
Abstract
The effectiveness of cerebrospinal fluid (CSF) drainage in lowering high intracranial pressure (ICP) is well established in severe traumatic brain injury (TBI). Recently, however, the use of external ventricular drains (EVDs) and ICP monitors in TBI has come under question. The aim of this retrospective study was to investigate the effect of CSF drainage on brain tissue oxygenation (PbtO2). Using a multi-modality monitoring system, we continuously monitored PbtO2 and parenchymal ICP during CSF drainage events via a ventriculostomy in 40 patients with severe TBI. Measurements were time-locked continuous recordings on a Component Neuromonitoring System in a neuroscience intensive care unit. We further selected for therapeutic CSF drainage events initiated at ICP values above 25 mm Hg and analyzed the 4-min periods before and after drainage for the physiologic variables ICP, cerebral perfusion pressure (CPP), and PbtO2. We retrospectively identified 204 CSF drainage events for ICP EVD-opening values greater than 25 mm Hg in 23 patients. During the 4 min of opened EVD, ICP decreased by 5.7 ± 0.6 mm Hg, CPP increased by 4.1 ± 1.2 mm Hg, and PbtO2 increased by 1.15 ± 0.26 mm Hg. ICP, CPP, and PbtO2 all improved with CSF drainage at ICP EVD-opening values above 25 mm Hg. Although the average PbtO2 changes were small, a clinically significant change in PbtO2 of 5 mm Hg or greater occurred in 12% of CSF drainage events, which was correlated with larger decreases in ICP, displaying a complex relationship between ICP and PbtO2 that warrants further studies.
Introduction
P
While ventricular fluid coupled ICP monitoring remains the gold standard of ICP measurements, the introduction of intraparenchymal intracranial monitoring (IPM) devices has provided institutions with a less invasive monitoring system with a lower rate of device complications, including hemorrhage and infection.
Kasotakis and colleagues 1 reviewed 377 traumatic brain injury (TBI) patients who were treated with either external ventricular drains (EVDs) or parenchymal ICP monitors and concluded that device selection did not affect neurologic outcome. Further, unless CSF drainage is deemed necessary, it was recommended to routinely place IPM devices in adult TBI patients because of the associated complication rates with EVDs and longer intensive care unit (ICU) length of stay. 1
The major advantage of EVDs over IPMs is the ability to provide a therapeutic maneuver by draining CSF, especially in cases of refractory ICP. 2 While CSF drainage is a validated tool in decreasing ICP values, there is no consensus as to its utility in improving other parameters of cerebral perfusion, such as cerebral oxygenation. The aim of this study was to study the effect of CSF drainage on brain tissue oxygenation (PbtO2) using multi-modality monitoring in traumatic brain-injured patients.
Methods
Patient population
From 2014 to 2016, patients with severe TBI admitted to the University of New Mexico Hospital (UNMH), a Level I trauma center, who underwent invasive neuromonitoring were eligible for this study. Patients were identified retrospectively from a prospective observational database with institutional review board approval. Inclusion criteria was patients >16 years of age who sustained TBI and had a Glasgow Coma Scale score of less than 8 post-resuscitation requiring placement of invasive intracranial monitoring.
Monitoring
Patients with TBI who require intracranial monitoring are admitted to the neurosurgical ICU (NSICU). Blood pressure is measured with an arterial line and a cool guard central line is placed for core temperature control. For invasive neuromonitoring, the Hummingbird Synergy system is used, which allows placement of an external ventricular catheter to facilitate CSF drainage and ventricular ICP monitoring. The Hummingbird Synergy system also allows for parenchymal ICP monitoring, as well as placement of a Licox probe (Integra, Plainsboro, NJ), which measures PbtO2. All monitors are placed at bedside in the NSICU through a frontal burr hole using a twist drill. Monitoring systems are typically inserted into non-dominant frontal lobe to minimize the effect of hemorrhagic complications. The Licox probe is inserted into white matter at approximately 2 cm from the skull. The Licox probe is subjected to oxygen challenges by increasing the ventilator FiO2 to 100%. Non-functioning Licox probes are typically removed from the patient and any data collected from non-functioning probes before removal were not included in the study. All monitors are confirmed post-placement by a computed tomography scan. All physiological data are collected on a Component Neuromonitoring System (Moberg Research, Inc., Philadelphia, PA).
