
Abstract
Examination of trends in Veterans Health Administration (VHA) healthcare utilization and costs among veterans with mild traumatic brain injury (mTBI) is needed to inform policy, resource allocation, and treatment planning. The objective of this study was to assess the patterns of VHA healthcare utilization and costs in the 3 years following TBI screening among veterans with mTBI, compared with veterans without TBI. A retrospective cohort study of veterans who underwent TBI screening in fiscal year 2010 was conducted. We used VHA healthcare utilization and associated costs by categories of care to compare veterans diagnosed with mTBI (n = 7318) with those who screened negative (n = 75,294) and those who screened positive but had TBI ruled out (n = 3324). Utilization and costs were greatest in year 1, dropped in year 2, and then leveled off. mTBI diagnosis was associated with high rates of utilization. Each year, healthcare costs for those with mTBI were two to three times higher than for those who screened negative, and 20–25% higher than for those who screened positive but had TBI ruled out. A significant proportion of healthcare use and costs for veterans with mTBI were associated with mental health service utilization. The relatively high rate of VHA utilization and costs associated with mTBI over time demonstrates the importance of long-term planning to meet these veterans' needs. Identifying and engaging patients with mTBI in effective mental health treatments should be considered a critical component of treatment planning.
Introduction
T
To facilitate identification and treatment of veterans returning from the wars in Iraq and Afghanistan with symptomatic mTBI, the Veterans Health Administration (VHA) implemented a TBI screening program in April, 2007. 10 VHA's TBI screening program involves: (1) screening all veterans returning from the wars in Iraq and Afghanistan for history of TBI and current symptoms during their initial VHA visit using a four item screening tool that VHA developed for this purpose and (2) comprehensive TBI evaluation for those who screen positive. VHA's TBI screen identifies veterans with possible TBI history and current symptoms, including such common and nonspecific symptoms as irritability, sleep problems, and headaches. 10 Veterans who report already having been diagnosed with a TBI are not screened, but are offered assessment by the TBI team. During the comprehensive TBI evaluation, a TBI specialist confirms or rules out TBI history, assesses injury etiology and TBI severity and, regardless of TBI history, refers the veteran for services to further evaluate and/or treat the identified symptoms or diagnoses. The VHA has screened almost all Afghanistan and Iraq war veterans who had a qualifying appointment. 11
Given the purpose of VHA's TBI screening program, to identify veterans with symptomatic mTBI and refer them for appropriate follow-up, one would expect an association between screening outcomes and healthcare utilization. Available research suggests that this is the case in the year following screening. In a study based on national VA data from 2007 and 2008, Stroupe and colleagues 12 reported higher healthcare utilization and costs in the year following screening among those diagnosed with TBI than among those who had screened negative and those who screened positive but did not receive a TBI diagnosis. There are two important limitations to this work. First, their sample of veterans with TBI included all severity levels, making it impossible to determine how findings generalize to those with mild versus more severe TBI histories. Given the clinical differences between mild and more severe TBI, 13 one might expect differences in patterns of utilization and costs. The need for research on the healthcare use and costs associated with mTBI in particular has been well recognized because of its relative frequency. 14 Second, Stroupe and colleagues examined utilization and associated costs in the 1st year only following TBI screening. It is unknown whether the observed pattern of elevated use and costs among those with TBI continues after this 12 month period. Information on patterns of healthcare utilization and costs over longer periods of time is needed to inform policy and decisions regarding resource allocation, and to understand the clinical needs of veterans with TBI over time. Estimates of healthcare needs of Iraq and Afghanistan war veterans therefore require an examination of healthcare use and costs beyond the year following TBI screening.
The primary objective of this descriptive study was to evaluate trends in VHA healthcare utilization and costs in the 3 years following TBI screening among veterans with mTBI, and to compare these patterns with those observed in two groups of veterans without TBI: those who screened negative for TBI and those who screened positive but had TBI ruled out after undergoing a comprehensive TBI evaluation. Including both of these comparison groups was important, because those who screen positive but do not have TBI are clinically different from those who screen negative. This study, therefore, provides information on patterns of utilization and costs of care for veterans with mTBI to inform policy and long-term planning.
