
Abstract
The level of spinal cord injury (SCI) affects baroreflex regulation of blood pressure. While a parasympathetic cardiac chronotropic effect is preserved, baroreflex response could be impaired by sympathetic dysfunction under the SCI level. This study was aimed to evaluate the baroreflex function in SCI patients by the analysis of causal interaction between systolic blood pressure (SBP) and inter-beat intervals (IBI). Blood pressure was continuously recorded in 13 cervical SCI patients (CSCI), nine thoracic SCI (ThSCI) and 13 able-bodied controls (Con) during two phases: sitting (PS) and orthostatic challenge (PO). Beat-to-beat SBP and IBI sequences were obtained from continuous blood pressure recording. Closed loop of SBP-IBI interaction was mathematically opened by bivariate autoregressive model; causal coherence and baroreflex sensitivity (BRS) were calculated in baroreflex direction. Coherence quantifies causal synchronicity between SBP and IBI. The gain of transfer function from SBP to IBI represents BRS. PS (medians of CSCI/ThSCI/Con) coherence was 0.28/0.33/0.25 (no significant difference) and PS BRS was 6.98/7.54/6.66 (no difference). PO coherence was 0.18/0.58/0.45 (CSCI < ThCSI and Con; p < 0.01) and PO BRS was 2.38/5.87/6.22 (CSCI < ThCSI and Con; p < 0.01). For position change effect, there was no change in CSCI coherence; for ThSCI and Con, PS < PO (p < 0.05). For BRS in the CSCI group, PS < PO (p < 0.01); for ThSCI and Con, there was no change. BRS and coherence correlated negatively with SCI level (p < 0.01). In conclusion, baroreflex dysfunction in SCI patients was detected using causal analysis methods during orthostatic challenge only. Baroreflex dysfunction is probably an important mechanism of the more expressed blood pressure decrease associated with CSCI. The severity of autonomic dysfunction was related to SCI level.
Introduction
S
Cardiovascular complications are responsible for about 40% of mortality after SCI. 5 Importantly, changes in the cardiovascular autonomic control after thoracic and cervical SCI can significantly contribute to the development of many secondary health complications, including coronary artery disease, orthostatic hypotension, deep venous thrombosis, and autonomic dysreflexia. 4,6 –9
Baroreflex—as the most important cardiovascular reflex—controls blood pressure by heart rate changes mediated predominantly by parasympathetic activity modulation and by influencing peripheral vascular resistance via sympathetic activity. Impaired vascular response mediated by baroreflex is suggested to be one of the factors predisposing to orthostatic hypotension occurring in almost three-quarters of patients with SCI. 6,10 –13 Orthostatic hypotension accompanied by insufficient brain perfusion in many patients results in an orthostatic syncope—a potentially dangerous and daily activities–limiting condition. 6 Patients with thoracic SCI experience these events less often, compared with those with cervical SCI. 10
Although it is assumed that cardiac baroreflex pathways are intact in patients with SCI, baroreflex sensitivity (BRS) quantifying heart rate response related to blood pressure changes has been studied in these patients in several studies with contradictory results; while in some studies a decreased BRS in patients with high level SCI was shown, in the majority of studies no BRS change in SCI patients was reported. 12,14 –20 However, previous studies focused on the BRS analysis in SCI patients ignored the bidirectional closed-loop interaction between inter-beat intervals (IBI) and systolic blood pressure (SBP; the existence of IBI influence on SBP in addition to expected baroreflex influence from SBP to IBI), potentially severely influencing the analysis results. 21 –23
Therefore, the present study was focused on the baroreflex function assessment by analysis of interactions between IBI and SBP considering the bidirectional closed-loop interaction between IBI and SBP in patients with traumatic spinal cord lesion. Moreover, since the orthostatic challenge might demask the baroreflex impairment in SCI patients, orthostatic test was employed. The influence of the spinal cord lesion level on baroreflex function also assessed based on the hypothesis of the more expressed baroreflex impairment in patients with cervical versus thoracic SCI. 5
