
Abstract
There are no reliable neuroimaging biomarkers to predict long-term outcome after spinal cord injury. This prospective longitudinal study evaluates diffusion tensor imaging (DTI) in predicting long-term outcome after cervical spinal cord injury (CSCI). We investigate the admission DTI parameters measured in 30 patients with CSCI, with 16 of them followed up to one year, and 15 volunteers serving as controls. All magnetic resonance imaging examinations were performed within 24 h of injury. The DTI parameters were measured in patients and controls, avoiding areas of hemorrhage in patients and at corresponding upper/middle/lower regions of the spinal cord in controls. Stepwise regression analysis was performed to find relevant parameters (normalized DTI values, age, sex, hemorrhagic contusion [HC or non-HC]) that correlated with two primary outcome measures: patient International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) motor and Spinal Cord Independence Measure (SCIM III) scores at one year. Among all DTI measures, axial diffusivity (AD) most strongly correlated with both motor (r2 = 0.76, p < 0.01) and SCIM III scores (r2 = 0.77, p < 0.01) at one year. Further stepwise regression indicated that including AD (p = 0.0001) and presence of HC (p < 0.0001) in the regression model provided the best model fit for one year ISNCSCI (r2 = 0.93). The AD is a more specific parameter for axonal injury than radial diffusivity; this may indicate that axonal injury in the cord is the main factor affecting patient recovery. Our study demonstrates DTI measurement at the CSCI is a potential neuroimaging biomarker in predicting long-term neurological and functional outcome in blunt CSCI.
Introduction
T
Conventional magnetic resonance imaging (MRI) is used routinely to demonstrate the anatomical site of SCI. The presence of spinal cord hemorrhage, lesion length, and amount of spinal cord compression are used as limited prognostic indicators. 3 –5 Diffusion tensor imaging (DTI) is a noninvasive, advanced MR technique that is sensitive to Brownian motion of water and provides information on the integrity of white matter tracts within the spinal cord that are not visible on structural MRI. 6 –10 The DTI can provide quantitative measurement both in the longitudinal and transverse directions to the long axis of axons.
Pre-clinical and clinical studies have established a robust relationship between DTI measurements and pathological changes to myelin and axons in white matter tracts immediately after SCI. These studies have reported that the typical pattern observed in DTI measurements after axonal injury—a decrease in axial diffusivity (AD) and an increase in the radial diffusivity (RD) and mean diffusivity—are associated with inflammation and edema. 8,9,11 Determining the microstructural changes to myelinated axons and injured versus preserved neurons can be crucial for predicting recovery, triaging to new clinical trials, and deciding on optimal therapy and rehabilitation.
We hypothesize the derangement of DTI parameters measured at the injury site after blunt cervical SCI (CSCI), using a technique that could be performed on most clinical MR scanners in the acute post-injury period, can be a reliable neuroimaging biomarker to predict longitudinal clinical neurological and functional outcomes.
Methods
This prospective, single institutional, longitudinal study was approved by our Institutional Review Board and is Health Insurance Portability and Accountability Act compliant. Written informed consent was obtained.
Subjects
This study was performed between January 2013 and March 2015. Participants had an acute subaxial blunt CSCI resulting in an American Spinal Injury Association Impairment Scale (AIS) A, B, C, D injury. Inclusion criteria: (A) age ≥18 years, both sexes; (B) admitted after blunt trauma; (C) a neurological deficit that can be localized to the cervical spine on clinical examination; (D) a CSCI demonstrated on conventional MRI performed within five days of injury. Exclusion criteria: (A) age <18 years; (B) penetrating mechanism; (C) moderate or severe traumatic brain injury or cerebrovascular accident; (D) concomitant extremity fractures preventing neurological assessment; (E) neurological deficit without cervical spinal contusion; (F) peripheral cord or nerve injury.
All 30 patients were admitted from the accident scene to our hospital (Fig. 1). Patients underwent both computed tomography (CT) and MRI examination of the cervical spine within 24 h from the time of accident. The CT images helped to determine the morphology of cervical spine fracture.
