
Abstract
The aim of this study was to characterize autonomic lesions in participants with spinal cord injury (SCI; n = 10) using an autonomic reflex screen, incorporating sudomotor, cardiovagal, and sympathetic adrenergic tests, as well as hemodynamic responses to head-up tilt (HUT). Hemodynamic responses were compared to healthy controls (n = 20) and previously published normative cutoffs in order better identify autonomic impairments. Sympathetic skin responses (SSRs), heart rate response to deep breathing (HRDB), and heart rate and beat-to-beat blood pressure responses to Valsalva maneuver (VM) and HUT were measured. SCI participants demonstrated impairment in at least one domain, with 7 of 10 demonstrating autonomic impairment across all domains. No single test was concordant with orthostatic hypotension on HUT, in all participants. Measures of cardiovagal function, including HRDB (SCI = 7.7 ± 3.8 beats/min vs. controls = 17.6 ± 8.1 beats/min) and Valsalva ratio (SCI = 1.53 ± 0.29 vs. controls = 1.85 ± 0.37), were significantly reduced in SCI participants, compared to controls (p < 0.05). These findings suggest that an autonomic reflex screen, which includes standardized testing protocol and normative data for comparison, is useful for determining the autonomic domains affected by the neurological injury in SCI. We also demonstrated significant cardiovagal impairment in SCI participants compared to controls, which warrants further investigation to determine whether cardiovagal dysfunction is associated with the negative cardiovascular outcomes, which are known to occur in SCI.
Introduction
A
Many measures are available to evaluate autonomic function; however, there is no single test reflective of function in all autonomic domains. The absence of sympathetic skin responses (SSRs), which represent the sympathetic cholinergic pathway, has frequently been used to characterize autonomic dysfunction in SCI. 11 SSRs are noninvasive and easy to acquire, but they have not always been shown to be associated with impairment in other autonomic domains. 12,13 Previnaire and colleagues 12 evaluated the relationship between level of neurological injury and severity of sympathetic autonomic dysfunction in patients with chronic, complete lesions above T6 (mean duration from injury = 4.1 years), including abdominal electrical stimulation and cold pressor tests below the level of the lesion, systolic blood pressure (SBP) responses to Valsalva maneuver (VM), as well as SSRs. They demonstrated concordance between the neurological level of injury and presence of sympathetic impairment below the level of the lesion, however not all participants demonstrated concordant SBP responses on all tests in the presence of absent SSRs. Further, some participants demonstrated some discordance between sudomotor and sympathetic adrenergic tests (e.g., absent SSRs with preserved SBP response to VM). This highlights the concept that a battery of autonomic tests are required to accurately and comprehensively evaluate the autonomic lesion in SCI. In addition, further information regarding the involvement of specific autonomic pathways in SCI is required, given that these tests are not routinely used in clinical settings, provide little information regarding the severity of impairment, and do not have control data for comparison. In order to comprehensively assess the ANS, measures of cardiovagal function should be included with sympathetic tests, given that abnormal vagal control of the heart has been implicated in the long-term risk of cardiovascular morbidity in other clinical populations. 14,15
The quantitative autonomic reflex screen (ARS), developed by Low and colleagues, 16 comprises sudomotor, cardiovagal, and sympathetic adrenergic tests, has a well-established test protocol, has comparative, quantitative reference data, and is widely used in clinical autonomic clinics. 16 –18 The ARS has been validated in many clinical populations, other than SCI. 18 –20 The ARS also incorporates hemodynamic responses to head-up tilt testing (HUT), which provide clinically meaningful information about the resilience of the ANS to orthostatic stress. Although some components of the ARS have been studied in the SCI population, no study to date has included all of the elements of the ARS to evaluate autonomic function in SCI. Systematic evaluation using the ARS could improve our understanding of the complexity of autonomic injury and provide information about the severity of autonomic impairment, compared to normative data and within the context of HUT.
Accordingly, the aim of this study was to use a validated and comprehensive clinical autonomic battery to characterize autonomic lesions in SCI, to determine the autonomic domains affected by the neurological lesion. In order to better identify cardiovagal and sympathetic adrenergic impairments, we compared SCI participants to healthy controls and to established normative cutoffs. We hypothesized that there would be some heterogeneity in the domains affected by the neurological injury, such that not all autonomic domains would be affected in all participants. Further, we hypothesized that comparing hemodynamic responses to normative cutoffs and a control group would be useful in identifying autonomic impairments.
Methods
Study participants
Consecutive SCI participants, who were eligible for and consented to the study, were recruited from the inpatient rehabilitation ward at a single academic center. Recruitment took place between 2014 and 2015. All participants underwent detailed physical examination, including the ISNSCI examination by their attending physician, upon admission for inpatient rehabilitation. Participants were included if they sustained traumatic SCI within the previous 3–6 months, had a ISNCSCI level A, B, or C, and had a neurological level of injury at T6 or above. 5 All ISNCSCI examinations were repeated on the day of testing by one of the study investigators (M.B.) to ensure accurate classification. T6 was selected, because lesions at this level or above are typically associated with significant cardiovascular sequelae, including OH and autonomic dysreflexia. 1 Patients were excluded or data collection was delayed in those receiving treatment for an acute medical condition. Common active conditions in this population were: delayed weaning from mechanical ventilation requiring tracheostomy, urinary tract infection or urosepsis, or skin ulcer in a location where data collection instruments would be applied to the skin.
