
Abstract
Our study aim was to assess the neurological outcomes of surgical decompression and stabilization within 5 and 24 h after injury. We performed a multi-center, retrospective cohort study in adolescents and adults 15–85 years of age presenting cervical spinal cord injury (CSCI) at one of 6 Austrian trauma centers participating in the Austrian Spinal Cord Injury Study (ASCIS). Neurological outcomes were measured using the American Spinal Injury Association Impairment Scale (AIS) grade according to the International Standards For Neurological Classification Of Spinal Cord Injury (ISNCSCI) form after at least 6 months of follow-up (FU). Of the 49 enrolled patients with acute CSCI, 33 underwent surgical decompression within 5 h (mean 3.2 h ± 1.1 h; very early group) after injury, and 16 underwent surgical decompression between 5 and 24 h (mean 8.6 h ± 5.5 h; early group). Significant neurological improvement was observed among the entire study population between the preoperative assessment and the FU. We identified a significant difference in the AIS grade at the last FU between the groups the using Jonckheere–Terpstra test for doubly ordered crosstabs (p = 0.011) and significantly different AIS improvement rates in the early group (Poisson model, p = 0.018). Improvement by one AIS grade was observed in 31% and 42% of the patients in the early and very early groups, respectively (p = 0.54). Improvement by two AIS grades was observed in 31% and 6% of the patients in the early and very early groups, respectively (p = 0.03; relative risk [RR], 5.2; 95% CI, 1.1–35). Improvement by three AIS grades was observed in 6% and 3% of patients in the early and very early groups, respectively (p = 1.0). Decompression of the spinal cord within 24 h after SCI was associated with an improved neurological outcome. No additional neurological benefit was observed in patients who underwent decompression within 5 h of injury.
Introduction
T
The pathophysiology of SCI involves the primary mechanical injury, which occurs via the trauma mechanism. Primary injury is triggered by rapid cord compression caused by bone dislocation that directly disrupts axons and blood vessels. The primary mechanical injury initiates a signalling cascade that includes vascular dysfunction, edema formation, ischemia, inflammation, and delayed apoptosis, which comprise the secondary injury phase. 1 –3
A proposed therapeutic approach for the initial phase to improve the neurological outcome of patients is decreasing the secondary injury via early decompression. 4 This approach is based on the goal of promptly reducing pressure on the spinal cord caused by fractures, dislocations, and associated vertebral trauma. 5,6 However, the definitions of “early” and “late” surgery have not been standardized to date. 4
Many pre-clinical and clinical studies examining early decompression have consistently demonstrated improved outcomes. 4,7 –12 In addition, studies using animal models have indicated neurological improvement after fast spinal cord decompression. 13
However, the ideal timing for undergoing surgery following tSCI, particularly general and acute cervical SCI (CSCI) has been widely debated for decades, with arguments both for and against early decompression and surgical stabilization. Early decompression has become more common during the last century, especially when fast transfer to specialized units is feasible and operative capacities are available.
There are currently still no time-related guidelines for decompression in acute tSCI. Proponents for early decompression believe that surgical stabilization in a hemodynamically adequate patient is fundamental for preventing further neurological worsening and may even accelerate healing to foster neurological improvement.
In addition to early decompression preventing further secondary damage, early operative stabilization promotes mobilization and rehabilitation and, therefore, may decrease the likelihood of adverse events developing from prolonged bed rest. A meta-analysis of a small case series showed that decompression within 24 h after injury results in statistically better neurological outcome than late decompression or even conservative means. 13
Nevertheless, proponents of delayed surgery insist that early decompression does not lead to better results and even can harm the patient as a result of additional iatrogenic damage to the swollen cord. 14,15
The purpose of this study was to assess the neurological outcomes of operative decompression and stabilization performed within 24 h of injury and to determine the median time to decompression in cases of isolated traumatic CSCI in Austria. We further evaluated whether very early spinal cord decompression <5 h after injury fosters additional improvements in neurological healing. Neurological outcomes were measured by the American Spinal Injury Association (ASIA) neurological examination using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) form.
Methods
Study design and ethical approval
This study performed a multi-center retrospective analysis of patients with isolated traumatic CSCI who underwent decompression over a 10 year period (2001–2014). The following Austrian trauma hospitals were involved in this study: University Clinic Vienna, Kepler University Clinic Linz, University Clinic of the Paracelsus Medical University Salzburg, Trauma Hospital Linz, Trauma Hospital Salzburg, and State Hospital Feldkirch. Clinical data were collected prospectively from 2012 within a fixed time schedule according to established standards of the Austrian Spinal Cord Injury Study (ASCIS) database. The ASCIS database is a national registry connected to the European Multicenter Study about Spinal Cord Injury (EMSCI) that includes data from tSCI patients in a seven staged follow up (FU) time schedule. The study protocols for the ASCIS were approved by the local ethics committee in Salzburg, and the study was performed in accordance with the declaration of Helsinki. Retrospectively acquired data were presented to the local ethics committee, and this study was approved by the ethics committees of the Austrian Social Insurance for Occupational Risks (AUVA) and of Salzburg. Personal rights were respected in this study.
