
Abstract
While pathophysiology underlying post-concussion symptom burden is unknown, data suggest that cerebrovascular dysfunction may be among the culprits. We sought to determine whether the degree of impairment in the ability of cerebrovasculature to buffer against changes in arterial gases (vasoreactivity) is associated with concussion symptoms. In 15 participants (19 ± 5 years, 1 week to 1 year post-injury) diagnosed with concussion, we assessed vasoreactivity from the slope of the linear relationship of beat-by-beat middle cerebral artery blood flow velocity (transcranial Doppler ultrasound) to end-tidal CO2 during progressive increases in end-tidal CO2 (air rebreathing). Symptom burden was assessed using the Post-Concussion Symptom Scale. Subsequently, we explored the relationship between vasoreactivity and the severity of post-concussion headache and cognitive difficulties by linear models. During rebreathing, CO2 increased from 32.6 ± 1.6 to 46.8 ± 1.8 mmHg and cerebrovascular conductance (i.e., flow velocity over pressure) increased from 0.48 ± 0.04 to 0.74 ± 0.06 cms−1 mmHg−1. There was a strong linear relationship between the increase in CO2 and in conductance (R2 = 0.81 ± 0.05; p < 0.05). On average, cerebral vasoreactivity was 0.018 ± 0.003 cm−1 s−1 mmHg CO2 −1. Although vasoreactivity tended to be somewhat higher in the asymptotic participants (0.019 ± 0.003 vs. 0.015 ± 0.005 cm−1 s−1 mmHg CO2 −1), this difference was not statistically significant (p = 0.48). Higher vasoreactivity was strongly associated with more severe headaches (R2 = 0.57; p < 0.01) and worse cognitive symptoms (R2 = 0.71; p < 0.01). Thus, cerebral vasoreactivity relates strongly to post-concussive headache and cognitive symptom burden. This has significant implications for understanding the pathophysiology underlying post-concussive symptom burden and for devising effective treatment options.
Introduction
A
After concussion, optimal cerebral blood flow is necessary to meet the metabolic needs of the injured brain. However, cerebral blood flow is diminished globally post-injury 5 (although there are reports that severe injuries may be associated with hyperperfusion attributed to a reduction in metabolic needs 6 ), suggesting a derangement in cerebrovascular function. Among the primary mechanisms of cerebrovascular function is its ability to respond changes in arterial carbon dioxide (CO2) level. This is a key mechanism given that arterial CO2 can fluctuate widely from one breath to the next and can change significantly with everyday stressors, such as moving from supine to upright postures. 7 Hypercapnia (i.e., high CO2) leads to vasodilation and increases in flow, whereas hypocapnia (i.e., low CO2) leads to vasoconstriction and decreases in flow. This response, termed “cerebral vasoreactivity,” is a vital homeostatic function that helps regulate and maintain central pH.
In animal models, a disruption in cerebral vasoreactivity is typical in the days immediately after occurrence of mild brain injuries. 8 This has also been observed after sport-related concussion. 9 It should be noted that impairments in vasoreactivity may be associated with the development and persistence of symptoms similar to those observed after a concussion. For example, studies on individuals with migraine have shown that both the increase and decrease in cerebral blood flow in response to hypercapnia and hypocapnia are excessive compared to nonmigraine controls. 10 Thus, it is possible that impairment in cerebral vasoreactivity may play a role in the manifestation of prolonged post-concussion symptoms. However, whereas some studies with athletes who had recently been diagnosed with a concussion reported that vasoreactivity is reduced, 9,11,12 one 12 reported that this impairment may resolve within 4 days post-injury, and none explored whether there is a link between this impairment and post-concussion symptom burden. We sought to explore this relationship, and hypothesized that the degree impairment in cerebral vasoreactivity is related to the symptom burden.
Methods
We conducted a cross-sectional cohort study to determine whether impairment in cerebral vasoreactivity was associated with concussion symptoms. We recruited 15 young adults who were diagnosed by primary care sport medicine physicians and cared for at an outpatient sports concussion clinic within a period of 1 week to 1 year post-injury. All participants were normotensive, nonsmokers, free from cardiovascular and neurological diseases, not on any cardiovascular medications, and of average body weight and height for their age (Table 1). The study protocols were approved by institutional review boards of Spaulding Rehabilitation Hospital and Boston Children's Hospital and conformed to the Declaration of Helsinki. All participants gave their written informed consent before their participation.