When possible, all testing was performed on the same day and individual components of the ARS were performed in the same order. In 1 participant, the VM was performed a separate day (1 week preceding the rest of the ARS). Participants were instructed to abstain from eating, drinking, and cigarette smoking for 8 hours preceding testing. Tests were usually administered early in the morning, before medication administration. In this manner, anticholinergic and sympathomimetic medications that could confound hemodynamic measurements were held before testing.
A modified ARS was used in this study to measure multiple domains of the autonomic nervous system. Sudomotor function was measured with SSRs, cardiovagal function was measured with heart rate response to deep breathing (HRDB) and the Valsalva Ratio (VR), and sympathetic adrenergic function was assessed with hemodynamic responses to VM and HUT test. It is important to note that SSRs were selected as the measure of sudomotor function in this study. The ARS, originally described by Low, typically utilizes quantitative sudomotor axon reflex testing (QSART), for sudomotor testing. We did not elect to use QSART in this study because it predominantly assesses the integrity of the post-ganglionic sympathetic cholinergic neurons, which presumably would not be affected by the neurological lesion in SCI. Further, SSRs are one of the most frequently used tests used to evaluate autonomic function in the SCI literature. 11 In this regard, the ARS used in this study is to be considered a modified version of Low's ARS.
All tests were performed supine, with the exception of HUT. Testing was preceded by a minimum of 5 min of supine rest. The order of the testing was SSRs, HRDB, VM, and HUT, with 5 min of supine rest allocated between tests. Approval for the study was obtained from the local institutional ethics board. Informed consent was obtained before testing.
Hemodynamic parameters in SCI participants during HRDB, VM, and HUT were compared to the results from randomly selected age- and sex-matched control subjects taken from a large normative data set that has been published previously. 17 The protocols used in the present study for data collection were similar to those used in the normative data set, with the exception of the angle of the tilt-table during HUT (see below).
Sympathetic skin responses
SSRs were acquired and stored for offline analysis with standard clinical electromyography equipment (Dantec Keypoint® 4 system; Natus Medical Incorporated, San Carlos, CA). Self-adhesive silver/silver chloride electrodes were applied bilaterally to the hands and feet, after the skin was abraded with fine sandpaper and cleansed with isopropyl alcohol, in order to minimize impedance. Active recording electrodes were placed over the mid-palms and mid-soles, whereas reference electrodes were placed over the dorsum of the hands and feet. Ground electrodes were placed over bony protuberances at the wrist and ankle. Electrical stimulation was used to elicit SSRs. Supralesional stimulation sites were the supraorbital nerve above the eyebrow or the median nerve at the wrist, depending on the neurological level of injury. A constant current stimulator (intensity = 10–100 mA; duration = 0.2 ms) was used, and stimulation intensity was increased incrementally until a muscle twitch was observed, in order to verify stimulator placement. A total of five supralesional stimuli were delivered for each participant, separated by a minimum of 60 sec, in order to prevent habituation. SSRs were classified qualitatively as present or absent, based on the characteristic latency and bi- or triphasic pattern of the waveform. 11 A participant was determined to have absent sympathetic cholinergic function, if the number of infralesional responses was 0–1 bilaterally and no impairment if the number of infralesional responses was 2–5 bilterally. 21
Heart rate response to deep breathing, Valsalva maneuver, and head-up tilt
Beat-to-beat BP was measured over the second or third digit by finger cuff photoplethysmography (Finometer PRO; Finapres Medicine Systems, Amsterdam, The Netherlands). Brachial blood pressure (BP) was measured with an automated arm cuff (Dinamap Pro 300 V2; GE Healthcare, Milwaukee, WI) to corroborate the measures from the Finometer. Single-lead electrocardiography (ML 132; ADInstruments, Colorado Springs, CO), with electrodes over the anterior deltoids and left flank, were used to measure R-R interval. All data were collected at a sampling rate of 1000 Hz using an A-D converter and stored for offline analysis using data collection software (Powerlab/16SP ML 795 and LabChart 7; ADInstruments).
For HRDB, participants were instructed to perform eight breathing cycles at a frequency of 6 breaths/min, using auditory cueing. The study examiner observed each participant to ensure inhalation and exhalation were performed as deeply as possible. The five largest consecutive amplitudes were averaged to calculate HRDB for each participant (Fig. 1).