Methods
Subjects
Patients with transversal traumatic spinal cord lesion in segments C5-Th12 (on average, 7 years after injury, minimally 3 years) were included in the current study performed during the years 2010–2012. A total of 22 patients were examined in the post-traumatic stage by neurological examination and magnetic resonance imaging. Patients were clinically classified as having complete or incomplete neurological loss based on the presence or absence of motor and sensory function in the lowest sacral segments in accordance with the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). 24 Patients were divided into two groups: 13 patients with cervical SCI (CSCI group) and nine patients with thoracic SCI (ThSCI group). Using American Spinal Injury Association (ASIA) Impairment Scale (AIS), all patients were classified as AIS A. 25 The control group (Con) consisted of 13 healthy able-bodied volunteers (Table 1). All examined patients were in the chronic stage of SCI without any medication affecting the cardiovascular system or autonomic nervous system. All patients regularly (at least two hours a week) performed a physical exercise (appropriate for their handicap) and were familiar with the procedure of verticalization being a part of their physical therapy. Prior to examination, SCI patients catheterized themselves to empty the bladder and all subjects were asked to avoid drinking coffee, black tea and all caffeinated drinks.
Age and body mass index (BMI) are presented as median (lower quartile-upper quartile).
Con, able-bodied controls; ThSCI, patients with thoracic SCI; CSCI, patients with cervical SCI.
The study was approved by ethical committee of the Faculty of Medicine at Masaryk University Brno, Czech Republic. All subjects included in the study signed informed consent based on the World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects, and were informed about the study aim and applied examination methods.
Experimental protocol
Arterial blood pressure was measured continuously and non-invasively in a quiet room (temperature, 22°C) using the volume-clamp plethysmography method according to Penaz (Finometer; FMS, the Netherlands). The study protocol consisted of two phases: 1) 10 min at rest in sitting position with paced breathing at a frequency of 0.33 Hz (20 breaths per min) and 2) 8–10 min in the orthostatic phase. No participant experienced difficulties in following the metronome when controlling the breathing pattern. An orthostasis of SCI patients—a verticalization—was performed using a Balance Thera-trainer device (Medica Medizintechnik GmbH, Germany) while an orthostatic challenge of controls was performed as an active standing.
For analysis, blood pressure recordings taken after 5 min of sitting (phase 1) and after position change (phase 2) were selected. The first stationary segment of the signal in the orthostatic position was chosen for the analysis to avoid the influence of muscular spasms in lower extremities often occurring in SCI patients. In the upright position, we monitored if subjects developed pre-syncopal symptoms (light-headedness, dizziness, blurred vision). In the case of pre-syncopal symptoms occurrence, the patients (seven from the CSCI group, none in ThSCI) were returned back to a sitting position.
Data analysis
Values of SBP, diastolic blood pressure (DBP), and IBI (defined as a time interval between two neighboring local blood pressure minima corresponding to DBP) were detected from the continuous blood pressure signal for each heartbeat. As a result, we obtained sequences of beat-to-beat IBI, SBP, and DBP values denoted as ibi, sbp, and dbp, respectively. Time series of pulse pressure (pp) were computed as the difference between corresponding SBP and DBP values. The time series of ibi and sbp were aligned as follows: the i th SBP value occurred inside the i th IBI. The analysis of IBI–SBP interactions was done on 300 beats long sequences of ibi ([ibi 1 , ibi 2 ,…, ibi300]) and sbp ([sbp 1 , sbp 2 , …, sbp300]). Mean values of the ibi, sbp, dbp, and pp (mIBI, mSBP, mDBP and mPP, respectively) were calculated.