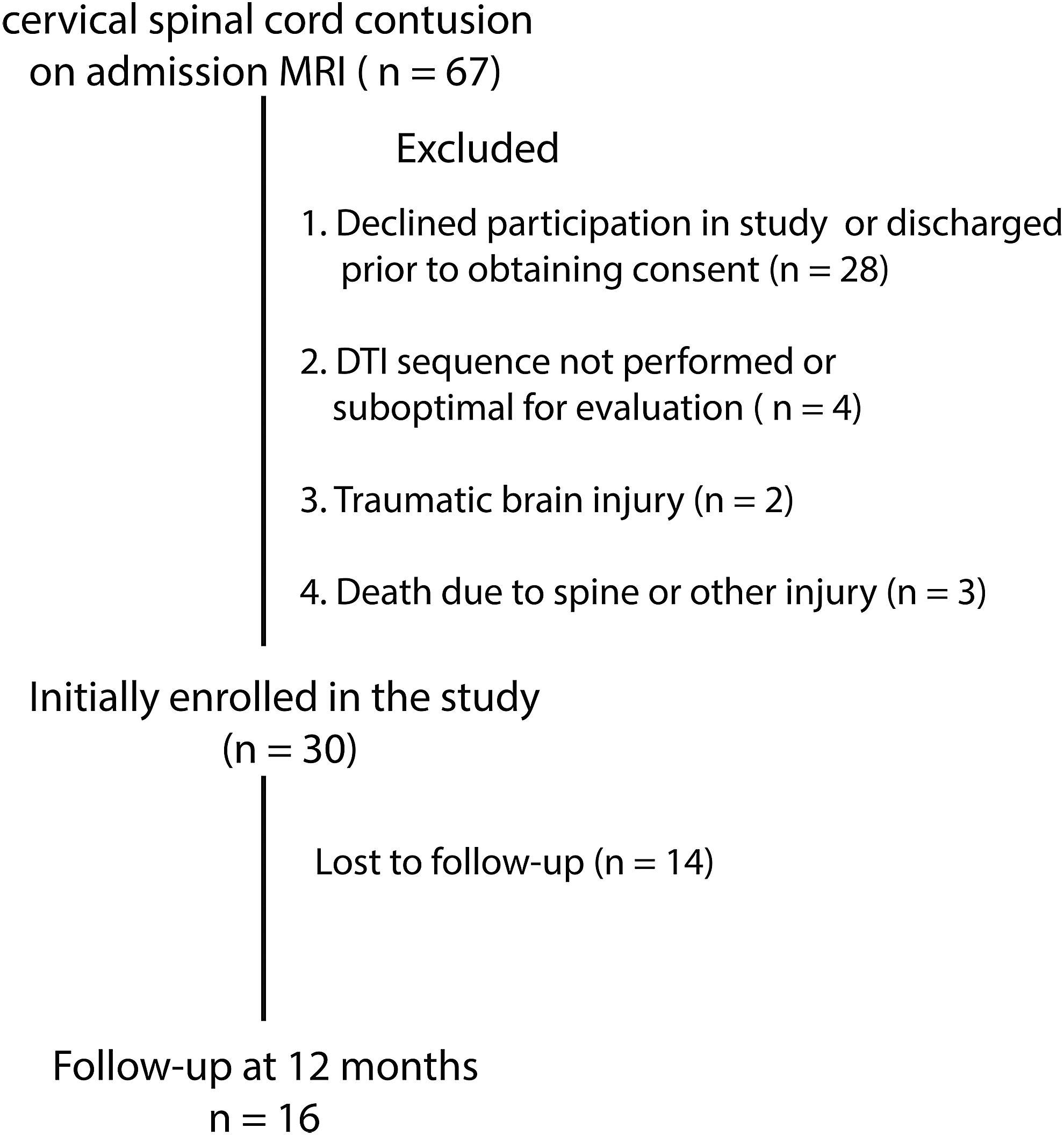
Enrollment of study group. MRI, magnetic resonance imaging; DTI, diffusion tensor imaging.
We enrolled 15 healthy volunteers with comparable age and sex as controls. They underwent the same MRI examination.
MRI technique
All MRI imaging was performed on a 1.5-T Avanto scanner (Siemens Medical Solutions; Erlangan, Germany) using a 12-channel head and four-channel neck array with parallel imaging capability. Conventional MRI included sagittal T2 (echo time/repetition time [TE/TR]: 109/4000 msec), fluid attenuation inversion recovery (FLAIR) (TE/TR: 102/8000 msec, echo train length [ETL]: 13), and axial T2 and T2*, three-dimensional [3D] susceptibility weighted imaging (SWI) (TE/TR: 16/30 msec, flip angle: 20 degrees) images. The DTI was acquired using single-shot echo planar imaging (EPI) sequence at a TE/TR of 87/2800 msec. Partial Fourier factor of 6/8 was used, resulting in a reconstructed resolution of 128 × 128 over a 20-cm field of view.
Diffusion weighting was applied in 20 directions with an effective b-value of 700 sec/mm2 and three averages. A parallel imaging acceleration factor of two was used. A total of 20 axial slices at 4-mm slice thickness were acquired centered at the location of the contusion for patients. For volunteers, three acquisitions were performed each with 20 slices placed at upper (lower brainstem to C2), mid (C3-C5), and lower (C6 to T1) sections. Sagittal T2-weighted short tau inversion recovery (STIR) images and b = 0s/mm2 images from the DTI scan were used for anatomic reference.
