
Abstract
Neuromonitoring can be used to observe intracranial pathological conditions in neurointensive care; however, use of intracranial pressure (ICP) monitoring is low in Japan. In this study, we retrospectively investigated the effects of ICP monitoring in the treatment of severe traumatic brain injury (TBI), using data from the Japan Neurotrauma Data Bank (JNTDB). The study was conducted in 1091 subjects enrolled in the JNTDB (Project 2009) from July 2009 to June 2011. The subjects were divided into those treated with and treated without ICP monitoring in intensive care for severe TBI. Age at admission, sex, level of consciousness (Glasgow Coma Scale [GCS] score), pupillary findings, findings on head CT, treatment, and outcome were compared between these groups. The subjects were also classified into two groups based on the outcome. Relationships among patient background factors, including ICP and clinical outcome were evaluated. The rate of ICP monitoring in treatment of severe TBI was 28%. Therapies were performed aggressively in the ICP monitoring group, and this group had a significant reduction in mortality, but no increase in the favorable outcome rate. In multivariate analysis, age, GCS, pupillary abnormalities, perimesencephalic cistern disappearance or compression, and ICP were associated with a favorable outcome, but the therapeutic method did not affect outcome. We conclude that ICP monitoring and management of ICP are both important for management and care of severe TBI. However, current therapies do not control ICP sufficiently, and more effective therapies are needed.
Introduction
M
Many pathological conditions can be treated by neurosurgery, including cerebral infarction, intracranial hemorrhage, and TBI, with the common therapeutic aim of maintaining cerebral circulation. ICP monitoring is one of several methods that have been devised to assess cerebral circulation. In this approach, cerebral perfusion pressure is calculated based on ICP and systemic blood pressure, which allows indirect monitoring of the intracerebral circulation. 4 However, the rate of ICP monitoring in treatment of severe TBI is only 55% in Japan, 5 compared with 77.4% in the United States in 2006, 6 based on a questionnaire survey. The lower rate in Japan may be the result of a lack of human resources and low cost effectiveness. 5 Moreover, the efficacy of ICP monitoring in treatment of severe TBI could not be shown in a multi-center randomized trial in the United States, 7 and this may also be a cause of the low use in Japan.
In this study, we retrospectively investigated the effects of ICP monitoring on treatment of severe TBI, using data from the Japan Neurotrauma Data Bank (JNTDB). Based on these results, we suggest approaches for use of ICP monitoring in treatment of severe TBI.
Methods
The JNTDB was established by the Japan Society of Neurotraumatology in 1996. 8 Investigations are conducted intermittently with completion of one project every 2 years. The JNTDB includes >200 items with information on the characteristics of the injury, diagnosis, treatment and complications. 8,9 Patient data regarding severe TBI are entered into the JNTDB from 23 collaborating clinical centers: Sapporo Medical University Hospital, Aomori Prefectural Central Hospital, Sendai City Hospital, Tokyo Medical University Ibaraki Medical Center, Chiba Cardiovascular Center, Chiba Emergency Medical Center, The Jikei University Kashiwa Hospital, Tokyo Medical University Hospital, Nippon Medical School Hospital, Nihon University Hospital, Teikyo University Hospital, Showa University Hospital, National Disaster Medical Center, Japanese Red Cross Musashino Hospital, St Marianna University Hospital, Tokai University Hospital, Juntendo University Shizuoka Hospital, Saiseikai Shiga Hospital, Kyoto Kujo Hospital, Kagawa University Hospital, Yamaguchi University Hospital, Kurume University Hospital, and Japanese Red Cross Kumamoto Hospital.
