
Abstract
Neurogenic shock, a distributive type of circulatory shock after spinal cord injury (SCI), results in profound hypotension. The consequent hemodynamic instability complicates clinical management, delays surgical intervention, and impacts neurological outcome. Moreover, the reported incidence of this condition varies significantly. We establish the true incidence of neurogenic shock by comparing the most common clinical definitions used to diagnose the condition. Further, we characterize the acute progression and recovery of neurogenic shock. Daily blood pressure, heart rate, and fluid management as well as vasopressor therapy and neurologic status were collected over 30 days from 84 adults admitted to our tertiary trauma center after cervical (n = 56) and thoracic (n = 28) SCI. We found that the reported incidence of neurogenic shock varied greatly depending on which clinical definition was applied. By using a novel combination of hemodynamic and laboratory criteria to define neurogenic shock, the calculated incidence (29% cervical SCI) in our sample most appropriately reflects the true incidence, finding that hypovolemia was the primary factor responsible for the inconsistency in incidence reports between studies. In addition, we found a characteristic decline in blood pressure after the first week post-injury and that fluid management is not currently an integral aspect of clinical management (all persons were treated at a net fluid intake ≤ zero). The results demonstrate the need for accurate identification of neurogenic shock through consistent and appropriate criteria, which is not only important from a clinical point of view, but also in establishing accurate epidemiology to responsibly allocate resources to its management.
Introduction
N
To date, the reported incidence of neurogenic shock after SCI largely has been inconsistent. For example, reports indicate that after cervical SCI, the incidence of neurogenic shock can range from 14–44% depending on the criteria used. 3,5 Previous studies have identified neurogenic shock with a systolic blood pressure (SBP) as low as <90 mm Hg and heart rate (HR) of <50 beats per minute (bpm), while more recent studies have used a SBP of <100 mm Hg and a HR of <80 bpm, likely accounting for some of the variability in the literature. 6,7 In addition to discrepancies in the hemodynamic parameters, however, persons with SCI are more vulnerable to hypovolemia because they may not be able to generate reflex arterial vasoconstriction or tachycardia. 3 As such, neurogenic shock cannot be completely ruled out in a person with hypovolemia.
Accordingly, hypovolemic shock, a life-threatening condition resulting from a loss of more than 20% of the body's blood volume, is a significant confounder of neurogenic shock. 8 Because accurate estimation of the epidemiology of neurogenic shock is critical clinically to responsibly allocate resources to its management, we chose to account for hypovolemia by incorporating a key indicator of contracted volume in our operational definition. 9 This is in contrast to others 5,6,10 who have used signs of hemorrhage to simply exclude participants from their analyses.
From a rehabilitative point of view, neurogenic shock is particularly problematic. The severe hypotension of neurogenic shock is likely to result in hypoperfusion of microvessels within the spinal cord, leading to ischemia and a more pronounced secondary injury, decreasing the potential for partial recovery of neurological function. 3,11 –13 Therefore, management of neurogenic shock after acute SCI has focused on vasopressor 14 –17 and fluid therapy in an effort to maintain perfusion through the site of injury. Vasopressors, however, may in actuality do little to increase perfusion, because their effects are the result of increased vascular constriction and resistance, meaning that blood flow through the site of injury is unlikely to increase. 18,19 As such, it is unsurprising that the aggressive management of BP using alpha agonists has not been consistently shown to lead to substantial neurological recovery after SCI. 20 Instead, maintaining blood volume may be more crucial during the acute phase of SCI, which would both impact BP and blood flow to the site of injury. Accordingly, we sought to characterize the impact of current management standards on cardiovascular parameters after SCI.
We aimed to establish the incidence of neurogenic shock, account for the confounding influence of hypovolemia, and characterize the natural progression and recovery of cardiovascular parameters in persons with SCI.