Methods
Overview and study population
This retrospective cohort study used Department of Veterans Affairs (VA) and Department of Defense (DoD) administrative data sets. The institutional review board of the Minneapolis VA Health Care System approved the study.
Data sources
The population of Iraq and Afghanistan war veterans screened for TBI in fiscal year 2010 was identified using the VA/DoD Operation Enduring Freedom (OEF)/ Operation Iraqi Freedom (OIF)/Operation New Dawn (OND) roster and the VA TBI Screening and Evaluation data sets. We merged these datasets with VHA enrollment files, patient geocode files, VETSNET, and Corporate Data Warehouse (CDW) databases to obtain background information. We used CDW inpatient and outpatient domains to obtain TBI diagnoses and categorize inpatient and outpatient service utilization. We used MedSAS Fee Basis data to identify healthcare outside of VHA facilities but paid by VHA. We used VA Managerial Cost Accounting National Cost Extracts (MCA) to capture costs. MCA follows practices known as activity-based cost accounting, and these methods are designed to provide precise cost estimates for care that occurred within VHA facilities. 15,16
TBI status
We identified 98,072 Iraq and Afghanistan war veterans who were screened within the VHA's TBI screening program in fiscal year 2010, of whom 22% screened positive for possible TBI (Fig. 1). Almost three quarters of those who screened positive for TBI subsequently underwent a comprehensive TBI evaluation in which TBI was either confirmed or disconfirmed. Among those who screened positive, those with missing or incomplete evaluations were excluded. Among those who screened negative, those diagnosed with TBI in the year before or after screening or who were found to have a VA disability rating for TBI were excluded.
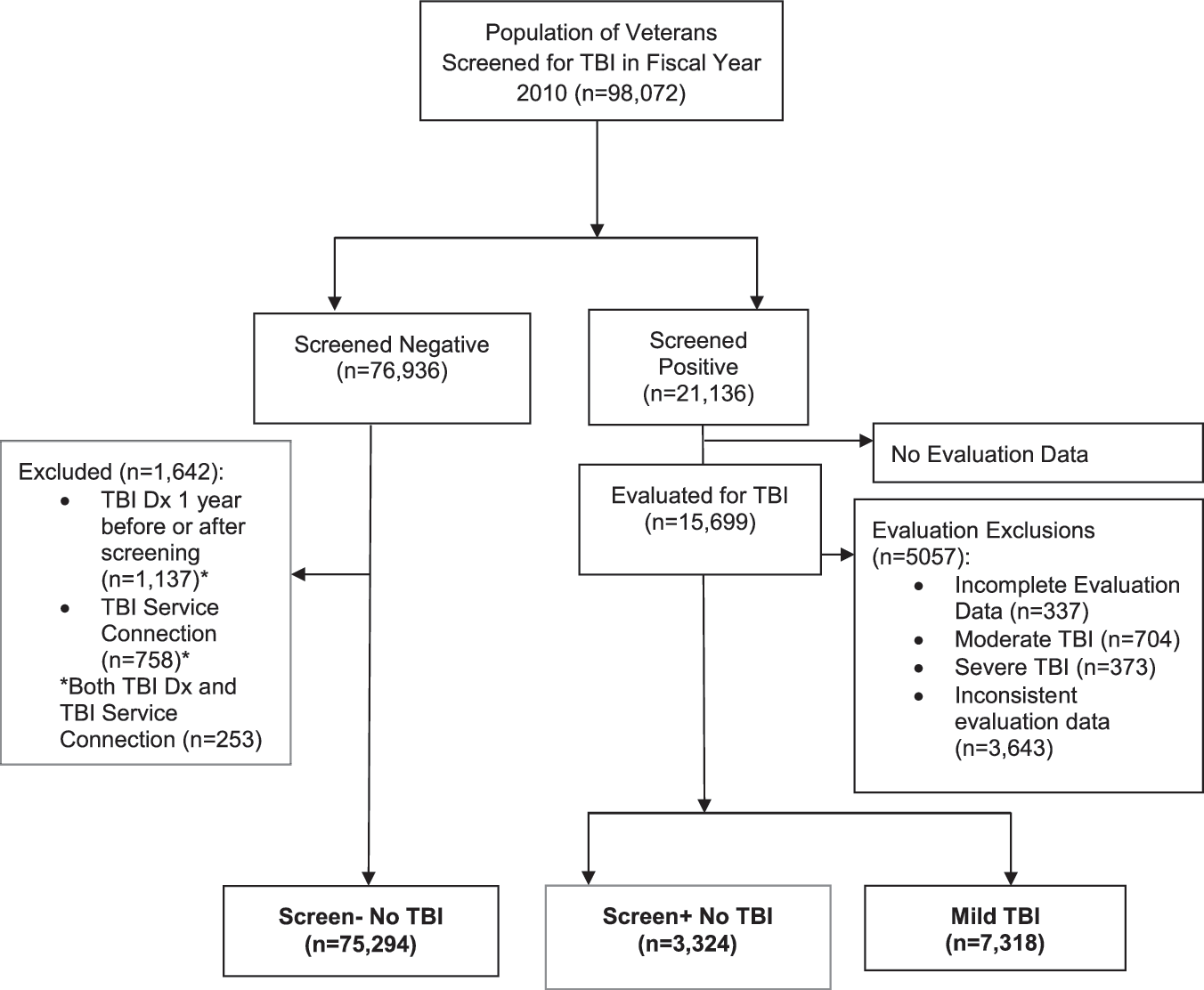
Study flow diagram.