The study was conducted on 1091 subjects enrolled in the JNTDB (Project 2009) from July 2009 to June 2011. All subjects had Glasgow Coma Scale (GCS) scores of ≤8 on admission, or deterioration to that level within 48 h of impact or craniotomy for traumatic hematoma. Criteria for use of ICP monitoring in these clinical centers should be consistent with Japanese guidelines for management and care of severe TBI; 3 however, the rate of use of ICP monitoring was low in institutions adhering to the guidelines, based on our earlier questionnaire survey. 5 Because this study was observational, there was no compelling reason for use of the criteria in ICP monitoring; however, it seems that judgments were made with consultation of the Japanese guidelines. The subjects were divided into those treated with and those treated without ICP monitoring in intensive care for severe TBI. Age at admission, sex, level of consciousness (GCS), and pupillary findings were compared between these groups. The pathological conditions of each group were also investigated, based on head CT findings at admission (Traumatic Coma Data Bank [TCDB] classification), 10 and cerebral hernia findings (disappearance or compression of the perimesencephalic cistern, and midline shift >5 mm). The TCDB classification 10 is as follows: diffuse injury I, no visible intracranial pathology on CT; diffuse injury II, cisterns present with a midline shift of 0–5 mm and/or no high- or mixed-density lesion >25 cc; diffuse injury III, cisterns compressed or absent with a midline shift of 0–5 mm and/or no high- or mixed-density lesion >25 cc; diffuse injury IV, midline shift >5 mm, no high- or mixed-density lesion >25 cc; evacuated mass lesion, any lesion surgically evacuated; unevacuated mass lesion, high- or mixed-density lesion >25 cc, not surgically evacuated.
Treatment with hyperventilation, hyperosmolar diuretics, sedatives, anticonvulsants, surgery (ventricular drainage, hematoma irrigation with trephination therapy, hematoma removal with craniotomy and decompressive craniectomy), and body temperature management (induced hypothermia and induced normothermia) were examined in the two groups. The Glasgow Outcome Scale (GOS) at discharge was used to assess patient outcome, with good recovery (GR) and moderate disability (MD) defined as a favorable outcome.
To exclude bias in the treatment, examinations were also performed in the ICP monitoring group alone. The subjects were classified into two groups based on a favorable or poor GOS outcome at discharge. Age at admission, sex, level of consciousness (GCS), pupillary findings, head CT findings, treatment, placement of an ICP sensor, and maximum ICP during treatment (ICPmax) were evaluated in these groups.
Statistical analysis
Statistical analysis was performed by Mann–Whitney U test or χ 2 test, with p < 0.05 considered to be significant. Clinical variables were used in multivariate logistic regression analysis to identify independent predictors of a favorable outcome. A p value, 95% confidence interval (CI), and odds ratio (OR) are reported for significant variables in this analysis. Receiver-operating characteristic (ROC) curve analysis was used to estimate an optimal cutoff value for ICPmax.
Results
The ICP monitoring group included 305 subjects (28.0%) and the non-ICP monitoring group had 786 subjects (72.0%) (Table 1). The rate of use of ICP monitoring in each institution ranged from 0 to 100% (Fig. 1), and criteria for use of ICP monitoring differed among institutions. Subjects in the ICP monitoring group were significantly younger than those in the non-ICP monitoring group (51.5 ± 23.5 vs. 57.1 ± 24.3 years) (Table 1). There were no significant differences in sex (male; 72.8% vs. 67.7%), GCS scores on admission (7.2 ± 3.7 vs. 7.2 ± 4.0), and pupillary abnormalities (40.0% vs. 44.3%) between the two groups (Table 1).
