
Abstract
Previous studies have indicated that there is no consensus about management of mild traumatic brain injury (mTBI) at the emergency department (ED) and during hospital admission. We aim to study variability between management policies for TBI patients at the ED and at the hospital ward across Europe. Centers participating in the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) study received questionnaires about different phases of TBI care. These questionnaires included 71 questions about TBI management at the ED and at the hospital ward. We found differences in how centers defined mTBI. For example, 40 centers (59%) defined mTBI as a Glasgow Coma Scale (GCS) score between 13 and 15 and 26 (38%) defined it as a GCS score between 14 and 15. At the ED various guidelines for the use of head computed tomography (CT) in mTBI patients were used; 32 centers (49%) used national guidelines, 10 centers (15%) local guidelines, and 14 centers (21%) used no guidelines at all. Also, differences in indication for admission between centers were found. After ED discharge, 7 centers (10%) scheduled a routine follow-up appointment, whereas 38 (54%) did so only after ward admission. In conclusion, large between-center variation exists in policies for diagnostics, admission, and discharge decisions in patients with mTBI at the ED and in the hospital. Guidelines are not always operational in centers, and reported policies systematically diverge from what is recommended in those guidelines. The results of this study may be useful in the understanding of mTBI care in Europe and show the need for further studies on the effectiveness of different policies on outcome.
Introduction
T
Among the patients with TBI presenting at the ED, the large majority (75–90%) are classified as having “mild” TBI (mTBI). The most frequently used definition of mTBI is a Glasgow Coma Scale (GCS) score between 13 and 15 and loss of consciousness of less than 30 min or amnesia not extending beyond 24 h after blunt head injury. 3,4 Because of the low risk of intracranial damage, a computed tomography (CT) scan of the head or hospital admission is not always necessary in these patients. To estimate the risk of intracranial abnormalities in mTBI, various prediction rules and guidelines have been developed, for example, the Canadian CT head rule, the National Institute for Health and Care Excellence (NICE) guidelines for head injury, and the CT in Head Injury Patients (CHIP) rule. 5 –8 Based on a set of minor and major risk factors, these prediction rules recommend whether a CT scan of the head should be performed. The results of the CT scan subsequently influence the decision on whether a patient should be admitted to the hospital or could be safely discharged home.
After mTBI, patients may experience post-traumatic symptoms such as headaches, dizziness, and memory or concentration problems, resulting in significant disability. In many cases these symptoms dissolve over time; however, a group of patients (estimated at between 5 and 30%) may suffer from prolonged symptoms. 9 Studies have shown that handing out discharge information and scheduling routine follow-up sessions could reduce these post-traumatic symptoms. 10,11
However, still little is known about the optimal treatment of mTBI and there is no consensus about management of these patients. 12 Therefore, variation in structure and process of mTBI care is expected, which may result in variation in outcome. In this study, we aimed to describe the current management of mTBI at the EDs and hospital wards in Europe. Specifically, we aimed to provide insight in the use of diagnostics, admission policy, and discharge policy at the ED and hospital ward.
Methods
Questionnaires
Between 2014 and 2016, we approached the principal investigators of 71 centers from 19 European countries and Israel, participating in the CENTER-TBI (Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury) study, a multicenter prospective observational study on TBI, 13 with the request to complete a set of 11 questionnaires about structure and process of care for TBI patients: The Provider Profiling (PP) questionnaires. The questionnaires were developed based on literature and expert validation and were subsequently pilot-tested. Questionnaires were discussed during presentations, workshops, and email conversations. Reliability, which was assessed by calculating concordance rates between duplicate questions (5% of the questions) in all 11 questionnaires, was adequate (median concordance rate of 0.85). More detailed information about the development, administration, and content of the total set of PP questionnaires is available in a previous publication. 14
For this study, we analyzed the results of a questionnaire about ED and a questionnaire about hospital admission policy, for a total of 71 questions (Supplementary Appendix 1; see online supplementary material at
Question formats and definitions
Most questions had a multiple choice format where one or more answers could be selected. Two questions had an open format. Questions addressed structures (e.g., “Is overnight observation at the ED available for patients with TBI?”) and processes (e.g., “Are guidelines or protocols used to decide when mTBI patients are discharged from the ED?”). The questions about processes refer to general policies rather than individual treatment preferences. General policy was defined as the way the majority of patients with a certain indication would be treated (>75%).