Management of ICP
For sustained high ICP (i.e., greater than 20 mm Hg for longer than 10 min), the EVD is opened to drain for 10 min and then re-clamped. If ICP remains greater than 20 mm Hg, the EVD is kept open at 20 cm H2O with parenchymal ICP recorded continuously and ventricular ICP checked hourly. Other goals include appropriate sedation and analgesia with fentanyl and propofol, an Na goal of 145-160 mEq with the use of 3% Na, as well as a PaCO2 goal of 35-38 mm Hg with hyperventilation (PaCO2 < 35) being avoided in the first 24 h. EVDs have CSF drawn twice a week for CSF analysis to monitor for infection.
A PbtO2-directed therapy is not standard protocol in the NSICU at UNMH. However, critically low PbtO2 initiates FiO2 challenges to ensure a working Licox probe. While a specific number is not targeted, Licox values do play into the daily decision-making of the critical care team to optimize brain tissue perfusion and oxygenation.
Data collection
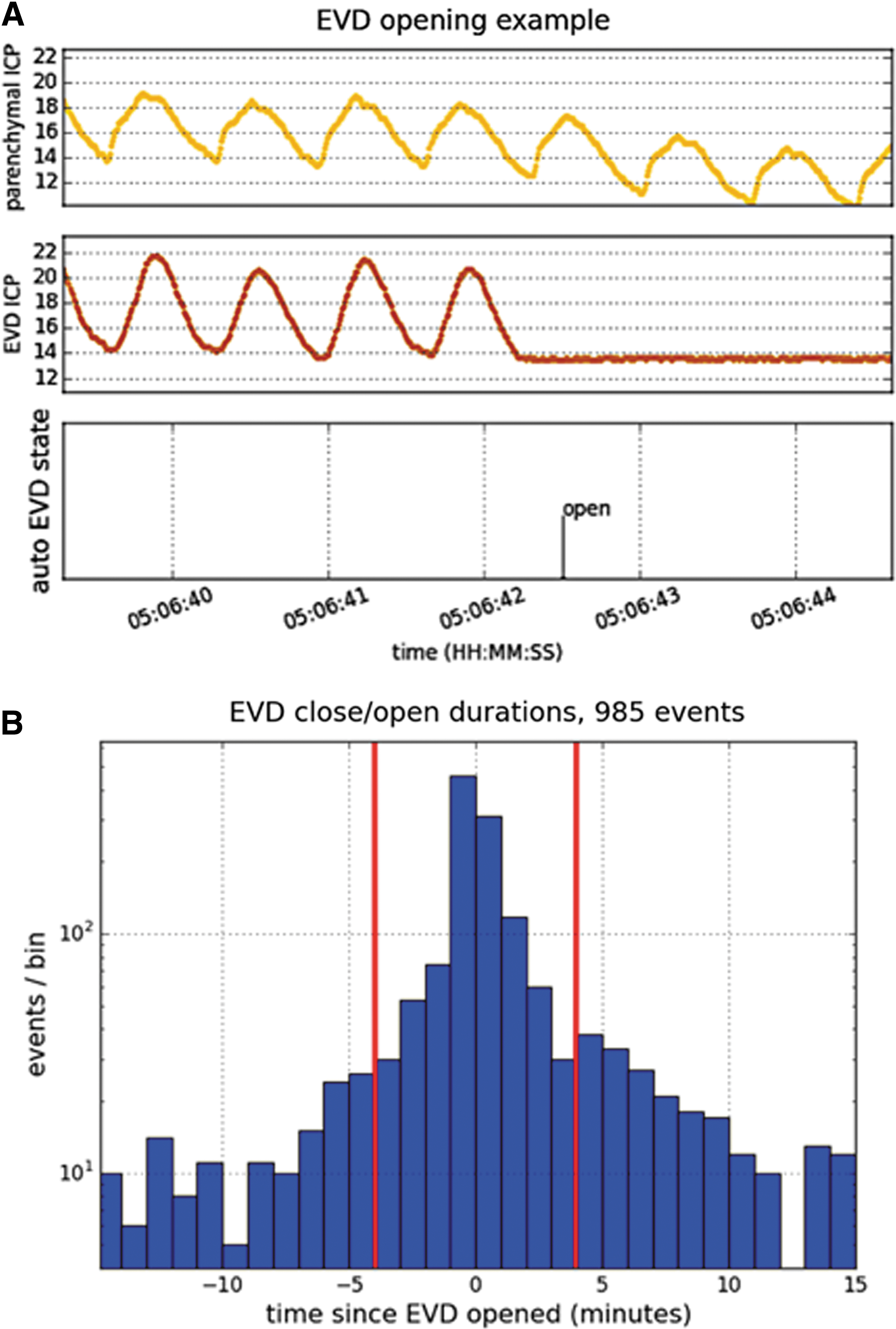
Parenchymal ICP, ventricular ICP and cerebral perfusion pressure (CPP) data were collected at 120 Hz. PbtO2 was collected at 0.5 Hz. At the moment the EVD is opened, the ventricular ICP waveform signal becomes a flat line, making it possible to search the ventricular waveform for opening events (Fig. 1A). Having identified all EVD openings and closings automatically, it is possible to observe the effect of CSF drainage on parenchymal ICP and PbtO2 for a continuously maintained EVD state. For automated analysis of ICP and PbtO2 data before and after drainage events, a duration time cut was imposed, both pre– and post–EVD opening. The time distribution of the opening and closing of the EVD showed that a reasonable number of events for analysis would be obtained if a 4-min window was chosen before and after the opening of the EVD as shown in Figure 1B, which is the basis for the short period of data acquisition during CSF drainage.