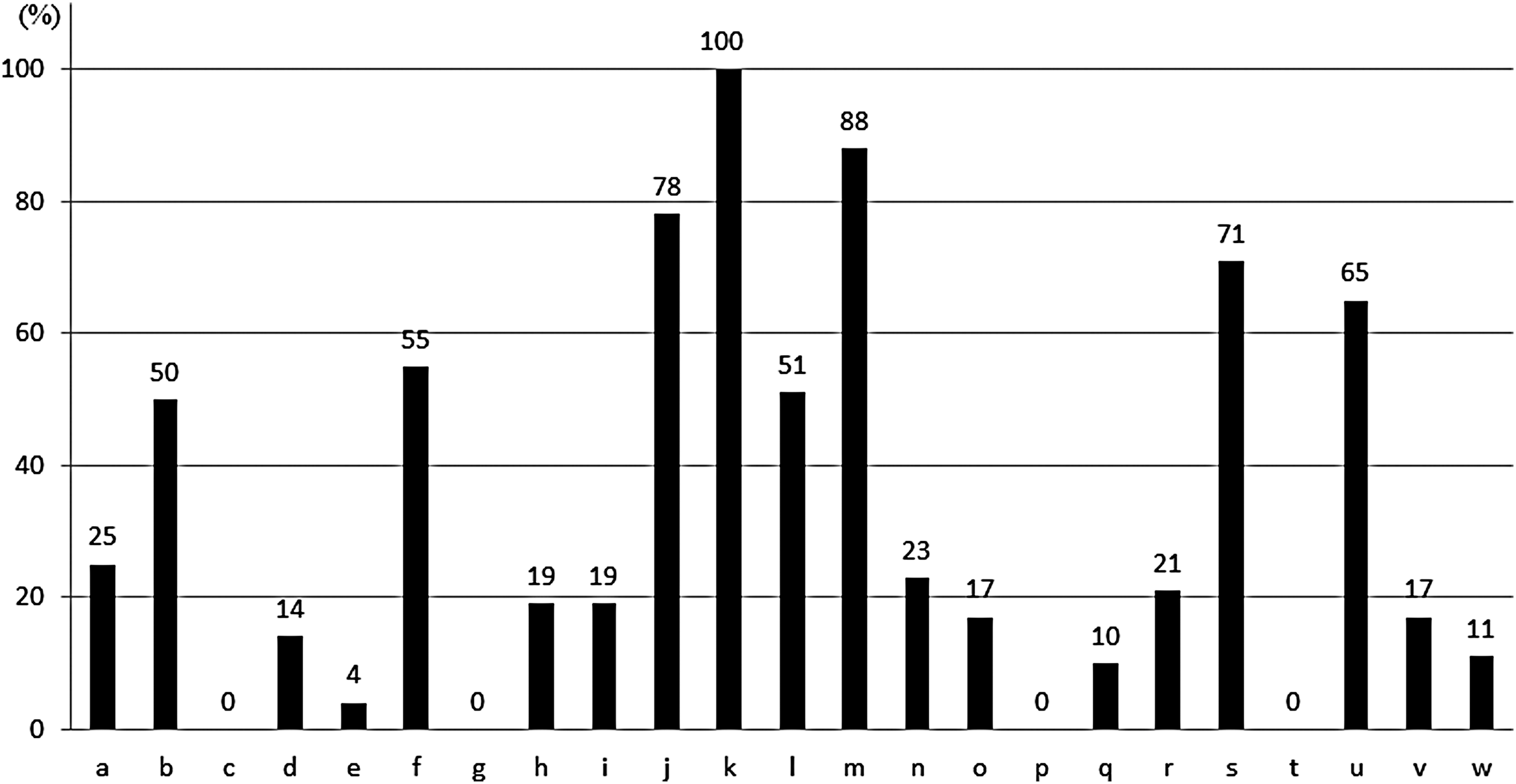
The rate of use of an intracranial pressure (ICP) sensor at each clinical center. The rate varied among the centers.
Values are presented as mean ± standard deviation.
Significantly different compared between two groups at p < 0.05.
JNTDB, Japan Neurotrauma Data Bank; ICP, intracranial pressure; TCDB; Traumatic Coma Data Bank.
Disease types on CT at admission were categorized using the TCDB classification as diffuse injury I–II (15.4% ICP monitoring vs. 26.0% non-ICP monitoring), diffuse injury III–IV (14.4% vs. 10.1%), and evacuated mass lesions (54.1% vs. 36.9%) (Table 1). The ICP monitoring group had significantly higher rates of disappearance or compression of the perimesencephalic cistern (69.8% vs. 57.3%) and midline shifts ≥5 mm (46.6% vs. 40.6%) (Table 1).
In treatment, the ICP monitoring group had significantly higher rates of hyperventilation (13.1% vs. 7.6%), hyperosmolar diuretics (64.9% vs. 31.9%), sedatives (78.4% vs. 28.5%), anticonvulsants (50.8% vs. 28.9%), and surgery (85.9% vs. 49.7%) (Table 1). Body temperature management was also performed significantly more frequently in this group, based on rates of induced hypothermia, induced normothermia, and no body temperature management of 26.9%, 41.6%, and 31.5%, respectively, in the ICP monitoring group, and 2.2%, 22.1%, and 74.8%, respectively, in the non-ICP monitoring group (Table 1).