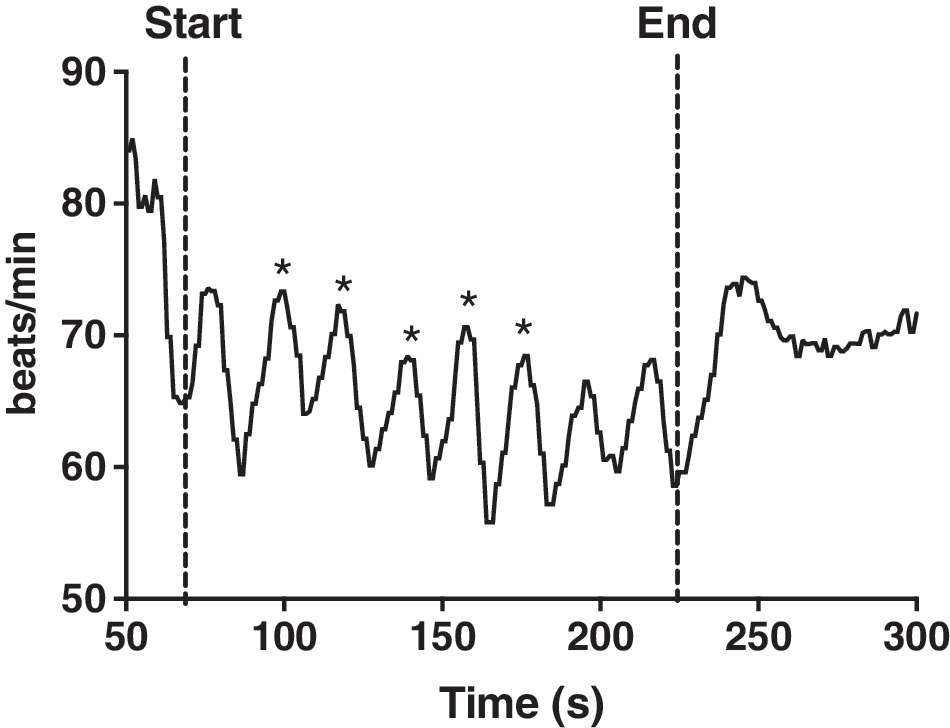
Heart rate response to deep breathing (HRDB) in a representative participant with spinal cord injury (participant 7 from Table 1). Eight breathing cycles (full inspiration and expiration) were performed at six cycles/min. The average amplitude of the five largest consecutive breaths (denoted by asterisk [“*”]) was used to calculate HRDB for each participant.
A commercially available portable sphygmomanometer connected to a breathing tube was used to facilitate VM. The breathing tube was connected to a mouthpiece that provided partial resistance to airflow. Two or three trials for VM were performed in order to yield two reproducible trials. Each trial was separated by 2 min of rest. The trial in which the participant achieved the best and most consistent effort was used for subsequent analysis. Participants were instructed to maintain exhalation pressure at 40 mm Hg for 15 sec, because this pressure and duration have been shown to yield the most valid and reproducible hemodynamic responses. 16 VR was calculated as the maximum HR during Phase II of the VM, divided by the minimum HR within 30 sec of Phase IV (Fig. 2). The beat-to-beat BP waveform was inspected visually to establish the presence or absence of sympathetic adrenergic-mediated phases (Phase II Late and Phase IV Overshoot) and to characterize the overall shape of the waveform as predominantly “M” pattern (normal hemodynamic response to VM) or “V” pattern (abnormal hemodynamic response to VM, with absent or blunted Phase II Late and Phase IV; Fig. 3), according to Palamarchuk and colleagues. 22
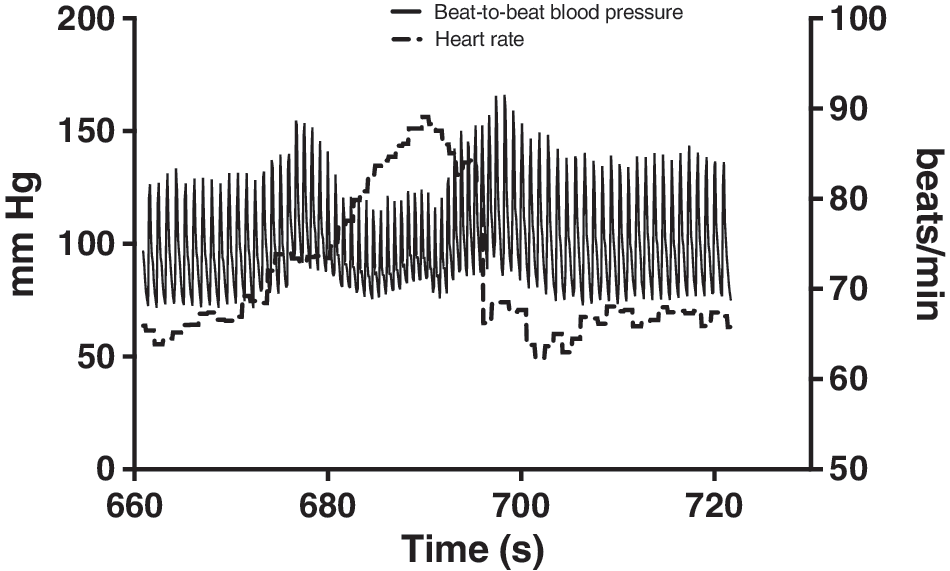
Beat-to-beat blood pressure (left y-axis) and heart rate (HR) responses (right y-axis) during a Valsalva maneuver (VM) in a representative participant with spinal cord injury (participant 8 from Table 1). The Valsalva Ratio is derived from the ratio of highest HR measured during the VM, to the lowest measured within 30 sec after VM is released.
