
Abstract
The rationale for implantation of autologous human Schwann cells (SCs) in persons with subacute spinal cord injury (SCI) is based on evidence that transplanted SCs are neuroprotective, support local axonal plasticity, and are capable of myelinating axons. A Phase I clinical trial was conducted to evaluate the safety of autologous human SC transplantation into the injury epicenter of six subjects with subacute SCI. The trial was an open-label, unblinded, non-randomized, non-placebo controlled study with a dose escalation design and standard medical rehabilitation. Participants were paraplegics with neurologically complete, trauma-induced spinal lesions. Autologous SCs were cultured in vitro from a sural nerve harvested from each participant and injected into the epicenter of the spinal lesion. Outcome measures for safety were protocol compliance, feasibility, adverse events, stability of neurological level, absence of detectable mass lesion, and the emergence of clinically significant neuropathic pain or muscle spasticity no greater than expected for a natural course cohort. One year post-transplantation, there were no surgical, medical, or neurological complications to indicate that the timing or procedure for the cell transplantation was unsafe. There were no adverse events or serious adverse events related to the cell therapy. There was no evidence of additional spinal cord damage, mass lesion, or syrinx formation. We conclude that it is feasible to identify eligible candidates, appropriately obtain informed consent, perform a peripheral nerve harvest to obtain SCs within 5–30 days of injury, and perform an intra-spinal transplantation of highly purified autologous SCs within 4–7 weeks of injury.
Introduction
C
In the lesion milieu, transplanted SCs may be effective through their production of growth promoting trophic molecules, 7 their deposition of matrix molecules collagen and laminin into the extracellular space, 8 as well as their expression of surface membrane cell adhesion molecules such as NCAM and L1. 9 SCs support the re-growth of many types of axons, 3,10 –13 ensheathe and myelinate regenerating or demyelinated axons, 3,4,6,10,11,14 restore axonal conduction, 15,16 and in some cases may improve functional recovery in subacute 4,17 and chronic 5 SCI animal models. SCs can reduce secondary tissue damage, neuronal cell death, and the cavitation that occurs after contusion SCI. 4,14,17,18 After transplantation into the spinal cord lesion epicenter, SCs form a hybrid tissue that consists of SCs, fibroblasts, astrocyte cell processes, axons, and extracellular matrix. Whereas they do not repair all damage and do not migrate into intact parenchyma, they mediate their effects in the injury epicenter in this modified milieu.
In studies of contusion SCI in the rat using mitogen-expanded cells, we have shown that SC transplantation at seven days after injury significantly fosters axon regeneration and myelination, improves host tissue preservation, 4 and reduces cavitation 4,14 in a thoracic SCI paradigm and increases numbers of preserved NeuN positive neurons rostral and caudal to the injury/graft site 17 after cervical SCI. Using mitogen expanded human SCs, placed as cellular cables in SCID mice and athymic female nude rats, the human SCs survive and are capable of enhancing axonal regeneration and forming myelin after transplantation in animals with sciatic nerve transection 19,20 or thoracic spinal cord transection. 21,22
Thus, human SCs are promising candidates for transplantation into the injury epicenter of humans with SCI. Large numbers of autologous human SCs (ahSCs) can be obtained for implantation after a peripheral nerve biopsy followed by dissociation and expansion of their cell numbers in culture with mitogens. 23 Autologous cells in general offer important safety advantages over allogeneic sources that include minimal risk of disease transfer, low risk of tumorigenicity, and the absence of immunosuppressive medication requirements.
There is no direct method to extrapolate the timing of cells delivered at seven days post-injury in rodents to an equivalent time in humans; and the definition of acute, subacute, and chronic time periods in rodents versus humans is not clearly delineated. When designing a Phase I trial involving the surgical delivery of cells into the spinal cord parenchyma during the first few months after injury, however, risk must be mitigated as much as possible. The trial design described below took into account the concomitant injuries that co-occur with acute complete thoracic SCI, the need for a nerve harvest and second spinal surgery, and the need for reliable baseline data.
On the basis of this substantial body of pre-clinical data establishing the efficacy of SC transplantation into the central nervous system, and the merits of autologous preparations, a Phase 1 clinical trial was conducted to evaluate the safety and feasibility of ahSC transplantation into the injury epicenter of six subjects with subacute SCI. The trial was an open-label, unblinded, non-randomized, non–placebo-controlled study with a dose escalation design. The primary end-point was to evaluate the safety through a one year follow-up when ahSCs were administered at one of three doses within 72 days of injury to participants with complete thoracic SCI. Determining the safety of subacutely delivered SC injections into the injured spinal cord is a critical step in enabling future trials combining additional strategies with SC transplantation.
Patients and Methods
Experiment design
This trial was conducted under an IND (#14856) application filed with the Food and Drug Administration with approval by the University of Miami Institutional Review Board. The trial was registered on ClinicalTrials.gov (NCT01739023). The detailed inclusion and exclusion criteria are listed in Table 1. The primary trial center was the University of Miami/Jackson Memorial Hospital. Delray Medical Center was a recruiting site for part of the trial, undertaking screening procedures and a sural nerve harvest for one subject. Delray Medical Center activities were approved by the Western Institutional Review Board. All baseline testing, transplantation operations, and follow-up were conducted at the University of Miami/Jackson Memorial Hospital site.
CHI, closed head injury; MEP, motor evoked potential; SSEP, somatosensory evoked potential.
A two-stage informed consent design was used for this trial. Consent was obtained according to the Declaration of Helsinki for persons expected to be eligible for screening. This screening included an interview with a psychologist specialized in SCI to ensure understanding of the nature and intent of the trial. The sural nerve harvest was then performed. Participants continued their inpatient rehabilitation course during the 3–5 weeks required for cell processing. During that time, participants also received education from multiple study team members about SCI in general, about SCs, and about the clinical trial in detail. Within five days before the scheduled transplantation surgery, electrophysiology was performed to evaluate for evidence of incomplete injury using somatosensory evoked potentials and motor evoked potentials. A second informed consent was then obtained for remaining trial activities, which were baseline testing (including a second interview with the clinical psychologist), ahSC transplantation, and follow-up assessments during the first week post-transplantation, at week two, and at months two, six, and 12.
Sural nerve harvest
In the operating room, the lateral calf above the lateral malleolus was infiltrated with local anesthetic with 1% epinephrine. The sural nerve was identified and an approximately 15 cm segment was harvested for ahSC preparation by sharp dissection.