Statistical analysis
We used standard descriptive statistics. Categorical variables were presented as frequencies and percentages and continuous variables were presented as medians and interquartile ranges (IQR). Analysis was performed using IBM Statistical Package for Social Sciences (SPSS) version 21.
Results
All 71 centers completed the Hospital admission questionnaire and 68 centers completed the ED questionnaire (response rates 100% and 96%, respectively). Among the centers that did not complete the ED questionnaire, three centers (4%) indicated that their center had no ED because they specialized in severe neurotrauma or collaborated with the ED of another hospital. The questionnaires were answered by ED physicians, neurosurgeons, neurologists, intensivists, and administrative staff members. The majority of participating centers were academic (n = 65; 92%), level 1 trauma centers (n = 48; 68%) situated at an urban location (n = 70; 99%).
Classification of TBI
It appeared that different definitions of severity levels for TBI were used (Table 1). Forty centers (59%) defined mTBI as a GCS score between 13 and 15 and 26 centers (38%) as a GCS score between 14 and 15. Moderate TBI was considered a GCS score between 9 and 12 in 38 centers (56%) and 9 and 13 in 22 (32%). The majority of the centers considered severe TBI as a GCS score between 3 and 8 (n = 62; 91%).
The responders were asked to enter the lowest and highest GCS score per TBI group; the bold GCS range represents the range most common in the literature.
GSC, Glasgow Coma Scale; TBI, traumatic brain injury.
Diagnostics at the ED
ED physicians (n = 35; 49%) and neurosurgeons (n = 15; 21%) were most often in charge of the treatment of TBI patients at the ED. At the ED, various rules or guidelines for the use of head CT in patients with mTBI were used: more than half of the centers used multi-nation guidelines, such as the NICE-guidelines (n = 16; 24%), the Scandinavian guidelines (n = 7; 10%), or other inter-nation guidelines (n = 12; 17%).
15
Only a few of the centers used prediction rules such as the Canadian CT Head rule (n = 4; 6%), the New Orleans criteria (n = 1; 1.5%), or the CHIP rule (n = 4; 6%).
16