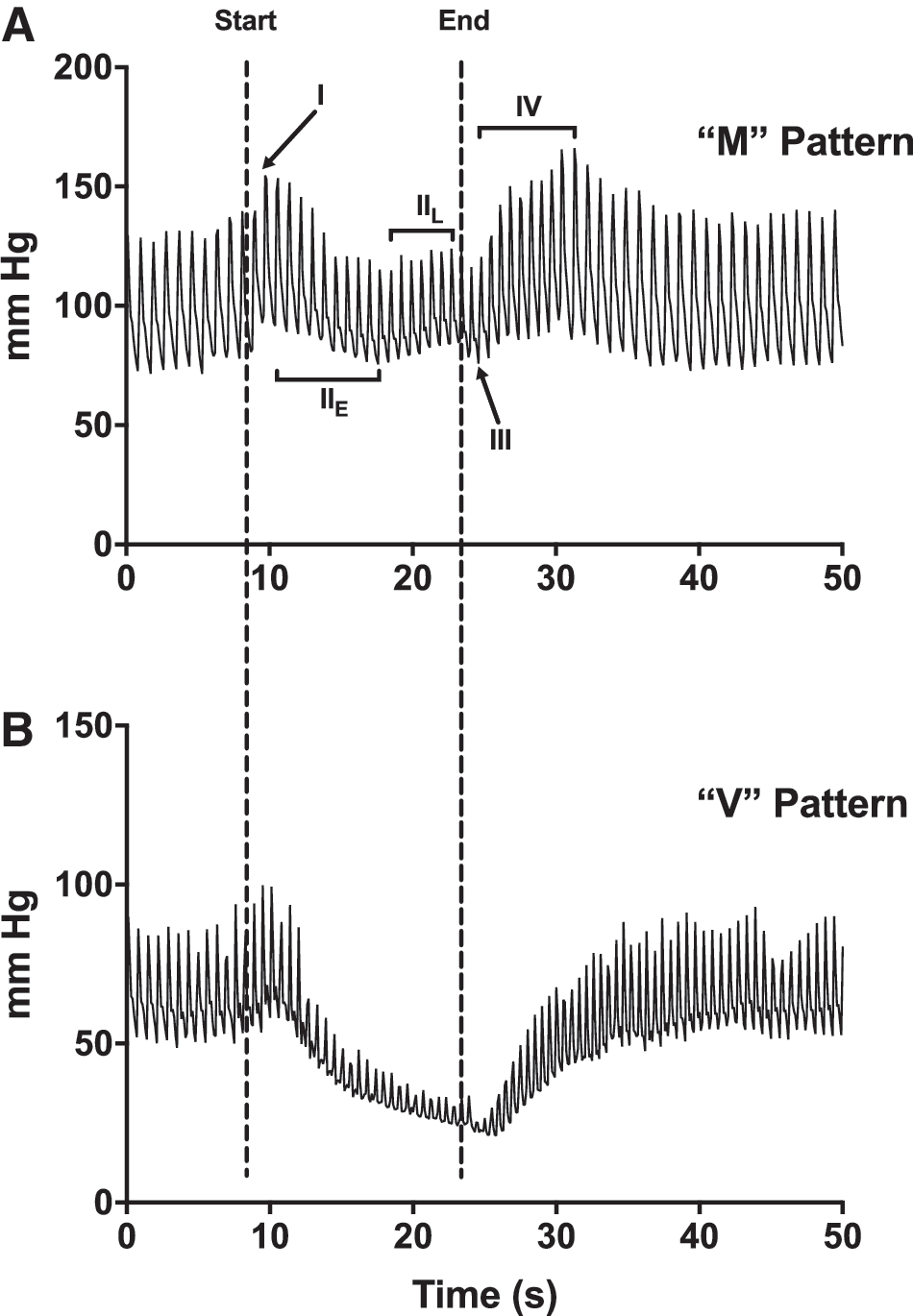
Beat-to-beat blood pressure (BP) traces during a 15-sec Valsalva Maneuver (VM) for a representative participant with a normal sympathetic adrenergic response (
HUT was performed with participants transferred to an automated tilt table. Velcro waist and thigh straps were used to secure participants to the tilt table. Supine and HUT BPs were taken with an automated arm cuff at 1-min intervals throughout the test, to ensure accurate recording from the Finometer. The participant's arm was positioned in a sling to keep the cuffed finger at heart level, in order to maintain Finometer BP calibration. The angle of tilt used in this study was 45 degrees, in order to ensure that participants with paresis could remain on the table in a neutral position. Further, 45 degrees was an ample orthostatic challenge to elicit OH in the majority of participants in the study (see Results). The target duration for upright tilt was 10 min, unless any one of the following stopping criteria were met: 1) precipitous drop in SBP >40 mm Hg; 2) intolerable orthostatic symptoms; or 3) an early alteration in consciousness. A period of 5 min of supine rest with ongoing hemodynamic monitoring occurred at the end of HUT, to ensure that each participant returned to baseline HR and BP. The hemodynamic parameters reported in this study were: 1) ΔHR = maximum HR between 2 and 5 min of HUT – average HR 30 sec before HUT and 2) ΔSBP = average SBP 30 sec before HUT – minimum SBP during HUT. For participants meeting the stopping criteria within the first 2 min of HUT, maximum HR and minimum SBP were used the calculate delta HR and delta SBP, respectively.