Image analysis
DTI data were reconstructed offline using Diffusion Toolkit (
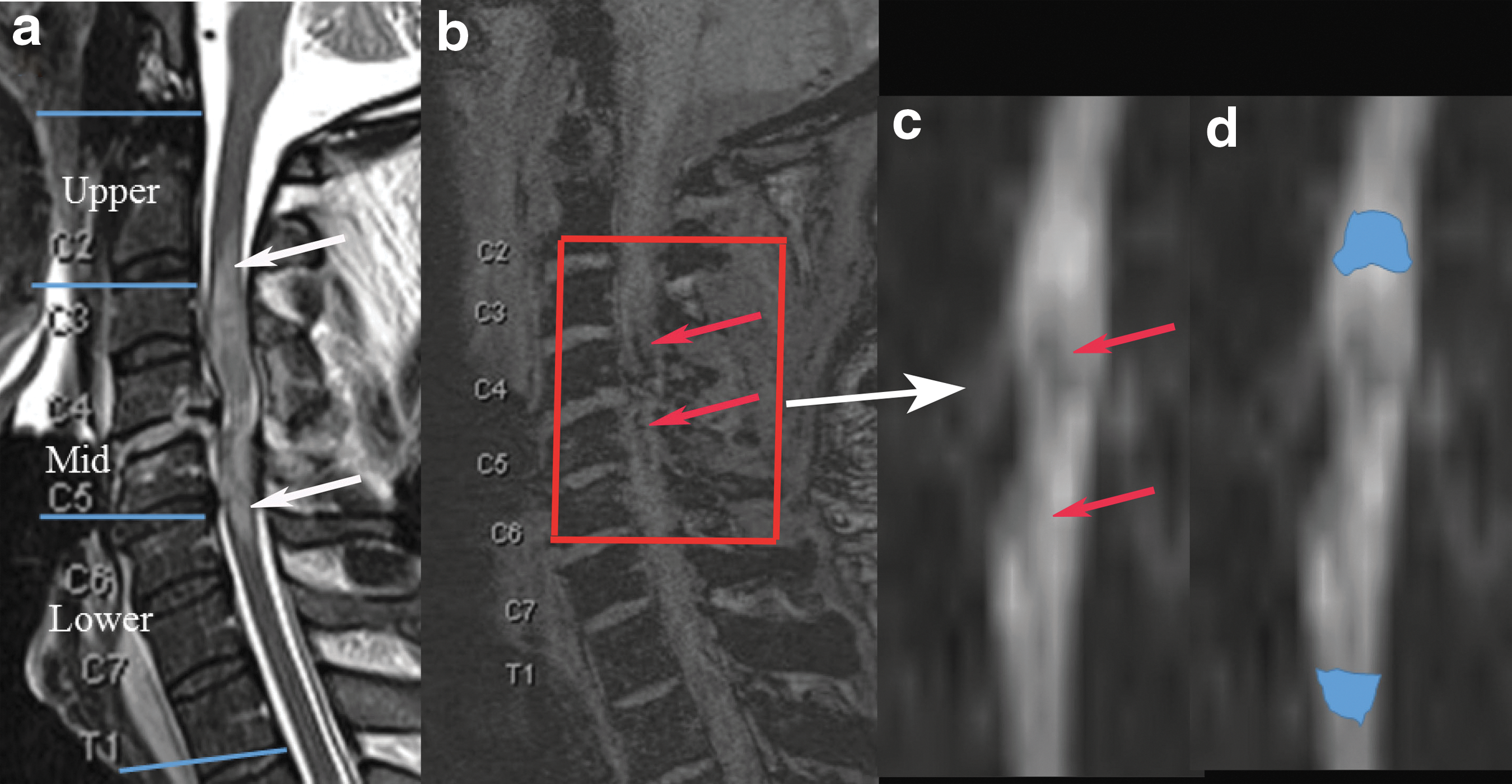
Conventional and diffusion tensor images of a patient admitted after a flexion distraction injury at the C4-C5 levels (
The ROIs were placed carefully to include the areas of edema within the injury site (which may include both gray and white matter) and avoid cerebrospinal fluid. Slices on which there was hemorrhage or areas of spinal stenosis where small amount of cord were visible were avoided. The ROIs included areas of edema that were confirmed using T2 and STIR sequences, and sites of hemorrhage were confirmed using SWI and T2* sequences. If disconnected ROIs were drawn, average DTI measurements were used for evaluation.
Because of the potential diffusion tensor differences based on anatomical location in the cervical cord in controls, an ROI was drawn on in the upper (lower brainstem–lower C2), mid (upper C3–lower C5), and lower (upper C6–lower T1) sections of the cervical spine (Fig. 2). 10 To account for anatomical differences because of injury location of the cord, normalized patient DTI values within the injury site were calculated by taking z-scores of patient ROI values as compared with control ROI values at the corresponding location in patient outcome prediction:
Normalized DTI value = (patient ROI mean–control ROI mean)/Control ROI SD
SD represents the standard deviation within the control data. In a case in which patient ROI encompasses more than one section of the control ROI, two or three levels of the control ROI mean values and variance were averaged to derive the control ROI mean and SD. The normalized DTI values reflect the deviation of these values from controls at the injured site. The SWI and T2* images were utilized to determine the presence of hemorrhage within the SCI to identify patients with hemorrhagic contusions (HC) and nonhemorrhagic contusions (NHC).