Power spectra of IBI were computed using fast Fourier transform on ibi sequence. Before power spectra estimation, non-equidistantly sampled signal ibi was interpolated by cubic spline and resampled at a frequency of 4 Hz. Value of HFSp 2 ibi was calculated as a mean spectral power in the high frequency band (HF; 0.15–0.5 Hz) to quantify the respiratory sinus arrhythmia magnitude reflecting parasympathetic activity. 26 –28
Mutual interactions between SBP and IBI were estimated by linear bivariate autoregressive model enabling a separate evaluation of causal coherences and gains in both directions (from SBP to IBI and from IBI to SBP). 22,23,29 The unidirectional causal coherence and gain were calculated to minimize an effect of non-baroreflex interaction (transfer of oscillations from IBI to SBP) on baroreflex sensitivity estimation. Causal coherence (Coh 2 sbp→ibi) represented the strength of linear coupling from SBP to IBI in the low frequency band (LF; 0.04 – 0.15 Hz). Causal gain (Gainsbp→ibi) of transfer function from SBP to IBI in LF band represented baroreflex sensitivity (BRS). BRS is defined as a change of IBI caused by a change of SBP by 1 mm Hg. LF band was used to avoid the respiratory oscillations influence on the analysis of causal IBI–SBP interactions.
Statistical analysis
Because of the non-Gaussian data distribution, non-parametric statistical analysis was employed. Between-group comparisons were evaluated by Kruskal-Wallis test (non-parametric analysis of variance), followed by Mann-Whitney post hoc test. The differences between positions were analyzed by Wilcoxon test. The level of spinal lesion was transformed into a variable hL as follows: C1 = 1, C2 = 2…, Th1 = 8, …, Th11 = 18. Then, the correlation between cardiovascular measures and hL was estimated by Spearman correlation analysis. The results are presented as median (lower quartile-upper quartile) and p values ≤0.05 were considered to be statistically significant.
Results
Between-group differences
Basic cardiovascular characteristics of the groups are summarized in Table 2. During both phases of the measurement protocol—sitting and orthostasis—CSCI patients showed significantly lower SBP and PP than Con and ThSCI subjects. During orthostasis, IBI was shorter in CSCI than in Con.
Median (lower quartile-upper quartile) of cardiovascular variables computed for the control (Con), thoracic spinal cord lesion (ThSCI), and cervical spinal cord lesion (CSCI) groups. Variables: inter-beat interval (IBI), systolic blood pressure (SBP), diastolic blood pressure (DBP), and pulse pressure (PP).