Methods
Study design and data collection
Patient charts were obtained from admission to the emergency department with a traumatic SCI at our tertiary care center in Vancouver, Canada from January 2008 to October 2010. Demographic information including age, sex, cause of injury, and associated injuries were collected from admission documents. At 0, 7, 14, and 30 days post-injury, each individual's level and severity of SCI was assessed according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI), 21 including American Spinal Injury Association (ASIA) Impairment Scale (AIS), and injury level (cervical C1–C7, high thoracic T2–T5, low thoracic T6–T12, and lumbar L1 and below). After clinical recommendations, 22 patients were treated to a target mean arterial pressure (MAP) >85 mm Hg for the first five to seven days post-injury. After this time, patients were treated symptomatically. Cardiovascular parameters including SBP, diastolic blood pressure (DBP), MAP, and HR were recorded daily for the duration of each patient's admission. Pharmacological management, including the use of vasopressor therapy, as well as intravenous fluid administration, fluid output, and laboratory tests were also recorded daily. All data were transcribed from charts to a secured and anonymized computer database. Ethical approval was obtained from the Clinical Research Ethics Board at the University of British Columbia.
Establishing the incidence of neurogenic shock
To establish the incidence of neurogenic shock in our population of patients with SCI, we performed a literature search and compared our sample against the numerous definitions of neurogenic shock used currently. Definitions of neurogenic shock included the following hemodynamic criteria: SBP <90 mm Hg, 3,23 –25 SBP <100 mm Hg, 1,5,7 simultaneous SBP <90 mm Hg and HR <50 bpm, 26 and simultaneous SBP <100 mm Hg and HR <80 bpm. 6,7,10,27 In addition, we examined the use of hemoglobin (males >11.8 g/dL; females >10.3 g/dL) at admission to account for hypovolemic shock, a potential confounder of previous incidence reports. This was done before application of the hemodynamic criteria, where individuals satisfying both requirements were considered to have neurogenic shock. The admission hemoglobin cutoffs were chosen for their association with moderate hypovolemic shock. 9 Because previous studies 3,6 reported the presence of isolated bradycardia in persons suspected of having neurogenic shock, we included the incidence of bradycardia (HR <50 bpm and <80 bpm) in the absence of hypotension (SBP <100 mm Hg).
Natural progression of cardiovascular parameters
To evaluate the natural progression of cardiovascular parameters after traumatic SCI, we compared the mean hemodynamic values among those with cervical, upper thoracic, and lower thoracic SCI for the duration of a patient's stay. This was performed every day for the first week, followed by every second day until day 30.
Vasopressor usage
When characterizing vasopressor usage, we quantified the length of administration (days), as well as the type and number of vasopressors administered (dopamine, norepinephrine, or both), vasopressor therapy switching, and administration of multi-drug therapy (defined as any individual receiving both vasopressors with at least two days of overlap).
Statistics
Repeated measured analyses were conducted in SAS Version 9.4 (©2002–2012 SAS Institute Inc., Cary, NC) using the MIXED procedure. The five outcomes of interest were HR (bpm), SBP (mm Hg), DBP (mm Hg), MAP (mm Hg), and net fluid intake (mL). The relationship between each outcome and time (days) as a continuous variable was estimated per level of SCI (cervical, upper thoracic, and lower thoracic) with five linear mixed models. For each model, the fixed effects included time, sex, level of SCI, and the interaction between time and level of SCI. The random effects included the intercept and time to account for repeated measures per individual. Pairwise comparisons of the slope between levels of SCI were conducted using the CONTRAST statements in the MIXED procedure to obtain F-statistics and p values. Statistical significance was taken at p < 0.05.
Results
Participants
Medical records from 92 patients were reviewed, four of whom were excluded from the study because of missing hemodynamic data. In addition, four persons with lumbar SCI were excluded from analysis because of lack of previous literature substantiating their inclusion with regard to neurogenic shock. The remaining 84 patients (56 cervical [C1–C7], eight upper thoracic [T1–T5], and 20 lower thoracic [T6–T12] SCI) were included in the analysis of hemodynamic management (pharmacologic and fluid resuscitation) as well as cardiovascular hemodynamic parameters (Table 1). Of those included in the study, 38 (45%) had isolated SCI while the remaining 46 (55%) had other associated injuries (fractures, 25 [30%]; lacerations, 10 [12%]; pneumothoracies, six [7%]; vertebral artery dissection, four [5%]; subarachnoid hemorrhage, three [4%]; abrasions, three [4%]). Seventy-nine (94%) of the individuals were admitted to our care center within 24 h of injury.
