
Abstract
Persons with incomplete spinal cord injury (iSCI) face ongoing struggles with walking, including reduced speed and increased reliance on assistive devices (ADs). The forces underlying body weight support and gait, as measured by ground reaction forces (GRFs), are likely altered after iSCI because of weakness and AD dependence but have not been studied. The purpose of this study was to examine GRF production during overground walking after iSCI, because greater insight into GRF constraints is important for refining therapeutic interventions. Because of reduced and discoordinated motor output after iSCI, we hypothesized that persons with iSCI would exert smaller GRFs and altered GRF modifications to increased cadence compared with able-bodied (AB) persons, especially when using an AD. Fifteen persons with chronic iSCI, stratified into no AD (n = 7) and AD (n = 8) groups, walked across an instrumented walkway at self-selected and fast (115% self-selected) cadences. Fifteen age-matched AB controls walked at their own cadences and iSCI-matched conditions (cadence and AD). Results showed fore-aft GRFs are reduced in persons with iSCI compared with AB controls, with reductions greatest in persons dependent on an AD. When controlling for cadence and AD, propulsive forces were still lower in persons with iSCI. Compared with AB controls, persons with iSCI demonstrated altered GRF modifications to increased cadence. Persons with iSCI exhibit different stance-phase forces compared with AB controls, which are impacted further by AD use and slower walking speed. Minimizing AD use and/or providing propulsive biofeedback during walking could enhance GRF production after iSCI.
Introduction
S
Numerous studies show reduced lower extremity force production compromises walking ability in older adults 4,5 and individuals with stroke, 6,7 but it remains unclear whether similar alterations in force production may contribute to compromised walking in persons with iSCI. Spinally injured cats have shown altered limb loading that contributes to a 55% reduction in vertical ground reaction forces (GRFs) compared with intact felines. 8 Similar reductions are also evident in hindlimb propulsive and braking forces in rats after spinal injury, 9 resulting in limited locomotion. 10 A paucity of studies, however, has explored the impact of iSCI on force production during overground walking in humans. Desrosiers and associates 11 showed that persons with iSCI present with weaker force generation at push-off during inclined walking compared with healthy subjects. Other studies have found muscle coordination deficits including altered knee extensor and ankle plantar flexor activity, 12,13 as well as abnormal hip-knee coupling, 14 which may limit weight acceptance and propulsion during the stance-phase of walking. Although insightful, these previous human studies did not assess whether limited force production after iSCI may impair level overground walking performance, as quantified by clinically relevant metrics such as gait speed and AD use.
Reduced walking speed and increased reliance on ADs are major factors that contribute to limited community walking after iSCI. 2,15,16 Therapeutic strategies often target general lower extremity muscle weakness and altered muscle coordination to increase walking speed and reduce AD dependence. Unfortunately, beneficial outcomes from these therapies are typically modest Because of, in part, a limited understanding of how best to target mechanisms that may contribute to walking deficits and dyscoordination. Imbalance in preserved pathways distal to the injury may contribute to a limited repertoire of motor function (i.e., recruitment, number, and coordination) after iSCI. 13
Although Hayes and colleagues 13 provided important evidence that constraints on muscle activity can affect overground walking speed, this study did not address the impact of these constraints on gait mechanics (i.e., stance-phase force production) during overground walking. This is an important gap, because the human neuromotor system permits a broad range of compensatory strategies to achieve locomotion. For example, ADs counter functional limitations and ensure safe overground walking; however, they generally require use of the less impaired upper extremities to compensate for limited control and weakness of the lower extremities and may actually constrain lower extremity force production. Some studies argue that despite providing safety, ADs promote greater reliance on the intact upper extremities during walking, which may limit recovery. 15,17,18
Quantifying the effects of ADs on GRF production is important for characterizing adaptive and maladaptive compensatory strategies used by persons with iSCI to overcome their walking deficits. While inherent flexibility of the intact neuromotor system provides numerous strategies to produce GRFs necessary for overground walking, disruption of these pathways after iSCI likely limits this flexibility, resulting in altered GRFs. The resulting spatiotemporal constraints on GRFs are thought to compromise recovery of walking speed and contribute to greater reliance on ADs, but remain poorly understood. Thus, quantifying GRF production and the relation GRF production has on overground walking ability is vital to defining the functional consequences of altered lower extremity force production during walking. 19
The purpose of this study was to examine GRF production during overground walking at different cadence conditions in two cohorts of persons with iSCI: those who use an AD to walk and those who do not. Based on previous demonstrations of altered motor output after iSCI, 12,20 we hypothesized that, regardless of AD use, persons with iSCI would exert smaller stance-phase GRFs compared with able-bodied persons. In addition, we explored the extent to which persons with iSCI modify GRFs with increased cadence as observed in able-bodied persons. 21 –23 We hypothesized that persons with iSCI would exhibit attenuated GRFs that do not increase with increased cadence because of limited flexibility of the impaired neuromotor system. Because ADs provide a source for distributing force production via effort from upper extremities, we also predicted that healthy adults trained using the same ADs of persons with iSCI would exert smaller GRFs but preserve task-appropriate modification with cadence. The results of this study have implications for understanding how generation of GRFs is altered because of iSCI and the extent to which dependence on ADs may further constrain lower extremity generation of GRFs necessary for restoring walking ability.
