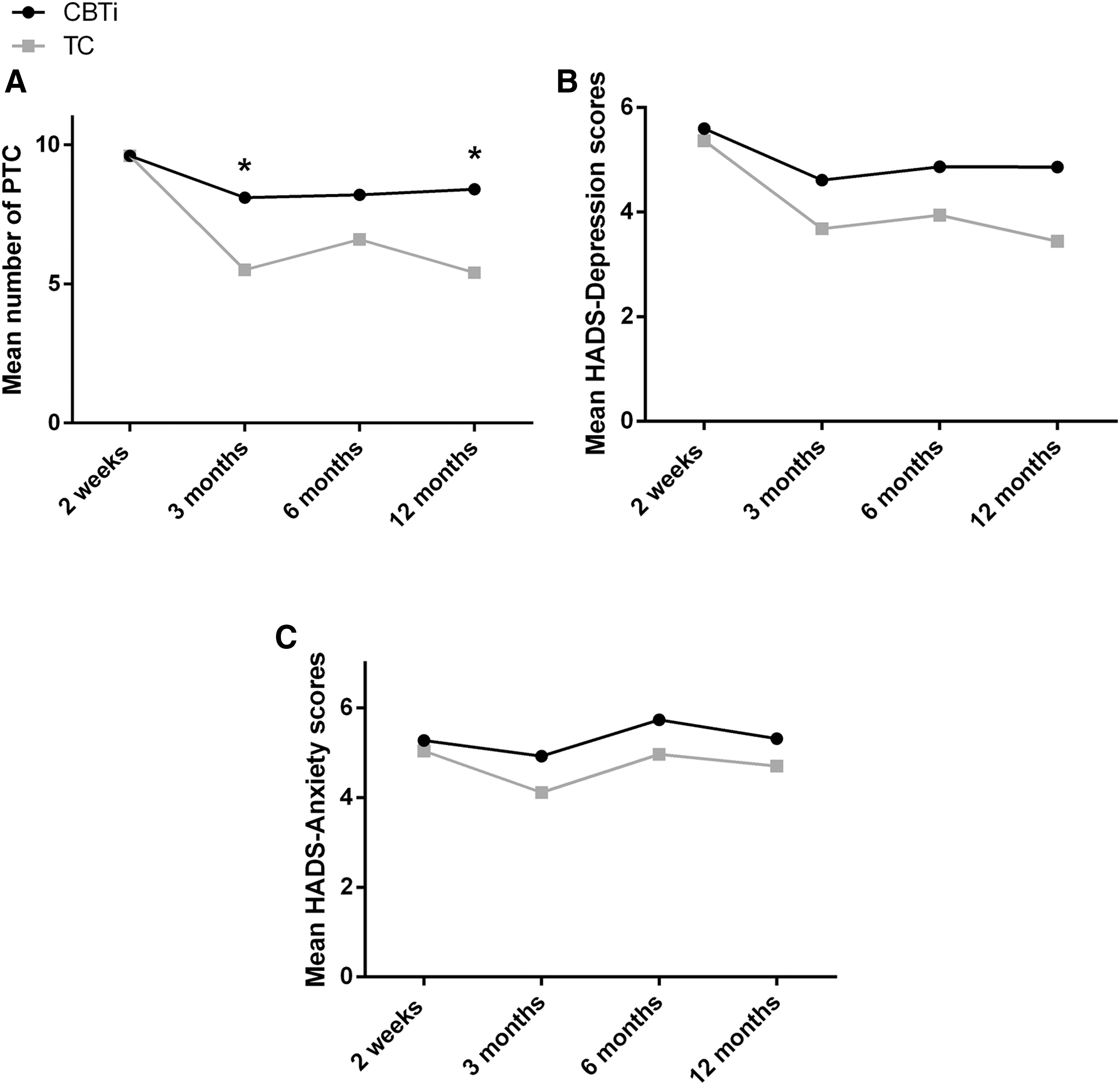
Figure 3A shows the effect of the two interventions over time on the number of reported post-traumatic complaints. Pre-intervention, no significant difference was found in the number of reported complaints between groups. The mean number of post-traumatic complaints significantly decreased over time in the TC group (F (3, 102) = 10.98; p < 0.001), but not in the CBTi group (F (3, 90) = 1.76; p = 0.161). Post-hoc analyses showed that the number of reported post-traumatic complaints was significantly lower in the TC group from 2 weeks to 3, 6, and 12 months post-injury (M = 4.17; p < 0.001; d = 1.46; M = 3.02; p = 0.002; d = 0.8 and M = 4.25; p < 0.001; d = 1.08). Post-intervention, there was a significant interaction between the intervention conditions and time on post-traumatic complaints (F (3, 192) = 2.97; p = 0.033). Patients in the TC group reported significantly fewer complaints at 3 and 12 months than those in the CBTi group (8.4 vs. 5.8; t = 2.63; p = 0.010; d = 0.61 and CBTi 8.5 vs. TC 5.2; t = 2.82; p = 0.006; d = 0.65). No differences between groups were found on the 6-month follow-up (CBTi 8.3 vs. TC 6.5).