Clinical assessment
Patients underwent comprehensive clinical assessment using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) protocol before discharge from the hospital (mean 17 days, range 3–58 days) and at one year after injury. 12,13 The Spinal Cord Independence Measure (SCIM III) was administered at one year after injury to assess functional outcome. 12,14 The assessment was performed by a trained certified physical therapist with at least seven years of experience evaluating patients with SCI without the knowledge of the type of SCI or of DTI measurements. Both of these scores range from 0 to 100, with a higher score indicating greater ability. The demographic, neurological, and functional imaging collected prospectively from each patient are shown in Tables 1a and b. Based on their injury severity, patients were administered tailored rehabilitation programs to maximize recovery.
N/A, not applicable; MVC, motor vehicle collision; MRI, magnetic resonance imaging; ISS, Injury Severity Score; SD, standard deviation; TRISS, Trauma and Injury Severity Score; RTS, Revised Trauma Score; ASCOT, A Severity Characterization of Trauma; SBP, systolic blood pressure; GCS, Glasgow Coma Score; ICU, intensive care unit.
ISNCSCI, International Standards for the Neurological Classification of Spinal Cord Injury; SCIM - Spinal Cord Independence Measure; NA, not available; H, hemorrhagic cord contusion; NH, non-hemorrhagic cord contusion.
Level of cord contusion on conventional MRI: 1 = lower brainstem ∼ lower C2, 2 = upper C3 ∼ lower C5, 3 = upper C6 ∼ lower T1.
Statistical analysis
A descriptive analysis of patients' characteristics and related measures and clinical assessments was performed with absolute and relative frequencies for qualitative variables and means (SD) for quantitative variables. One-way analysis of variance (ANOVA) followed by pair-wise comparison was used to test for group differences in DTI parameters in patient versus control at different levels (lower, mid, upper) of the cervical spine. Further paired t test was performed to compare DTI parameters within the control group. The associations between normalized DTI parameters at admission and SCIM III and motor scores at one year, patient age, sex, type of contusion, and discharge ISNCSCI motor scores were analyzed by examining the Pearson correlation coefficients. To adjust other variables associated with outcomes, multiple regression models with SCIM III or motor scores at 1 year as dependent variables and each of the normalized DTI parameters and other potential variables such as age and HC as independent variables were investigated with stepwise selection procedure.
With respect to each of two clinical assessments, regression models involving each of the normalized DTI parameters were analyzed and r-squared (r2) measuring the fitness of the models were calculated. The same regression analysis was performed using admission motor score only, to compare performance of the acute normalized DTI measures and the admission motor scores ability to predict outcome. To account for performing multiple regression tests across many DTI parameters, the Bonferroni approach of multiple comparison correction was applied. Statistical analyses were performed with the SAS software package version 9.4 (Cary, NC).
Results
Figure 3 and Table 2 show the patient DTI values compared with different sections of the cervical spine of normal controls. Differences were observed in DTI values among the three anatomical levels in the control cervical spinal cord; the paired t test results indicate a gradual reduction in FA (upper vs. lower: p = 0.001; mid vs. lower: p = 0.0005) and a gradual increase in MD (upper vs. lower: p = 0.02; mid vs. lower: p = 0.05) and RD (upper vs. lower: p = 0.007; mid vs. lower: p = 0.002). Changes in AD were only observed with an increase from the mid to lower section (p = 0.014). The DTI measurements reported in this study are similar to those of other studies reported in the literature by Ellingson and associates 15 and our institution. 10 The technique we used is similar to that used by Ellingson and coworkers, 15 and the short scan times are suitable to use in the scenario of multi-trauma subjects with cervical SCI. The ANOVA indicates that there is a significant group difference (p < 0.0001) for patients versus controls for any DTI parameter. Patients FAs and ADs were significantly lower than controls at any location (p < 0.001). Patients RDs were significantly higher than the middle (p = 0.0088) and upper (p < 0.001) sections of controls.