Patient inclusion and exclusion criteria
Every SCI patient presented to one of the participating centers was assessed for suitability against a predefined set of inclusion and exclusion criteria (Table 1). Data from patients from the participating centers who presented a CSCI from the C2 to the Th1 level and were between 15 and 85 years of age were considered and were included if the following requirements were met: documentation of time of injury and time of surgery; preoperative neurological examination according to the ISNCSCI protocol; preoperative radiological assessment including CT scan or MRI (prior to study or registry enrolment); postoperative neurological examination according to the ISNCSCI protocol at discharge; and last neurological examination according to the ISNCSCI protocol available at least 6 months after injury. The FU of 6 months was based on recommendations used in the National Acute Spinal Cord Injury Study (NASCIS) and Sygen trials. 16 –18 Clinical data from the ASCIS database were collected prospectively within a fixed time schedule according to the established standards at the centers participating in the ASCIS project. For this analysis, the ISNCSCI information collected 1 year or 2–3 years after injury was used.
AIS, American Spinal Injury Association Impairment Scale; CSCI, cervical spinal cord injury; FU, follow up; GCS, Glasgow Coma Scale; ISS, injury severity score.
Because of the retrospective analysis of some patients who were not included in the ASCIS registry, FU examinations performed as routine re-evaluations or as part of repeated rehabilitation sessions had longer FU times. In such cases, the last available clinical status was taken as the ISNCSCI assessment. Trained research assistants or physicians performed the neurological examinations at the indicated time points. A change in American Spinal Injury Association Impairment Scale (AIS) grade was defined as AIS grade improvement and taken as the grade increase within AIS classification grades. Patients with a Glasgow Coma Scale (GCS) of <14, an accompanying traumatic brain injury, history of neurological deficits, or intubation at the time of presentation were excluded from further analysis. In all cases, clinical examinations assessing neurological function were performed by the local treating clinicians. The diagnosis of traumatic CSCI was confirmed by reviewing radiographic images. A radiological examination was performed preoperatively in all cases based on a CT scan or MRI corresponding to local practice on admission. Clinical status was documented in patients' medical records. If calculating the AIS score was not part of the initial assessment protocol, a neurological consultant experienced in evaluating traumatic neurological disorders retrospectively graduated patients based on the documentation of the neurological evaluation. This was possible if all relevant information for assessing the AIS score were available. If essential clinical findings were not documented, and evaluation of the AIS score was not possible, the patient was excluded from further analysis. Any associated injuries were managed accordingly. Patients with severe multiple injuries and an injury severity score (ISS) >25 were excluded. Application of corticosteroids during the initial phase of CSCI was dependent on regional routines and was documented.
Postoperative mobilization and structured physical therapy was introduced after the operation as soon as the patient was medically stable. Patients underwent further therapy in rehabilitation centers after discharge from the hospital, as required. Regular clinical checkups with re-evaluations of neurological status were performed and documented in the patients' records.
Patients were assigned to groups according to decompression time points within the first 5 h after the incident (very early decompression group) and thereafter within 24 h (early decompression group). At all the participating centers, it is common practice to treat patients as soon as is medically and logistically possible under the premise that CSCI patients are highly prioritized. No repeated surgery for inadequate decompression was required in either group. In each group, patients were distributed based on their neurological status upon admission into two subgroups: “complete,” which included patients with AIS A, and “incomplete,” which included patients with AIS B, C and D.
Data collection and management
Clinical trial coordinators together with physicians collected all data beginning with pre-hospital care through the rehabilitation phase in a de-identified manner. Regular FU examinations were required. The following information was collected from medical charts: gender, age, cause of injury, level of injury, type of treatment, neurological status, and hospitalization periods. Data collected within the ASCIS database were provided by the study coordination team in a de-identified manner to respect patient privacy.
Statistical analysis
The data were checked for consistency and screened for outliers. Because of the small sample sizes, Monte Carlo methods were used to test hypotheses in the cross-tabulation tables. Fisher's exact test, McNemar's test, Pearson's χ2 test, and marginal homogeneity were used for unordered cross-tabulations tables, and the Jonckheere–Terpstra test was used for doubly ordered tables. The relative risk (RR) was computed for selected cross-tabulation tables. Independent Student's t tests were used to compare the means of two normally distributed variables. Improvement in terms of the number of steps from the pre-treatment to the FU AIS was modelled using a generalized linear model based on the Poisson distribution with the log link function and pre-treatment AIS as the covariate variables. The robust estimator for the covariance matrix was used. All reported tests were two sided, and p values <0.05 were considered statistically significant. All statistical analyses in this study were performed using STATISTICA 13 (Hill, T., and Lewicki, P. Statistics: Methods and Applications, StatSoft, Tulsa, OK), Mathematica 7 (Wolfram Research, Inc., Mathematica, Version 7.0, Champaign, IL), PASW 22 (IBM SPSS Statistics for Windows, Version 21.0., Armonk, NY), and StatXact 10 (Cytel Software 2013, Cambridge MA) by one of the authors (W.H.).