Cell processing
The sural nerve was dissected, and fascicles were pulled from the epineurium and transferred to a triangular T-75 flask (Corning, Oneonta, NY) and placed in an incubator at 37°C with 8% CO2. Culture medium, which contained 1 × Dulbecco modified Eagle medium (Life Technologies, Grand Island, NY), 10% fetal bovine serum (Hyclone, GE Healthcare Life Sciences, South Logan, UT), 2 mM forskolin (Sigma-Aldrich, St. Louis, MO), 10 nM human recombinant heregulin β1 (Genentech, South San Francisco, CA), 4 mM
On day seven ± two, the dissociation enzyme solution that contained neutral protease NB (2 DMCU/mL; SERVA Electrophoresis GmbH, Heidelberg, Germany), collagenase NB1 (0.5 PZU/mL; SERVA Electrophoresis GmbH) in 1 × high-glucose Dulbecco modified Eagle medium (Life Technologies) supplemented with 3.1 mM CaCl2 (International Medication Systems Limited, South El Monte, CA) was added to the fascicles and placed inside the incubator overnight. The fascicles were dissociated, D-10 (Life Technologies) (10 mL) was added to a tube containing the fascicles, which was centrifuged at 150 × g for 5 min at 4°C to pellet the cells. The cells were washed and plated onto mouse laminin-coated (1 μL/cm2, with a stock concentration of 1 mg/mL; Sigma-Aldrich) plates using the culture medium, then fed with culture medium every three days. After 7 days, cells generally reached 80–90% confluence. The viable cell counts of final harvests before the transplantation ranged between 11.4 and 436.8 million cells for all six products.
During the trial, the cell processing techniques were optimized to yield higher cell recovery rates; hence, the wide range of viable cells. These modifications were tested and validated before being implemented into the trial; they led to the routine yield of more than 200 million SCs. The SCs purity by immune staining ranged from 92.2–98.7% (Fig.1A–G) and the SCs viability also ranged from 93.2–97.2%. The final cell products were washed to remove mitogens, laminin, and bovine products. Several controls were employed throughout the manufacturing process to ensure that the product was essentially free of process-related contaminants, including the wash steps described above and release testing of the final product. Mycoplasma (via polymerase chain reaction [PCR]) testing was negative for all six ahSC products infused; final endotoxin levels were less than 0.2 EU/kg; Gram stains were negative. Post-transplantation sterility results after 14 days of culture were also negative for aerobic, anaerobic, and fungal organisms.
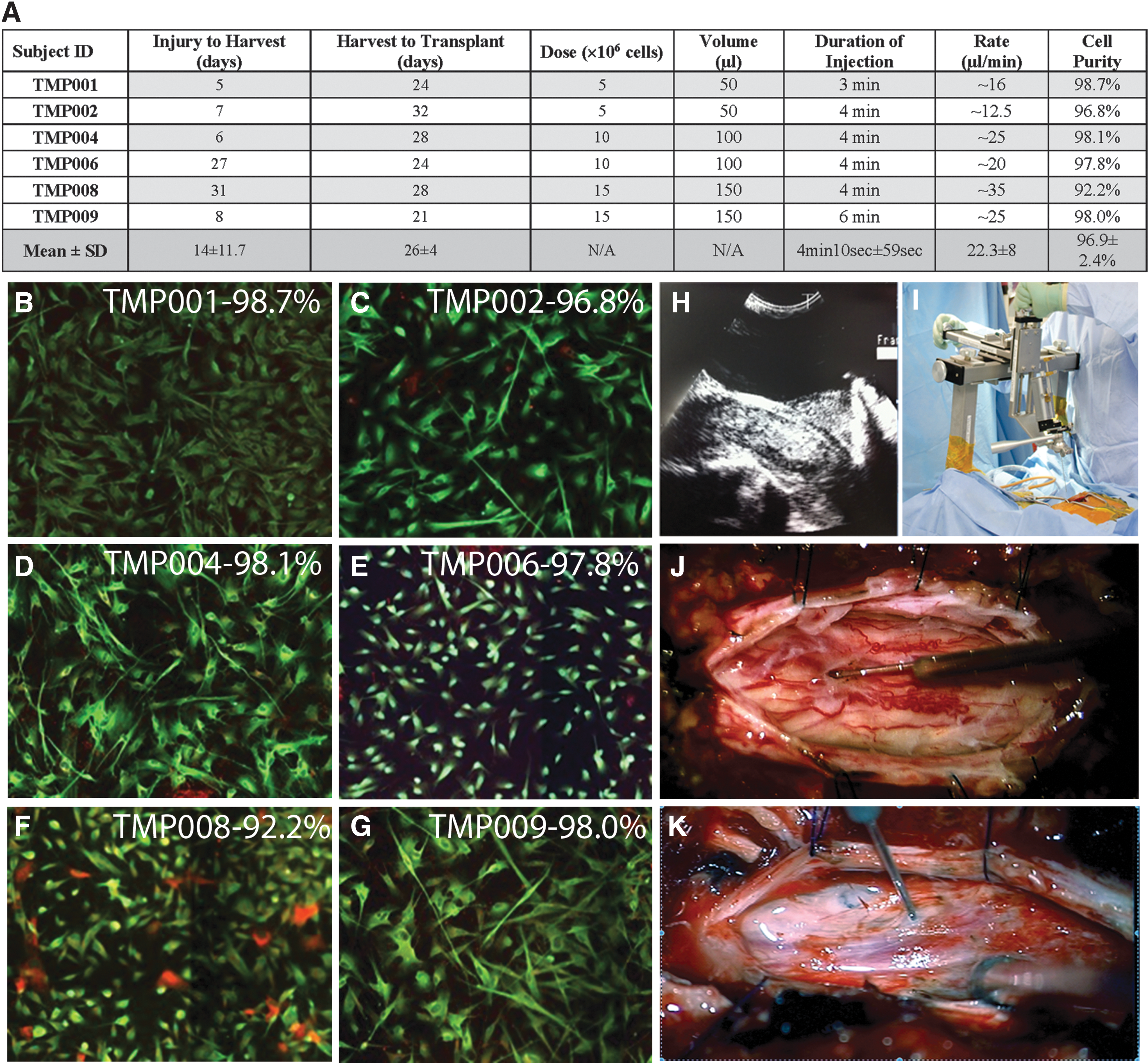
Transplantation information per subject. (
For immunostaining, SCs were plated onto laminin-coated four-well glass chamber slides at 50,000 viable cells per well and fixed the following day with 4% paraformaldehyde (Electron Microscopy Sciences, Hatfield, PA). For identification of SCs, an anti-human S100 (final dilution 1:200; Dako, Dallas, TX) primary antibody was used. Within the peripheral nerve tissue, SCs are the only cell type that expresses S100 protein. To identify the second major cell type that is a constituent in the nerve dissociate, we used an antibody that recognizes fibronectin, which is abundantly present in fibroblast extra-cellular matrix; an anti-fibronectin (final dilution 1:200; Santa Cruz Biotechnology, Santa Cruz, CA) primary antibody was used. The secondary antibodies used were a solution combination of Alexa 488 goat anti-rabbit IgG and Alexa 594 goat anti-mouse IgG (Life Technologies) diluted (1:200) in 1.5% normal goat serum and 1 × DPBS (Life Technologies). All wells received Hoechst nuclear marker (final dilution 1:1,000; Life Technologies). Fluorescent images were obtained using a fluorescent microscope.