Favorable outcomes did not differ significantly between the groups (29.2% ICP monitoring vs. 30.0% non-ICP monitoring), but mortality was significantly lower in the ICP monitoring group (32.5% vs. 45.0%) (Table 1).
ICP monitoring group
Of the 305 patients in this group, 89 (29.2%) had favorable outcomes and 216 (70.8%) had poor outcomes (Table 2). Subjects with favorable outcomes were significantly younger than those with poor outcomes (39.1 ± 22.9 vs. 56.5 ± 21.8 years) (Table 2). There was no significant difference in sex (male 70.8% vs. 73.6%) (Table 2). GCS scores on admission were significantly higher in patients with favorable outcomes (8.9 ± 3.8 vs. 6.6 ± 3.4), whereas the rate of pupillary abnormalities was significantly higher in patients with poor outcomes (14.7% vs. 50.5%) (Table 2).
Values are presented as mean ± standard deviation.
Significantly different compared between two groups at p < 0.05.
ICP, intracranial pressure; ICPmax, maximum ICP; TCDB, Traumatic Coma Data Bank.
Disease types on CT at admission were diffuse injury I–II (21.3% favorable outcome vs. 13.0% poor outcome), diffuse injury III–IV (9.0% vs. 16.7%), and evacuated mass lesions (53.9% vs. 54.2%) (Table 2). Patients with poor outcomes had significantly higher rates of disappearance or compression of the perimesencephalic cistern (51.7% vs. 77.3%); however, there was no significant difference in midline shifts of ≥5 mm (42.7% vs. 52.8%) (Table 2).
There were no significant differences in the rates of hyperventilation (11.2% vs. 13.9%), sedatives (80.9% vs. 77.3%), and anticonvulsants (57.3% vs. 48.1%), but hyperosmolar diuretics (44.9% vs. 73.1%) and surgical treatment (77.5% vs. 89.4%) were performed significantly more frequently in patients with poor outcomes (Table 2). In contrast, those with favorable outcomes had significantly higher rates of body temperature management (78.7% vs. 64.4%) (Table 2).