BMI, body mass index; PCSS, Post-Concussion Symptom Scale.
Study protocols
Upon recruitment and screening, volunteers participated in a 1-h study session. Because subjects were recruited, screened, and studied the same day as their clinic visit (to minimize subject burden), we were not able to strictly control for volunteers' alcohol and caffeine intake and physical activity, which may impact cerebral blood flow. Instead, we asked our volunteers whether they consumed any alcoholic of caffeinated beverages within the last 24 h and about their physical activity within the last 48 h. None of the volunteers consumed any alcohol within 24 h, and only 1 subject had a coffee the same day as his clinic/study visit. All but 1 were normally active (walking, yoga, or leisurely biking) within the last 48 h (1 had a 3-h basketball practice the day before).
During the study session, volunteers were instrumented for measurements of beat-by-beat arterial waveforms (Portapres Blood Pressure System, Finapres, Ohmeda), end-tidal CO2 (Vacumed, Silver Edition) measured through a sampling tube, and cerebral blood flow velocities. For cerebral blood velocities, a transcranial Doppler ultrasound (Spencer S3) probe was placed on the right temple to measure flow velocity at the M1 segment of the right middle cerebral artery (MCA) at a depth of 45–65 mm. Although this signal is velocity and not flow, there are close correlations between relative changes in cerebral flow velocity and flow assessed by various techniques: xenon; single-photon emission computed tomography; magnetic resonance imaging (MRI), and direct Fick calculations from the arterial to jugular venous oxygen difference. 13 –15 Moreover, the diameter of the MCA remains relatively constant during mild hypercapnia (6% CO2 rebreathing) and hypocapnia (hyperventilation), 16 and change in diameter and cross-sectional area are observed only when the level of CO2 exceeds ∼2 kPa (i.e., >11–13 mmHg) relative to normocapnia. 17 Thus, flow velocity can be used as an adequate surrogate for cerebral flow.
After instrumentation, we assessed vasoreactivity by measuring the increase in cerebral blood flow velocity in response to progressive increases in inspired CO2 while the subjects were seated. Cerebral vasoreactivity is a standard test of the cerebrovascular vasodilatory responses. After a 1-min baseline acclimatization period, subjects breathed from a 5-liter rebreathing bag filled with room air for 2 min. Vasoreactivity was quantified by plotting breath-by-breath cerebrovascular conductance against the corresponding end-tidal CO2 values. It is possible that arterial pressure may change during air rebreathing, influencing cerebral blood flow independent of changes in end-tidal CO2. Although there was indeed a small increase in arterial pressure during rebreathing (77.9 ± 2.0 mmHg 30 sec before rebreathing vs. 83.0 ± 2.3 mmHg during the last 10 sec of rebreathing, i.e., an increase of 6%), this increase was much less than that in cerebral blood flow (41.3 ± 3.3 vs. 56.7 ± 3.9 cm/s, i.e., an increase of 37%). Therefore, it is unlikely that the increase in cerebral blood flow in response to increases in arterial CO2 can be attributed to the change in arterial pressure. Nonetheless, to account for possible influence of arterial pressure independent of changes in end-tidal CO2, we used cerebrovascular conductance (i.e. flow/pressure), instead of blood flow velocity, to assess vasoreactivity. Subsequently, we used a piece-wise linear regression to determine the linear portion of the relationship between cerebrovascular conductance and end-tidal CO2 (see Fig. 1). This provides a slope of this relationship (change in cerebrovascular conductance per change in end-tidal CO2: cm−1 s−1 mmHg CO2 −1), which can be used to quantify cerebral vasoreactivity.

Representative data from 1 participant showing the estimation of cerebral vasoreactivity. Top three panels show hemodynamic variables, and the bottom panel shows the relationship between cerebrovascular conductance and end-tidal CO2 during 1 min of rest and 2 min of rebreathing (shaded areas). Cerebral vasoreactivity is the slope of the linear portion of this relationship during rebreathing.