Dose escalation was performed in three cohorts with the first cohort receiving 5 million cells in 50 μL, the second cohort receiving 10 million cells in 100 μL, and the third cohort receiving 15 million cells in 150 μL. The dose to be administered and backup aliquots of cells were placed on ice to transport to the operating room for transplantation.
Intra-medullary injection of ahSCs
After induction of general anesthesia and intubation, the subjects were placed in the prone position on a Jackson table (Mizuhosi OSI, Union City) (
Previously, all patients had undergone decompressive laminectomy and/or spinal re-alignment and instrumented fusion after injury. A priori, surgical planning for stabilizing instrumentation was performed to avoid placing pedicle screws and cross-link at the site of injury epicenter to avoid instrumentation artifact during MRI. The middle portion of the previous midline skin incision was re-opened to expose the surgical transplantation site. Sharp dissection of very adherent scar tissue down to the dura was needed in all patients. Additional partial laminectomy above or below the injury site was needed in a few patients to obtain appropriate dural exposure at the transplantation site. The injections were performed with maintenance of the posterior spinal instrumentation in place.
Intra-operative ultrasonographic imaging (Hitachi HI Vision Ascendus, Hitachi Medical Systems Europe Holding AG, Switzerland/12 MHz linear array transducer on an IU22 scanner ([Aloka Medical America, Inc, Wallingford, CT]) was used to visualize intra-medullary changes, especially cystic cavities (Fig. 1H). This information was used in addition to estimation of the borders of the traumatic lesion based on the extent of the altered intra-medullary signal changes on T1 and/or T2 images that are typical of SCI. According to the ultrasound and MRI findings, the extent of the dural opening was determined. Dural tackup sutures were placed. Using the magnification and illumination of the operating microscopic, the dorsal surface anatomy was exposed. Extensive untethering or fenestration of a spinal cord cyst was avoided. The table-mounted syringe positioning device designed by Geron Corp. was anchored to the operating table in a sterile fashion (Fig. 1I) and its components assembled.
Special care was taken to avoid damaging superficial blood vessels (Fig. 1J,K). The ahSC dose was pre-determined according to the escalation parameters. Gentle swirling and tapping of the vial was required to disperse the cells before syringe loading. A commercially available 250 μL Hamilton syringe with 10 μL marks was used to draw up and deliver the cells through a 26S-gauge needle tip. The syringe was mounted into the syringe positioning device and lowered into proximity of the target injection site. Apnea was invoked to reduce spinal cord excursions because of ventilation, with continuous infusion of 100% oxygen through the endotracheal tube to maintain oxygen saturation of the blood (see Supplementary Table 1; see online supplementary material at
Using the syringe positioning device microstage and depth adjustment, the injection needle was advanced to the pial surface and a small pial opening created with a tip of a #11 blade to prevent cord compression during needle insertion. The needle was then carefully inserted perpendicular to the pial surface until the tip reached the desired depth calculated based on the pre-operative MRI and intra-operative ultrasonography. The site targeted for injection was the injury epicenter—most commonly 3–4 mm below the pial surface. The cells were infused over approximately 4 min (Fig. 1A), followed by an additional 1 min dwell time to avoid reflux of cells along the needle tract. On withdrawal of the needle, special attention was given to the pial surface to document cell reflux from the needle tract. After the intra-medullary injections, the dura was closed in a watertight fashion with 5-0 Prolene sutures, ultrasonography was repeated, and the dura covered with Duragen Plus (Integra, Plainsboro, NJ).
Primary end-points for safety
Primary outcome measures for safety were protocol compliance, feasibility, adverse events (AEs), and stability of neurologic level. Compliance and feasibility were chosen because of the complexity of the protocol, particularly related to the need for two surgical procedures in the subacute period in addition to the primary decompression and fixation operation. Evaluation of AEs is a key indicator of safety. Stability of the neurologic level was chosen because of the plan to inject cells into the epicenter of the subacute lesion and the possibility of interference with the evolving spinal cord cavitation or resolving inflammatory process that might lead to neurologic deterioration. Deviations from the protocol were documented to monitor compliance and feasibility. All AEs and serious adverse events (SAEs) were recorded and a determination of relatedness to ahSCs was made. To document neurologic change, the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) was used along with the AIS grading of completeness. 24
Secondary end-points for safety
Secondary outcome measures for safety were absence of detectable mass lesion on MRI, the emergence of clinically significant neuropathic pain no greater than expected for a natural course cohort, and emergence of clinically significant muscle spasticity no greater than expected for a natural course cohort. Absence of detectable mass lesion was chosen because cell therapies in general carry the inherent risk of tumorigenesis, even though human SCs themselves carry a very low risk. Pain and spasticity were chosen as secondary safety end-points because of the possibility that they could be impacted negatively by aberrant neuroplasticity.
MRI scans of the thoracic spine without and with gadolinium were performed on a Siemens 1.5T magnet using metal artifact reduction sequences to limit instrumentation artifact. MR imaging was generally performed immediately post-injury, one to two days before transplantation (baseline), day one and months six and 12 post-transplantation. Lesion volume was determined by using the free hand measurement tool on axial images to calculate the area of signal abnormality multiplied by the cut thickness. Pain was assessed using a combination of a pain drawing, the International SCI Basic Pain Dataset, 25 and the Neuropathic Pain Symptom Inventory. 26 Spasticity was evaluated in the hamstrings and quadriceps using the Modified Ashworth Scale. 27
Exploratory domains for efficacy
Although the primary end-point for this trial was safety, we wanted to evaluate multiple domains for preliminary indicators of efficacy. We chose measures recommended by the SCI field or commonly used clinically for assessment of functional ability related to activities of daily living, subclinical neurologic connectivity, bladder and bowel control, and participant impression of change. Functional ability was measured with the Spinal Cord Independence Measure version III 28 and the Functional Independence Measure.® To evaluate the burden of injuries sustained during the initial trauma the Injury Severity Score 29 was calculated. Electrophysiology measures of somatosensory and motor evoked potentials were performed as a secondary evaluation of neurological connectivity and sympathetic skin response as an evaluation of autonomic neurological connectivity. Bladder and bowel control was evaluated with the International SCI Lower Urinary Tract Basic Dataset 30 and the International SCI Bowel Function Basic Dataset. 31 The Patient Global Impression of Change was used to rate participant impression of change after enrollment.
Statistical analysis
As an open label study lacking a control group, statistical analysis is limited other than for the independent variable of cell dose. The primary end-point analyses occurred at 12 months post-transplantation. All analyses were based on descriptive measures of the cohort and within-subject changes.