We categorized veterans into three groups by TBI status. The mTBI group included people who a clinical evaluator determined had TBI, and who reported exposures and symptoms consistent with the American Congress of Rehabilitation Medicine (ACRM) criteria for mTBI 3 during the comprehensive TBI evaluation following positive TBI screen. Those who reported LOC >30 min, alteration of consciousness >24 h, and/or post-traumatic amnesia >24 h during the comprehensive TBI evaluation were excluded because their injury exceeded these criteria. As can be seen in Figure 1, among the 8395 veterans with mild, moderate, or severe TBI, the majority (87%) had mTBI. The first no-TBI comparison group included those who screened negative for TBI (Screen- No TBI, n = 75,294); the second no-TBI comparison group included those who screened positive for TBI but had TBI ruled out during the comprehensive TBI evaluation (Screen+ No TBI, n = 3324).
Healthcare utilization and costs
The care veterans received during each of the 3 years following the screening visit was categorized into the following groups: any outpatient care, any pharmacy care, any inpatient care, and any fee basis invoices. Each outpatient encounter was further categorized, using VHA stop codes, into: primary care, mental health, TBI specialty, other specialty care, and all other care. Inpatient stays were categorized using VHA bed sections into: general medicine, surgery, mental health, rehabilitation, and other inpatient. Fee basis costs were split out into outpatient and inpatient care. Details on the specific stop codes used to define the subcategories of care are documented elsewhere. 17
Cost data were collapsed into the same groupings as utilization data. For each category of care, a yes/no indicator was created to identify whether or not the veteran had that category of care during each year of follow-up. The indicator of having care was based on utilization data, with exceptions for pharmacy data and some prosthetic and miscellaneous care that only had costs.
Statistical analysis
We used descriptive statistics to compare groups in terms of demographic and military characteristics and to summarize VHA healthcare utilization and costs. Within the different categories of care, we identified the proportion of veterans with that type of care, the mean number of outpatient encounters, total costs, and costs attributed each category. Because costs were highly skewed, in addition to means we present median and interquartile ranges.