Significance of differences between phases of sitting and orthostasis (Wilcoxon test): °0.05 < p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001.
Significance of differences between groups of Con, ThSCI, and CSCI (Mann-Whitney test):
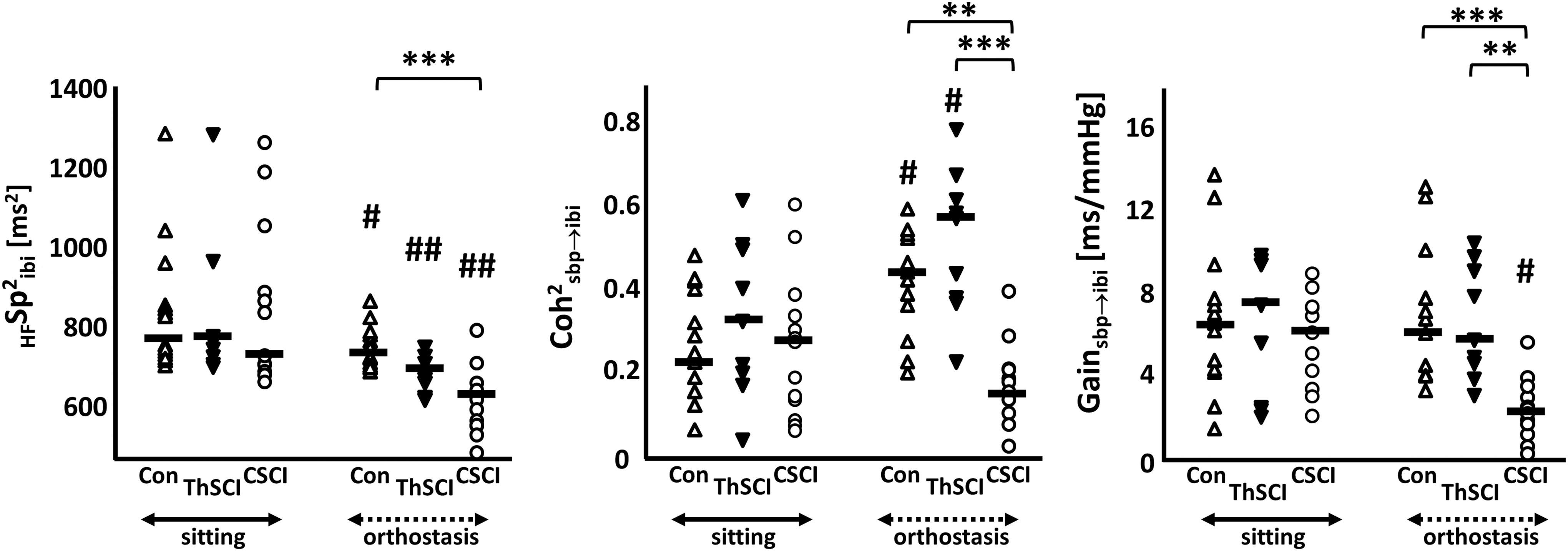
Causal baroreflex related coherence and gain (Coh 2 sbp→ibi and Gainsbp→ibi, respectively) did not differ between groups at rest in the sitting position. In contrast, significant between-group differences were found in orthostatic position (Fig. 1): CSCI exhibited lower causal coherence Coh 2 sbp→ibi and lower causal gain Gainsbp→ibi than the other two groups. Moreover, during orthostasis spectral power of IBI oscillations in HF band (HFSp 2 ibi) was lower in CSCI group, compared with controls.
Distribution of the HFSp
2
ibi, Coh
2
sbp→ibi and Gainsbp→ibi.. in examined groups: healthy controls (Con, Δ); thoracic spinal cord injury (ThSCI, ▿); cervical spinal cord injury (CSCI, o) during sitting and orthostasis. Variables: HFSp
2
ibi, spectral power of inter-beat intervals in high frequency band (0.15–0.25 Hz), Coh
2
sbp→ibi, causal coherence in baroreflex direction in the low frequency band (0.04–0.15 Hz), Gainsbp→ibi, causal gain in the low frequency band (baroreflex sensitivity). Significance of differences between groups (Kruskal-Wallis post hoc test): **p < 0.01, ***p < 0.001. Significance of differences between phase of sitting and phase of verticalization (Wilcoxon test):
Differences between experimental phases
Compared with in the sitting position, IBI decreased in each group during orthostatic challenge (in ThSCI the decrease was of borderline significance; p = 0.066). Mean SBP and DBP during orthostasis decreased significantly in the CSCI group only, while DBP increased in controls. PP decreased significantly in the control group and a decrease of borderline significance was observed in the CSCI group (p = 0.064).
Compared with in the sitting position, causal coherence in baroreflex direction Coh 2 sbp→ibi during orthostasis increased in controls, while no significant change in baroreflex gain (Gainsbp→ibi) was found. Similar changes were observed in ThSCI. On the other hand, in the CSCI group, both HFSp 2 ibi and causal baroreflex gain decreased during verticalization. HFSp 2 ibi significantly decreased in all groups: the largest decrease was found in CSCI and the smallest one in Con (difference between sitting and orthostasis was significantly lower in Con than in CSCI; p = 0.041).