Symptom burden
Post-concussion symptom burden was assessed using the Post-Concussion Symptom Scale (PCSS). The PCSS consists of 22 subjectively experienced symptoms, including those in the headache and cognitive domains, and has been used as an outcome measure in numerous published studies. 18 –21 For all volunteers, the PCSS was either obtained immediately before the study session or within less than a week of the study if assessed as part of their clinical care.
Statistical analysis
Results are presented as mean ± standard error. Differences between symptomatic and asymptomatic patients were assessed using a t-test. Relations between cerebral vasoreactivity and symptom burden were assessed by linear regression, and the strength of the associations (i.e., R 2 ) was adjusted for the sample size to ensure maximum generalizability of our results.
Results
Six participants were asymptomatic at the time of study. Among the 9 symptomatic ones, total PCSS ranged from 6 to 30. Mean PCSS score was 5.8 ± 0.9 in the headache domain and 4.8 ± 1.2 in the cognitive domain. There were no differences in symptom burden between males and females (p > 0.45 for all). One participant was studied less than 2 weeks (8 days) post-injury, 6 were less than 3 months post-injury, and 8 were over 3 months post-injury.
Across all participants, mean resting heart rate was 72 ± 3 bpm, mean arterial blood pressure was 77 ± 3 mmHg (120 ± 2 systolic and 61 ± 3 diastolic), mean MCA cerebral blood flow velocity was 47.2 ± 3.8 cm/s, and mean end-tidal CO2 was 34.5 ± 1.1 mmHg. There were no significant differences in any of the resting hemodynamic variables between symptomatic and asymptomatic patients (Table 2).
MCA, middle cerebral artery.