Repeated-measures analysis of variance for post-traumatic complaints (
Figure 3B,C shows the mean depression and anxiety scores over the different time measurements. Pre-intervention, both groups started with equal levels of depression and anxiety. No differences in mean anxiety scores were found over time for the TC (F (3, 75) = 0.56; p = 0.639) and CBTi group (F (3, 78) = 1.09; p = 0.357). For mean scores on depression, no differences were found over time for the TC (F (3, 75) = 2.66; p = 0.054) and CBTi group (F (3, 75) = 0.89; p = 0.452). There was no significant interaction between the intervention and time on depression (F (3, 150) = 0.199; p = 0.884) or anxiety (F (3, 153) = 0.196; p = 0.882). Although there seems to be a trends toward patients in TC having lower depression and anxiety scores, no significant differences between groups were found on either the 3-, 6-, or 12-month measurements.
Coping style
Pre-intervention, both groups had a comparable use of the active coping style (CBTi 19.4 vs. TC 19.3). Patients in the TC group had a significantly higher use of the passive coping style before the start of the intervention (CBTi 10.5 vs. TC 12; p = 0.043). The mean score on the passive coping scale did not change over time in the TC (F (2, 46) = 0.57; p = 0.569) or the CBTi group (F (2, 38) = 1.23; p = 0.303). The mean score on the active coping scale significantly decreased over time in the TC group (F (2, 38) = 4.39; p = 0.019), but not in the CBTi group (F (2, 44) = 0.148; p = 0.148). Post-hoc analyses showed that active coping scores were significantly lower in the TC group from 2 weeks to 3 months only (M = 1.95; p = 0.021). No interaction effect was found of the CBT and TC interventions over time on the use of these coping styles (F (2, 78) = 0.543; p = 0.583 and (F (2, 80) = 0.450; p = 0.639).
Discussion
The primary aim of this study was to investigate the additional value of an early preventative CBT intervention in comparison to early TC in improving RTW in at-risk mTBI patients. Secondary goals of the intervention were to enhance coping skills and decrease post-traumatic complaints, anxiety, and depression. Previous research has already demonstrated that TC was effective in decreasing post-traumatic complaints when compared to care as usual. 22 We hypothesized that an early CBT intervention might even be more effective in reducing post-traumatic complaints as well as improving RTW and outcome. In contrast with this expectation, we found that it was TC that had a positive influence on recovery. We did not find that CBT resulted in better RTW than TC, but patients in the TC group reported fewer post-traumatic complaints than those in CBTi at 3 and 12 months post-injury. Moreover, without pre-intervention differences between groups, patients who received TC had a better functional outcome than those in the CBT intervention group 1 year post-injury. No effects were found of either intervention with regard to coping styles and levels of anxiety and depression.
Interestingly, we not only found that the TC group reported fewer post-traumatic complaints on 3 and 12 months post-injury than the CBTi group, but also that the TC group had a compellingly larger percentage of patients with a favorable recovery (62% vs. 39%). With regard to the results on post-traumatic complaints, the fact that we did not find significant differences on 6 months post-injury might be explained by the temporary increase in complaints. Although we cannot confirm this with our data, it is possible that this is the point of time in which patients fully resume their previous activities, which temporarily causes an increase in complaints. 39 The overall decrease in complaints over time can be explained by earlier research, in which the advantageous effects of solely giving information, education, and reassurance 40 –42 have been repeatedly shown. As expected, our results with regard to the decrease in post-traumatic complaints were analogous to the study by Bell and colleagues. 22 They found a reduction in complaints at 6 months post-injury when compared to care as usual. However, their reported differences between groups were modest and a nonvalidated scale was used for outcome, which makes it difficult to determine the clinical relevance of their findings. Our study is the first to report a clinically meaningful positive effect of TC on (long-term) functional outcome.