AIS, American Spinal Injury Association impairment scale; MVA, motor vehicle accident.
Neurogenic shock incidence
The incidence of neurogenic shock in persons with cervical SCI, in our data set, was higher than previous reports for SBP <100 mm Hg + HR <80 bpm (53.6% vs. 19.3%) and SBP <100 mm Hg (57.1% vs. 24.4% and 13.8%), but lower for SBP <90 mm Hg (19.6% vs. 43.8%) and SBP <90 mm Hg + HR <50 bpm (3.6% vs. 28.9%) (Table 2). Incidence was also higher in our data set in individuals with thoracic SCI for SBP <100 mm Hg + HR <80 bpm (35.7% vs. 7%), SBP <100 mm Hg (67.9% vs. 5.5%), and SBP <90 mm Hg (25.0% vs. 0%) (Table 2). For SBP <90 mm Hg + HR <50 bpm, we found no previously reported incidence in those with thoracic SCI and found an incidence of 0% in our data set (Table 2).
Criteria are organized by date of most recent use, with studies using these criteria listed under references.
Adjusted: listed criteria after hypovolemia correction (hemoglobin (males >11.8 g/dL; females >10.3 g/dL).
SBP, systolic blood pressure; HR, heart rate; N/A, not applicable.
Reported incidence for thoracic and lumbar injuries together.
Reported incidence for cervical and high thoracic injuries together.
After correcting for hypovolemic shock, incidence of neurogenic shock in those with cervical SCI was higher in our data set for SBP <100 mm Hg + HR <80 bpm (29.1% vs. 19.3%) and SBP <100 mm Hg (32.7% vs. 24.4% and 13.8%), but lower for SBP <90 mm Hg (10.7% vs. 43.8%) and SBP <90 mm Hg + HR <50 bpm (0% vs. 28.9%) (Table 2). Incidence was also higher in our data set in persons with thoracic SCI for SBP <100 mm Hg + HR <80 bpm (18.5% vs. 7%), SBP <100 mm Hg (33.3% vs. 5.5%), and SBP <90 mm Hg (10.7% vs. 0%). For SBP <90 mm Hg + HR <50 bpm, we found no previously reported incidence in those with thoracic SCI and found an incidence of 0% in our data set (Table 2).
Incidence of isolated bradycardia (HR <80 bpm) was higher in those with cervical SCI compared with thoracic SCI (42.9% vs. 28.6%). Incidence of isolated bradycardia taken as HR <50 bpm was higher in those with cervical SCI compared with thoracic SCI (14.3% vs. 0%) and lower than the incidence rates reported for isolated bradycardia (HR <80 bpm) (cervical SCI, 42.9% vs. 14.3%; thoracic SCI, 28.6% vs. 0%).
Patterns of acute cardiovascular recovery
Persons with cervical, upper, and lower thoracic SCI followed similar hemodynamic progressions over time (MAP, p > 0.05; SBP, p > 0.05; DBP, p > 0.05) (Fig. 1). The MAP was maintained above 85 mm Hg during the first seven days post-injury, followed by a characteristic decrease and remained below 85 mm Hg until discharge. The SBP followed a similar pattern. The SBP was maintained above 120 mm Hg in all three SCI groups, followed by a characteristic decline below 120 mm Hg for the remainder of care. The DBP remained largely unchanged throughout recovery. Mixed model linear regression analyses showed that during the 30-day time course, HR was lower among patients with cervical SCI compared with upper thoracic SCI (F = 9.20; p = 0.0025) and lower thoracic SCI (F = 11.56; p = 0.0007), even after taking into account time post-injury and sex. Patients with cervical SCI were the only group that consistently presented with a HR below 80 bpm.
