
Abstract
Spinal cord injury (SCI) is a devastating condition that affects patients on both a personal and societal level. The objective of the study is to improve the prediction of long-term functional outcome following SCI based on the acute clinical findings. A total of 76 patients with acute traumatic SCI were prospectively enrolled in a cohort study in a single Level I trauma center. Spinal Cord Independence Measure (SCIM) at 1 year after the trauma was the primary outcome. Potential predictors of functional outcome were recorded during the acute hospitalization: age, sex, level and type of injury, comorbidities, American Spinal Injury Association (ASIA) Impairment Scale (AIS), ASIA Motor Score (AMS), ASIA Light Touch score (LT), ASIA Pin Prick score (PP), Injury Severity Score (ISS), traumatic brain injury, and delay from trauma to surgery. A linear regression model was created with the primary outcome modeled relative to the acute clinical findings. Only four variables were selected in the model, with performance averaging an R-square value of 0.57. In descending order, the best predictors for SCIM at 1 year were: LT, AIS grade, ISS, and AMS. One-year functional outcome (SCIM) can be estimated by a simple equation that takes into account four parameters of the initial physical examination. Estimating the patient long-term outcome early after traumatic SCI is important in order to define the management strategies that might diminish the costs and to give the patient and family a better view of the long-term expectations.
Introduction
W
Costs associated with SCI are greatly influenced by the patient's severity of injury and resultant degree of disability. 4 In 2011, average per-person yearly expenses in the U.S. were $523,089 in the first year and $79,759 in each subsequent year. 5 In Canada, the estimated lifetime economic burden per individual with SCI ranges from $1.5 million for incomplete paraplegia to $3.0 million for complete tetraplegia. The annual economic burden associated with 1389 new persons with SCI surviving their initial hospitalization is estimated at $2.67 billion. 6
Prognosticating the patient functional outcome early after traumatic SCI is important in order to guide the management strategies that might diminish the costs and to give the patient and family a better view of the long-term expectations. The meta-analysis published by van Middendorp and colleagues in 2013 showed that despite the fact that “early” spinal surgery was significantly associated with improved neurological outcome and decreased length of stay, the evidence supporting early spinal surgery after SCI lacks robustness as a result of different sources of heterogeneity within and between original studies. 7 The prediction model published by Wilson and colleagues in 2012 did not include the time to decompressive surgery that may influence patient outcomes. 8 In addition, they used the Functional Independence Measure (FIM), which is not specific to patients with spinal cord injuries. Indeed, the Spinal Cord Independence Measure (SCIM) is the only functional recovery outcome measure designed specifically for SCI and the latest version of the SCIM (SCIM III) is recommended to be implemented worldwide as the primary functional recovery outcome measure for SCI. 9 Moreover, SCIM has the most appropriate performance regarding the instrument's psychometric properties 10 and is more responsive to change than the FIM for the respiration and sphincter management subscale 11 and mobility indoors and outdoors. 12
The AMS (American Spinal Injury Association [ASIA] Motor Score) has been shown to be a predictor of the outcome for SCI, 8 while being an integral part of the basic neurological examination, along with the light touch (LT) and pin prick (PP) sensory examination. Preservation of PP sensation below the zone of injury is associated with excellent prognosis for regaining functional ambulation. 13 LT has a tendency to score higher than PP in SCI subjects. The discrepancies between LT and PP could relate to the greater complexity of the PP testing or to a difference in the extent of injury to the posterior columns (LT) and spinothalamic (PP) tracts. 14
The Injury Severity Score (ISS) is an anatomical scoring system that provides an overall score for patients with multiple injuries. This scale is an independent predictor of death following severe trauma and correlates well with disability and hospitalization. In patients with SCI treated in Level I trauma centers, the severity of injury was significantly associated with an unfavorable outcome. 15 There also are reports supporting the negative impact of the brain injury on the functional outcome and community integration. 16 Given the incidence of combined traumatic brain injury (TBI) and SCI, 17 one must take into account the former parameter.