Results
Study population
A total of 107 subjects were screened for enrolment, among which 49 fulfilled the study inclusion and exclusion criteria (Fig. 1). Of the 49 study participants, 33 underwent surgery <5 h after CSCI and were allocated to the very early surgery cohort. The remaining 16 participants underwent surgery between 5 h and 24 h post-SCI and were allocated to the early surgery cohort. Table 2 provides an overview of the demographic and injury characteristics of the entire study population (0–24 h), the very early surgery group and the early surgery group.
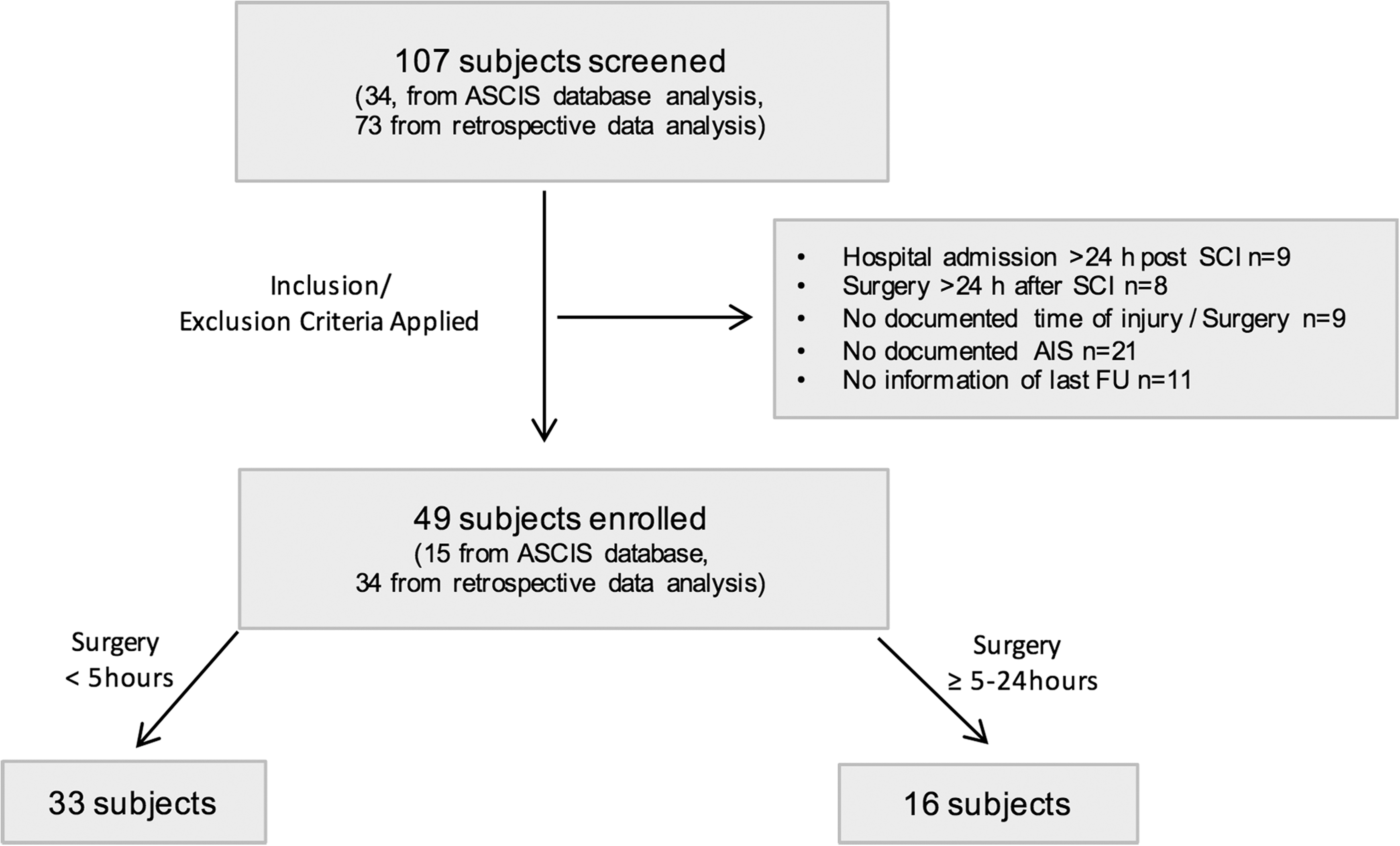
Flow diagram of patient selection.
Student t test. bFisher's exact test. cPearson's χ2 test. dWilcoxon–Mann–Whitney test for two ordered multinomial.
AIS, American Spinal Injury Association Impairment Scale; DC, decompression surgery; FU, follow-up; HA, hospital admission.