Healthy control participants
Hemodynamic responses to HRDB, VM, and HUT were compared between SCI participants in this study and previously published data from 20 participants drawn from a large normative data set. 17 Control subjects were age- and sex-matched to the SCI participants, because hemodynamic parameters differ between males and females and across age ranges. 17 The only difference in protocol between the present study and the control study was that control subjects performed HUT at an angle of 70 degrees. Otherwise, similar methods were used to obtain HR and BP parameters during HRDB, VM, and HUT. Participants were characterized as having abnormal cardiovagal function by comparing HRDB to previously established normative cutoffs, stratified for age and sex. 18 Sympathetic adrenergic impairment was defined by a “V” patterned beat-to-beat BP waveform, in response to VM. 22 OH was defined by a drop in SBP >20 mm Hg or DBP >10 mm Hg on HUT. 23
Statistical analyses
Demographic data were described with means and standard deviations (SD). Unpaired t-tests were used to assess difference between SCI participants and healthy controls for demographic and hemodynamic parameters. Level of significance was set at p < 0.05. All statistical tests were performed with GraphPad Prism software (version 7; GraphPad Software Inc., La Jolla, CA).
Results
Demographic characteristics for SCI participants and healthy controls are presented in Tables 1 and 2, respectively. No significant difference was observed between the two groups for age, height, or mass, and SDs were similar for both groups (p > 0.05). SSRs for SCI participants are presented in Table 3, where 8 participants demonstrated absent infralesional SSRs and 1 participant demonstrated two infralesional SSRs, but only unilaterally. Hemodynamic responses to HRDB, VM, and HUT are presented in Table 4. Cardiovagal parameters (HRDB and VR) were significantly lower in SCI participants, compared to healthy controls (p < 0.05). For HUT, ΔHR was similar between groups (p > 0.05), whereas ΔSBP was significantly reduced in SCI participants (p < 0.05).
ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; SD, standard deviation; M, male subjects; F, female subjects.
SD, standard deviation; M, male subjects; F, female subjects.
aSupralesional stimulation site was the supraorbital nerve for lesions at C4–T1 and median nerve for lesions at T2–T6.
ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; RH, right hand; LH, left hand; RF, right foot; LF, left foot.
Significant difference between SCI subjects and healthy controls (p < 0.05).
HRDB, average heart rate variability with deep breathing; VR, Valsalva ratio; ΔHR, change in heart from supine to head-up-tilt; ΔSBP, change in systolic blood pressure from supine to head-up-tilt; SCI, spinal cord injury; SD, standard deviation.
Figure 4, Figure 5, and Table 5 are used to illustrate autonomic parameters for individual SCI participants. Individual beat-to-beat BP traces during VM are presented in Figure 4. Eight participants demonstrated a “V” patterned BP response to VM, with absent Late Phase II, Phase IV Overshoot, or both indicative of sympathetic adrenergic impairment. Two participants demonstrated normal, “M” pattern responses. Individual HR and SBP responses to HUT are presented in Figure 5. Seven participants met for OH, and HUT was terminated early in 6 of these individuals for meeting at least one of the stopping criteria. Table 5 is used to illustrate an individual participant's response to the multiple autonomic domains that were tested in this study. Seven participants demonstrated autonomic impairment across all domains, and OH on HUT. The BP response to VM, representing sympathetic adrenergic dysfunction, was concordant with SBP response to HUT in 9 of 10 participants (i.e., a participant demonstrating “V” pattern during VM similarly met the criteria for OH during HUT, whereas a single participant demonstrating an “M” pattern during VM similarly had no evidence of OH during HUT).