With regard to the delay to surgery, there are reports that suggest that the patients with SCI who undergo surgical decompression (SD) within 8 h after injury have superior neurological outcomes than patients who undergo SD 8–24 h after injury, without any increase in the rate of adverse effects. 18,19 Previous data also suggest that patients with traumatic SCI should be promptly operated on earlier than 24 h following the injury to reduce complications while optimizing neurologic recovery. 20,21
Older individuals with SCI have a substantially increased mortality rate during the first year, compared with younger patients. Among survivors, for a similar neurological improvement after the SCI, the functional gain is lower for older patients, compared with young patients. 22
The aim of this study is to examine whether different clinical parameters obtained in the acute period post-SCI, including the demographic factors and delay to surgery are predictors of the functional outcome at 1 year, evaluated with SCIM III.
Methods
Data source
A prospective cohort of 76 patients with a cervical or thoracolumbar traumatic SCI consecutively admitted to a single Level I SCI-specialized trauma center between April 2010 and November 2013 was studied. Patients entered the cohort at the time of admission after consent and were followed until discharge from the SCI-center. They were included if they sustained an acute traumatic SCI at the cervical (C1 to C8) or thoracolumbar (T1 to L1) requiring surgical management, which was performed in our institution, were aged 16 years or older and presented at their 1-year post-trauma follow-up visit. Patients were excluded if they had a penetrating trauma, received non-surgical management, had a diagnosis of central cord syndrome or neurological deficit without evidence of spinal instability, or did not come to the 1-year follow-up visit. The study was approved by the institutional review board and all patients were enrolled on a voluntary basis. Neurological status was assessed systematically at arrival to the hospital prior to surgery, in accordance with ASIA recommendations by a trained physician or nurse. No patient received steroids before or after the decompressive surgery.
Predictor variables
Independent variables consisted of variables that have been described in the literature as outcome predictors (Table 1). These independent variables were collected prospectively during the early acute period after the SCI and describe the baseline characteristics of the patient and trauma, as well as the delay to surgery. For neurological classification, 28 dermatomes were assessed bilaterally using PP and LT sensation (0: absent; 1: impaired or 2: normal) and 10 key muscles (from 0 [total paralysis] to 5 [full range of motion against resistance]) were assessed bilaterally for AMS. The results were summed to produce overall sensory and motor scores. LT and PP each scored out of 112 (28 locations bilaterally with a maximum score of 2 at each location) while AMS scored out of 100 (10 locations bilaterally with a maximum score of 5 at each location).
ASIA, American Spinal Injury Association.
Outcome and follow-up
We quantified the outcome using the SCIM III score at 1 year (Table 2). The SCIM score consists in 19 items that take into account three domains: self-care (six items, scores range from 0–20); respiration and sphincter management (four items, scores range from 0–40); and mobility (nine items, scores range from 0–40). The total SCIM score ranges from 0 to 100. 12
Statistical analysis
To explore the data, we performed a univariate and bivariate analysis, and then focused on inference and modeling. Central tendency, dispersion, and frequency of variables were analyzed. For continuous variables, their normal distribution was tested using a Kolmogorov-Smirnov test. Most variables did not have a Gaussian distribution. Therefore, we occasionally used median for central tendency and non-parametric tests for statistical inference. All categorical data were bilaterally tested on SCIM with a level of significance of 0.05 using t-tests or one-way analysis of variance. The statistical modeling for SCIM was based on a linear regression model with forward stepwise method, which met conditions of independence of errors and approached a studentized distribution of residues. Collinearity problems were tested using variance inflation factors. To account for missing data, a multiple imputation analysis was performed with 10 imputation iterations using Markov chain Monte Carlo method. Internal validation was obtained using a bootstrap re-sampling procedure of the imputated dataset. All statistics were performed using SPSS software (v.20, SPSS, Inc., Chicago, IL).
Results
Study population
The mean age was 43 years (± 18; Table 3) and most patients presented with fractures (64.5%) or fracture-dislocation injuries (27.6%). Remaining patients had acute traumatic disc and soft tissue injury causing overt spinal instability. There was a peak incidence for the levels C5-C7 (40.7%) and T11-L1 (31.6%) in terms of anatomical lesions (Fig. 1).