In the total study population, the mean age was 50 years ±20 (mean ± SD; min. 15 years; max. 83 years), and the majority of patients (78%) were male. In the very early surgery cohort, the mean age was 47 years ±20 (mean ± SD; min. 15 years; max. 83 years) with 27 males (82%) and 6 females (18%). In the early surgery cohort, the mean age was 55 years ±18 (min. 17, max. 80 years) with 11 males (69%) and 5 females (31%).
The mean time between accident and spinal decompression for the total study population was 4.99 h ± 4.07 (mean ± SD; min 0.5 h to max. 23.9 h). The mean time between accident and hospital admission was 1.37 h ± 0.94 (mean ± SD; min. 0.4 h; max. 4.4 h). In the very early group, the time between accident and surgery was 3.24 h ± 1.06 (mean ± SD; min. 0.5 h; max. 4.93 h), and the patients were admitted to the hospital at 1.00 h ± 0.49 (mean ± SD; min. 0.40 h; max. 2.23 h). The time from accident to surgery in the early cohort was 8.60 h ± 5.47 (mean ± SD; min. 5.00 h; max. 23.9 h), and the time between the accident and hospital admission was 2.12 h ± 1.18 (min. 0.50 h; max. 4.40 h; independent Student's t test, p = 0.002).
The major cause of SCI among the entire study population was falls (40%), of which 22% were falls from a standing level and 18% were falls from a height. The second most common cause of injury was sport or recreational activities (37%). No significant difference was observed in the etiology distribution between both groups (Pearson's χ2 test, p = 0.09) as the primary cause of SCI was sport and recreation activities (39%) followed by falls (30%). In the early group, the most common cause of injury was falls (44%) followed by sport and recreation activities (31%).
The most frequent fracture level of injury was C6 (33%) followed by C5 (29%) and C4 (22%). No significant difference in the level of fracture was observed between the groups (Pearson's χ2 test, p = 0.63).
Neurological outcome
Neurological improvement according to the change in AIS grade from the preoperative assessment until the last FU, at least 6 months after injury, is represented in Tables 3, 4, and 5 and Figure 2. The average time from preoperative AIS scale scoring to the last FU examination was 2.61 years ±2.32 (mean ± SD; min. 0.5 years; max 10.88 years) for the entire study population, 3.14 years ±2.49 for the very early group, and 1.74 years ±1.69 for the early group (Table 2). The total study population included 20 AIS A, 5 AIS B, 12 AIS C, and 12 AIS D patients at admission (Table 2).