The data were further filtered by reviewing the PbtO2 waveforms for changes caused by ventilator setting changes. FiO2 can be increased to 100% for endotracheal suction or to challenge the Licox probe, which could bias the effects of CSF drainage on PbtO2 if it occurred during or within the analyzed minutes of the drainage event. To eliminate such events, changes in PbtO2 around drainage events were reviewed to delete those recordings from the analysis. Statistical analysis was done by Graphpad Prism version 6.0 by repeated measures one-way analysis of variance followed by paired Student's t-test with a significant p value of 0.05 and Bonferroni correction (0.05/n).
Results
From 2014 to 2016, 49 patients were identified retrospectively. Nine patients were excluded because of lack of ICP data. Forty patients had sufficient ICP data and at least one CSF drainage event to be further analyzed. Of the 40 patients, 30 were male and 10 were female. The average age was 39 years with a range of 16 to 75 years. Seventeen more patients were excluded because CSF drainage only occurred during ICP values less than 25, which could be due to routine CSF sampling or to check patency of the drain during morning examinations. In 23 patients, 204 therapeutic CSF drainage events were initiated at ICP values above 25 mm Hg. During the 4 min of opened EVD and subsequent CSF drainage, ICP decreased by 5.7 ± 0.6 mm Hg. CPP increased by 4.1 ± 1.2 mm Hg, while PbtO2 increased by 1.15 ± 0.26 mm Hg. These results are summarized in Table 1.
ICP, intracranial pressure; CPP, cerebral perfusion pressure; PbtO2, brain tissue oxygenation; CSF, cerebrospinal fluid; ICP, cerebral perfusion pressure; EVD, external ventricular drain.
Graphic plots of the time course of changes in ICP, CPP, and PbtO2 for all patients are shown in Figure 2. While the average changes in PbtO2, ICP, and CPP were relatively small, highly significant changes occurred in all variables relative to the time of EVD opening, showing an increase in PbtO2, a decrease in ICP, and an increase in CPP. The median ICP before opening of the EVD was 28.4 mm Hg. In 51 CSF drainage events (29%), the PbtO2 was equal to or less than 15 mm Hg. In 21 events (12%), the PbtO2 showed larger clinically significant changes of 5 mm Hg or greater. The 12% of drainage events that showed an increase in PbtO2 of 5 mm Hg or greater were distributed among nine patients in whom the average age was 29 years.

Data for all patients.
Figure 3 displays a linear regression of the delta in PbtO2 during all CSF drainage with three other variables: delta ICP, starting ICP, and starting PbtO2 during CSF drainage. Figure 3A shows a significant inverse correlation between the changes in PbtO2 and the changes in ICP during CSF drainage events, with larger improvements in PbtO2 as the ICP improves. Figure 3B and Figure 3C displays no significant correlation between the changes in PbtO2 with starting PbtO2 values or starting ICP values, respectively, during CSF drainage events. Overall, the most important variable in determining the magnitude of change in PbtO2 during CSF drainage is the magnitude of the drop in ICP during that drainage event.