Results
Participants
Between November 2012 and July 2015, we pre-screened 39 persons who we suspected might qualify for the trial. Nine of those persons were enrolled and six received ahSC transplantation. A CONSORT diagram is included in Supplementary Fig. 1; see online supplementary material at
AIS = American Spinal Injury Association (ASIA) Impairment Scale; ID = identification; ATV = all-terrain vehicle; MVA = motor vehicle accident.
ahSC culture and transplantation
The mean (all data to follow presented as mean ± standard deviation) number of days between injury and nerve harvest was 14 ± 11.7 (Fig. 1A). The length of sural nerve harvested was 15.9 ± 4.0 cm. The number of days between nerve harvest and transplantation surgery was 26 ± 4.0 (Fig. 1A). Transplantations occurred an average of 40 ± 12.3 days post-injury. High SC purity at product release was obtained for all transplantations (Fig. 1 A–G) with the mean being 96.9 ± 2.4%. After meticulous removal of the scar, intra-operative ultrasonography (Fig. 1H) was used to define the epicenter of the injury, the dura was opened, and the syringe positioning device was set up (Fig. 1J,K). Apnea was induced, mean duration 6 min 12 sec ±30.0 sec, (see Supplementary Table 1; see online supplementary material at
In five of the six patients, ahSC efflux from the injection site after needle removal was of minimal volume, which was observed under the surgical microscope at high magnification and adsorbed onto cottonoid patties. In one subject, a larger volume of efflux was observed early during the injection, and the injection was stopped for 30 sec to adsorb the efflux, the needle was deepened by 1 mm, and injection resumed. No cells were delivered into the intra-thecal space. Each syringe was pre-loaded with the dose to be delivered plus an extra 30 μL of cell suspension to enable adjustment for any efflux volumes.
In regard to induced apnea during cell injection, durations of up to 6 min 45 sec were well tolerated with suitable pre-oxygenation and initial CO2 levels in the low-normal range (see Supplementary Table 1; see online supplementary material at
Primary evaluation of safety
The AEs were recorded from the time of enrollment through 12 months post-transplantation. Figure 2A shows the cumulative number of AEs for all six transplanted participants categorized by body system. The AEs were those reasonably expected for a trial enrolling participants shortly after a traumatic injury. Notably, there were no occurrences of deep vein thromboses, pulmonary emboli, meningitis, or pseudomeningoceles. Figure 2B shows the number of AEs for all participants across time beginning with the baseline assessment pre-transplantation. The shaded area indicates the time window during which five of the six participants were discharged from their inpatient rehabilitation setting. One subject, TMP008, sustained significant poly-trauma with his injury and was not discharged from the acute hospital setting until just before 9 months post-transplantation. He also experienced the most AEs—21.