American Spinal Injury Association Impairment Scale (AIS) grade change and AIS grade improvement: very early versus early surgical groups.
Marginal homogeneity test indicates significant change over time, p = 0.0001.
AIS, American Spinal Injury Association Impairment Scale; FU, follow-up.
Marginal homogeneity test indicates significant change over time, p = 0.0002.
AIS, American Spinal Injury Association Impairment Scale; FU, follow-up.
Marginal homogeneity test indicates significant change over time, p = 0.0001.
AIS, American Spinal Injury Association Impairment Scale; FU, follow-up.
Total study population
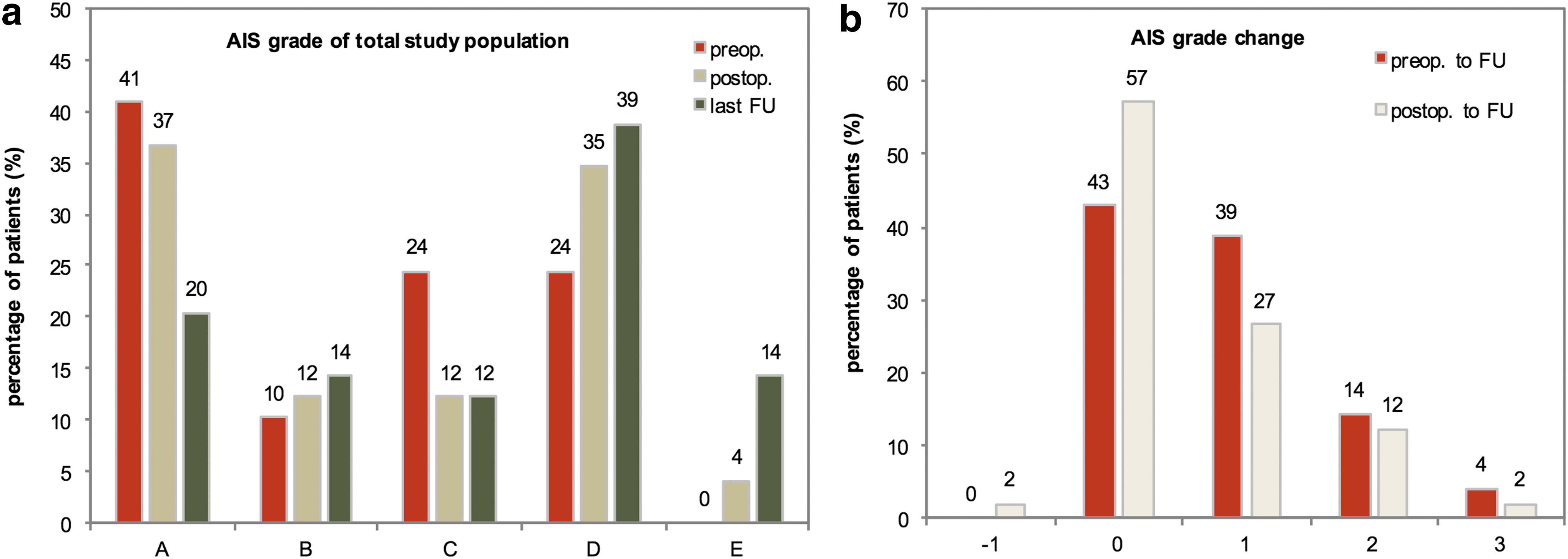
In the total study group, the degree of neurological improvement was significant as measured by a change in AIS grade between the preoperative period to the last FU (marginal homogeneity test, p = 0.0001) (Fig. 3). In general, 28 patients (57%) showed neurological improvement within the total study population. Approximately 41% of the patients had a preoperative AIS grade of A, but only 20% of the patients had an AIS A grade at the last FU (Fig. 3a, McNemar's test, p = 0.002). A remission in terms of resuming the AIS E grade at the last FU was encountered in 14% of all the patients (Fig. 3a). AIS changes are also depicted in Figure 3a at the postoperative AIS examination. The changes in AIS grades from the preoperative period to FU were as follows: 43% showed no improvement, 39% improved by one AIS grade, 14% improved by two AIS grades, and 4% improved by three AIS grades (Fig. 3b). The change in the AIS from the postoperative AIS examination to FU is also depicted in Figure 3b. Fifty-seven percent of the patients showed no AIS improvement, 27% improved by one AIS grade, 12% improved by two AIS grades, and 2% improved by three AIS grades (Fig. 3b).
Distribution of American Spinal Injury Association Impairment Scale (AIS) grade and improvements of the total study population.
Very early versus early populations
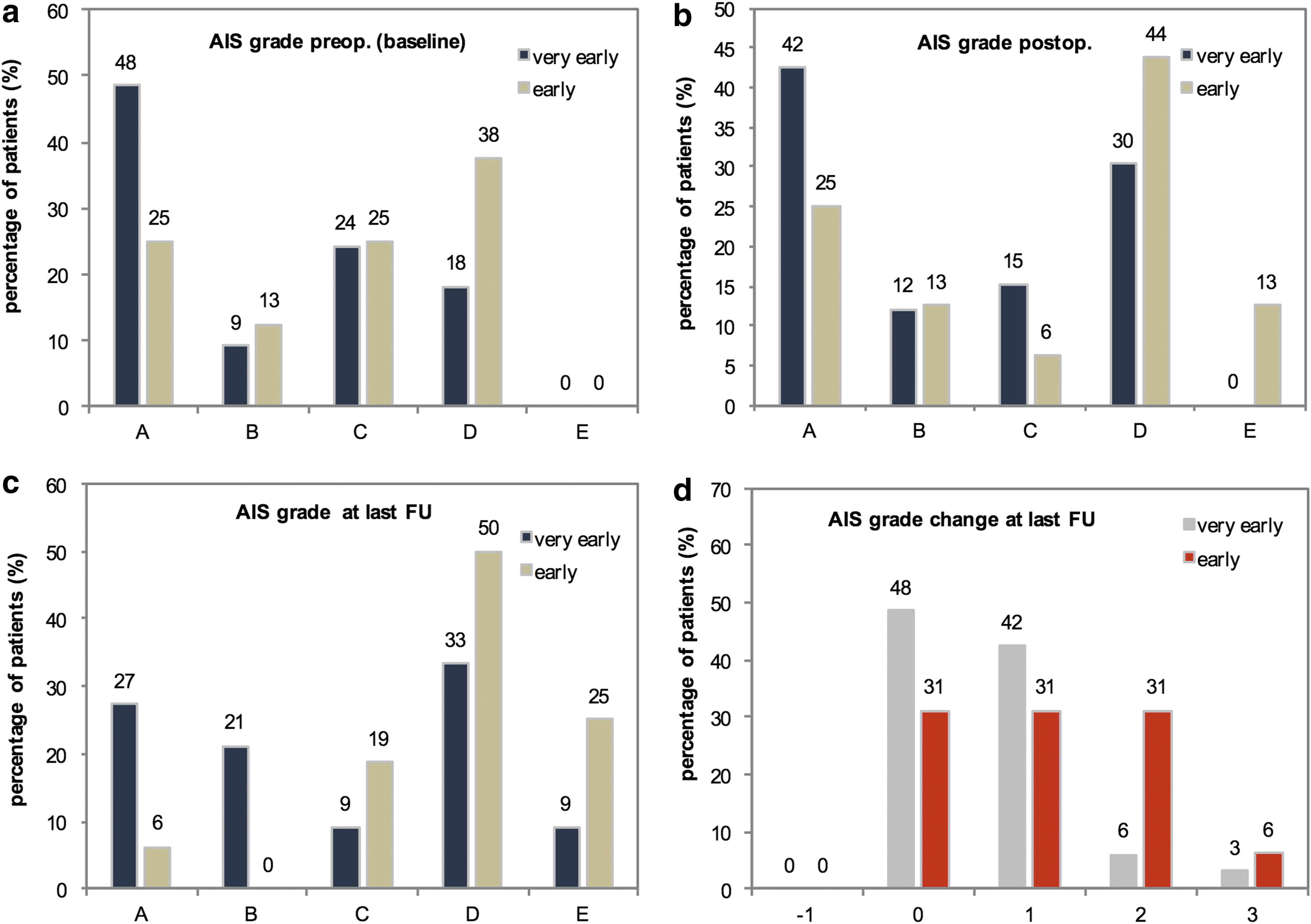
The distribution of AIS grades on admission was not significantly different between the very early (0–5 h) cohort and the early (5–24 h) cohort (Jonckheere–Terpstra test for doubly ordered crosstabs, p = 0.098). We identified a significant difference in AIS grade at the last FU between groups (Jonckheere–Terpstra test for doubly ordered crosstabs, p = 0.011) and a significantly higher AIS improvement rate in patients who were decompressed within 5–24 h (early group) (Poisson model, p = 0.018). Tables 3, 4, and 5 and Figure 2 a-d depict preoperative AIS scores and their changes during the observation period for both groups.