Methods
Subjects
Fifteen adults with American Spinal Injury Association Impairment Scale (AIS) D iSCI (47.6 ± 15.5 years old; mean ± standard deviation) and 15 able-bodied (AB) controls (44.0 ± 15.9 years old) participated in this study (Table 1). The AB persons were selected to match sex as well as approximate age and body type. All subjects provided written informed consent approved by the Emory University Institutional Review Board (IRB protocol IRB00044670) before study participation. We included persons who sustained an iSCI between levels C2 and T12 who were at least one year post-injury (i.e., chronic), who could walk over ground at least 10 m without human assistance, and who could follow simple verbal, visual, and auditory commands. We excluded persons with brain injury or cognitive impairment impacting the ability to follow simple commands, progressive SCI, other concurrent severe medical conditions, or severe weight-bearing pain that limited walking ability.
LEMS, lower extremity motor score; SS, self-selected; iSCI, incomplète spinal cord injury; AD, assistive device; C, cervical; T, thoracic.
More impaired leg.
Clinical assessments
Injury severity, lower extremity strength and spasticity, and walking speed were assessed using standardized clinical measures. The AIS was used to categorize neurological injury level and completeness. 24 Lower extremity strength was assessed using the Lower Extremity Motor Score (LEMS) from the AIS, and spasticity was measured using the Spinal Cord Assessment Tool for Spastic Reflexes (SCATS). 25 The 10-Meter Walk Test (10MWT) was used to assess fast walking speed, 26 with the average of three trials used for analyses. The SCI Functional Ambulation Inventory (SCI-FAI) was used to identify clinically observable gait deficits. 27 Participants performed walking tests with the AD they typically used for community walking.
Equipment
Subjects walked over a 0.1 m raised, level floor that included two embedded six-degrees-of-freedom force plates (AMTI OR6-7-2000; Advanced Mechanical Technology Inc., Watertown, MA) located equidistant from markers at either end of an 8 m walkway. 28 A metronome placed approximately 2 m from the walkway provided auditory cues for cadence matching. The GRFs were amplified using two AMTI signal conditioners (MSA-6, Gen-5). The AMTI MSA-6 used a two-pole, low-pass 1 kHz filter, and the AMTI Gen-5 used a 1 kHz anti-aliasing filter. The output of the amplifiers was then sampled at 2.5 kHz by a 16 channel, 16 bit analog-to-digital data converter (NI PCI-6289; National Instruments, Austin, TX) and collected using custom software in Matlab (Mathworks, Inc, Natick, MA).
Experimental protocol
To examine the effects of iSCI on stance-phase force production during walking, we compared vertical and fore-aft GRFs and GRF modifications because of increased cadence between persons with iSCI and AB controls. Forces exerted by the more impaired limb (defined by LEMS) were recorded for persons with iSCI, and the same limb was recorded for their AB match. Subjects walked across the level walkway at self-selected (SSmet) and fast (Fmet = 115% of SSmet) cadences while listening to a metronome. Cadences matched the metronome within 7% (SS) and 8% (F) error for all subjects. In general, persons with iSCI (n = 13) showed significantly lower SS cadences (71.0 ± 22.2 steps/min) compared with AB controls (108.4 ± 10.4 steps/min) (p < 0.001), especially when ambulating with an AD. The SS (n = 11, r = 0.79, p = 0.004) and F (n = 11, r = 0.77, p = 0.006) cadences were also highly correlated with walking speed (10MWT) in persons with iSCI. Details of the experimental setup for cadence-matching conditions have been published previously. 13
To control for cadence and AD on GRF production, AB participants also performed additional trials at the SS cadence of their iSCI match (SScadence), as well as the SS/F cadences of their iSCI match using the matching AD (SSmatch/Fmatch) when applicable. A licensed physical therapist instructed AB controls on appropriate use of the AD to preserve the SCI-match gait pattern. 13 AB controls were provided up to 10 minutes of practice with the AD. The cadences performed by AB controls were comparable to their iSCI match during SSmatch (paired t test of actual cadences walked, n = 13, p = 0.49) and Fmatch (p = 0.63) conditions. The GRFs were collected across a minimum of three gait trials per cadence and AD condition. The order of prescribed cadence conditions (SS, F) was randomized between subjects to minimize order effects. There were significant differences between SS and F cadence conditions for persons with iSCI (SSmet = 71.0 ± 22.2 steps/min, Fmet = 79.1 ± 25.2 steps/min, p < 0.001), between SS and F cadences for AB controls (SSmet = 107.8 ± 9.8 steps/min, Fmet = 119.6 ± 12.0 steps/min, p < 0.001), and between SS and F iSCI-matched cadences for AB controls (SSmet = 74.1 ± 26.2 steps/min, Fmet = 82.6 ± 27.9 step/min, p < 0.001).