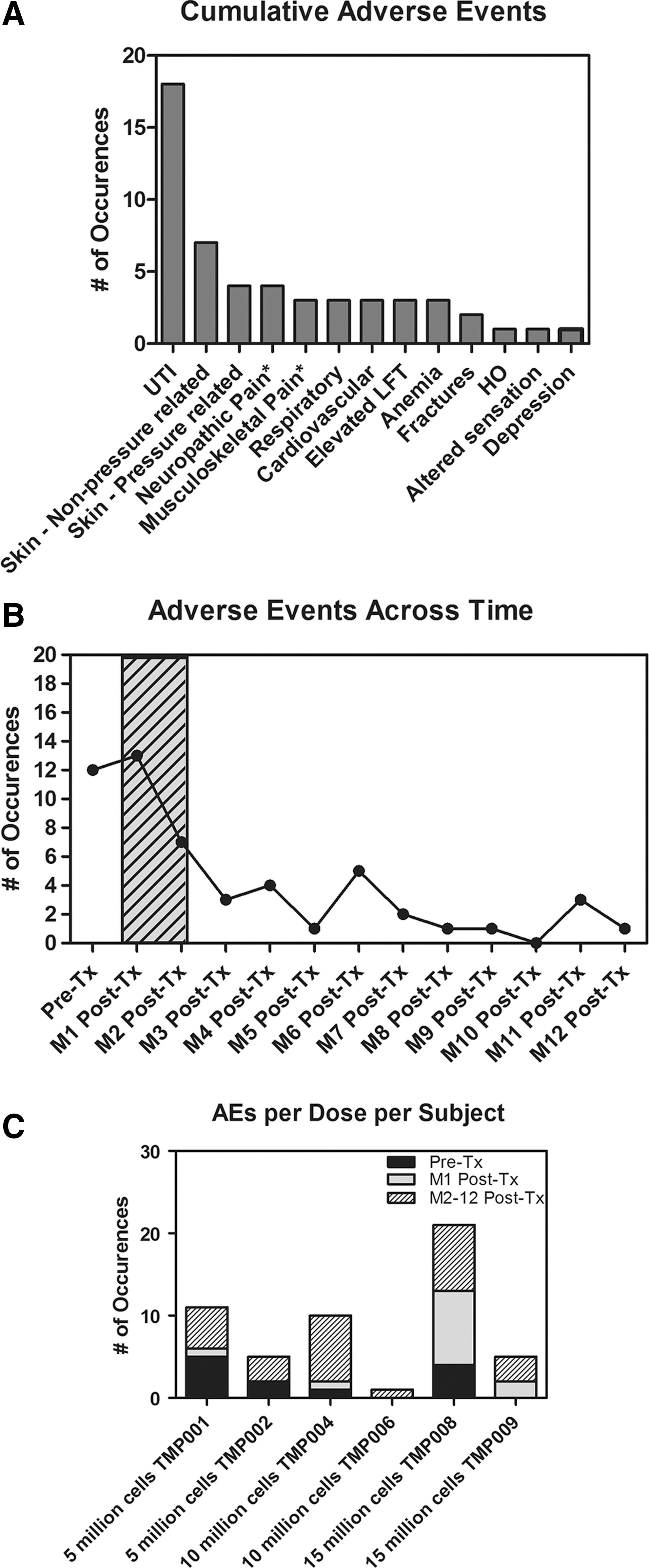
Adverse events (AEs). (
Figure 2C shows the number of AEs experienced per participant dependent on dose. See Supplementary Table 2 (see online supplementary material at
The ISNCSCI and AIS were used to evaluate neurologic changes. Figure 3 shows diagrams of normal and impaired dermatomes and myotomes for each participant at baseline as well as at month 12 post-transplantation (created using the
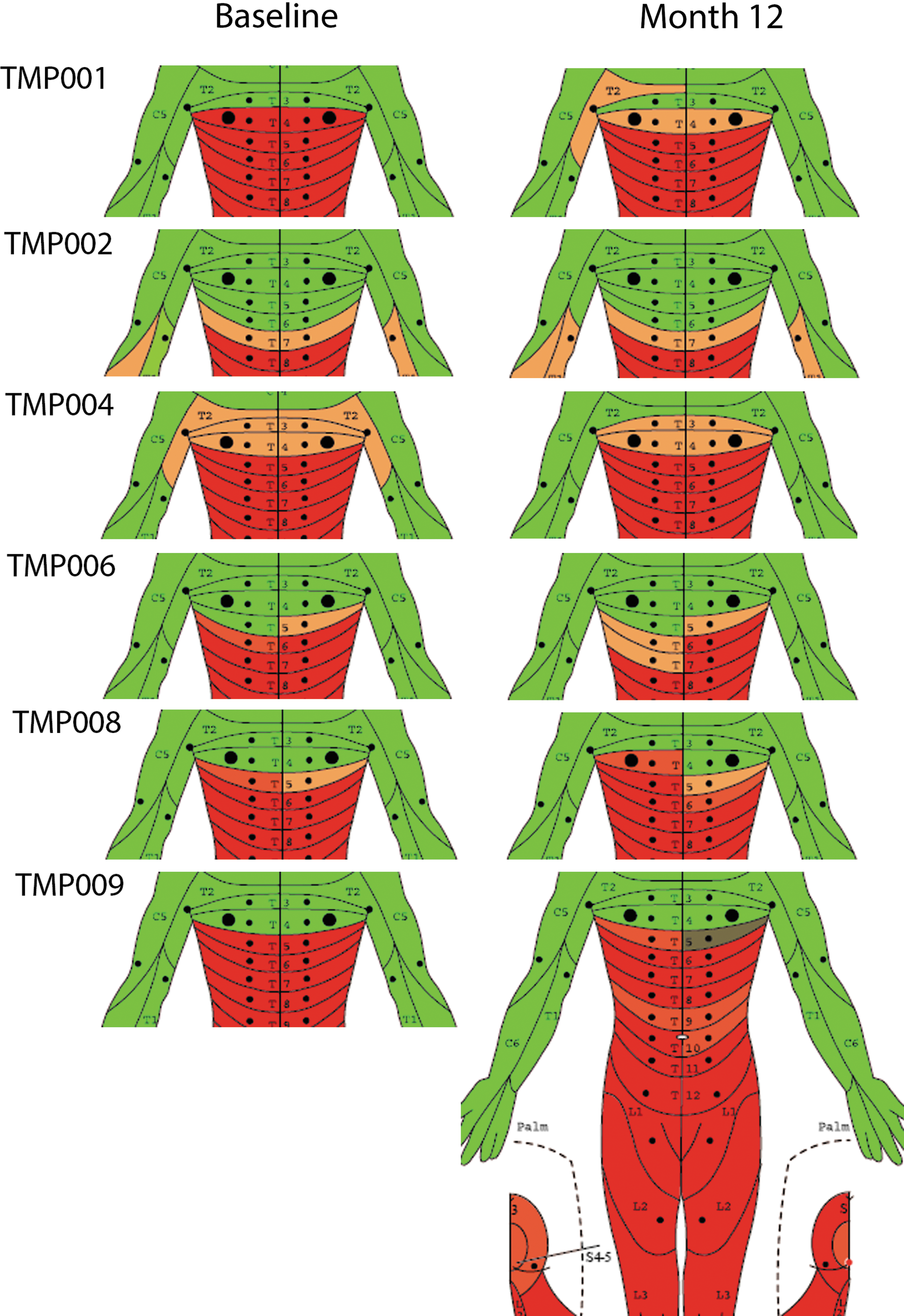
International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) pre-transplantation (baseline) and at month 12. Baseline and month 12 ISNCSCI diagrams for each subject. Green represents normal motor and/or sensation, red represents absent motor and/or sensation, orange and light red shaded areas represent sensation that is present but abnormal.
Specifically, TMP001 gained two sensory points from baseline, but lost two levels per the single neurologic level (SNL) because of the altered sensation described above; the zone of partial preservation (ZPP) descended 1 level. TMP002 lost three sensory points, but there was no change in SNL or ZPP. TMP004 gained two sensory points, and the SNL descended one level within the ZPP. TMP006 gained two sensory points, had no change in the SNL, but the ZPP descended one level. TMP008 lost three sensory points, and the SNL ascended one level, but the ZPP descended one level. The most change was observed in TMP009. At six months post-transplantation. he converted from an AIS Grade A to B, which persisted at month 12. He gained nine sensory points by month 12, but his SNL did not change.
Secondary evaluation of safety
The MRI at baseline demonstrated significant variability in intra-medullary post-traumatic changes; lesion length varied from 2.5–7.6 cm with a mean of 5.6 ± 2.1 cm, and lesion volume varied from 0.8–4.1 cc with a mean of 2.3 ± 1.2 cc (Fig. 4). Whereas spinal cord transection was an exclusion, the degree of cord damage was severe, and there were no limits set on lesion size. Lesion characteristics were at times obscured by the presence of instrumentation despite a priori surgical planning. In some cases, it was difficult to distinguish structural injury versus peri-injury edema. The spinal cord was well decompressed at the time of the ahSC transplantation in all but one patient in whom there was an epidural fluid collection (TMP002).