In the very early group, AIS grade improvements were as follows: 48% had no improvement, 42% improved by 1 AIS grade, 6% improved by 2 AIS grades, and 3% improved by 3 AIS grades (Fig. 2d). In the early group, 31% had no AIS improvement, 31% improved by one AIS grade, 31% improved by two AIS grades, 6% improved by three AIS grades, and no patients decreased in AIS grade (Fig. 2d). Based on this information, 69% of patients in the early group and 52% of those in the very early group experienced an improvement of at least one grade or more (Fisher's exact test, p = 0.36). Improvements by two AIS grades were observed in 6% of patients in the very early group and in 31% of patients in the early group (Fisher's exact test, p = 0.03; RR very early vs. early: 5.2 [95% CI: 1.1–35]). An improvement by three AIS grades was observed in 6% of patients in the early group and in 3% of patients in the very early group (p = 1.0) (Fig. 2d).
We further analyzed if one step and two or more steps of neurological improvement differed between the complete (AIS-A) group and the incomplete (AIS non-A) group.
Performing the same analysis for patients in the complete group with an improvement of one or more AIS grade revealed no significant difference between the very early and early groups (p = 0.58).
Three patients in the very early group (9%, 95% CI 2–24%) exhibited neurological improvement by two or more steps, among which two patients were initially AIS-A patients, versus six patients (25%, 95% CI 7–52%) in the early group who exhibited neurological improvement by two or more steps. Among the six patients in the early group, three were initially AIS-A patients (38%, 95% CI 15–65%, Fisher's exact test, p = 0.04, RR [4.1, 95% CI: 1.2–30, p = 0.01 for RR]). Among the incomplete (AIS non-A) group of patients, we also observed no significant difference between the very early and early groups (for one or more steps, Fisher's exact test: p = 0.46 steps; for two or more steps, Fisher's exact test: p = 0.28).
We investigated whether the patients' age (which did not differ between the two decompression groups at baseline) was also a predictor of AIS improvement. Our analysis indicated that age was an independent predictor for neurological improvement, as no significant differences were observed between the groups.
Discussion
Our study showed a significant improvement in neurological outcomes of patients with isolated CSCI after early decompression within 24 h of injury. Although complete remission of neurological impairment after traumatic CSCI in all patients remains elusive, even minor progress in healing can have a dramatic impact on quality of life in these patients.
Immediately after CSCI, small intraparenchymal hemorrhages develop in the gray matter, and edema in the white matter expands during the following hour with bleeding, reaching peak swelling 48–72 h after injury. 14 From a pathophysiological point of view, primary and secondary mechanisms after SCI lead to myelin damage. 3 According to Fehlings and colleagues in 2005, persistent compression of the cervical spinal cord is one of the potentially reversible mechanisms of secondary injury. 13
In all patients studied, decompression and stabilization were performed within 24 h. Our decision to employ the 24 h definition was in accordance with many publications, which observed a significant AIS improvement in those who underwent decompression within 24 h of injury. 4,19,20
The decision for the very early time point of 5 h was based on data suggesting that clinical outcomes could be potentially optimized if surgery was performed within 8 h after injury. 10 A potential limitation in conducting a surgical-based randomized controlled trial on the acute management of tSCI was the difficulty of recruiting eligible subjects in the early hours after sustaining a severe injury, which favors the decision for choosing a later decompression time point for evaluation. However, the Austrian healthcare system, its pre-hospital transportation system, and the availability of trauma units experienced in operatively treating spinal trauma allow the operative treatment to be administered within a short period of time for most patients. Therefore, it was possible to address an earlier decompression time point at 5 h, and we hypothesized that this shortened window would result in improved neurological outcomes. Therefore, in the second step, we questioned whether an earlier time point of surgery confers a beneficial effect on neurological outcome, focusing on patients treated within 5 h. Therefore, we split the study population into two cohorts: “very early” (< 5 h) and “early”: (≥ 5–24 h) groups.