ICP sensors were placed subdurally in 64 subjects (21.0%), epidurally in 4 (1.3%), in brain tissue in 206 (67.5%), and ventricularly in 30 (9.8%), indicating that most sensors were placed in brain tissue (Fig. 2). Patients with favorable outcomes had a significantly lower ICPmax than those with poor outcomes (22.1 ± 12.3 vs. 39.6 ± 29.5) (Table 2).
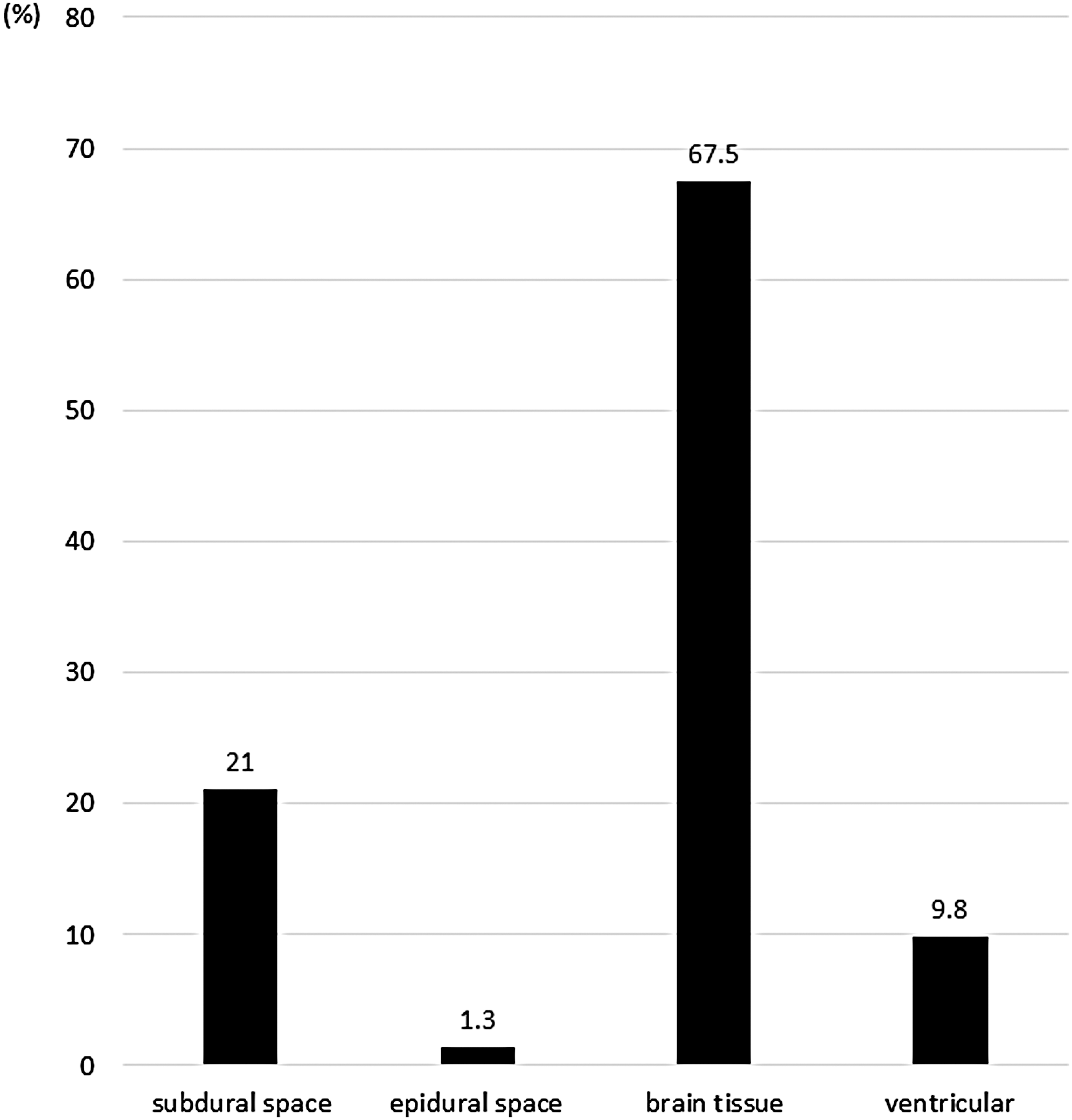
Rates of placement of an intracranial pressure (ICP) sensor. Most sensors were placed in brain tissue.
In a multivariate model, five variables were associated with a favorable outcome: age (OR = 0.9; 95% CI = 0.93–0.96), GCS (OR = 1.2; 95% CI = 1.05–1.28), pupillary abnormalities (OR = 5.1; 95% CI = 2.11–12.12), perimesencephalic cistern disappearance or compression (OR = 2.9; 95% CI = 1.37–6.17), and ICPmax (OR = 0.94; 95% CI = 0.92–0.97) (Table 3). To determine the relationship between ICPmax and outcome, a ROC curve was generated. The area under the ROC curve for ICPmax was 0.708 (95% CI = 0.648–0.768, p < 0.001), with sensitivity of 65.2% and specificity of 64.6% at a cutoff of ICPmax of 22.5 mm Hg (Fig. 3).

Receiver operating characteristic (ROC) curve analysis of maximum intracranial pressure (ICPmax) for outcome.
Significantly different compared between two groups at p < 0.05.
GCS, Glasgow Coma Scale; ICP max, maximum intracranial pressure.
Discussion
The rate of ICP monitoring in treatment of severe TBI of 28% in this study suggests that use of this method has declined, compared with previous rates of 55% found in a questionnaire survey, 5 and rates of 34.1% based on data from the JNTDB (Project 1998). 11 This may be because of the absence of a large-scale clinical trial showing evidence of the efficacy of ICP monitoring 7 , rather than lack of human resources or low cost-effectiveness. 5 Evidence for efficacy of treatment of severe TBI in a large-scale trial has not been reported for more than a decade, and this is a serious future concern in the field of neurotraumatology.