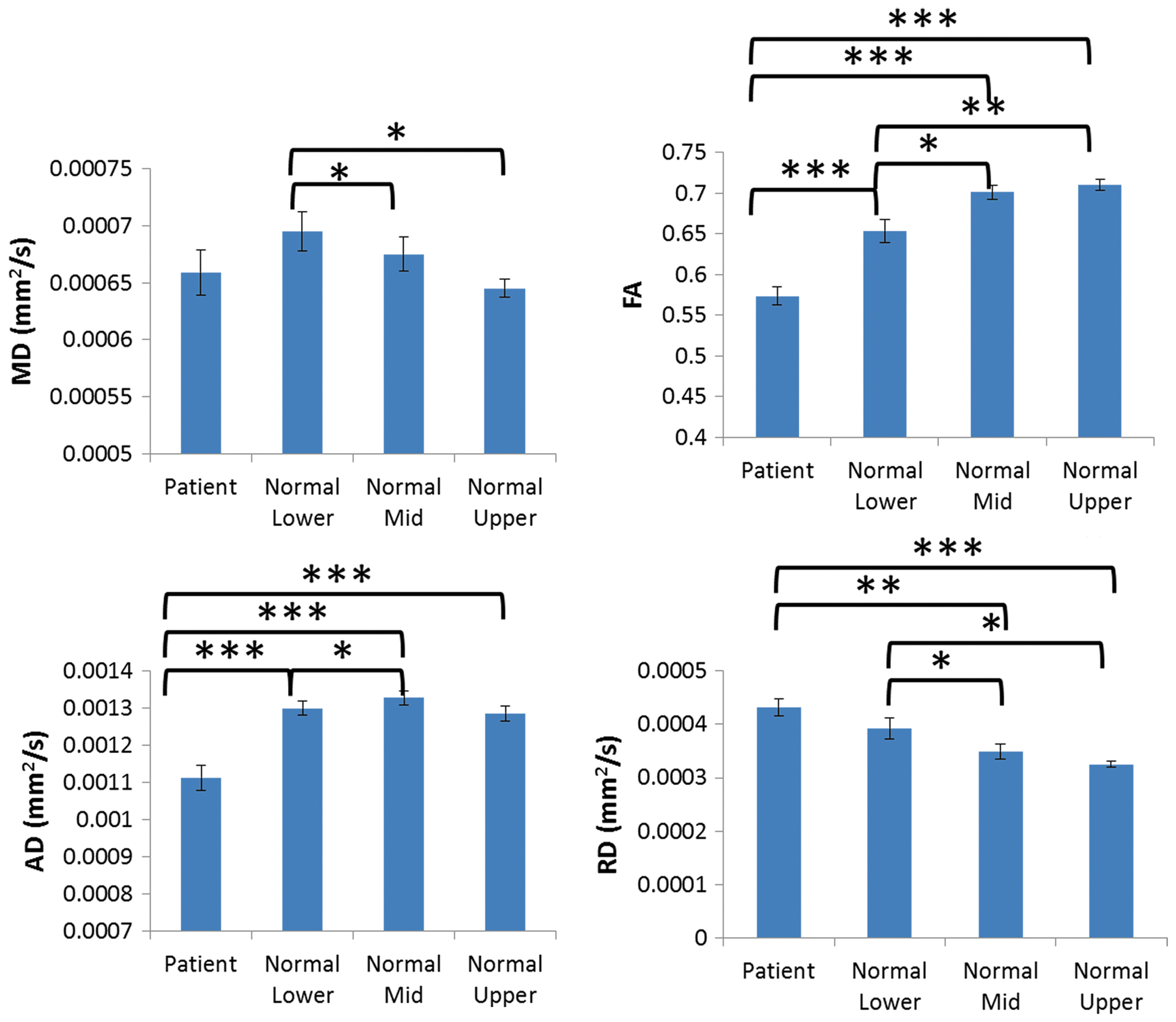
Diffusion tensor values for patients (at contusion) and controls (lower, mid, upper sections). The p values indicate significant differences between different sections within controls, as well as patients versus controls. *: p < 0.05, **: p < 0.001, ***: p < 0.0001. MD, mean diffusivity; FA, functional anisotropy; AD, axial diffusivity; RD, radial diffusivity. Color image is available online at
FA, fractional anisotropy; MD, mean diffusivity; AD, axial diffusivity; RD, radial diffusivity.
The p values shown are unpaired t test for patients versus controls. Bold indicates p values <0.05. Upper: lower brainstem to C2, mid: C3-C5, and lower: C6 - T1
DTI values (FA, MD, AD and RD) in patients at the contusion site, and controls at lower, mid, and upper levels in the cervical spinal cord.
Table 3 shows the Pearson correlation coefficients for normalized patient DTI measures with patient age, sex, type of CSCI, and ISNCSCI motor and SCIM III scores at one year. The MD, FA, and RD significantly correlate with age, indicating age related white matter changes in the spinal cord are similar to those seen in the brain. 16 AD showed strongest correlation with type of CSCI, motor, and SCIM scores. FA showed no correlation with any patient clinical measures.
MD, mean diffusivity; FA, fractional anisotropy; AD, axial diffusivity; RD, radial diffusivity; HC, hemorrhagic contusion; NHC, nonhemorrhagic contusion; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; SCIM, Spinal Cord Independence Measure.