In addition, 10 centers (15%) used other local guidelines and 14 centers (20.5%) used no guidelines at all. More than 90% (n = 62) of the centers considered their CT scanning policy liberal. Most centers (n = 45; 66%) stated they are more restrictive in the use of a CT scan in children compared with adults. CT scans at the ED were mostly ordered by ED physicians (n = 37; 54%) and neurosurgeons (n = 16; 24%). Only in 7% of the centers (n = 5, including 4 centers from The Netherlands) do neurologists order the CT scans. Most centers standardly perform a CT scan in patients with clinical signs of skull base fracture, any neurological deficit, or a seizure (Fig. 1). In some situations the indication for CT differs among centers. For example, 50 centers (74%) standardly use a CT scan in patients on anticoagulant therapy, whereas 15 (22%) indicated that they would do this often. The CT scanning guidelines were mainly implemented by written protocols and algorithms (n = 38; 56%) or via verbal direction from senior doctors in 22 centers (32%, Supplementary Table 1; see online supplementary material at
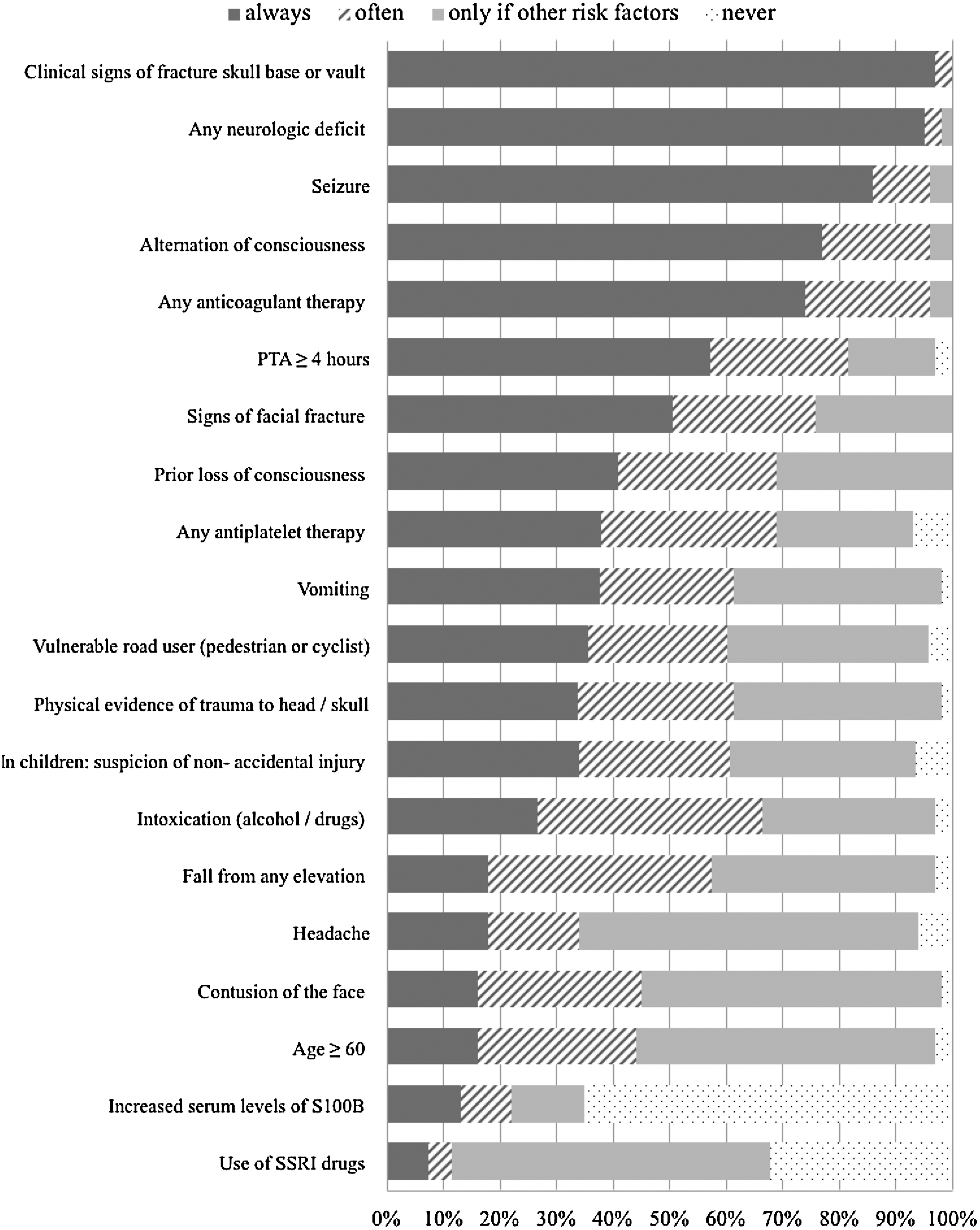
Frequency of ordering head computed tomography (CT) scan in patients with mild traumatic brain injury (mTBI), by clinical indication. Per situation the responders had to choose the correct policy for their center: always/general policy: if the situation is, in general, a reason for ward admission in your hospital. This must represent a general consensus among colleagues, rather than individual preference; often/partial: the situation is often seen as a reason for ward admission in your hospital. However, it is not general practice, because not everyone in your hospital agrees or admission is only general policy in a subset of the patients; only in the presence of other risk factors: if the situation is never solely a reason for ward admission, but it might be a reason in combination with one or more other risk factors; never: if the situation is never the only reason for ward admission. PTA, post-traumatic amnesia.
Magnetic resonance imaging (MRI) was used in addition to the CT scan if there was discrepancy between clinical symptomatology and presence of CT abnormalities in mTBI patients (75% of the centers). In 6 centers (9%) from Austria, Denmark, Spain, Sweden, and United Kingdom, s100B is routinely determined as a prognostic biomarker for neurological deterioration. Many centers had the availability of overnight observation at the ED for patients with TBI before they were discharged (n = 54; 79%).