To describe between-group differences in costs, we examined cost ratios, comparing mTBI to the Screen+ No TBI and the Screen- No TBI groups in each of the 3 years post- screening. However, between-group differences could be partially attributable to between-group differences in background characteristics, skewed distribution of costs, or between-group differences in proportion of veterans using VHA healthcare in years 2 and 3 of the study. Therefore, we also computed three additional cost ratios controlling for potential confounders (sex, geographic region, race, ethnicity, rank, service, military component, urban/rural status, education, age at screening, and time between screening and last deployment): (1) assuming a normal distribution for costs, (2) assuming a log gamma distribution for costs, and (3) excluding from the denominator the veterans who did not have any healthcare utilization or cost in the year of interest. All analyses were performed using SAS version 9.2 (SAS Institute Inc., Cary, NC).
Results
Participants
Demographics of the 85,936 veterans included in the three groups are presented in Table S1 (see online supplementary material at
Healthcare utilization
Across all three groups, healthcare utilization was greatest in the year following screening. The drop in the proportion using VHA care in the 2nd year was maintained in year 3 (Table 1). More than one third of veterans in the Screen- No TBI group did not return in subsequent years for any VHA care, whereas ∼15–20% of veterans with mTBI and 18–22% in the Screen+ No TBI groups did not return for care in the 2nd and 3rd years following screening. In general, a larger proportion of those with mTBI received each category of outpatient and inpatient care, pharmacy, and fee basis services in the 3 years after screening than those in the two no-TBI comparison groups. The difference was far more dramatic when we compared mTBI with the Screen- No TBI group than when we compared the mTBI group with the Screen+ no TBI group.
We removed one encounter from the Mild TBI and Screen+ No TBI groups to account for the comprehensive TBI evaluation.
TBI, traumatic brain injury; VHA, Veterans Health Administration.
Table 2 shows mean number of outpatient encounters by categories of care over time. On average, veterans with mTBI had 35.5 encounters in the year following the screening visit compared with 14.3 and 30.0 for the Screen- and Screen+ No TBI groups, respectively. Although the overall mean number of encounters decreased in years 2 and 3, the trend for higher numbers of encounters in the mTBI group compared with both no-TBI groups persisted. Across years, in the mTBI and Screen+ no TBI groups, mental health care comprised the largest proportion of encounters. Specifically, approximately one third of all encounters were for mental healthcare, and this proportion increased slightly over time. However, across years, the number of mental health encounters was higher in the mTBI than in the Screen+ no TBI group. In the Screen- No TBI group, approximately one quarter of all encounters were for mental healthcare, whereas “other” outpatient encounters comprised the largest proportion of encounters. Not surprisingly, those with mTBI had more TBI specialty care encounters than those without TBI. In the mTBI group, the proportion of TBI specialty care encounters dropped noticeably after year 1.
We removed one encounter from the Mild TBI and Screen+ No TBI groups to account for the comprehensive TBI evaluation.
TBI, traumatic brain injury.
Healthcare costs
In the 1st year following TBI screening, veterans with mTBI had mean total costs of $12,045 (median = $7418) compared with $4515 (median = $2313) for the Screen- No TBI group and $10,116 (median = $5932) for the Screen+ No TBI group (Table 3). Overall costs decreased dramatically for all groups after year 1 (a 67–73% drop in median costs and a 39–45% drop in mean costs), but then plateaued. Veterans with mTBI had higher costs across almost all care categories throughout all 3 years compared with the two no-TBI comparison groups (Tables S2 and S3) (see online supplementary material at
Only the mean is presented because median and IQR = zero because of the low proportion of veterans using these services.
VHA, Veterans Health Administration; TBI, traumatic brain injury; IQR, interquartile range.
Ratio of healthcare costs
Table 4 shows the ratios of costs comparing the mTBI group with each no-TBI comparison group. In the 1st year after screening, regardless of adjustment and distribution, costs were almost three times higher in the mTBI than in the Screen- No TBI group. This difference was slightly less in the following 2 years. Excluding veterans who did not return to VHA care in years 2 or 3 from the average cost models explained some of the differences in costs between the mTBI and Screen- No TBI group (35% and 40% in years 2 and 3, respectively). However, veterans with mTBI still had 75% higher costs in year 3 than did the Screen- No TBI group. In general, healthcare costs were 20–25% more for those with mTBI than for those in the Screen+ No TBI group.