The Japanese guidelines for management and care of severe TBI 3 include the following indications for ICP monitoring: 1) GCS score <8, 2) low blood pressure (systolic pressure <90 mm Hg), and 3) CT findings of midline shifts or loss of the perimesencephalic cistern. In this study, ICP monitoring was performed significantly more frequently in subjects with an evacuated mass lesion. These subjects underwent craniotomy, which enabled placement of ICP sensors and may facilitate manipulation. Subjects showing cerebral herniation on CT also received ICP monitoring significantly more frequently. In Japan, ICP monitoring is likely to be performed aggressively in a case with suspected increased ICP on CT. The Japanese guidelines for management and care of severe TBI 3 suggest that the threshold to initiate treatment is an ICP of 15–25 mm Hg. Another report proposed that a lower level of <10 mm Hg should be the criterion for pediatric patients. 12 These thresholds have been established based on previous studies, 13 –15 in which ICP ≥20 mm Hg was found to be a critical predictive factor for neurological exacerbation. The current study also suggests that it is important to maintain ICP at ≤20 mm Hg for management and care of severe TBI.
Methods for ICP monitoring include various measurement sites and devices, each of which has advantages and disadvantages that should be fully understood in selection of a method for a particular pathological condition. 16 The commonly recommended method in different guidelines is measurement via a ventricular catheter, because this has the highest reliability and low cost, and can also be used for cerebrospinal fluid drainage. 16 However, insertion of a ventricular catheter is often difficult, because of factors such as ventricular compression and midline shift. This may explain why sensors were most commonly placed in brain tissue in the current study. Failure in treatment caused by missed detection of increased ICP is likely to lead to cerebral herniation and result in severe irreversible brain damage.
Treatment of elevated ICP typically progresses in stages from noninvasive therapy. 17 In this study, we examined hyperventilation; drug therapy with hyperosmolar diuretics, sedatives, and anticonvulsants; surgical treatment; and body temperature management. All these therapies were performed aggressively in patients who received ICP monitoring, which may be the result of the ICP data obtained from monitoring in this group. The results indicated a significant reduction in mortality in these patients, but no improvement of the favorable outcome rate as in previous reports. 18,19 Therefore, a further study is required to determine the appropriate treatment based on the results of ICP monitoring for improvement of the outcome of severe TBI.
The results also suggested that active treatment was discontinued in many patients who did not receive ICP monitoring. Therefore, the relationship of outcomes with treatment and ICP was evaluated only in those who did undergo ICP monitoring. Patients with favorable outcomes were significantly younger, had significantly fewer pupillary abnormalities, a significantly higher GCS, and a significantly lower incidence of midline shift on CT. In a comparison of treatment approaches, surgery was significantly more common in patients with poor outcomes, while body temperature management was significantly more frequent in those with favorable outcomes. ICPmax was significantly lower in patients with favorable outcomes.
Multivariate analysis identified age, GCS, pupillary abnormalities, midline shift, and ICPmax as independent predictors of outcome. These factors are consistent with previously identified predictors for outcomes of severe TBI. 20 Therefore, these results suggest that outcomes have no relationship with treatment contents, but rather with age, initial brain damage (GCS, pupillary abnormalities, and midline shift), and ICPmax. This reflects the limitation of current treatment, in which it is difficult to control ICPmax in elderly patients and patients with severe initial brain damage. This limitation results in no improvement of outcomes.
The results of the study show that ICPmax should be controlled at ≤20 mm Hg for improved outcomes of severe TBI. Management with ICP monitoring is necessary to achieve this treatment goal. Diagnostic imaging alone is insufficient. Several large-scale clinical trials of ICP monitoring have been unsuccessful, 7 but this is because ICP monitoring without ICP control results in poor outcome. That is, the effect of ICP monitoring is different from the therapeutic effect of ICP management, 21 and better recognition of this issue is required.
Conclusion
Age, level of initial brain damage, and ICPmax were identified as factors related to favorable outcomes of severe TBI. ICP monitoring and ICPmax management are required to achieve improved outcomes. However, current therapy does not provide sufficient ICPmax management, and more effective therapies need to be developed.
Footnotes
Author Disclosure Statement
No competing financial interests exist