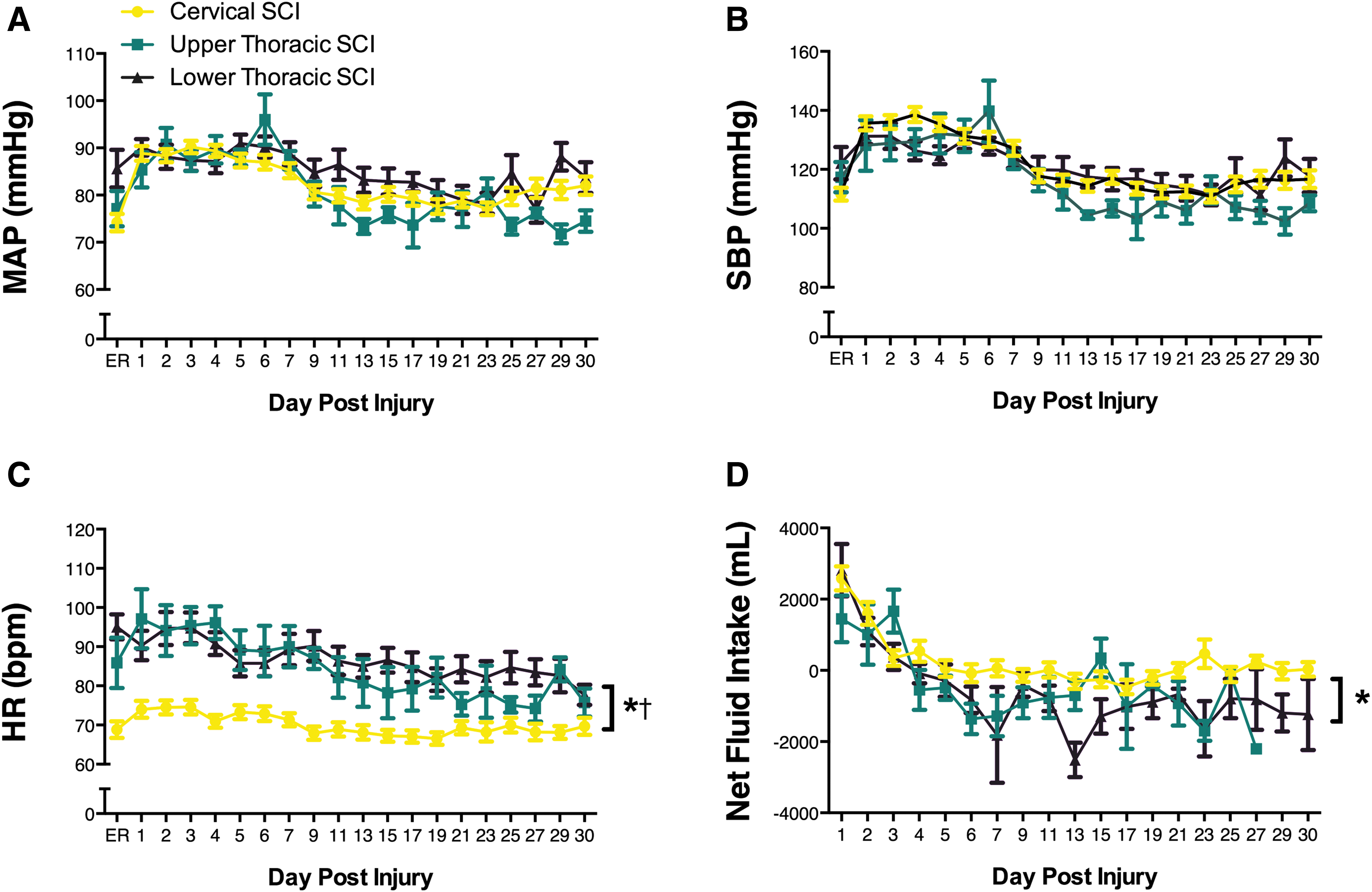
Time course of cardiovascular changes across time. (
Fluid management
In all persons with SCI, net fluid intake, as determined from intravenous fluid administration, was positive for the first three days post-injury (Fig. 1). After this time, those with thoracic SCI had a net fluid deficit (upper thoracic, mean = −836 mL, p = 0.1093; lower thoracic, mean = −871 mL, F = 11.78; p = 0.0006) compared with those with cervical SCI who had a mean net fluid intake of 0.163 mL.