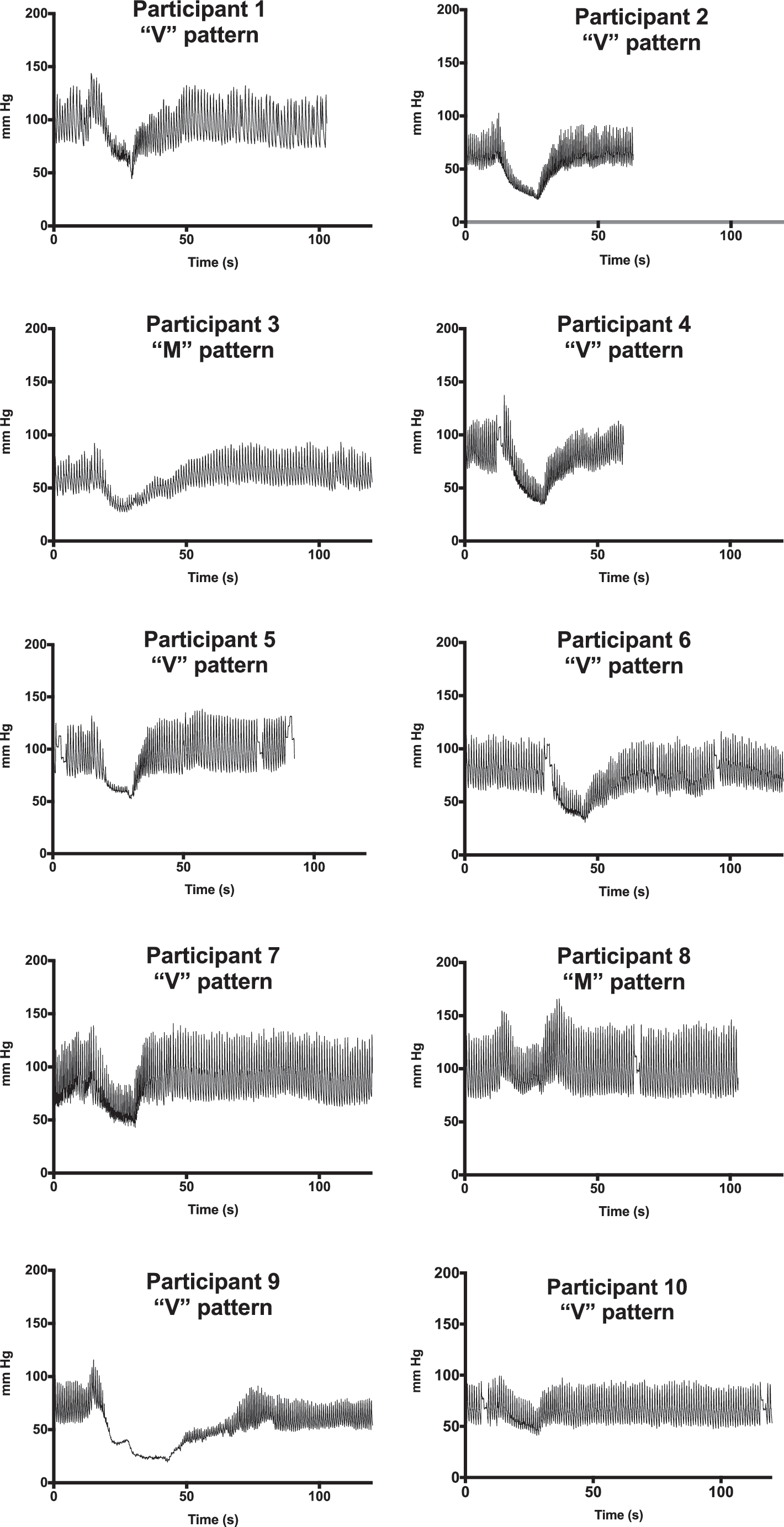
Individual beat-to-beat blood pressure traces for each study participant with spinal cord injury. Each figure is labeled with corresponding qualitative waveform pattern (i.e., “V” pattern indicative of sympathetic-adrenergic dysfunction; “M” pattern indicative of normal sympathetic adrenergic function).

Individual systolic blood pressure (black line; left y-axis) and heart rate (dotted line; right y-axis) responses to head-up-tilt, for participants with spinal cord injury. The test duration for each participant that met the stopping criteria for early test termination is labeled accordingly. Note that participant 5 displayed significant heart rate variability from 114 to 155 sec into the test as a result of a misplaced electrocardiogram electrode.
“±” represents presents/absence of autonomic impairment.
Defined by HRDB less than the normative cutoff described in Novak. 18
Defined by “V” pattern of beat-to-beat BP waveform during Valsalva maneuver.
Defined by SBP drop >20 mm Hg on head-up tilt, according to Kaufmann. 23
ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury Impairment Scale; OH, orthostatic hypotension; HRDB, heart rate response to deep breathing; BP, blood pressure; SBP, systolic blood pressure.
Discussion
The ARS, pioneered by Low and others, 16,18 is routinely used in the diagnosis of autonomic impairment in many clinical populations, and this study constitutes the first application of a modified version of the ARS protocol for measurement of multiple domains of autonomic function in participants with SCI. The major findings of this study are: 1) heterogeneity in the domains of autonomic function affected by the neurological lesion in SCI, such that impairment is not uniform across all domains, and in all participants, and 2) significant cardiovagal abnormalities in SCI participants compared to healthy controls and to normative cut-off values, using standardized autonomic measures. We also provide visual representations and novel qualitative characterizations of the hemodynamic response to VM, which could be a useful reference for clinicians in the diagnosis of sympathetic adrenergic impairment in SCI.