Correlation of cardiovascular control measures with spinal cord lesion level
Spearman correlation analysis of HFSp 2 ibi, Coh 2 sbp→ibi, and Gainsbp→ibi with the level of spinal cord lesion (hL) are presented in Figure 2. During sitting, no correlation of assessed measures with hL was found (rs = 0.174–0.217; p = 0.332- 0.438). In the vertical position, HFSp 2 ibi, Coh 2 sbp→ibi, and Gainsbp→ibi significantly decreased with the decrease in hL (i.e., the higher the spinal lesion [from Th11 to C4 segments], the lower the Coh 2 sbp→ibi, Gainsbp→ibi, and HFSp 2 ibi). SBP and PP significantly decreased with the decrease in hL during both positions (sitting – SBP: rs = 0.663; p < 0.001; PP: rs = 0.476; p = 0.025; orthostasis – SBP: rs = 0.707; p < 0.001; PP: rs = 0.712; p < 0.001). Mean values of IBI and DBP did not correlate significantly with hL (rs = −0.046–0.397; p = 0.067–0.837) in any position.
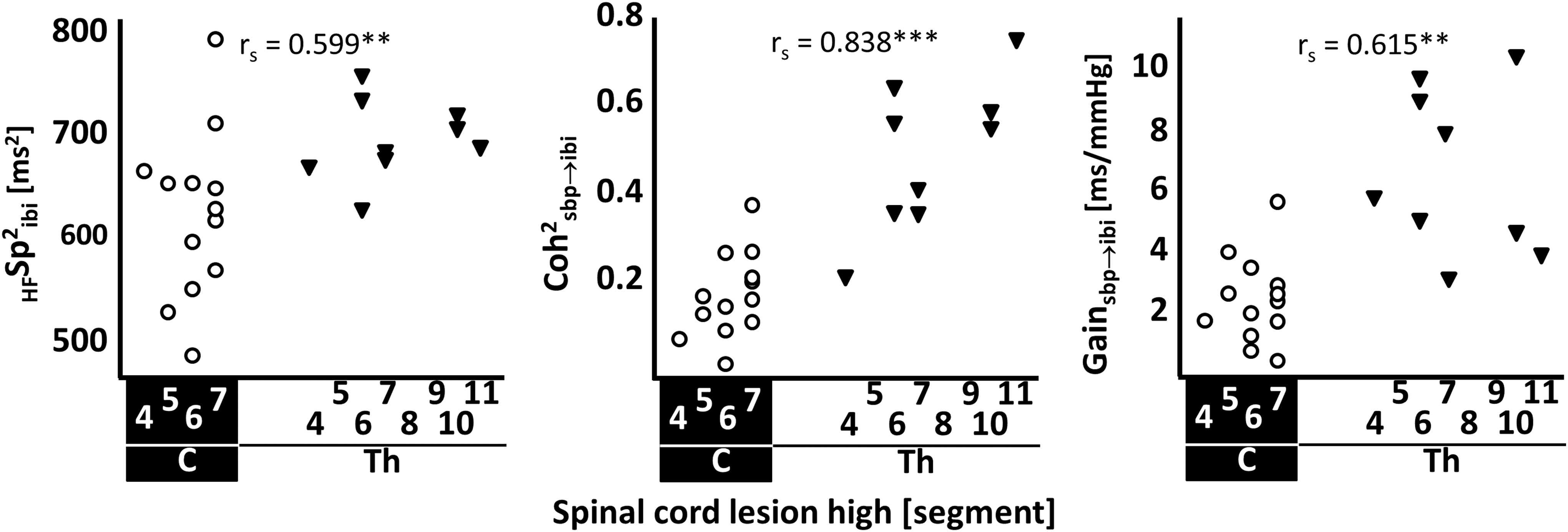
Dependence of the HFSp 2 ibi, Coh 2 sbp→ibi, and Gainsbp→ibi on spinal cord lesion level during orthostasis in both groups of patients (thoracic [Th] spinal cord injury, ▿ and cervical [C] spinal cord injury, o). Variables: HFSp 2 ibi, spectral power of inter-beat intervals in high frequency band (0.15–0.25 Hz); Coh 2 sbp→ibi, causal coherence in baroreflex direction in the low frequency band (0.04–0.15 Hz); Gainsbp→ibi, causal gain in the low frequency band (baroreflex sensitivity). Significance of the Spearman correlation rs: **p < 0.01, ***p < 0.001.