Admission at the ward
At the hospital ward, neurosurgeons (n = 56; 79%) were most often in charge of the treatment of TBI patients. Forty-four (65%) centers indicated use of guidelines in the decision on whether mTBI patients should be admitted to the hospital ward. Most centers admitted patients with TBI to the neurosurgical ward (n = 53; 75%). In addition, patients with TBI were routinely admitted to the neurology (n = 16; 23%) or surgery (n = 15; 21%) ward. Patients with cerebrospinal fluid (CSF) leak, CT progression, new CT abnormalities, or shock were standardly admitted to the ward. For other admission indications, the policy was more diverse. For example, 25 centers (37%) indicated that patients with pre-injury anticoagulation were routinely admitted to the ward, whereas 27 centers (39%) indicated that they would only admit these patients to the ward if other risk factors are present (Fig. 2).
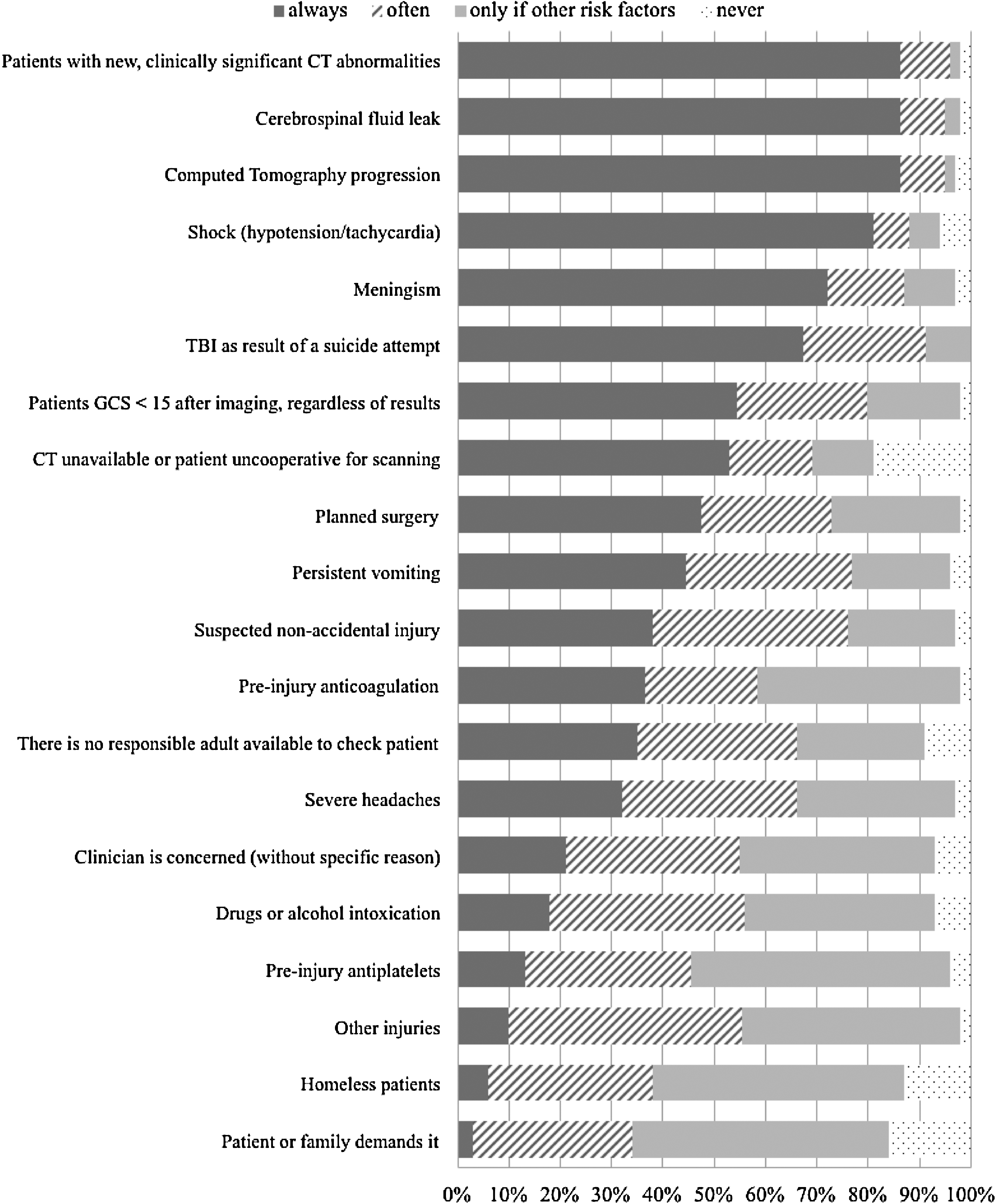
Frequency of ward admission of patients with mild traumatic brain injury (mTBI), by clinical indication. Per situation the responders had to choose the correct policy for their center: always/general policy: if the situation is, in general, a reason for ward admission in your hospital. This must represent a general consensus among colleagues, rather than individual preference; often/partial: the situation is often seen as a reason for ward admission in your hospital. However, it is not general practice, because not everyone in your hospital agrees or admission is only general policy in a subset of the patients; only in the presence of other risk factors: if the situation is never solely a reason for ward admission, but it might be a reason in combination with one or more other risk factors; never: if the situation is never the only reason for ward admission. CT, computed tomography.