Previnaire and colleagues 12 used a battery of sudomotor (SSR) and sympathetic adrenergic tests (SBP response to VM, cold pressor testing, abdominal electrical stimulation, and mental arithmetic) to demonstrate that the majority of patients with complete, chronic SCI have sympathetic impairment below the level of the lesion. However, they also demonstrated that not all autonomic tests are equal in demonstrating impairment. For example, 18 of 26 participants demonstrated SBP increases (indicative of absent or impaired supraspinal control) during either abdominal electrical stimulation or foot cold pressor testing, but not both. Further, some paraplegic patients demonstrated discordance between infralesional sympathetic cholinergic and sympathetic adrenergic function in participants with chronic SCI, particularly in paraplegic participants. Some participants in their study had preserved infralesional SSRs, but displayed concomitant abnormalities in the sympathetic responses to cold pressor testing, abdominal electrical stimulation, or in the Phase IV Overshoot of the SBP response to VM.
In keeping with the results of Previnaire's group, the majority of our participants demonstrated autonomic involvement in all domains, particularly those with complete, tetraplegic injuries (Table 5). However, our results also highlight the possibility of heterogeneity of autonomic lesions in SCI, given that 3 participants in our study had preservation of normal autonomic responses in some domains and not all participants had OH with HUT, despite having some autonomic impairment. The results of Previnaire's group warranted further investigation because they did not assess cardiovagal function, did not include a clinical measure of dysautonomia such as HUT, and did not select sympathetic adrenergic tests with standardized protocol or definitions of autonomic impairment. In particular, hemodynamic responses to cold pressor testing and abdominal electrical stimulation are not standardized and do not have established cutoffs for abnormality. Although they did use SBP response to VM, they only described the Phase IV of the response and did not present visual representations of the responses for qualitative analysis. Further, their study was performed in participants with chronic SCI.
We studied both sensorimotor complete and incomplete participants during the inpatient rehabilitation phase of SCI. Although we do not possess a large enough sample to make inferences about lesion severity and autonomic dysfunction, our results do suggest that those participants with more proximal and complete injuries (American Spinal Injury Association Impairment Scale A or B) are more likely to have involvement across autonomic domains. Further, identification of specific domains of impairment in participants in this study could have clinical implications with regard to the diagnosis and management of secondary complications of SCI, including pressure ulcers (sudomotor dysfunction), OH and reduced exercise tolerance (sympathetic adrenergic dysfunction), and, potentially, the increased risk of cardiovascular morbidity (cardiovagal dysfunction; see below for further discussion). 1 Future studies are required to address the relationship between neurological level of injury and the particular autonomic domains affected, because our standard methods of SCI classification with ISNCSCI do not adequately capture the complexity of the autonomic lesion. Also, the clinical implications of particular autonomic deficits require further characterization.
SSRs are commonly used to understand the relationship between neurological level of injury, autonomic injury, and cardiovascular dysfunction (typically the presence of OH or autonomic dysreflexia). 13,21,24 SSRs have been postulated to represent the integrity of the entire sympathetic pathway, attributed to the close anatomical relationship between sympathetic cholinergic and adrenergic fibers. 25 They have been shown to be reliable and predictive of cardiovascular dysfunction in SCI, when characterized qualitatively (specifically the presence vs. absence of response). 11,26 Our study results highlight the concept that generalizations about multi-domain autonomic impairment cannot be made based on the presence or absence of SSRs alone, and that a standardized autonomic battery would be more useful in assessing the integrity of the entire autonomic system.
Another significant finding of this study was impairment in cardiovagal function (HRDB and VR) in SCI participants, which was identified through comparisons to healthy controls and normative cutoffs for HRDB (9 of 10 participants). 18 The finding of cardiovagal impairment is not uniform across the literature however, with many studies reporting no difference in cardiovagal parameters between SCI participants and healthy controls. 13,27 –29 Studies of cardiovagal function in the SCI population have used spontaneous HR variability spectral analysis. This technique has been criticized, given that it may not reflect cardiovagal responses to perturbations during daily activities. 30 The noninvasive techniques used in the present study cause perturbations in the baroreflex. HRDB and VR are both straightforward tests, with clearly defined cutoffs for abnormality. 18 HRDB in particular, which is a pure test of cardiovagal function (as opposed to VR, which reflects both cardiovagal and sympathetic adrenergic effects on the heart), 16 was significantly impaired in our participants.
The significance of cardiovagal dysfunction in SCI is unclear. Reduced cardiovagal sensitivity is unlikely to contribute to orthostasis, given that the HR response to orthostatic stress has not been shown to compensate for reductions in BP. 27 Chronic cardiovagal dysfunction in other disease populations has been shown to be predictive of cardiovascular morbidity and mortality. 14,31 It is well established that chronic SCI is associated with increased risk of negative cardiovascular outcomes, 3 and it is possible that cardiovagal dysfunction is, at least in part, responsible. In this regard, measurement of cardiovagal function as part of an autonomic battery could be useful in identifying SCI patients at risk for cardiovascular dysfunction; however, this concept requires further study.