Surprisingly, in contrast to our assumption that an earlier surgical decompression would be beneficial, we found a significantly higher AIS difference after the last FU in patients who underwent surgical decompression >5 h after the trauma (p = 0.011). We were unable to demonstrate any additional improvement in patients who were decompressed within 5 h.
Nevertheless, many treating physicians have the perception that decompression and internal stabilization as fast as possible provide better outcomes, which has been proven in various animal models. 21 –25
We analyzed the proportion of patients who improved two or more AIS grades between the early and very early groups and found better neurological outcomes in patients who had undergone surgery between 5 and 24 h.
CSCI in particular is much more serious and life threatening than thoracic and lumbar SCI, as it leads to potential damage to the phrenic nerve or even disturbance of the respiratory center. In addition to hypoxia and paresis of the upper and lower extremities, secondary mechanisms can also cause systemic shock, spinal shock, and hyperthermia, rendering operative procedures during the acute phase after injury impossible. 26
We also analyzed patients in the complete group who experienced an improvement of two or more steps in the early versus the very early group, which revealed a significant improvement in patients in the complete group who were operated after 5 h. This effect was not found in patients in the incomplete group, and the effect was also not observed for mild improvement (i.e., improvement by one AIS grade). These data suggest that AIS-A patients more likely exhibit improvements if operated after 5 h, which may be the time required for stabilization of the patient's vital parameters. Previously, published studies suggested that stable hemodynamic conditions are required to safely perform decompression and stabilization. 27 Intervention in patients with multiple injuries did not lead to a higher complication rate in a study by Randle and colleagues. 28 Croce and colleagues 29 noted a significantly higher incidence of mortality in patients with an ISS >25 who were operated within the first 72 h after injury compared with those who received late surgery.
Proponents of late surgery argue that later surgery corresponds to reduced mortality and decreased neurological deterioration compared with early surgery. 14 Further, cord swelling may subside and theoretically reduce the risk of iatrogenic cord injury. 30 Therefore, operative procedures should be performed after the patient has not only been medically stabilized but also neurologically stabilized. Some studies support this method of treatment especially in CSCI patients with high tetraplegia or severe systemic injuries, as these patients are critically unstable because of cardiorespiratory compromise. 31 Our data cannot support this argument, although the patients included in this study by definition had an ISS of <25.
Arguments against immediate decompressive surgeries are that the patient might be in a vulnerable phase after the accident and that therefore the complication rate could be higher. The major arguments for delayed intervention are, on the one hand, the need to hemodynamically stabilize these patients after injury and, on the other hand, the assumption that complete deficits are irreversible irrespective of the surgical intervention. Although the relatively high number of complete deficits in our patients may be possibly attributed to an overestimation in the initial phase, studies have demonstrated that potential neurological improvement can be achieved in these patients. Even if not proven, many treating physicians argue that stabilization of the fractured vertebral bone protects adjacent neurological segments, which is of great importance, especially in the cervical spine. Conservative management via non-operative therapy has a risk of up to 10% neurological deterioration. 32
Defining “early,” and determining the best time point for surgical intervention following tSCI, particularly in general and CSCI patients, have not yet been elucidated. In a systematic review by Furlan and colleagues reported in 2009, assessment of 19 decompression studies in several different animal SCI models concluded that 11 favored a time-dependent effect after early surgery according to FU functional status and myelin destruction. The majority of these animal studies regarded the optimal operative timing as being between 8 and 24 h. 33 In 1999, Dimar and colleagues 24 reported an inverse relationship between neurological recovery and the duration of spinal cord compression using an experimental rat model. In that study, the effect of spinal cord decompression was evaluated at 0, 2, 6, 24, and 72 h after injury.
La Rosa and colleagues in 2000 and Fehlings and colleagues in 2005 concluded in their publications that early decompression within 24 h after CSCI does lead to better neurological outcome. 13,19 A positive effect of early decompression as measured by motor score recovery was published in a meta-analysis by van Middendorp and colleagues. 34 Overall, clinical literature tends to support surgery performed within the first 24 h after trauma, showing an association with improved neurological recovery. Early surgery has been described as surgery between 8 h after injury and up to 4 days after SCI. However, most studies have defined 24 h as the cutoff for early surgery. 8 In clinical studies that failed to demonstrate neurological improvement following surgery within 72 h, a wide range of time points (0–72 h) were analysed, resulting a heterogeneous group of patients and potentially causing a bias.