Discussion
The major findings of our study can be summarized as follows: First, using analysis taking into consideration both feedback (baroreflex) and feedforward (non-baroreflex) interactions between SBP and IBI, Gainsbp→ibi quantifying baroreflex sensitivity was preserved during orthostasis in Con and ThSCI, but decreased in CSCI group. Nonsignificant differences between groups were observed during a sitting rest. Second, in all groups, orthostasis led to a decrease of IBI variability in HF band (respiratory sinus arrhythmia). This decrease was strongest in the CSCI patients. Third, although IBI decreased in CSCI during orthostasis, this baroreflex reaction did not prevent a decrease in blood pressure in this group.
Baroreflex function in patients with spinal cord lesion
At rest (in sitting or supine position), previous studies assessing BRS in patients with SCI provided contradictory results. When BRS was estimated by a stimulation of baroreceptors through neck suction, baroreflex dysfunction in SCI patients was detected, 15,18 whereas studies using the Oxford technique or Valsava maneuver did not find any change in BRS. 17 –19 Methods of BRS estimation from spontaneous SBP and IBI oscillations (time-domain sequence method and cross-spectral analysis) were not able to reveal a baroreflex dysfunction in cervical SCI in supine rest. 12,14,17,20,30
Spontaneous BRS during orthostatic stress was analyzed in few studies only. BRS differed between cervical SCI group and able-bodied controls during orthostatic stress. In addition, a decreased BRS in orthostatic stress, compared with resting conditions, was found in patients with cervical SCI only. 12,14,20 Munakata and colleagues observed even an increase of BRS in high-level SCI, compared with the supine position, during orthostatic stress, 12 but this unexpected result can be attributed to the inclusion of non-baroreflex coupling between IBI and SBP at respiratory frequency in this study. When thoracic SCI patients were studied, no difference in BRS versus able-bodied subjects was found. Taken together, common findings of the previous studies employing spontaneous BRS analysis were in accordance with present study—preserved baroreflex function in ThSCI and an impaired baroreflex function in patients with cervical SCI demasked during orthostatic stress.
Closed-loop interaction between IBI and SBP
Importantly, none of the above-mentioned studies took into consideration that IBI and SBP mutually interact in a closed-loop: IBI influences SBP by feedforward non-baroreflex ways, while as SBP influences IBI via feedback control baroreflex pathway. Many recent studies demonstrated that non-baroreflex transfer of oscillations prevailed over the baroreflex mediated oscillations transfer at rest. Heart rate (or IBI) oscillations are transferred to SBP oscillations by several mechanisms, including Frank-Starling mechanism and run-off effect. Therefore, traditionally computed BRS is significantly affected by non-baroreflex influences and results on BRS using non-causal approaches can be markedly distorted. 21,31 –34
Considering a bidirectional closed-loop interaction between IBI and SBP, our study represents the first study applying the causal approach for BRS assessment in patients with SCI. The advantage of this approach is a possibility to mathematically open closed-loop interaction between IBI and SBP and to quantify baroreflex feedback characteristics separately from the non-baroreflex influences. BRS calculated as a causal gain (Gainsbp→ibi) of the transfer function from SBP to IBI, and a coherence (Coh 2 sbp→ibi) expressing a synchronicity between SBP and IBI were calculated as two principal baroreflex function characteristics in our study.
Resting BRS and Coh 2 sbp→ibi did not differ between assessed groups. While there was no change in BRS, an increase of Coh 2 sbp→ibi was observed in both ThSCI and Con groups as a response to orthostatic challenge. In contrast, CSCI patients showed a decrease in the BRS together with an unchanged Coh 2 sbp→ibi during orthostasis.
Several mechanisms can be involved in observed BRS and coherence changes in controls and ThSCI groups. Based on the mathematical model presented by Porta and colleagues, 23 we suggest that resting variability of IBI contains a large amount of non-baroreflex “noise” (i.e., IBI variability not caused by baroreflex, including respiratory sinus arrhythmia). This manifests as a lower synchronization between SBP and IBI oscillations (a lower coherence Coh 2 sbp→ibi) in all groups. Orthostasis suppresses this “noise” in IBI variability and, if baroreflex gain is not changed, Coh 2 sbp→ibi increases.