Vasopressor usage
A total of 50 (60%; 42 cervical SCI, two upper thoracic SCI, six lower thoracic SCI) patients received vasopressor therapy (either dopamine or norepinephrine). Among the 50 patients, 26 received a single vasopressor and 24 received two vasopressors with at least one day of overlap. Of the treated individuals, the predominant first choice of vasopressor was norepinephrine in 24 (48%; 24/50) of the patients. The alternative, dopamine, was first line in 18 (36%; 18/50) of the patients. Vasopressor therapy with norepinephrine was more common among patients with upper cervical SCI (52%; 16/31) while therapy with dopamine was more common among patients with lower cervical SCI (72%; 8/11). The type of vasopressor was switched for three patients with cervical SCI (7%; 3/42). On average, patients with cervical SCI and thoracic SCI were, respectively, administered vasopressors for eight days and four days after injury.
Discussion
We demonstrate clearly the dire need for consistent criteria in the identification of neurogenic shock because currently employed definitions not only vary between centers, but also result in significantly varied reports of incidence for the condition. The wide range of previous incidence reports (13.8%–43.8%) in those with cervical SCI is in part because of differences in the patient populations in which the incidence of neurogenic shock was investigated. Those reporting incidences of 7%, 10 13.8%, 5 and 19.3% 6 did so in subsets of the cervical SCI population (respectively: penetrating injuries, blunt trauma, and isolated SCI), and likely resulted in lower incidence rates in these studies.
In addition, any evidence of hemorrhage disqualified an individual from being classified as having neurogenic shock in these studies, further reducing the incidence reports. Because persons with high level SCI are more vulnerable to hypovolemia from a diminished ability to generate arterial vasoconstriction or tachycardia, 3 neurogenic shock cannot be ruled out completely in a person with evidence of hemorrhage. Therefore, studies reporting incidence in this lower range of 7% to 19.3% may not be representative of the true incidence of neurogenic shock in the general cervical SCI population.
Studies reporting the incidence of neurogenic shock to be 24.4%, 7 28.9%, 26 and 43.8% 3 do so in the general cervical SCI population. These studies include a wider variety of injury types and thereby may be more representative of the true incidence of neurogenic shock in the cervical SCI population. While we considered the possibility that the reported incidence of 43.8% 3 may be an outlier, we found the injury severity of their study population (Frankel A/B, 31; C/D, 17) to be comparable to that found in our study (AIS A/B, 39; C/D, 17). Similarly, Billelo and associates, 26 who reported an incidence of 28.9%, found a comparable need to that of Lehmann and coworkers 3 for vasopressor and fluid therapy in their study population. As such, we reason that the incidence report by Lehman and colleagues 3 is a valuable consideration.
Despite the numerous operating definitions of neurogenic shock and the significant heterogeneity with which these are applied, the concordance between the studies reporting in the general cervical SCI population (24.4%, 7 28.9%, 26 and 43.8% 3 ) leads us to consider that the true incidence of neurogenic shock may be somewhere in this spectrum. While the confounding influence of hypovolemia is an important consideration, it is equally important to recognize that both hypovolemia and neurogenic shock are not mutually exclusive. As such, we chose to account for a significant hypovolemic component by excluding individuals with signs of moderate hypovolemia (hemoglobin: males >11.8 g/dL; females >10.3 g/dL). 9 Following this exclusion criteria, the calculated incidence of neurogenic shock (SBP <100 mm Hg and HR <80 bpm) in our population of cervical SCI (29%) remains concordant with previous considerations, and is representative of the average incidence (26%) found from previous work. 3,5 –7,26 As such, this definition likely increases the accuracy of measuring the incidence. Future prospective work should also consider the inclusion of other hypovolemic markers such as urine output or capillary refill. While these were inaccessible because of the retrospective nature of this study, they are likely to increase further the reliability of neurogenic shock incidence.