Stepwise regression for ISNCSCI motor score at one year showed age and sex had no effect on the outcome, while presence of HC and specific normalized DTI parameters were important factors in predicting outcome (adjusted p < 0.001). Among the four normalized DTI parameters, AD in the regression model provided the best model fit (r2 = 0.93, AD) (Fig. 4,5). Other significant normalized DTI parameters included MD (r2 = 0.89, MD) and RD (r2 = 0.86, RD). The DTI parameters AD, RD, and MD are significant for predicting ISNCSCI motor score at one year, but not FA. In both NHC and HC patients, higher normalized MD, AD, and RD are indicative of higher ISNCSCI motor score at one year. For SCIM III score, regression model including HC and AD has r2 = 0.84.
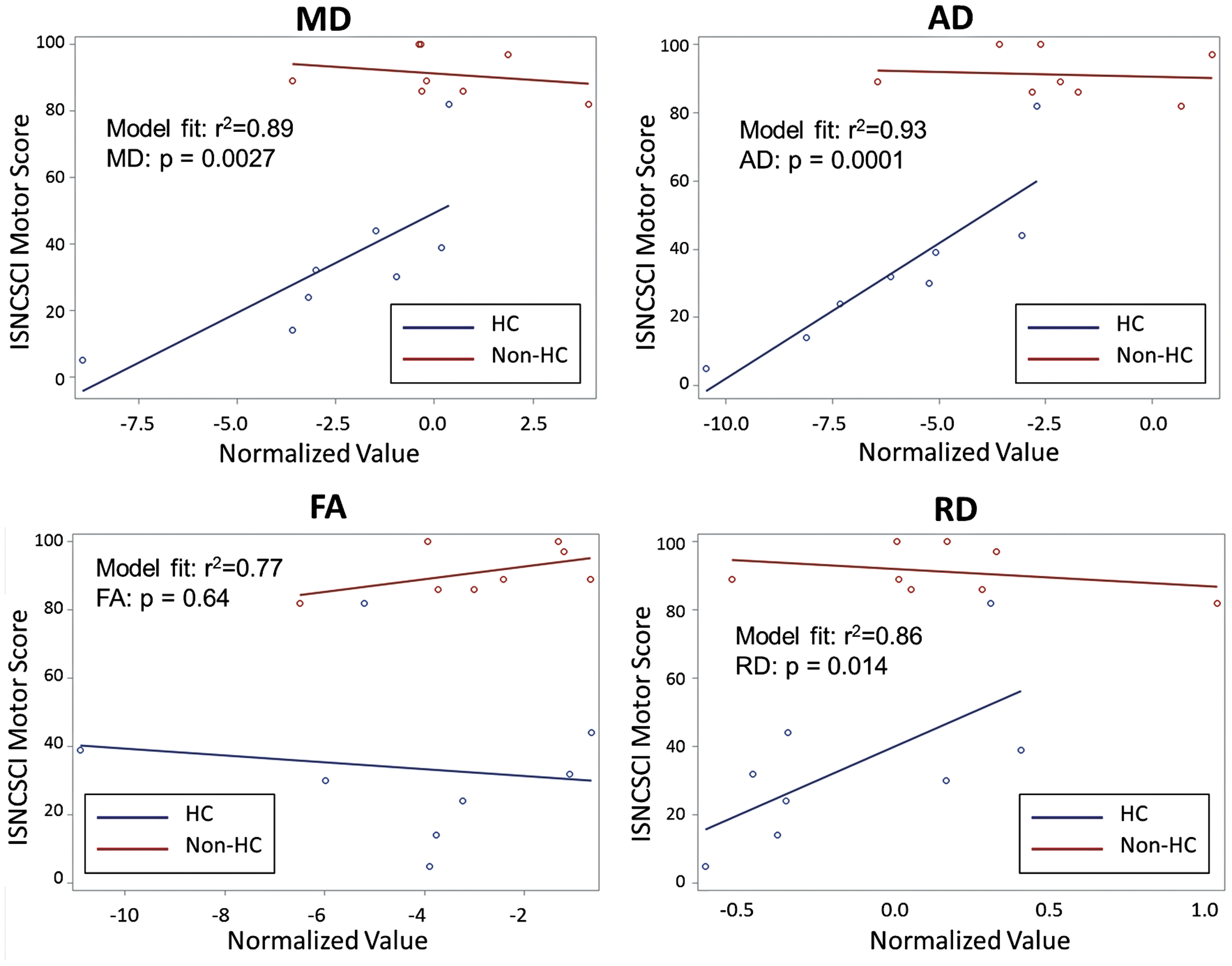
Correlations between the diffusion tensor imaging (DTI) measurements at contusion (represented as z-score compared with control measurements at corresponding spine levels) and 12 month International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) motor score with nonhemorrhagic (Non-HC) and