Multivariable adjusted (MV) models included age, sex, race, ethnicity, geographic region of the screening visit,
military service, education, and time between screening and last deployment.
All veterans in the models that excluded “non-users” had to be living in that year and have some utilization and costs in that year.
VHA, Veterans Health Administration; TBI, traumatic brain injury.
Discussion
This study makes two major contributions to the literature. It is the first study of VHA healthcare utilization and costs among veterans with mTBI. The lack of high-quality data on costs associated with deployment-related TBI and mTBI, in particular, has been identified as an important limitation in estimating the overall costs of post-deployment conditions. 18 Most prior studies have looked at utilization and costs among those with moderate to severe TBI or with TBI of mixed severity, without separating mild from more severe TBI. 12,17,19 –22 Two of these prior studies have reported utilization and cost data from veterans identified through the VHA TBI screening and evaluation program. 12,22 Our study confirmed that the majority of those identified as having symptoms following TBI through this program had mTBI. Therefore, even if individuals with moderate and severe TBI histories incur different healthcare costs per person than those with mild TBI, total costs associated with TBI in VHA will resemble the total costs of those with mTBI reported here and in these other two studies. This, however, does not take away from the possibility that per-person costs associated with mTBI may be different from per- person costs associated with moderate and severe TBI. Information specific to mTBI is needed because individuals with mTBI are clinically distinct from those with more severe TBI, 13 and because mTBI represents the vast majority of TBI cases, regardless of population (e.g., civilian and military). 5,6,11 Second, this is the first study to examine trends in VHA healthcare use and costs among veterans with TBI over a number of years. Prior research using VHA data has focused on the year following TBI screening, 12,22 which our data indicate is unique relative to future years. Specifically, we found that healthcare use and costs were greater in the year following screening than in the subsequent 2 years for all veterans who underwent TBI screening. This is likely a byproduct of the screening and referral processes triggered when veterans first access VHA services, and may reflect a pent-up need for care among veterans newly enrolled in VHA. Therefore, time since screening needs to be taken into consideration in efforts to describe typical patterns of utilization and costs of care among veterans screened for TBI.
Overall, we found that veterans with mTBI were high users of VHA outpatient healthcare, with an average of over 35 encounters in the 1st year following TBI screening, and approximately half as many total encounters in subsequent 2 years. The rate of use of inpatient services was also relatively high. More than three quarters of veterans with mTBI continue to use various types of VHA services over time, underscoring the importance of VHA care for this population, and the need to ensure capacity to meet these veterans' long-term healthcare needs.
Veterans with mTBI used more healthcare across a wide array of categories of care than veterans without mTBI in all 3 years. As expected, the observed trends in utilization were reflected in the costs of care. Mean healthcare costs for the 7318 veterans with mTBI were $12,045, $6,912, and $6,261 in years 1, 2 and 3 following screening, respectively, which brings the combined 3 year overall healthcare costs for mTBI veterans identified in 1 year to nearly $185,000,000. Importantly, the differences in utilization and costs were far greater when we compared veterans with mTBI with veterans who screened negative than when we compared veterans with TBI with those who screened positive but had TBI ruled out. Specifically, across all 3 years, average costs of care for veterans with mTBI were more than twice the costs for veterans who screened negative and ∼20% more than costs for those who screened positive but had TBI ruled out.
It is not surprising that there was less of a difference between those with mTBI and those who screened positive but had TBI ruled out. Veterans who screen positive for TBI have not only a history of exposure to potentially traumatic events but also current symptoms that are not specific to TBI. 11,23 That is, the TBI screen identifies symptomatic individuals and is known to have poor positive predictive value. 23 Those who screen positive but have TBI ruled out, therefore, also have health service needs that overlap with those of veterans who screen positive and then receive a mTBI diagnosis during the comprehensive TBI evaluation. Although this finding makes sense in light of how the VHA's TBI screening process works, it also underscores the importance of carefully selecting and characterizing a comparison group for research involving VHA patients diagnosed with mTBI. We would have derived different conclusions regarding the difference between groups had we combined veterans who screened negative for TBI with veterans who screened positive but had TBI ruled out into one no-TBI group.