Bimodal distribution of the level of anatomical lesions.
SD, standard deviation; LoS, length of stay; ASIA, American Spinal Injury Association; SCIM, Spinal Cord Independence Measure.
We found a male/female distribution ratio of 3/1. The most common causes of injury in our series are falls (36.8%), motor vehicle accidents (34.2%), and sport-related injuries (19.7%). Most patients were healthy with no comorbidities (75%) and almost half of them (46.1%) presented with TBI (Table 4).
SCIM, Spinal Cord Independence Measure; TBI, traumatic brain injury; AIS, American Spinal Injury Association Impairment Scale.
Functional outcome and modeling
The functional outcome tested using the SCIM III had a mean value of 72% (± 25) at 12 months. As expected, the SCIM was significantly correlated with the AIS grade (p < 0.001).
In our model, the most powerful predictor variables proved to be, in descending order, the ASIA LT score, AIS grade, ISS, and the AMS score, all collected at the admission.
The pre-operative LT score was available for 67 patients while the AIS grade, the ISS and the AMS were respectively available for 75, 75, and 71 patients. To account for missing data, multiple imputations with 10 iterations was performed, resulting in a complete dataset of 760 patients in order to perform a linear regression less susceptible to bias. For the linear regression model, the performance was reflected by an R-squared value of 0.573.
The relative importance of the significant predictors were explained in terms of standardized coefficients (Table 5), reflecting the contribution of each variable in the prediction model.
SCIM, Spinal Cord Independence Measure; CI, confidence interval; ASIA, American Spinal Injury Association; AIS, American Spinal Injury Association Impairment Scale; ISS, Injury Severity Score.
The pre-operative LT score had a statistical predictive value of 0.382 (which reflect the participation of the variable in the model). The second most powerful predictor, the AIS grade, had a predictive value of 0.281 while the third predictor, the ISS, had a value of 0.272. The fourth predictor in order of importance was the AMS, with a predictive value of 0.068.
The other predictor variables with statistical significance were: the pre-operative ASIA PP scores and the hospital length of stay (p < 0.05). We found no predictive value for the sex, age, comorbidities, TBI, and type of injury or level of injury. Moreover, there was no significant correlation between the delay to surgery and the SCIM at 1 year.