hemorrhagic (HC) spinal cord injury. Also shown on figure are r2 values for the regression model fit, and p value for the specific DTI measurement within the model. MD, mean diffusivity; AD, axial diffusivity; FA, functional anisotropy; RD, radial diffusivity. Color image is available online at
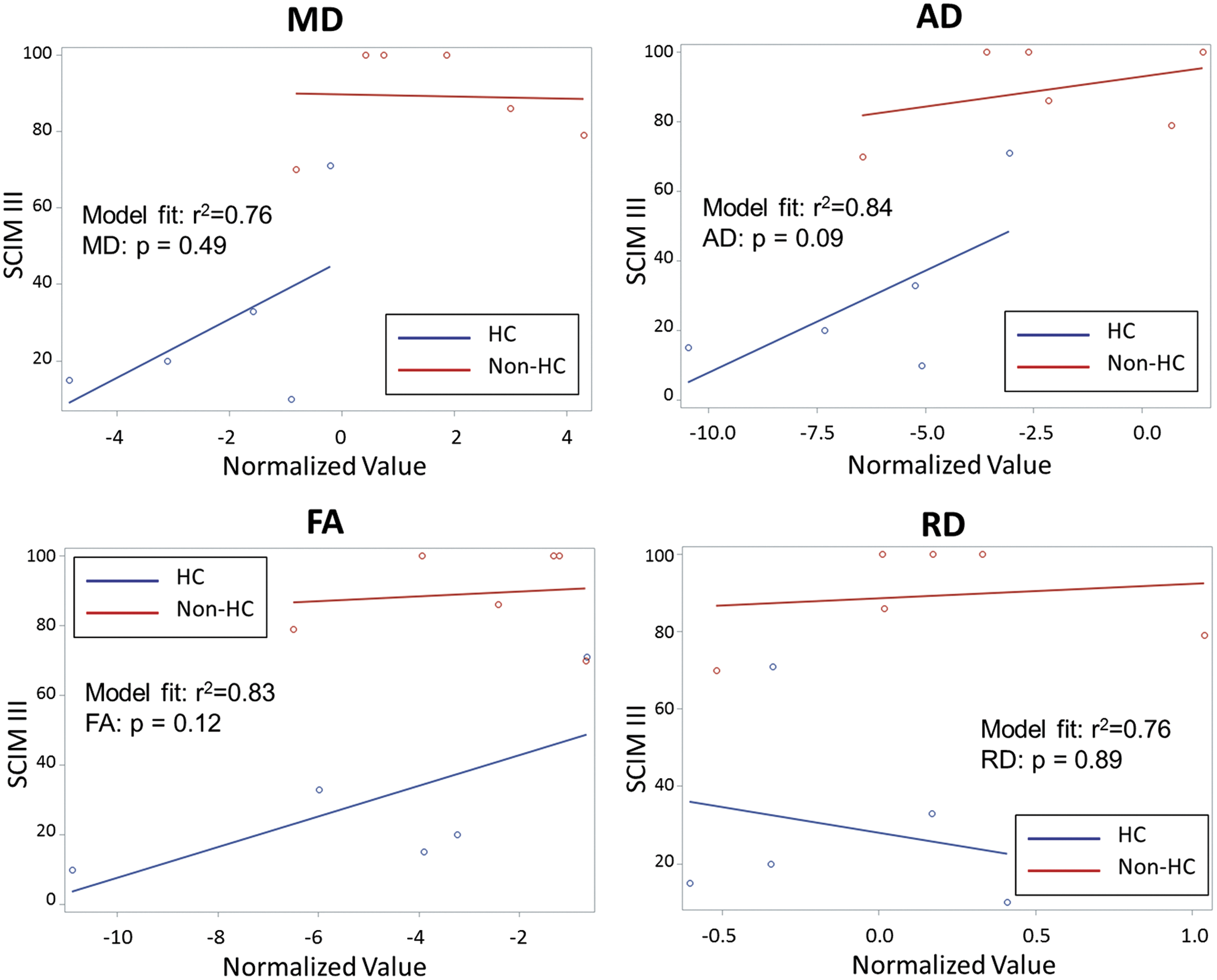
Correlations between the diffusion tensor imaging (DTI) measurements at contusion (represented as Z-score compared with control measurements at corresponding spine levels) and 12 month Spinal Cord Independence Measure (SCIM) III score with nonhemorrhagic (Non-HC) and hemorrhagic (HC) spinal cord injury. Also shown on figure are r2 values for the regression model fit, and p value for the specific DTI measurement within the model. MD, mean diffusivity; AD, axial diffusivity; FA, functional anisotropy; RD, radial diffusivity. Color image is available online at
Replacing normalized DTI measures with discharge ISNCSCI motor scores as the same regression model parameters for motor and SCIM III scores at one year were r2 = 0.78 and r2 = 0.88, respectively.