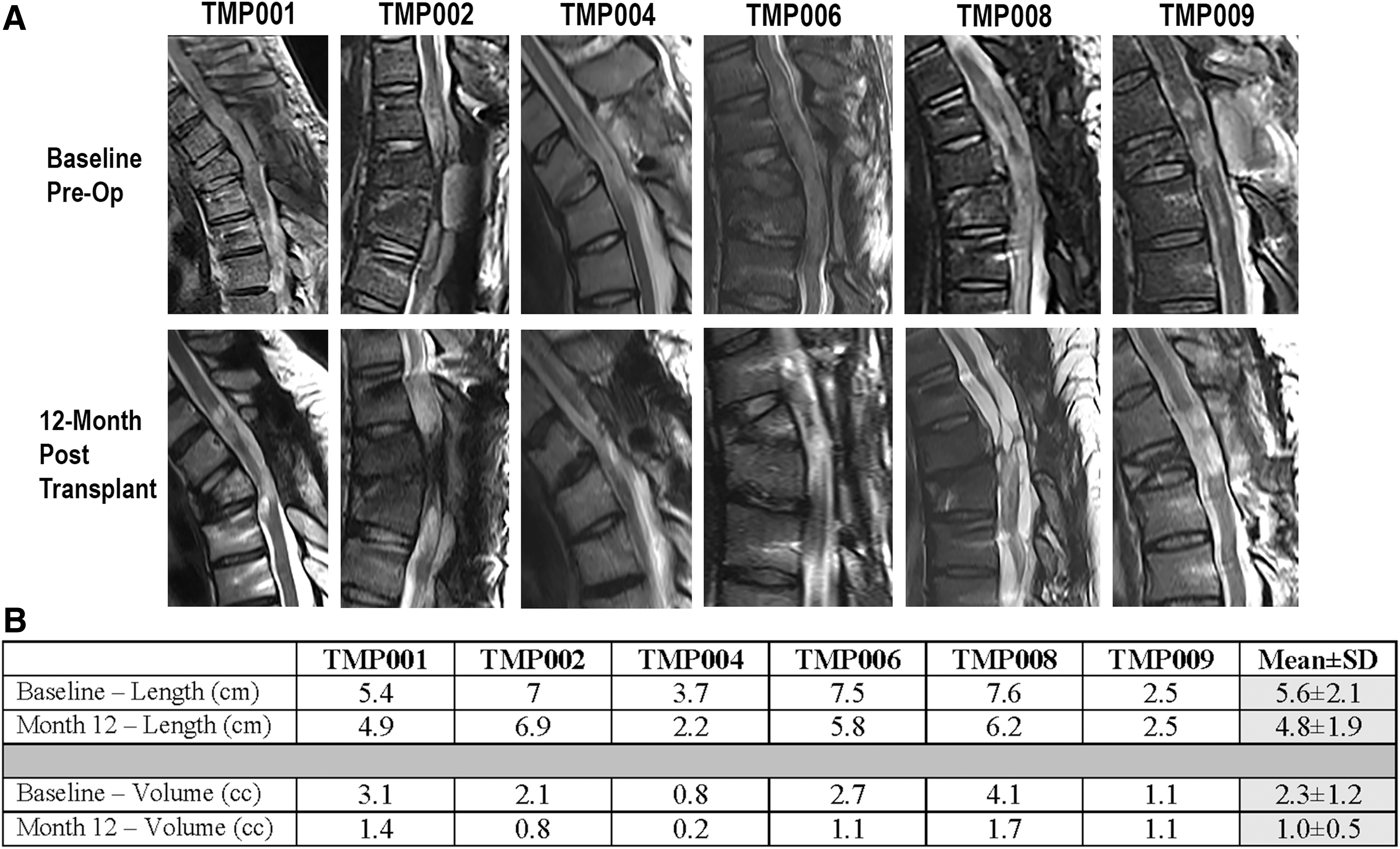
Magnetic resonance imaging (MRI) of lesions. (A) Sagittal T2-weighted images performed at baseline in all six subjects with sub-acute SCI before Schwann cell transplantation. Baseline MRI performed from 24–57 days post-injury. Twelve month post-transplantation MRI demonstrates spinal cord myelomalacia and areas of cystic change in some participants. (
Participants were re-scanned on day 1 post-transplantation. Whereas small post-operative fluid collections were seen at the revision laminectomy site, there were no areas suggestive of intra-medullary hemorrhage resulting from the cellular injection, independent of the dose. On the 12 month MRI scan, there was atrophy of the spinal cord (Fig. 4). In one patient (TMP008), there was atrophy and focal tethering of the spinal cord. Lesion length at 12 months varied from 2.2–6.9 cm with a mean of 4.8 ± 1.9 cm. Lesion volume at 12 months varied from 0.8–1.7 cc with a mean of 1.0 ± 0.5 cc. Lesion length and volume were significantly different between baseline and 12 months post-transplantation. For lesion length, using an unpaired two-sided t-test, the p value was 0.008 (Graphpad Instat 3.01). For lesion volume, using the same statistical comparison, the p value was 0.034.
Pain was monitored as a secondary outcome measure of safety. Figure 5 shows the distribution of musculoskeletal (blue), neuropathic (red), and mixed musculoskeletal/neuropathic (purple) pains for each participant. Three participants did not experience neuropathic pain either at pre-transplantation or at 12 months post-transplantation (Fig. 5A,C,D). Two participants experienced neuropathic pain at pre-transplantation, which had increased in severity at 12 months post-transplantation (Fig. 5B,F). One participant did not experience neuropathic pain at baseline but had developed neuropathic pain at 12 months post-transplantation (Fig. 5E). The neuropathic pains that were experienced by three persons at 12 months post-transplantation were severe and interfered with various life activities (see Supplementary Table 3 for detailed pain data and narrative descriptions of each participant's pain pre-transplantation and at 12 months post-transplantation; see online supplementary material at
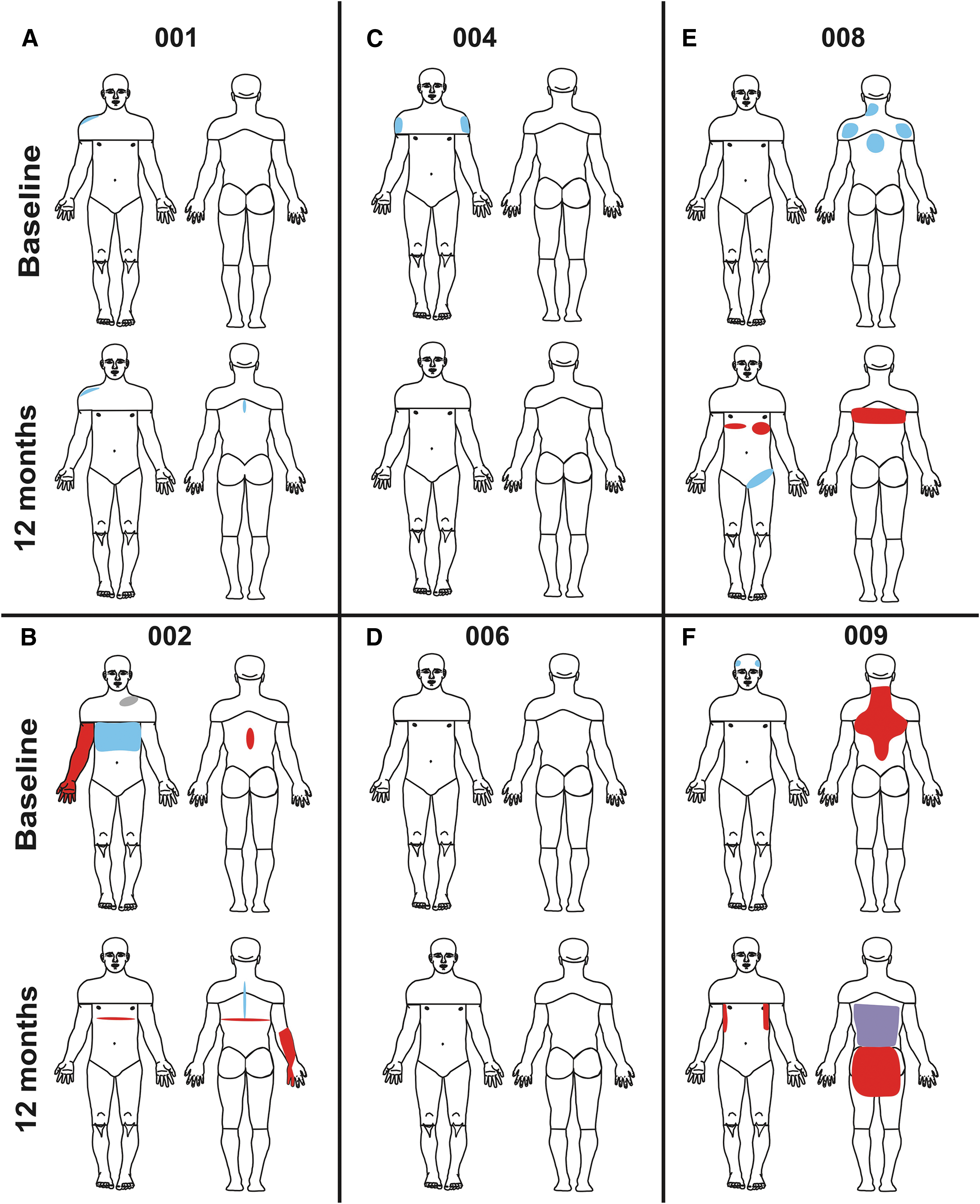
Pain drawings pre-transplantation (baseline) and at month 12. (
MAS = Modified Ashworth Scale; ISS = Injury Severity Score associated with initial trauma; FIM = Functional Independence Measure; SCIM III = Spinal Cord Independence Measure version III; MEP = motor evoked potentials; EMG = electromyography; R = Right; L = Left; PGIC = Patient Global Impression of Change; P = Present; A = Absent; P* = Present under facilitation.