During air rebreathing, end-tidal CO2 increased from 32.6 ± 1.6 to 46.8 ± 1.8 mmHg and cerebrovascular conductance increased from 0.48 ± 0.04 to 0.74 ± 0.06 cm s−1 mmHg−1. As expected, there was a strong linear relationship between CO2 and conductance (R 2 = 0.81 ± 0.05; p < 0.05). On average, cerebral vasoreactivity was 0.018 ± 0.003 cm−1 s−1 mmHg CO2 −1. There was no sex-related difference in vasoreactivity (p = 0.43). Although vasoreactivity tended to be somewhat higher in the asymptotic group (0.019 ± 0.003 vs 0.015 ± 0.005 cm−1 s−1 mmHg CO2 −1 in asymptomatic patients), this difference was not statistically significant (p = 0.48). However, higher vasoreactivity was strongly associated with more severe headache (R 2 = 0.57; p < 0.01) and worse cognitive symptoms (R 2 = 0.71; p < 0.01; Fig. 2). Excluding the volunteer who consumed coffee before the study session or the 1 who participated in basketball training the day before, the study session did not change these relationships (R 2 = 0.58 and 0.72). Thus, cerebral vasoreactivity alone accounted for almost 60% of the variation in post-concussive headache burden and over 70% of the variation in cognitive symptoms.
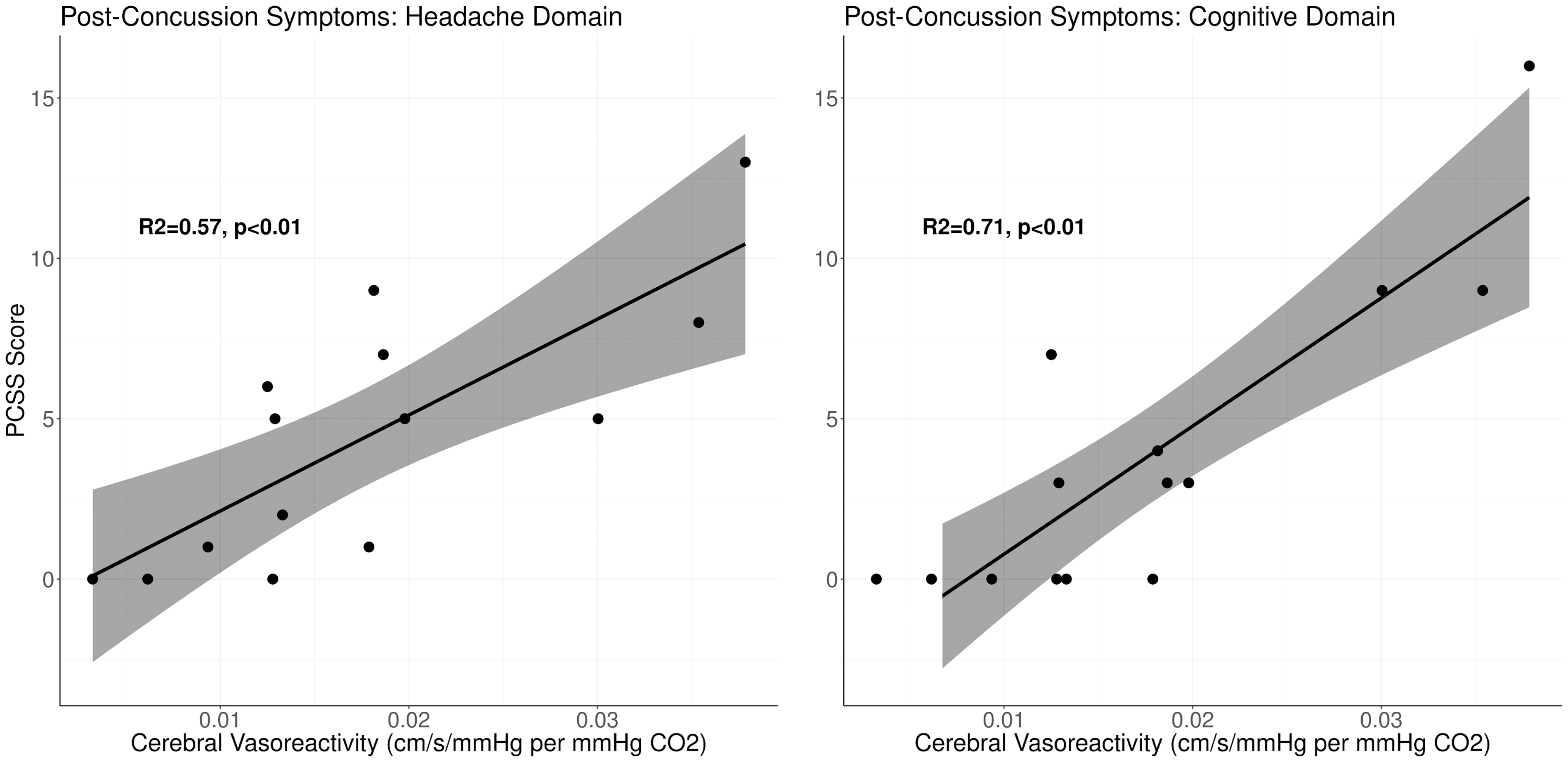
Relation between cerebral vasoreactivity and PCSS scores in headache and cognitive domains. PCSS, Post-Concussion Symptom Scale.
Discussion
In this study, we sought to explore the potential relationship between post-concussive symptom burden and cerebral vasoreactivity (the ability to increase blood flow in response to increase in CO2), a key component of cerebrovascular function. We found a remarkably strong relationship between vasoreactivity and post-concussive headache and cognitive symptom burden: Individuals with more severe post-concussion headaches and cognitive symptoms showed larger responses to CO2. This suggests that cerebral blood flow may be more vulnerable to moment-by-moment variations in arterial gases during recovery from a concussion, and this vulnerability may underlie, at least partly, post-concussive symptom burden.