Discussion
Our study provides new insight showing DTI measurements made within 24 h of SCI at the site of contusion seen on conventional MRI can be a reliable, accurate neuroimaging biomarker to predict long-term neurological and functional outcomes at one year. Normalized DTI values were used here to represent a deviation of contusion values from normal control, while controlling for anatomical variation in DTI values in the cord, depending on injury location. Among the DTI measurements, AD was the best predictor of both neurological and functional outcomes. Accurately measuring the extent of neuronal injury can address the pressing need to provide information that can be utilized to optimally triage patients into appropriate new therapies and rehabilitation.
A decrease in AD, the diffusion properties of water parallel to white matter tracts, has been associated with axonal injury in in vivo animal studies. 9,12,16 –20 Although AD is more specific for axonal injury than RD, there could be contribution from myelin damage as well. These pre-clinical models report excellent correlation between reduced AD and histological analysis of the extent of injured spinal cord. For example, the reduction in AD measurements observed at the contusion epicenter after graded injury to mouse spinal cord demonstrated correlations with the amount of cytotoxic edema and white matter necrosis on spinal cord histological evaluation. 16,17
The authors postulate axonal beading, a characteristic morphology that occurs in nerve cells subjected to ischemic or stretching insult, may occur in CSCI as well. The underlying mechanism was thought to be cytoskeletal damage from calcium influx through mechanically induced axolemmal pores and the subsequent activation of calpains. 19 Focal disruption of cytoskeleton leads to impaired axonal transport, and the accumulated membranous cargo leads to axonal beading, which could start minutes post-traumatic injury. Beaded axons affect water diffusion along the direction parallel to the axons, which directly manifests as reduced AD, as has been shown through biophysical modeling. 20
Among the four measurements (AD, RD, MD, and FA) made in our study, AD best predicted both neurological and functional outcomes at one year, akin to that reported in pre-clinical studies. There was optimum correlation between admission normalized AD measurements within the SCI and both the ISNCSCI motor and SCIM III scores at one year suggesting that admission AD is the best biomarker among the four DTI parameters measured in this study. To our knowledge, this is the first study to demonstrate that admission AD has the potential to be a DTI neurobiomarker to predict both long-term functional and neurological outcomes after CSCI. Therefore, DTI has the potential to be used in the future to prospectively triage patients into appropriate therapeutic intervention and plan long-term rehabilitation. These novel results, however, need further validation using a larger sample size.
In our study we used SWI, a high resolution three-dimensional gradient-echo imaging technique very sensitive to blood products, to identify areas of hemorrhage within the SCI. 21,22 It has been shown that high spatial resolution SWI is more sensitive than traditional gradient recalled-echo MR sequence in demonstrating hemorrhage within spinal cord contusions. Artifact arising from hemorrhage can decrease the accuracy of DTI measurements. 23,24 This helped avoid areas of hemorrhage and include only areas of NHC within the hand drawn ROI, providing accurate DTI measurements.
All the patients in our study came directly from the accident scene to our hospital, enabling us to obtain the MRI examination for the entire study group within 24 h of the accident. Because of spinal shock during this hyperacute period, typically the neurological assessment is unreliable and cannot be used to accurately predict long-term outcome. The technique we used to obtain both conventional and DTI sequences is obtainable on most clinical MR scanners in the acute post-injury period in U.S. trauma centers. The DTI measurements we report in our study are obtainable on standard workstations provided by all MR vendors and will be the only biomarker available immediately after the MR examination. It has the potential to prognosticate functional outcome, a currently unmet need, as well as help formulate optimum definitive therapy and triage patients to novel new therapies. Providing accurate, long-term functional and neurological prognoses early after SCI may help to alleviate the immense anguish most patients and families face during this period.
Our study has some limitations, including the small sample size with a limited number of patients with follow-up neurological and functional outcome scores, especially the correlation between the DTI parameters and SCIM III. These small numbers are because of the difficulty in recruiting patients with cervical SCI in a single center and obtaining follow-up assessment at one year. The drop-off rate in this study is similar to that reported in other studies. Also, some of the small hemorrhages seen on SWI may have been incorporated in the manually drawn ROI used to contribute to the DTI values obtained. Patients did not undergo a uniform rehabilitation regime, which may have influenced the recovery rates. Despite these limitations, however, we were able to demonstrate a robust correlation between admission DTI parameters and long-term outcome. Obtaining the MRI examination within 24 h of injury in all patients when ISNCSCI motor scores are unreliable is a strength of this study.
Conclusion
Our study provides insight into a new, robust potential neuroimaging biomarker that can be measured early after SCI to accurately prognosticate long-term functional and neurological outcomes. These results should be validated using a larger sample size to determine the important role of AD in evaluating new therapies, designing trials, improving rehabilitation planning, and setting functional goals.
Footnotes
Acknowledgment
Source of funding is FA8650-12-2-6D07.
Author Disclosure Statement
No competing financial interests exist.