Exploratory evaluation of efficacy
Functional recovery as measured by the Functional Independence Measure® and the Spinal Cord Independence Measure III occurred as would be expected (Table 3, columns labeled as “FIM” and “SCIM III”), but was influenced by the severity of the associated trauma sustained during the initial injury. The Injury Severity Score (ISS) ranges 0–75 with 25 being considered severe and 75 being considered unsurvivable; it was used to evaluate the initial burden of trauma. We calculated that the presence of a severe thoracic SCI automatically accounted for an ISS of 16 (Table 3, column labeled “ISS”). TMP001 also sustained a rotator cuff injury and wrist fracture, which increased his ISS to 20. TMP002 sustained a significant brachial plexus injury along with scapula, clavicle, and rib fractures, which increased his ISS to 24. TMP008 sustained three fractures (femur, scapula, and thumb) and significant chest trauma (hemothorax, respiratory failure, pulmonary contusions), which generated an ISS of 34. The higher burden of injury in these three participants is reflected by their lower functional ability scores at baseline (Table 3, columns labeled as “FIM” and “SCIM III”).
A detailed analysis of electrophysiological findings will appear in a separate report, but in no subject was a consistent reproducible somatosensory evoked potential waveform observed. Baseline electrophysiology was performed within five days before transplantation and again at two, six, and 12 months post-transplantation. The subject that converted to AIS B (TMP009) had detectable motor evoked potentials in both legs at both six and 12 months, and three subjects were able to voluntarily activate electromyography signal in the legs (Table 3, columns labeled “MEP” and “EMG in legs”) when a Jendrassick maneuver was performed. All of this activity was below the level of clinical detection; i.e., in 0/5 scored muscles. The detection of sympathetic skin responses was complicated in subjects receiving anti-cholinergic medications because sweating was blocked pharmacologically via concomitant medication (data not shown). Bladder and bowel control did not change (data not shown). All participants rated their overall global impression of change as having improved by some degree at 12 months post-transplantation (Table 3, column labeled “PGIC”), although this could also be expected to occur in untreated persons during the first year post-injury.
Rehabilitation in this trial was per standard medical care; activities were not prescribed by the trial. As such, standard medical rehabilitation is designed unique to the individual and injury. In general, however, inpatient rehabilitation consisted of a therapy program involving three hours each day, five days each week based on the individual's injury, rate of progress, and therapeutic milestones set by the clinical rehabilitation team. The six participants received an average of 6.6 ± 2.1 (standard deviation) weeks of inpatient rehabilitation.
Discussion
This study of six subjects transplanted with autologous purified SCs, evaluated for one year, showed no clear indication of adverse events specifically linked to the nerve harvest, cell transplantation procedure, or presence of the cells within the spinal cord. It is feasible to identify, appropriately obtain informed consent, perform a peripheral nerve harvest within 5–30 days of injury, and introduce an intra-spinal transplantation within 4–7 weeks of injury, even in persons who have sustained severe injury.
An initial time window of five days post-injury was set as a cutoff for the nerve harvest and 42 days post-injury as a cutoff for the ahSC transplantation in an attempt to maximize the potential neuroprotective properties of SCs while working within the required time for cell processing. The five-day time window, however, proved to be difficult when trying to recruit participants within the context of the strict inclusion and exclusion criteria and in using a single center enrollment site.
Approximately one year into the trial, approval was obtained to extend the cutoff for nerve harvest to seven days post-injury while maintaining the 42-day post-injury cutoff for the transplantation. At the same time, the age cutoff was extended to 60 years from 50, and the upper and lower limits of the liver functioning tests were removed from being exclusionary criteria. Extension of the age range to 60 years was determined to not impose any additional risk because (1) persons with significant health concerns would be excluded by the other criteria and (2) negative effects of age (independent of health status) on co-morbidities after SCI are more frequent in elderly persons—i.e. >60 years of age. 33,34
In addition, it is not uncommon for persons having sustained an acute traumatic injury, like SCI, to have some laboratory values outside of the typically accepted ranges. 35,36 Our first two participants both had laboratory values for their liver function tests outside of the ranges initially listed in our criteria, yet the values were not ones that would raise safety concerns for the transplantation procedure. Approximately six months later, we extended the window for the nerve harvest to 30 days post-injury and the transplantation to 72 days post-injury and added a second site for recruitment and screening procedures.
Several logistics regarding trial design were made clear as a result of this experience. The transfer and transportation of patients between medical centers during the first week post-injury (acute stage of medical care) is challenging and can impact recruitment negatively. That impact is compounded when recruitment is restricted to a single site, as is often the case for Phase I trials. It is also compounded when trying to recruit from a small subpopulation; T3-T11 AIS A injuries comprise approximately 18% of traumatic spinal injuries in the United States. 37 By extending the enrollment window into the subacute period, many of these barriers can be overcome, facilitating transfer logistics. The longer time window also allows acute injury co-factors such as mild head injury and liver injury to resolve, which would otherwise be criteria for exclusion. There is also more time to educate the patient and his or her family about the trial. Hence, we conclude that administration of cell therapies in the subacute period is feasible and worth pursuing.