According to the findings, we created a predictive equation of the SCIM score at 1 year after the SCI, based on the four most powerful predictive variables: LT, AIS, ISS, and AMS (Table 6). The effect of LT score in predicting SCIM at 1 year is highlighted in Figure 2.
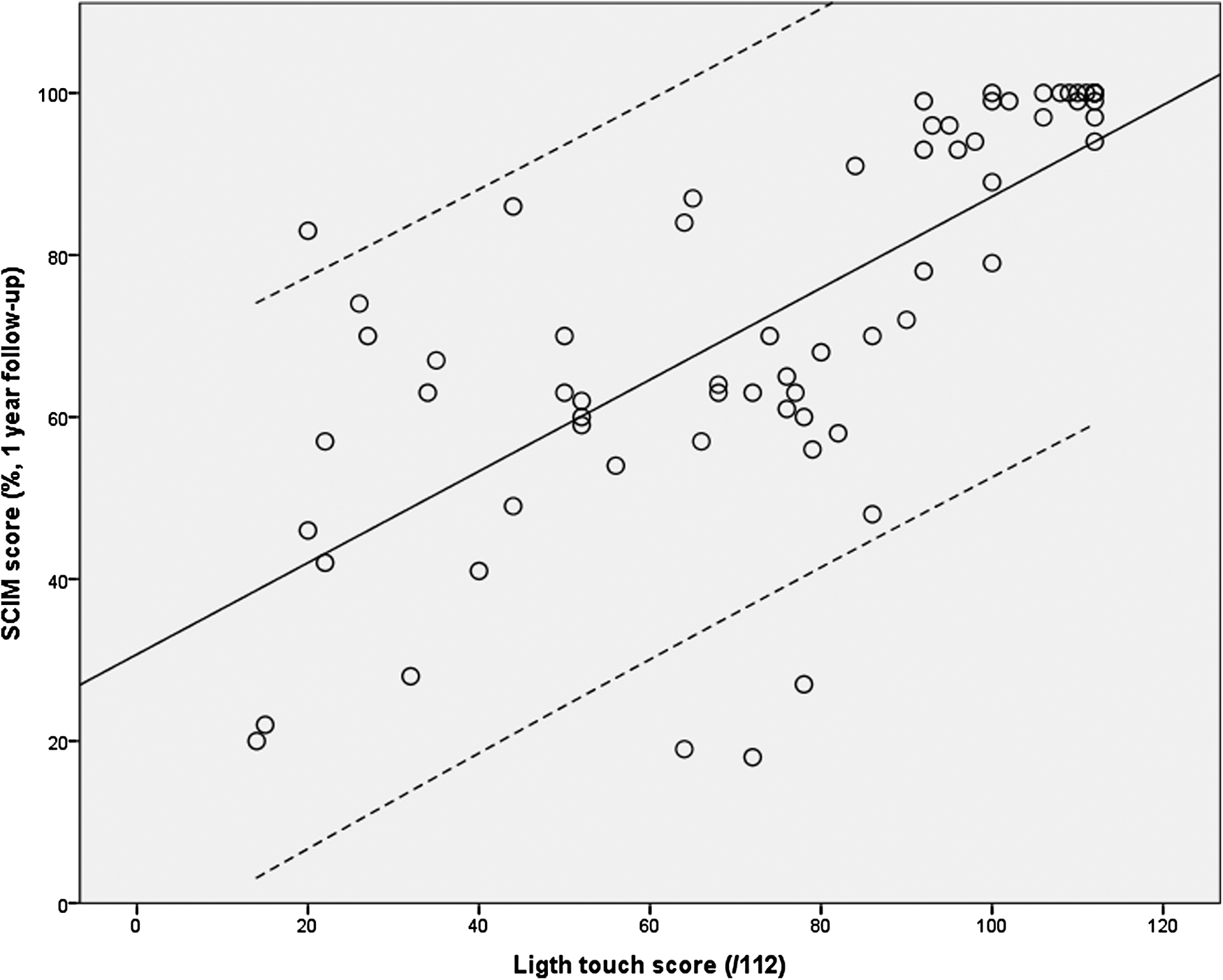
Correlation between pre-operative American Spinal Injury Association Light Touch score and Spinal Cord Independence Measure (SCIM) at 1 year.
SCIM, Spinal Cord Independence Measure.
Discussion
This is the first study in the literature proposing a predictive model of the SCIM III total score based on acute predictors. By using only four predictors (LT, AIS grade, ISS and AMS), the model was associated with an R-squared value of 0.573, thereby explaining 57% of the variance in SCIM III total score.
Many studies have utilized walking as the primary measure of long-term functional outcome but if mobility function is highly important to individuals with paraplegia, restoration of arm and hand function is a specific priority for individuals with tetraplegia that needs to be taken into account. 23 Some authors 8 have measured functional outcome using the FIM, which is not specific to patients with SCI. Moreover, many authors underscore the importance of incorporating outcome tools that include multi-dimensional assessments of functional status. In our series, the outcome is measured using the SCIM III. The choice was based on the fact that SCIM is the only functional recovery outcome measure designed specifically for SCI 9 and the score with the most appropriate performance regarding the instrument's psychometric properties. 10
Interestingly, LT was by far the most powerful predictor for the SCIM at 12 months. Because the LT score uses all the dermatomes unlike the AMS, we believe that it provides a better understanding of the severity of injury. The AMS uses only 10 groups of muscles (C5-T1, L2-S1) and this could explain its lower significance. Other authors, such as Wilson and colleagues, 8 suggest an important predictive value for the AMS but did not include the LT in their analysis. By including both AMS and LT in our analysis, our data suggest a greater predictive value for the LT score. This might be due to the fact that in the regression model, most of the variance explained by the AMS is already determined by the LT score (i.e., collinearity between the two variables). We find this to be the main reason why, in our study, the LT score has the highest predictive value of SCIM at 1 year post-injury. The same argument prevails regarding the PP score.