Our results are in line with other recent observations. In a cohort study of 51 children (24 asymptomatic), Barlow and colleagues explored the relationship between cerebral blood flow measured by arterial spin labeling and post-concussive symptom burden assessed by PCSS, and reported that global cerebral blood flow, when combined with pre-injury symptoms, explained almost half (42%) of the variation in overall post-concussive symptom burden. 22 Another recent study with 25 adult patients who were recently (<3 months) diagnosed with a mild traumatic brain injury (based on American Academy of Neurology criteria) reported a positive (although somewhat weak; r = 0.4) correlation between post-concussive symptom burden (Sport Concussion Assessment Tool 2 scores) and cerebral vasoreactivity assessed by MRI in response to CO2 rebreathing. 23 These results, as well as ours, are similar to previous observations on the development and persistence of comparable symptoms in other populations. For example, both the increase and decrease in cerebral blood flow in response to hyper- and hypocapnia are reported to be higher in migraineurs compared to nonmigraine controls. 10 Moreover, migraineurs with side predominance show stronger responses to hypercapnia compared to healthy controls, and responses appear to be greater on the predominant migraine side, compared to the contralateral side. 24 In addition, the same cohort study by Barlow and colleagues 22 reported that around ∼15% of the variation in cognitive symptoms after a concussion is explained by alterations in cerebral blood flow. Therefore, there is preliminary evidence of a link between cerebrovascular function and post-concussive headache and cognitive symptoms. It should be noted that there are three primary factors that can affect cerebral blood flow: arterial blood pressure, arterial CO2, and neural metabolic demand. 25,26 Therefore, cerebral blood flow at a given moment reflects a combination of three distinct, but potentially interacting, regulatory mechanisms (autoregulation, which buffers against pressure fluctuations; vasoreactivity, which changes blood flow in response to changes in arterial gases; and neurovascular coupling, which mediates local changes in blood flow to meet metabolic demand). 25,26 Each of these mechanisms may relate to different symptoms, and concussion may impact each mechanism differentially. 27 In the current study, we assessed only one critical aspect of cerebral blood flow regulation (i.e., vasoreactivity) explicitly, determined its relation to specific domains of chronic symptom burden (headache and cognitive symptoms), and found that almost 60% of the variation in headache severity and almost three quarters (71%) of the variation in cognitive symptom severity is explained by cerebral vasoreactivity alone. This strong relation has significant implications for understanding the pathophysiology of some concussion symptoms.
Alterations in vasoactive factors, induced by CO2 (and, consequently, pH), are among the main physiological mechanisms of cerebral vasoreactivity responses, and endothelial release of nitric oxide is key among these factors. 28 At the same time, data from both animals and humans suggest that the autonomic sympathetic system may impact cerebral blood flow responses to CO2. For example, in dogs, lowered arterial pressure (yielding to elevated sympathetic outflow) is reported to blunt cerebral vasoreactivity, 29 and in humans, cerebral vasoreactivity increases by almost 50% subsequent to a ganglionic blockade. 30 These data are indicative that the autonomic sympathetic system may restrain cerebral blood flow responses to CO2, although the specifics of this mechanism remain unclear. 25,31 Thus, excessive responsiveness of cerebral vasculature to CO2, when viewed in light of these data, suggest that there may be a derangement in autonomic control after a concussion. In fact, there are also inferential data suggesting that autonomic dysfunction after a brain injury is common. For example, in patients with traumatic brain injuries, heart rate and electrodermal responses are diminished during psychological tasks compared to healthy controls, despite similar state or trait anxiety. 32 Given that increased sympathetic activity mediates the heart rate response in part, 33 and is responsible for the cutaneous response, 34 this may implicate compromised autonomic sympathetic control after a brain injury, although our results do not directly address this possibility.
Current guidelines emphasize the need for diagnostic tools that are useful in identifying individuals at increased risk for severe or prolonged early impairments, and for interventions that enhance recovery and diminish the long-term sequelae of concussion. 35 Our results provide a promising first step toward addressing these needs. Current assessment of symptoms (most notably, headache and cognitive difficulty) associated with a concussion relies primarily on self-reports (albeit using standardized questionnaires) and physician's judgment. In our study, assessment of cerebral vasoreactivity was done in a clinical setting with relative ease (approximately 20 min including instrumentation) using portable equipment available in most hospitals, if not in smaller clinics. Thus, if confirmed in larger and longitudinal cohorts, the strong relation between vasoreactivity and post-concussion symptom burden observed in this study can serve as an objective diagnostic tool.