The changes in neurological function after transplantation were not clinically meaningful in five of six subjects, but this may reflect the severity of the enrolled thoracic SCIs, as demonstrated by the large lesion sizes, and the relative low number of transplanted SCs. Very few persons with thoracic AIS A injuries will spontaneously convert to incomplete grades. 38 One of the six subjects in this trial converted to AIS B. This represents approximately 16% of participants, which falls within the expected 18% rate of spontaneous conversion. 38
It is also common to observe minor gains or losses in sensory levels as well as the single neurological level in thoracic injury, most often limited to one segment. 38 A deterioration of three or more thoracic sensory levels would be unusual and has been suggested as a marker to track safety in Phase I clinical trials targeting acute/subacute SCI. 38 None of the six subjects who underwent transplantation experienced a loss of three levels. In addition, none of the subjects experienced any neurological or functional deterioration during the first days or weeks after the transplantation.
Autologous cells were selected to preclude a need for immunosuppression. In allogeneic studies of cell transplantation for SCI, many questions remain about the necessary dose, duration, and the number of immunosuppressive drugs needed. The cell population was purified toward being predominantly SCs to minimize the fibroblast component. Although we do not know the optimal ratio of different cell types in nerve-derived transplantation products intended for the injured spinal cord, it is anticipated that a high fraction of fibroblasts may contribute to more robust scar formation.
The necessity of having a well-characterized cell population is a critical component of safety. Cells with the ability to proliferate extensively carry the inherent risk of tumor formation after transplantation. As such, pre-clinical experiments analyzing the tumorigenicity of a cell population are critical safety assessments that should be performed as part of the data portfolio supporting a proposed clinical trial. They were required by the Food and Drug Administration as part of the Investigational New Drug application for the use of ahSCs in SCI. Recent reports have been published documenting tumor formation in persons who received uncharacterized cell transplantations under “stem-cell tourism” settings. Dlouhy and colleagues 39 described an autograft-derived spinal cord mass from an olfactory mucosal cell transplantation in a person with a lower thoracic SCI. This mass was identified eight years after the transplantation. Berkowitz and colleagues 40 described a glioproliferative lesion in the spinal cord and thecal sac of a person who had received multiple intra-thecal infusions of mesenchymal, embryonic, and fetal neural stem cells. In our pre-clinical testing of SC transplantation we did not find evidence of tumor formation in rodents, pigs, or primates. As an extra precaution, we plan to monitor all of our ahSC recipients for five years after the transplantation.
Whereas SCs promote axonal growth and axonal myelination, their release of neurotrophic factors, prostaglandins, and cytokines can also activate and sensitize nociceptors and modulate sensory neuron gene expressions leading to neuropathic pain. 41 One of our safety concerns, therefore, was the possibility of development of neuropathic pain induced by the cell transplantation or by associated inflammation.
Persistent and severe pain is common after SCI, 42,43 with approximately 60% experiencing neuropathic pain within one year post-SCI. 32 Consistent with the natural course of neuropathic pain development after SCI, three to four of our six participants would be expected to experience neuropathic pain at one year post-injury. In the present study, three subjects experienced neuropathic pain at 12 months post-SCI. Thus, the ahSC implant was associated with neuropathic pain within expected frequency without any attenuation of the neuropathic evolution. Based on these data, it appears that a cause and effect relationship between subacute ahSC implants and the development or attenuation of neuropathic pain 12 months post-SCI cannot be determined.
Subjects who sustain complete thoracic SCI tend to experience a high degree of force as occurs in motorcycle, all-terrain vehicle, and motor vehicle accidents. Often these spinal injuries are associated with additional long bone, pulmonary, cranial, peripheral nerve, and other system injuries. We found that it was impractical to exclude such subjects because an isolated system thoracic SCI is quite rare, and further would narrow the external validity of our study. It does appear that the burden of associated injuries can have an impact on the rate of natural recovery, perhaps by limiting the ability to participate fully during inpatient rehabilitation. The rotator cuff and brachial plexus injuries experienced by participants TMP001 and TMP002, respectively, did have an impact on their initial rehabilitation activities. The associated trauma and subsequent complications resulting from those injuries experienced by TMP008 significantly delayed the onset of his inpatient rehabilitation and the rate of his natural recovery. All three of these subjects had lower than expected functional abilities (as evidenced by Spinal Cord Independence Measure III and Functional Independence Measure scores) at baseline examinations.
Future prospects
Given that safety concerns were not identified in this small open label study, there is no apparent clinical reason not to pursue further studies of SC transplantation. No clear efficacy was found, but the effect of SC transplantation might be more notable in less severe injuries, or when more cells are delivered. Most pre-clinical studies showing an effect of transplanted SCs have been conducted in animals with incomplete contusions. Given the difficulty of predicting eventual recovery from acute SCI, it may be sensible to test SC transplantation in persons with chronic SCI who have a stable neurological baseline with incomplete injury. Transplantation into established, chronic injuries would allow for much larger doses of cells to be administered, which would provide additional safety information. It is known that the inner margin of the preserved parenchyma contains severed and demyelinated axons. 1 To the extent these are accessible to SCs, focal repair of these axons may be possible in the chronic setting.
Further, it is widely recognized that it will be necessary to utilize therapeutic combinations to optimize neurological recovery that includes multiple biologics as well as exercise and rehabilitation after SCI. We have initiated a study that builds on our experience, but enrolls subjects with chronic SCI with smaller lesions, that will escalate through sequential cohorts beginning with complete thoracic and cervical subjects to subjects with severe incomplete injury. A cavity-filling SC dose strategy will be employed to optimize cell survival and efficacy in the penumbra and tissue formation within the cavity.
Footnotes
Acknowledgments
We would like to acknowledge all of the team members that contributed to the trial, including James Adcock, Gagani Athauda, Francisco Benavides, Adrianna Brooks, Diana Cardenas, Kevin Dalal, Maxwell Donaldson, Shelly Garcia, Katie Gant, Anil Lalwani, Alberto Martinez-Arizala, Katie Nagle, Andrea Santamaria, Risset Silvera Rodriguez, Steven Vanni, Michael Wang, and Lloyd Zucker. The syringe positioning device utilized for the injections was provided to the Miami Project for the clinical study by Dr. Ed Wirth. We are grateful for the critical oversight provided by our Data Safety Monitoring Board members (Drs. Robert Grossman, Howard Landy, Steve Kirshblum, and Nick Boulis) and our External Advisory Board members (Drs. Dan Lammertse, Mark Tuszynski, and James Fawcett). Most importantly, we are indebted to all of our participants and their families for deciding to participate in this trial and contribute to the advancement of our field. Funded by the Buoniconti Fund to Cure Paralysis and the Miami Project to Cure Paralysis as well as the Bryon Riesch Paralysis Foundation, Peacock Foundation, the Norman & Bettina Roberts Foundation, and the Katie Samson Foundation. DDP acknowledges support from The John M. and Jocelyn H.K. Watkins Distinguished Chair in Cell Therapies. MBB acknowledges support from the Christine E. Lynn Distinguished Chair in Neuroscience. ADL acknowledges support from the Robert M. Buck Distinguished Chair in Neurological Surgery.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.