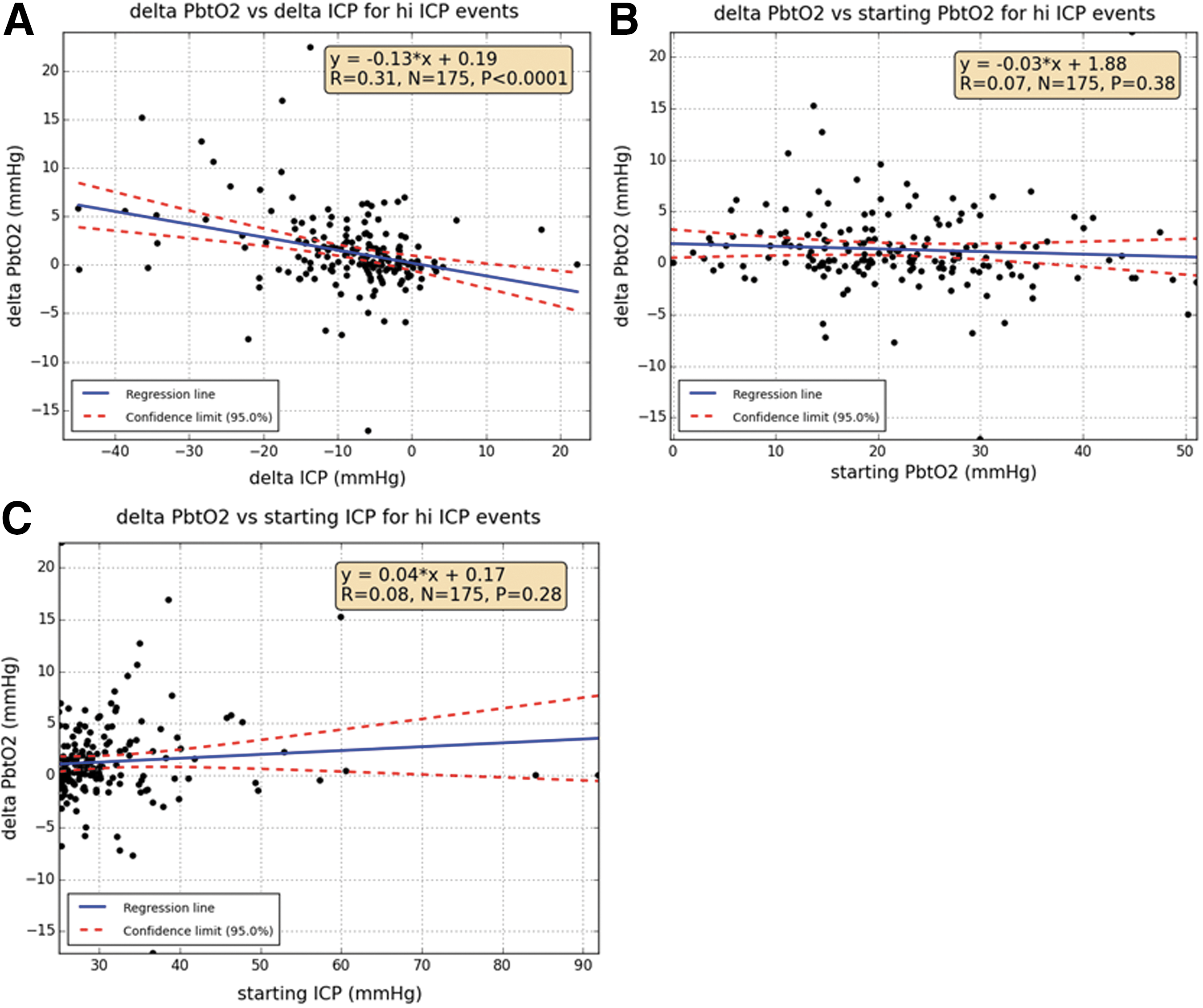
Regression lines for 175 cerebrospinal fluid (CSF) drainage events, in patients with elevated intracranial pressure (ICP), with the y-axis being change in brain tissue oxygenation (PbtO2) plotted against three variables:
Discussion
CSF drainage via ventriculostomy has been shown to be an effective therapy in lowering ICP. 3 However, its effect on other parameters of cerebral perfusion has been less straightforward. Kinoshita and colleagues found that CPP management by CSF drainage may decrease the total infusion volume of crystalloid potentially decreasing the risk of brain edema caused by excessive fluid resuscitation. 4
Kerr and colleagues reported on 58 patients and 142 CSF drainage events, which revealed a significant reduction in ICP and increase in CPP. 5 However, only two patients had improved cerebral oxygenation or flow velocity, concluding that lowering of ICP specifically by CSF drainage was not associated with improvement in cerebral blood flow velocity (CBFV) or oxygenation as measured by global indices.