Although we cannot rule out that the CBT might have had some beneficial effects on functioning of the patients, these were similar to, or significantly lower than, those of the TC treatment. It is possible that for this population with rather mild injuries, an intervention that requires patients to return to the hospital five times to see a psychologist is overdone. It might even magnify patients' perception of the severity of their injury and diminish the positive effect of psychoeducation. In an earlier study, it was found that patients who had stronger beliefs about the seriousness of their injury had an increased risk of developing persistent complaints. 11 It is possible that our CBTi sessions in groups unintentionally had a medicalizing and reinforcing effect on the perceived complaints, 43 whereas the individual TC sessions were more low key and more suited for giving information and reassurance. For example, the TC sessions might have been more tailored to the needs of the individual patient, by not having a fixed duration. However, although the CBTi group did have a higher number of complaints and a higher number of patients with an unfavorable outcome, RTW was equal to the TC group. Therefore, the focus on how to deal with work situations and the company doctor during the CBTi sessions might have contributed to patients resuming their work despite their complaints.
Regarding the secondary aim in our study to decrease levels of anxiety and depression, we found no differences between CBTi and TC over time with regard to these measures. Considering the fact that CBT has proven to be successful in treating anxiety or depression by facilitating the use of an adaptive coping style post-mTBI, 18,44 we expected the CBTi group to show a higher reduction of these signs of psychological distress when compared to the TC group. However, our at-risk group, included on the basis of complaints, comprises a broad range of patients, of which only some patients showed additional signs of distress, such as depression and/or anxiety. This even more at-risk subgroup of patients with additional mental problems are likely to benefit more from the intensive approach of a CBT treatment. However, we consider it possible that for these patients with psychological comorbidities, our five-session prevention was even too short.
With regard to the additional aim of improving coping styles, we did not find any effect of the interventions on the passive or active coping styles. However, we did find that active coping style scores in the TC group decreased significantly over time, in the early phase post-injury (2 weeks to 3 months). Although counterintuitively, active coping in the early stages post-injury has been found to be predictive of poor outcome, 45 by having high demands of one's own level of functioning and doing too much in a phase in which resting is very important for recovery. Therefore, a decreased use of this coping style could thus have supported the more favorable outcome of the TC group.
Although this study offers valuable new findings with important clinical implications, some limitations need to be addressed. First, our study did not have a control group with a high number of post-traumatic complaints that received care as usual. This could potentially weaken the conclusions that can be drawn from this study. However, our population was comparable to the population in which Bell and colleagues 22 did compare the effects of TC with care as usual and found beneficial effects of TC. Our aim was to build on the findings of this study, concluding that TC was superior to care as usual, and investigate the additional value of CBT techniques. Second, although we used a widely used and accepted measure of RTW, 46 it remains a multi-dimensional variable. There are several non-treatment-related factors that can influence RTW, such as job satisfaction and the influence of economic circumstances, 46 which complicates our ability to draw causal conclusions on the rate of RTW in relation the intervention groups.
In summary, patients that received five TC sessions had a significant decrease of complaints over time and reported fewer post-traumatic complaints both at 3 months and 1 year post-injury than those that received five CBT sessions early post-injury, who showed no significant decrease of complaints over time. Moreover, significantly more patients in the TC group (more than 1.5 times as many) show a full recovery 1 year post-injury when compared to the CBTi group. No differences between groups were found with regard to RTW, anxiety and depression, and coping styles. This study is the first to report a positive effect of TC on long-term outcome, and these promising results could hold important implications for clinical practice. First, we deem it necessary to assess mTBI patients early post-injury on at least post-traumatic complaints to determine their risk of suffering from persistent post-traumatic complaints. Second, for the patients that are at risk, TC might constitute a very valuable intervention method, by being relatively nonexpensive and easy to implement. However, for at-risk patients with anxiety and mood disorders, a more intensive form of CBT might be warranted. Future research should be focused on optimizing allocation of at-risk patients to the most appropriate intervention, which will shed more light on the extent of the applicability of this intervention method.
Footnotes
Author Disclosure Statement
No competing financial interests exist.