According to some authors, the AIS conversion outcome measure is poorly related to the ability to walk in traumatic SCI patients. 24 Moreover, unlike the sensory or motor scores, the AIS grade is categorizing the patients in only 5 grades. We consider this to be the main reason for the lower statistical significance when compared with the LT.
The ISS score has a very high predictive value in patients with SCI. This is in correlation with the importance of the clinical management in the acute setting. Indeed, the secondary insults from local ischemia, hypotension, hypoxia, and inflammation needs to be identified, prevented, and treated. 25 In consequence, multiple injuries severity can have a large effect on functional recovery. This confirms the findings of Stephan and colleagues. 15
In their prediction model of the FIM 6 to 12 months after the SCI, Wilson and colleagues 8 included four variables (R2 = 0.52). Patients' age was a predictor of functional outcome, as well as AMS, AIS grade, and magnetic resonance imaging (MRI) signal. Although we expected the same results, our data showed no correlation between SCIM and patients' age (p = 0.232). In another study, advanced age (> 65 years) was associated with worse functional outcome after SCI in terms of FIM. 26 The same authors noted that this effect was greatest for ASIA B and ASIA C patients and lesser for ASIA A and ASIA D patients. This could explain the absence of a significant relation between age and SCIM, given the fact that there were only eight (10.4%) ASIA B patients and seven (9.1%) ASIA C patients in our study.
There is growing evidence concerning the necessity of early decompression for optimal neurological recovery 21,27 but in terms of functional recovery, the references are more sparse. Surprisingly, the delay to surgery was not significant in our model for SCIM. This is in conflict with a recent publication of Grassner and colleagues. 19 In their study, where the population was divided into early (< 8 h) and late decompression, the outcome was measured at 1 year. SCIM was significantly higher in the early group. In our data, there was a large range in terms of delay to surgery (Table 3). Moreover, the variable distribution was not Gaussian (mean: 58 h; median: 21 h). This may reflect the difficulty of routing some of the patients in a hospital, even a Level I trauma center in Canada, in such a wide territory. Thus, a median time of 21 h is probably too long for observing significant benefits in terms of functional outcome for patients undergoing early surgery, as opposed to the study of Grassner and colleagues 19 that specifically included a group undergoing early surgery within 8 h of the SCI.
Study limitations
Our series comprises 76 patients, which is a relatively small number. However, the size of our cohort was sufficient for identifying significant predictors of the functional outcome, and for obtaining an adequate performance of our predictive model (R2 = 0.573). We also recognize that other potential predictors such as abnormal MRI signal was not collected in our data, while some authors took this into account for their prediction model. 8 It is due to the fact that even if MRI carries great information about the spinal injury, it is not routinely performed in our trauma center when early surgery is required and when it is not likely to influence the surgical planning.
Conclusions
Prediction of functional recovery based on data available during the early acute period after the trauma is of paramount importance for the society, for the patients, and for the caregivers. This study highlights the importance of the initial ASIA evaluation (AIS grade, LT and AMS), as well as the ISS, in predicting patients' functional recovery at 1 year. Our prediction model including only these four predictors is efficient (R2 = 0.57) and has the potential to guide decision at clinical as well as societal levels.
Footnotes
Acknowledgments
The authors would like to thank for their financial support the Department of the Army (United States Army Medical Research Acquisition Activity) and the Rick Hansen Spinal Cord Injury Registry.
Author Disclosure Statement
Dr. Mac-Thiong reports receiving during the conduct of this study grants from Rick Hansen Institute and from the Department of the Army–United States Army Medical Research Acquisition Activity. He also reports receiving grants outside of the submitted work from Spinologics Inc., Fonds de Recherche du Québec-Santé, the Scoliosis Research Society, Fonds de recherche du Québec-Nature et technologies, the Natural Sciences and Engineering Research Council of Canada, the Canada Foundation for Innovation, and Medtronic of Canada, as well as other non-financial support from Medtronic of Canada.
For the other authors, no competing financial interest exist.