Performing surgery within 72 h after vertebral trauma decreased the occurrence of pneumonia, pressure ulcers, and further complications. A major goal of early surgery is to allow early mobilization in an attempt to reduce the occurrence of complications caused by prolonged recumbency. 27 Even if early surgery may be initially costlier, the decrease in the length of hospitalization potentially reduces overall costs. 35
Performing surgical decompression as fast as possible is an accepted therapeutic approach in Austrian trauma units. We believed that early decompression within 5 h after traumatic CSCI could be advantageous for improving neurological outcome, although we did not find an advantage compared with surgery performed between 5 h and 24 h after injury. Other circumstances such as pre-hospital transport, local logistical factors of the hospital, patient condition, and preferences of the treating surgeon also influence the time until surgery. However, the Austrian healthcare system, pre-hospital transportation system, and availability of trauma units that are experienced in operatively treating spinal trauma allow operative treatment to be administered within a short period of time for the majority of patients.
Study initiatives aimed at proving the efficacy of acute surgical decompression after tSCI in a prospective, observational European multi-center study (Spinal Cord Injury: a Prospective, Observational European Multicenter study [SCI-POEM]) are currently underway. The aim of that study is to evaluate whether decompressive spinal surgery within 12 h post-injury leads to improved neurological motor outcomes compared with the outcomes of late decompressive surgery occurring >12 h but within 14 days after tSCI. 36
Several factors are considered to influence neurological recovery. Based on the literature, confounding factors include age, sex, the ISS, the initial AIS, and the neurological level of injury of the patient. In addition, postoperative rehabilitation and the time from injury to FU may influence the outcome. Methylprednisolone has been investigated by the National Acute Spinal Cord Injury Studies (NASCIS). The studies showed a mild benefit when methylprednisolone was administered within 8 h of injury. 17 We encountered no significant differences between the two groups regarding these factors.
Although better therapeutic options for regenerating the myelin remain unavailable, the primary aim is to prevent negative effects of secondary mechanisms. Fast surgical decompression and pharmacological agents such as riluzole, ibuprofen, minocycline, and other drugs for neuroprotection can facilitate achieving better outcomes. 3
Limitations and strengths of the study
This study is limited by its retrospective nature and small sample size across multiple institutions. Our study may be criticized because of the disparity between the “very early” and “early” groups for surgical decompression and the disparity between AIS A and AIS non-A patients. Data for this study were retrospectively gathered from patient records and prospectively gathered from the ASCIS registry. Retrospectively acquired data may be less precise and comprehensive than prospectively designed studies. However, it is important that all variables included in the study were collected consistently for all patients at the participating centers. Therefore, we only included patients with complete FU documentation and neurological reports assessing all relevant data, to classify the patients according to the ISNCSCI protocol.
In terms of the FU examination, we included all patients with FU examinations of at least 6 months. However, disparities in the postoperative rehabilitation process and varying intervals to final examination remain limitations.
This study does not draw conclusions regarding the full rate of complications depending on the time of operation and additional injury, which must be managed accordingly. We believe that operative interventions were only performed in hemodynamically stable patients. This study does not address the types of procedures for decompression and stabilization. Surgeons in different centers may perform their operations very differently because of their level of experience. Different pre- and postoperative management techniques may also be criticized. The reasons for surgical delay were also not determined in this study, and reasons for delay may be manifold. We also did not radiologically classify the fracture or the amount of spinal stenosis caused by the dislocation. In all patients, a CT scan or MRI was performed preoperatively, and, therefore, a spinal compression was verified in all cases to different extents.
Because several raters may assess one patient over time, inter-rater reliability may remain an issue, even if regular assessment trainings are performed.
Conclusion
Surgical decompression and stabilization of patients with traumatic CSCI increase the degree of recovery in some way. Data from ASCIS suggest that the management of CSCI in Austria is rapid, and that transfer to spinal injury centers for surgical stabilization is effective.
Data from our study suggest that patients benefit from surgical intervention performed within 24 h of the time of injury. A definitive statement regarding the results of surgery being performed as soon as possible cannot be made. Although surgical stabilization between 5 and 24 h seems to improve the neurological outcomes more than very early decompression, we encountered a relatively high number of complete deficits in the very early group. Therefore, it may be possible that healing potential was lower, affecting the improvement in AIS grade. In this study, decompressive surgery prior to 24 h after SCI was performed safely and was associated with improved neurological outcome.
In summary, we suggest that patients with traumatic SCI should promptly undergo surgery earlier than 24 h under the premise that they are hemodynamically stable and that the operation is performed under the best possible circumstances. A planned randomized trial with a prospective sample size should determine whether very early surgery is truly associated with reduced levels of improvement as suggested by these results.
Footnotes
Acknowledgments
This project was funded by a research grant from the Austrian Social Insurance for Occupational risks (AUVA), Paracelsus Medical University (PMU), and the Austrian Society of Traumatology (OeGU) as supporters of the ASCIS. We are grateful to Heinz Redl for the editorial support and for constructive comments on the article. We also express our thanks to the patients and SCI centers that are participating in the ASCIS project, as well as to Manuela Aigner and Katharina Bogner for their assistance with data collection and data processing.
Author Disclosure Statement
No competing financial interests exist.