We observed that a significant proportion of healthcare use and costs among veterans in the mTBI and the Screen+ No TBI groups was associated with mental health service utilization. The rate of mental health service use among those with mTBI far exceeded the rate of TBI specialty care. Other studies have reported on the high rates of mental health disorders among veterans and nonveterans diagnosed with TBI. 21,22,24 –26 The fact that both those with mTBI and the Screen+ No TBI group used mental health services at such high rates suggests that the TBI screening process may be identifying individuals with mental health service needs. Given that the VHA TBI screening tool identifies trauma exposure and current nonspecific symptoms, this is not surprising; other investigators have reported that the TBI screen identifies people with higher rates of psychiatric disorders, including post-traumatic stress disorder (PTSD). 27 It is interesting that the rates of mental health service use were even higher among those with mTBI than among those who screened positive but did not have TBI both in terms of proportion of mental health service users and the number of encounters. This finding echoes the observation in prior research that outpatient mental healthcare use is higher among veterans with both TBI and PTSD compared with veterans with PTSD alone. 28 Whether this reflects enhanced access to or increased need for mental health services among veterans with mTBI remains unknown. Regardless, the contribution of mental healthcare to total costs for veterans with mTBI demonstrates the importance of identifying efficacious approaches to addressing their mental health needs. Few studies have examined the effectiveness and costs of evidence-based mental health treatment among veterans with TBI, 29,30 and none have examined downstream effects on healthcare use and costs.
Strengths of this study include its longitudinal design and focus on those with diagnosed mTBI. This allowed us to determine that VHA healthcare use is high in the 1st year following screening relative to subsequent years and, therefore, should not be used in isolation to project future costs. However, we acknowledge the need to follow veterans with mTBI beyond 3 years to estimate healthcare needs and costs as this population ages. Another strength of this research is that we also included fee basis data, which is often not considered in examining VHA utilization and costs. A limitation is that we did not have information on healthcare use and costs that were not paid for by VHA. As of this writing, 39% of OEF/OIF/OND veterans were not using VA healthcare at all and many more were using both VHA and non-VHA healthcare. 31 With broader implementation of the Veterans Access, Choice, and Accountability Act, which allows veterans who are unable to schedule an appointment at a VHA facility within 30 days, live >40 miles from a VHA facility, or experience excessive challenges accessing a VHA facility, to receive care from eligible non-VA healthcare entities or providers, 32 the number and proportion of veterans using non-VHA healthcare may increase. Future research on healthcare use and costs among veterans with mTBI should also ascertain non-VHA healthcare use.
Although the growing body of evidence indicates that moderate to severe TBI should be managed as a chronic health condition, there has been more uncertainty regarding long-term needs of veterans with mTBI. 33 This study finds a high level of healthcare utilization and costs among veterans with mTBI over a 3 year period. Because mental healthcare needs appear to play a predominant role in the interdisciplinary care provided to veterans with mTBI, identifying and engaging patients with mTBI in effective mental health treatments should be considered a critical component of treatment planning.
Footnotes
Acknowledgments
Funding for the study was provided by the United States Department of Veterans Affairs, Office of Research and Development, Health Services Research & Development Service (HSR&D), Washington, DC through a locally initiated project grant (#PLY 05-2010-2) from the Polytrauma and Blast-Related Injuries (PT/BRI) Quality Enhancement Research Initiative (QUERI). The funding source had no role in the study design, analysis, interpretation of the data, writing of the article, or decision to submit the article for publication. Preliminary results related to this article were presented at the VA HSR&D Annual Meeting July 8–10, 2015, in Philadelphia, PA.
Author Disclosure Statement
All authors of this manuscript report no conflicts of interest other than employment within the Department of Veterans Affairs. The views expressed herein do not necessarily represent the views of the Department of Veterans Affairs or the United States Government.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.