The above-described effects are not present in CSCI patients: Coh 2 sbp→ibi did not change as a response to orthostasis while Gainsbp→ibi decreased. A decrease in baroreflex gain can be explained by a prominent decrease in vagal activity demonstrated also by the most expressed HFSp 2 ibi drop in CSCI group. This vagal activity suppression could be associated with an excessive blood pressure decrease related to insufficient sympathetic vascular control (vasoconstriction) in CSCI patients. As an alternative explanation, since a slope of IBI–SBP relation is sigmoidal (Fig. 3), a shift towards lower SBP values could be associated with a less steep dependency of IBI on SBP, hence expressed as a lower baroreflex gain. 35,36 Based on the above-mentioned mathematical model, Coh 2 sbp→ibi did not correspondingly increase during orthostasis in CSCI group, when BRS together with other IBI oscillations decreased simultaneously.

Dependence of R–R interval on systolic blood pressure (graph modified from publications of Korner and colleagues 35 and Parlow and colleagues). 36 Graph illustrates possible reason for changed baroreflex sensitivity (BRS) in cervical spinal cord injury (CSCI) compared with thoracic spinal cord injury (ThSCI) and able-bodied controls (Con).
Similarly to our observations, an increase of the causal information transfer strength or an increased coherence from SBP to IBI during passive orthostasis (head-up tilt test) was observed in healthy persons. 21,31,37 Legramante and colleagues observed increased number of baroreflex sequences (an increase of SBP associated with an increase of IBI) in able-bodied subjects together with no change in this measure in patients with cervical SCI during head-up tilt, compared with supine rest. 20 Number of baroreflex sequences can be regarded as a non-causal analogy to the coherence measure.
Coh 2 sbp→ibi and Gainsbp→ibi during orthostasis significantly correlated with a level of spinal cord lesion: the higher the lesion, the lower the coherence or gain. Similarly, a significant correlation between SCI level and Mayer waves amplitude (LF power) in SBP oscillations in cervical, thoracic, and lumbar SCI (ASIA A) during head-up tilt was found. A changed SBP oscillations magnitude can be related to a suppression of baroreflex buffering associated with a higher lesion. 12
Heart rate and blood pressure changes
Blood pressure control in patients with SCI in chronic state is known to be altered: mean blood pressure is often decreased, compared with able-bodied subjects and many SCI patients suffer from strong orthostatic hypotension negatively influencing their daily life. Supraspinal sympathetic activity under spinal cord lesion is partially disrupted or completely interrupted in SCI, while vagal cardiac innervation remains intact. This leads to a decreased vascular tone and peripheral vascular resistance, and consequently to a decreased blood pressure not only during orthostatic stress but even at rest. Sympathetic impairment directly influences a function of the blood pressure control system, including baroreflex, potentially being the major mechanism of orthostatic hypotension in SCI patients—its severity depends on SCI level (sympathetic nerves exit spinal cord in segments C8-L3). It was demonstrated that cardiovascular complications occur more often in patients with SCI above the sixth thoracic segment (Th6). 2
Impaired baroreflex function in CSCI and preserved baroreflex function in ThSCI and Con groups partially explain the observed changes in blood pressure and IBI. Baroreflex increases the peripheral resistance and heart rate during orthostasis as the physiological reaction preventing blood pressure drop. Accordingly, a decreased IBI during orthostatic stress was observed in all groups, because of the anatomically intact and well-functioning cardiovagal baroreflex pathway.