Our observation of higher incidence of neurogenic shock in the cervical SCI population (29%) compared with thoracic SCI (19%) is consistent both with previous work 3,5 –7,26 and with expected changes because of neuroanatomical aberrations from the injury, because these individuals would have the most severe sympathetic nervous system disruption. 10 This holds true as well for our observation of higher incidence of isolated bradycardia in the cervical SCI population (HR <80 bpm, 42.9%; HR <50 bpm, 14.3%) compared with thoracic SCI (HR <80 bpm, 28.6%; HR <50 bpm, 0%). While our finding of a 19% incidence of neurogenic shock in the thoracic SCI population may seem disproportionately higher than previous reports (0.0%, 3 5.5%, 7 and 7% 6 ), this may be explained by a higher proportion of more severe neurological injury within our thoracic SCI population (20 AIS A, five AIS B, two AIS C, and one AIS D). It is difficult to generalize across previous work, however, because previous studies did not report on the severities of the injuries in those with thoracic SCI. 3,6,7
Second, we examined the natural progression and recovery of hemodynamics during the acute phase after SCI using a linear mixed model approach. Our data highlight that current management guidelines, which are to maintain MAP above 85–90 mm Hg for the first 5–7 days, were being following at our center; however, because of cessation of vasopressor therapy after seven days, we observed a near universal drop in MAP after this time point. 15,22 During these first seven days, proper blood flow is considered critical to remove cytokines, as well as their metabolites, from the injury site and maintain the integrity of neural tissue. 22 As such, the cessation of vasopressor therapy at the seven day time point and the clinical management of BP being focused entirely on vasoconstriction (which is unlikely to increase flow at the site of injury according to fundamental physiological principles), likely has substantial implications for both the inflammatory environment and the potential for subsequent neurological recovery in the acute phase. Because damage from the neuroinflammatory environment at the injury site may last beyond this seven-day period, 28 it is plausible that individuals may benefit from longer hemodynamic management after SCI.
With regard to fluid management, our data indicate that volume expansion is not part of standard care, because the fluid status of individuals with cervical SCI is a net fluid intake of zero (i.e., euvolemia) and those with thoracic SCI are treated at a net volume deficit (i.e., hypovolemia). While we do not have data on oral fluid intake, this finding remains particularly concerning from a physiological point of view, because volume, in addition to MAP and intrathecal pressure, is a crucial determinant of flow in the acute phase after injury to maintain perfusion to the microvessels around the injury site. Moreover, appropriate blood volume likely has a much greater impact on blood flow as opposed to alpha agonist administration, which increases vascular resistance and pressure concurrently, with little effect on flow according to fundamental physiological principles. 18
Therefore, the observed fluid loss should be recognized as a potential limitation in current management and thus may act as a target to improve care for individuals with acute SCI. While further work is needed to tease apart these mechanisms should targeted fluid management be a viable addition to standard care for acute SCI, it may be a more efficacious alternative for increasing blood flow through the site of injury compared with isolated vasopressor therapy in this population.
Conclusion
There is a need clearly for consistent criteria to determine the incidence of neurogenic shock, and the present data support the inclusion of hypovolemia correction, in addition to SBP and HR. Therefore, we recommend the use of these criteria for future investigations into the incidence of neurogenic shock because accurate estimation of its incidence is crucial for healthcare and resource allocation. In addition, our data reveal that current management guidelines may leave individuals with acute SCI vulnerable to a drop in BP. Accordingly, we identify this as a potential target to improve future care for persons with acute SCI.
Footnotes
Acknowledgment
This work was supported by the Christopher and Dana Reeves Foundation and funding to the laboratory of A.V.K. from the Canadian Foundation for Innovation, BC Knowledge Translation Foundation, the Canadian Institute for Health Research, and the Craig Neilsen Foundation. I.A.R. was supported by a Faculty of Medicine Summer Research Program Scholarship from the University of British Columbia. J.W.S. is supported by a Frederick Banting and Charles Best Doctoral Canada Graduate Scholarship and a Vancouver Coastal Health-University of British Columbia MD/PhD Studentship from the Canadian Institutes of Health Research as well as a Killam Doctoral Scholarship and a Four Year Fellowship from the University of British Columbia. AAP is funded by the Craig H. Nielson Foundation, the Heart and Stroke Foundation, the Michael Smith Foundation for Health Research, and by a Killam Postdoctoral Prize.
Author Disclosure Statement
No competing financial interests exist.