When patients are admitted at the ward, GCS is assessed systematically to detect neurological deterioration. About half of the centers (n = 37; 52%) used the scheme every “half-hour for 2 hours, then hourly for 4 hours, then every 2 hours,” thus in accordance with the NICE guidelines. The other half of the centers had another frequency of GCS assessment, ranging from hourly to every 24 h. In 11 centers (16%) the Galveston Orientation and Amnesia Test (GOAT), a test for post-traumatic amnesia (PTA), is systematically used at the ward and 12 centers (17%) use another form of PTA assessment.
Fifty-three centers (75%) have step-down beds for patients who no longer need intensive care unit (ICU) care but are also not well enough for a routine hospital ward. At these high-care wards, neurosurgeons (n = 32; 60%) and intensivists (n = 13; 25%) were most often in charge of the patients. Reasons for admission to the high-care wards in isolated patients with TBI included decreased consciousness level (n = 48; 68%), to monitor vital functions (n = 45; 63%), frequent GCS assessments (n = 38; 54%), confusion (n = 35; 49%), and intracranial complications (n = 32; 45%).
Treatment
Fifty-four centers (79%) state that they reverse pre-injury oral anticoagulation use if CT abnormalities are present, 46 (68%) do so if surgery was considered and 2 (3%) centers reverse anticoagulation in all patients admitted to the ward. Anticoagulation was commonly reversed with vitamin K (n = 62; 91%) or prothrombin complex concentrate (n = 55; 81%). Other treatments mentioned in this context were: fresh frozen plasma (FFP; n = 47; 69%), platelets (n = 40; 59%), fibrinogen (n = 20; 29%), and recombinant factor VII (n = 11; 16%).
If TBI patients have a CSF leak (with possibly an increased risk of infections), 34 of the centers (48%) would employ a strategy of watchful waiting before they start treatment with antibiotics. In contrast, 26 centers (37%) start antibiotics immediately and 9 (13%) start antibiotics only if patients have a fever.
TBI patients with an early seizure (a post-traumatic seizure occurring within 7 days of the trauma) receive anti-epileptic drugs (AEDs) immediately in 39 centers (55%). About one third (n = 22) start AEDs only in patients with CT abnormalities and an early seizure, and 7 centers (10%) never start AEDs in TBI patients with early seizure. Additionally, there are differences in the use of anti-seizure prophylaxis in patients with specific characteristics (Supplementary Fig. 1; see online supplementary material at
Discharge information
In 38 centers (56%) guidelines are used to decide whether patients with mTBI could be discharged from the ED. In 54 centers (79%) printed discharge information is available in the ED and hospital ward to hand out to patients who are discharged home. After discharge from the ED, 42 centers (62%) provide information about post-traumatic symptoms verbally, whereas 55 centers (78%) do so after discharge from the hospital ward. Overall, more information is provided verbally than in written form (Table 2).
ED, emergency department.