With the Hummingbird Synergy multi-modality system, the authors were in a unique position to quantify the change in ICP in real time during CSF drainage because of the dual parenchymal and ventricular ICP monitoring system, as well as the effect of CSF drainage on PbtO2. Continuous parenchymal intracranial pressure monitoring showed a significant decrease in ICP with CSF drainage during episodes of elevated ICP in TBI patients. As expected, CPP, which is mean arterial pressure minus ICP, also showed a significant increase with CSF drainage during episodes of elevated ICP in TBI patients. Both parameters show worsening values leading up to the drainage event. (Table 1; Fig. 2)
PbtO2 also showed worsening values before CSF drainage during increasing ICP values. After CSF drainage, PbtO2 showed a statistically significant increase of 1.15 mm Hg (Table 1). While an average change of 1.15 mm Hg in PbtO2 is not clinically significant, approximately 12% of drainage events resulted in a PbtO2 increase of 5 mm Hg or more. Larger decreases in ICP during CSF drainage appear to correlate with larger changes in PbtO2, as indicated by the linear regression models in Figure 3. Starting ICP and starting PbtO2 levels did not correlate with changes in PbtO2.
We hypothesize that improvements in absolute pulse amplitude, which are seen in our study during CSF drainage events in the parenchymal ICP pressure waveforms, indicate improvement in brain compliance and subsequently cerebral perfusion. Thus, the magnitude of change in ICP during CSF drainage directly affects the decrease in pulse amplitude, improvements in brain compliance, and ultimately the increase in PbtO2.
In our study, patients who had a larger increase (> 5 mm Hg) in PbtO2 with CSF drainage were on average younger TBI patients. This could be because older patients typically have atrophic changes allowing for more space intracranially than their younger TBI counterparts, making them more susceptible to cerebral edema and increases in ICP. Future studies are needed to identify the subset of patients or even time courses in TBI patients that yield a larger increase in PbtO2 with CSF drainage, as they most likely represent a type of TBI patient who is exquisitely more sensitive to shifts in ICP.
Significant literature exists indicating an association with improved outcomes in TBI patients when using a PbtO2-directed therapy. 6 –9 Nangunoori and colleagues published a systematic literature review of PbtO2-based therapy and outcome that reviewed four major papers. 10 In two of those articles, parenchymal ICP monitors were used solely, 6,7 and in the third article, 22% of patients received a ventriculostomy. 8 In the fourth article, written by Spiotta and colleagues, CSF drainage is listed as an ICP-lowering technique and a subsequent PbtO2-elevating strategy that was less frequently used. 9
While CSF drainage is widely accepted as a method to lowering ICP and an intermediate step before more aggressive measures such as decompressive craniectomy, the literature has no consensus on its role in PbtO2-guided therapy in managing traumatic brain injury or other markers of cerebral perfusion. There appears to be a complex relationship between ICP and PbtO2.
Limitations
Limitations of this study include its retrospectively reviewed data. We identified time points when the EVD was opened by reviewing the ventricular ICP pattern, which is flat during the open phase. However, this encompasses opening events that may not have been used for therapeutic drainage, such as CSF sampling events. In addition, there are numerous confounding variables that made analysis difficult to interpret with regard to changes in PbtO2 in relation to EVD opening. Changes in ventilator parameters, such as increases in FiO2 to either challenge the Licox or as standard respiratory therapy intervention, were not clearly marked on the PbtO2 timeline, introducing numerous outliers that were addressed in the data but most certainly biased the final results positively and negatively if they occurred near the CSF drainage event. A prospective study documenting the rationale for EVD opening, duration of EVD opening, amount of CSF being drained, and changes in ventilation, specifically the FiO2, would better quantify CSF drainage events and its relationship to PbtO2, as well ICP.
Conclusion
The Benchmark Evidence from South American Trials: Treatment of Intracranial Pressure trial, focused on maintaining monitored ICP pressure at 20 mm Hg or below, did not prove to be superior to non-ICP monitored care in TBI patients. 11 But the authors of this article believe that traumatic brain injury encompasses a multitude of pathologies yet to be fully understood and potentially treated. Further, the ability to monitor ICP and introduce therapeutic challenges in the form of CSF drainage has given us insight into part of the pathophysiology of TBI.
In traumatic brain injured patients with elevated ICP, CSF drainage remains an effective tool in lowering ICP and raising CPP. On average PbtO2 showed a small but significant increase with CSF drainage in patients with high ICPs. There are patients with clinically meaningful changes in PbtO2 with CSF drainage that appear to be correlated to the magnitude of change in ICP during those drainage events.
Footnotes
Author Disclosure Statement
No competing financial interests exist.