In contrast, sympathetic baroreflex mediated control of vessels was expected to be impaired in SCI (mostly in CSCI). 2,38 Sympathetic dysfunction manifested in CSCI as the lowest SBP value during sitting, compared with ThSCI and Con. A further decrease of blood pressure in CSCI observed during orthostasis was caused not only by impaired sympathetic baroreflex branch but also by cardiac baroreflex dysfunction demonstrated as a decreased BRS. Moreover, CSCI patients had a lower PP in both phases, indicating an impaired venous return and lower stroke volume, caused by an absent skeletal muscle pump effect. 39
Similarly to controls, mean SBP was not significantly changed during orthostasis in ThSCI. It reflects a net effect of the partially preserved sympathetic vascular control and intact cardiac baroreflex function in this group. With regard to CSCI patients, elevated heart rate without a sufficient peripheral vascular resistance increase was not effective enough to maintain blood pressure level during orthostatic challenge. Different behavior of IBI and blood pressure in patients with cervical versus thoracic SCI also was observed in previous studies, 9,12,14,20 and our study provides several possible explanations for the observed differences.
Clinical significance
Our results indicate that baroreflex dysfunction, as quantified by novel and more physiologically relevant causal measures, and hence an impaired short-term blood pressure control during orthostasis is related to SCI level. We found that not only vascular sympathetic baroreflex component is impaired, but cardiovagal baroreflex function can be significantly decreased in CSCI patients during orthostatic challenge. The observed phenomena are the potential mechanisms leading to an orthostatic syncope complicating daily life in some SCI patients.
Physiotherapeutic training of baroreflex might improve blood pressure control in SCI patients. Alternatively, compression stockings can help to increase venous return and prevent blood pressure drop during orthostasis. Whether training or compression stockings would be effective enough to prevent blood pressure drop or to prevent an occurrence of orthostatic syncope will require further research. We expect that a methodology of more refined baroreflex function assessment introduced in this study can be used in future for the monitoring of baroreflex dysfunction progression or its improvement during a rehabilitation process.
Study limitations
Patients were classified as a sensorimotor complete (AIS A) according to the ISNCSCI. However, with regard to the autonomic nervous system, spinal cord lesion could be incomplete in some of our patients with partially preserved sympathetic pathways. The first version of the international standards to examine remaining autonomic function in SCI was published in 2009 and the first revision was prepared in 2012. 40,41 Data presented in this study were collected between years 2010 and 2012, when International Standards to document remaining Autonomic Function after Spinal Cord Injury were still not generally used in clinical practice. Regardless, completeness of the autonomic control loss and causal baroreflex coherence and gain significantly correlated with SCI level and differed between CSCI and ThSCI or controls during orthostasis. It indicates that despite a potentially confounding variable of autonomic loss completeness, cardiovascular dysregulation, including baroreflex dysfunction, is clearly related to the SCI level.
A difference in the type of orthostatic challenge between SCI and control groups could be considered as another potential study limitation. Passive orthostasis effect in SCI (verticalization effect) is compared with an active orthostasis (active standing) effect in able-bodied subjects. Our goal was to compare the cardiovascular responses with normal daily life challenges. We cannot exclude that a difference between SCI and control groups can be attributed to this methodological difference. However, our results indicate that this effect is small—there was a similar effect of orthostasis on ThSCI and control subjects. In addition, a significant difference between CSCI and ThSCI groups was detected despite the application of the same orthostatic challenge procedure.
Conclusion
We conclude that baroreflex dysfunction in SCI patients was detected using causal analysis methods during orthostasis only. Baroreflex dysfunction could be an important mechanism of the more expressed blood pressure decrease occurring in CSCI. The severity of autonomic dysfunction was related to SCI level.
Footnotes
Acknowledgments
The work was supported by following grant projects: MUNI/A/1355/2016, APVV-0235-12, VEGA 1/0117/17, VEGA 1/0202/16, project “Biomedical Center Martin,” ITMS code: 26220220187, the project co-financed from EU sources and project no.LQ1605 from the National Program of Sustainability II (MEYS CR).
The authors wish to thank Eva Zavodna, MD, PhD, and Monika Reznickova, MSc, for their help with obtaining the data.
Author Disclosure Statement
No competing financial interests exist.