Follow-up policy
A routine follow-up appointment at the outpatient clinic is scheduled in 7 centers (10%) after discharge from the ED, at a median period of 4 weeks after discharge (IQR 2.5–6). After discharge from the hospital ward, 38 centers (54%) routinely schedule a follow-up appointment at a median period of 6 weeks (IQR 4–7.8). In 16 centers (24%) patients are referred to the general practitioner, regardless of persisting symptoms. In case of persisting symptoms, the patients are advised to go back to the general practitioner (ED, n = 30, 44%; and ward, n = 17, 24%) or hospital (ED, n = 34, 50%; and ward, n = 24, 34%).
Discussion
This study provides a broad overview of the current care for mTBI patients in Europe and shows that there are wide between-center variations in diagnostic, admission, and discharge policies. The most striking findings are the large variation in GCS scores that are considered a specific TBI severity, the use of CT guidelines, and policies for patients on anticoagulants. We also found large variation in follow-up policy after discharge, where the majority of patients are not receiving routine follow-up, despite the existing evidence and guidelines for TBI.
Our findings are in line with previous research. For example, in 2001 De Kruijk and colleagues 17 performed a survey study in 67 European centers. They also reported a lack of consensus of mTBI management (e.g., definitions, guidelines) in Europe at the ED and at hospital admission. Pulhorn and associates 18 investigated management of mTBI at 19 hospital wards in Britain and also found variation in the assessment of GCS at the ward and in discharge recommendations. Our study confirms results of Stern and co-workers, 19 ; they performed a survey study at the ED in 72 centers in New England and found significant variability in the use of guidelines and management of mTBI care as well.
What this study adds to previous research is that it shows that not only are guidelines not always operational in centers, but also that actual policies systematically diverge from what is recommended in those guidelines. Audits to check for adherence to the guidelines could give more insight into this, but the majority of the centers have not performed audits in the last 5 years. Moreover, our survey pinpoints areas of clinical controversy, which could do well with more clinical research.
In recent years the use of prognostic biomarkers such as s100B has been studied extensively. 20,21 The Scandinavian guidelines for mTBI even incorporated s100B in their CT scan recommendations. 22 However, in our study we observed that s100B is used as a prognostic biomarker in only 6 centers, of which 3 centers are Scandinavian.
Future research is needed to investigate whether the variation in guideline use and policies is associated with outcomes. Currently, all the participating centers are collecting patient outcomes data for the CENTER-TBI study. 13 By combining current data with data on patient outcomes, we will be able to investigate whether between-center differences in policy are associated with patient outcomes, and subsequently explore the effectiveness of different policy strategies in comparative effectiveness research (CER). CER requires variation to study effectiveness of treatments or policies by comparing centers that routinely perform an intervention with centers that do not, or that at least do so less frequently. 12 In our study we found large between-center differences that enable further study with CER approaches. For example, we can compare centers that routinely perform follow-up at the outpatient clinic, with centers that do not routinely perform follow-up and analyze the relation with outcome. And we can compare the effects of routinely giving platelets to patients on antiplatelet drugs, a procedure that has been associated with poor outcomes in spontaneous intracerebral hemorrhage (ICH), but has not been studied in TBI. Thus, in the CER context, we are actually satisfied with the observed variation in care because this provides the opportunity to compare outcomes between centers with different treatment policies.
This study has some limitations that should be taken into account when interpreting the data. The reliability of the results depends on the interpretation and willingness of the investigators to be truthful and transparent in their answers. We tried to enhance this by explicitly asking for general policy rather than individual preferences and explained all answer options carefully. Further, because the majority of participating centers were academic level 1 trauma centers, the findings might not be generalizable to centers with a lower trauma center designation. However, we believe the variation in policies will only increase when also lower trauma center designations are included.
Conclusion
Large between-center variations exist in policies for diagnostics, admission, and discharge decisions in patients with TBI at the ED and at the hospital ward. The results of this study may be useful in the understanding of TBI care in Europe and show the need for further studies on the effect of different policies on patient outcomes.
Footnotes
Acknowledgments
The authors would like to thank all the CENTER-TBI participants for completing the PP questionnaires. Data used in this article were obtained in the context of the CENTER-TBI study with support of the European Commission 7th Framework program (602150).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.