Although the most effective treatment option to improve vasoreactivity remains to be seen, one nonpharmacological treatment option is mild- to moderate-intensity aerobic exercise training. In healthy population, frequent physical exercise and better aerobic conditioning are associated with better cerebrovascular regulation. 36 During exercise, cerebral blood flow increases up to approximately 60% of maximal oxygen uptake, and returns toward baseline values at higher exercise intensities. 37 This is attributed to intensity-dependent effects of CO2 on cerebral flow during exercise; mild-to-moderate exercise is associated with a small increase in arterial CO2 that increases cerebral blood flow in concert with metabolism. 38 Thus, increased CO2 production attendant to an acute bout of aerobic exercise is accompanied by active engagement of cerebral vasoreactivity to regulate flow in response to hyper- and hypocapnia. 39 Our result suggests that, in symptomatic patients, this mechanism may be impaired such that increases in CO2 production leads to increases in blood flow beyond what is required for cerebral metabolism. This may, in fact, partly underlie exercise-mediated exacerbation of symptoms in some patients. At the same, it is conceivable that regular aerobic exercise training can “condition” cerebrovascular function by consistently engaging cerebral vasoreactivity. In fact, there are preliminary data showing that mild- to moderate intensity aerobic exercise after a concussion is safe, 40 and patients with post-concussion syndrome who exercise as part of their treatment plan have fewer symptoms than patients who were allowed only stretching exercises. 41 Further, preliminary evidence suggests that increased physical activity during recovery from a concussion is associated with shorter symptom duration, particularly among adolescents. 42 Therefore, subsymptom exercise training might serve as a noninvasive, effective therapy to improve cerebral vasoreactivity, potentially mitigating post-concussive headache and cognitive symptoms.
Recently, the main recommendation for the treatment of concussion has consisted mostly of rest, including physical rest and exercise restriction. 43 –45 However, the physical deconditioning that accompanies rest also results in deficits in cerebral blood flow regulation. For example, even a single day of bed rest reduces cerebral blood flow for a substantial period of time afterward, 46 and prolonged physical rest may lead to extreme deconditioning and resultant cardiovascular declines. 47 Thus, the prescribed treatment, physical rest, could result in a further exacerbation of the impairment in cerebral vasoreactivity and, consequently, in a derangement in cerebral blood flow. 48 As a result of this derangement, prolonged rest beyond the first couple of days after a concussion might hinder rather than aid recovery, 49 especially in athletes suffering prolonged symptoms.
Our study is not without its limitations. Although we have shown a remarkably strong relation between cerebral vasoreactivity and post-concussive symptom burden, our study is, by design, cross-sectional. Thus, our data cannot speak to possible temporal relations between cerebral vasoreactivity and symptom resolution, and future longitudinal studies are necessary to explore this relation. Second, our study included a relatively heterogeneous population of concussion patients, with a wide range of time post-concussion. It should be noted, however, that despite this heterogeneity, vasoreactivity alone accounted for a large variation in post-concussive headache (57%) and cognitive symptoms (71%). This result, despite the heterogeneity in symptom burden, suggests that, at worst, we may be underestimating this relationship. Last, we explored just one mechanism (vasoreactivity) of cerebrovascular function. Future work is needed to establish whether other key mechanisms of cerebrovascular function (its ability to buffer against changes in systemic pressure—autoregulation, and its ability to alter regional blood flow to meet metabolic demand—neurovascular coupling) are impaired after a concussion, and whether such impairments also relate to post-concussive symptom burden.
In summary, we have shown that the ability of cerebral vasculature to alter cerebral blood flow in response to changes in arterial CO2 (i.e., vasoreactivity) relates strongly to post-concussive headache and cognitive symptom burden, such that more-excessive elevations in blood flow indicate more severe headache and cognitive difficulties. This observation has significant implications for understanding the pathophysiology underlying post-concussive symptom burden and for devising effective treatment options.
Footnotes
Acknowledgments
Dr. Albalawi is supported by a scholarship from The Neuroscience Center at King Fahad Specialist Hospital, Dammam, Saudi Arabia.
Author Disclosure Statement
Dr. Meehan receives royalties from 1) ABC-Clio publishing for the sale of his books, Kids, Sports, and Concussion: A Guide for Coaches and Parents, and Concussions; 2) Springer International for the book Head and Neck Injuries in Young Athletes; and 3) Wolters Kluwer for working as an author for UpToDate. His research is funded, in part, by philanthropic support from the National Hockey League Alumni Association through the Corey C. Griffin Pro-Am Tournament and by a grant from the Football Players Health Study at Harvard University, which is funded by the NFL Players Association. The other authors declare no potential conflicts of interest.