Participants in our study demonstrated significant reductions in SBP, with preservation of HR responses, compared to healthy controls, consistent with sympathetic adrenergic dysfunction on HUT. This is consistent with the results of Houtman and colleagues 32 who demonstrated a lack of increase in sympathetic adrenergic activity (reflected by the low-frequency domain of BP variability) on HUT in tertra- and paraplegics, compared to able-bodied controls. The SBP response to VM, as a noninvasive measure of sympathetic adrenergic function, may provide robust information about the integrity of the entire sympathetic pathway when used in conjunction to SSRs. VM provides rapid, safe assessment of the integrity of sympathetic pathways and can be performed at the bedside with minimal equipment. 16 BP response to VM can be assessed quantitatively, through calculation of parasympathetic and sympathetic adrenergic components of baroreflex sensitivity, 33 or through qualitative analysis of the waveform morphology, particularly the sympathetic adrenergic-mediated phases (Phase II Late and Phase IV). 22 Previous studies in SCI participants reported abnormalities in the SBP waveform during VM 12,28,34 ; however, the criteria used to define abnormality are variable. Palamarchuk and colleagues 22 demonstrated a characteristic “V” pattern of the BP response to VM in participants with neurogenic OH secondary to variety of central nervous system disorders causing autonomic failure. The appearance of a “V” pattern is the result of a prolonged and exaggerated dip in SBP during Phase II, followed by a syncline resulting from an absence of Phase II Late and a prolonged or indefinite Phase III. The absence of Phase II Late and Phase IV Overshoot are associated with sympathetic adrenergic failure, because they reflect alpha- and beta-mediated vasoconstriction in response to baroreceptor-detected reductions in central venous return, respectively. 16,18 Similarly, the participants in our study demonstrated a concordance between morphology of the response to be VM and hemodynamic response to HUT. Seven participants with a “V” pattern response met the criteria for OH on HUT, whereas 2 participants with normal VM morphology (“M” pattern, which included sympathetic adrenergic-mediated Phase II Late and Phase IV), were able to adequately maintain hemodynamic stability during HUT. Only 1 participant (subject 1) demonstrated discordance between VM and HUT, with “V” pattern response to VM and relative hemodynamic stability during HUT. In this regard, VM may expand on HUT by revealing milder forms of sympathetic adrenergic dysfunction. 35
Limitations
It is important to note that SSRs are not part of the battery of tests routinely used in sudomotor assessment as described by Low and others. 16,18 QSART measures the integrity of the sympathetic cholinergic post-ganglionic reflex pathway. We did not use QSART in this study, because there is no anatomical justification for this part of the pathway to be affected in SCI.
A second limitation concerns the inherent lability of autonomic responses in general. It is possible that the responses of individual participants in our study could represent measurement error inherent in the autonomic tests selected. It is well known that SSRs demonstrate significant lability and habituation in many testing environments. 11 Additionally, VM in participants with presumably compromised expiratory muscle function could have affected the hemodynamic responses observed and orthostatic intolerance could have developed during the maneuver, resulting in suboptimal effort. Legg and colleagues 36 recently reported that only ∼40% of SCI participants in their study could complete an adequate VM. We recently demonstrated excellent test-retest reliability for SSRs in traumatic SCI, and we attempted to mitigate all of the technical factors that have been attributed to SSR lability. 26 The test-retest reliability of cardiovascular parameters in this study has been demonstrated in other disease populations, 37 but not in SCI. Palamarchuk and colleagues 37 demonstrated good test-retest reliability for HRDB and VR and variable reliability for quantitative parameters of the SBP response to VM. Further reliability studies of HRDB, VR, and qualitative SBP responses to VM specific to SCI are required to substantiate our study results.
Third, we did not control for standard nonpharmacological interventions for OH that are commonly used in clinical settings, in particular, the use of compression garments. This could have artificially reduced our ability to detect OH on HUT in some participants.
Finally, as with many studies in traumatic SCI, the generalizability of this study is affected by the small sample size. Because this was a single-center study, with a time-consuming protocol for participants who were concurrently undergoing intensive inpatient rehabilitation, our study sample is skewed toward motor complete participants. Further larger-scale studies using a modified ARS in this population are required to make inferences about the relationship between domains of autonomic impairment, lesion level, and duration from time of injury.
In conclusion, we demonstrated heterogeneity in the domains of autonomic function affected by the neurological injury in SCI participants, using a modified version of the ARS, originally described by Low. 16 We recommend multi-domain autonomic assessment, including sudomotor, cardiovagal, and sympathetic adrenergic tests, in order to fully characterize autonomic lesions in this population. We also demonstrated significant cardiovagal impairment; however, the clinical significance of this finding requires further elucidation. We also applied a simple, qualitative assessment of the SBP response to VM in this population, which could be useful for identification of sympathetic adrenergic dysfunction.
Footnotes
Acknowledgments
The authors are grateful to all the volunteers who participated in this study. This study was funded by the Craig H. Neilsen Foundation. A grant from the Canadian Foundation for Innovation provided support for all the data collection equipment used in this study.
Author Disclosure Statement
No competing financial interests exist.