GRF data analyses
Raw GRF data were processed using custom code written in Matlab (Mathworks Inc., Natick, MA). Stance phase was defined using vertical GRF data. Persons with iSCI, however, often walk with limited control of foot placement and exhibit shuffle gait or toe drag, resulting in GRF data features during swing phase in addition to stance phase. Thus, standard methods of determining stance phase from vertical GRF data do not work well on data with these swing-phase features. To characterize stance-phase GRFs in persons with iSCI, we developed a two-step stance phase cropping method (Supplementary Fig. 1; see online supplementary material at
In the first step, we used a preliminary cropping window at 20% of maximum vertical GRF. This preliminary cropping avoids toe drag or other low force events that occur during swing phase. It also removes the heel strike and toe off events of normal gait, however. Thus, in a second step, we extended the first cropping window to include heel strike and toe off events in typical gait. To determine the expansion of the cropping window for step two, we used normative GRF data from our AB controls (SSmet condition) and cropped the normative data using two methods: at 20% of maximum, and using a standard method at 5N. 29 In comparing the two methods of cropping on the normative data, we found that, on average, heel strike defined by cropping using the 5N vertical GRF method occurred earlier by 4.25% of preliminary stance phase, and that toe off occurred later by 7.97% of preliminary stance phase.
Thus, in step two for all data (AB and iSCI), we expanded the preliminary cropping window by 4.25% of stance phase before 20% body weight during loading, and by 7.97% of stance phase after 20% body weight during unloading. Visual inspection of all cropped data confirmed that this algorithm defined stance phase appropriately, both for AB and iSCI subjects. Cropped stance-phase GRF data were digitally filtered with an eighth order, zero-lag, 100 Hz low-pass Butterworth filter to remove high frequency noise before analysis and then normalized to the subject's body weight and stance phase duration.
We quantified fore-aft and vertical GRF profiles to compare stance-phase force production between groups and across cadence and AD conditions. Three variables were derived from fore-aft GRFs: transition point, braking impulse, and propulsive impulse (Fig. 1A). The transition point was defined as the time point (% stance phase) that the force curve switches from negative (braking) to positive (propulsion), found by locating the most negative excursion of the fore-aft GRF, and stepping forward to the next zero crossing. Braking impulse was defined as the area under the negative force curve before the transition point. Propulsive impulse was defined as the area under the positive force curve after the transition point. 6

General methodology. (
Three variables were also derived from vertical GRFs: V1Max, V2Max, and vertical modulation (Fig. 1B). Maximum vertical loading during 0–39% stance phase (weight acceptance) defined V1Max. Maximum vertical loading during 61–100% stance phase (push-off) defined V2Max. 30 We quantified vertical GRF modulation as the difference between the average of V1Max and V2Max, and the minimal vertical loading between V1Max and V2Max. Vertical GRF modulation quantifies the range of vertical loading between weight acceptance and push-off, and represents the amount of vertical lift of a person's center of mass (COM) at midstance. 31
Based on visual inspection of the GRF profiles, fewer than 1% of gait trials (four of 401) were classified as outliers and removed from analyses. In one case, the data acquisition was not started in time, and the first half of the stance phase was not recorded. In three other cases, the contralateral foot or part of an AD likely may have touched the force plate during stance phase. One sample t tests confirmed that these three trials were outliers compared with other trials for that subject under the same walking condition (p < 0.05 for at least one GRF parameter).
Statistical analyses
Descriptive statistics (mean and standard deviation) were calculated for cadence and each GRF variable, and normality of the data was assessed using the Shapiro-Wilk test. Independent sample t tests or Mann-Whitney U tests were used to compare fore-aft and vertical GRF variables between persons with iSCI and AB controls (iSCI SSmet vs. AB SSmet, n = 15). Because use of an AD can change GRFs substantially, we also stratified iSCI participants into two groups: those who did use an AD to walk (n = 8) and those who did not (n = 7). While there were no differences in age and time post-SCI between groups (p > 0.05), there were differences in self-selected walking cadence (independent sample t test, p = 0.001) and lower extremity strength (LEMS total score, p = 0.02).
We used independent sample t tests or Mann-Whitney U tests for between-group comparisons (iSCI SSmet vs. AB SSmet, iSCI SSmet vs. AB SScadence, iSCI SSmet vs. AB SSmatch), and paired sample t tests or Wilcoxon Signed Rank tests to examine GRF modifications across cadences (iSCI SSmet vs. iSCI Fmet, AB SSmatch vs. AB Fmatch) in these stratified groups. Linear regression analyses were also performed to examine the relationship between GRFs and clinical measures of strength, spasticity, and walking ability. All statistical analyses were performed using SPSS 22 (IBM SPSS Inc., Chicago, IL) with a significance level of p < 0.05.
Results
Fore-aft GRFs are attenuated in persons with iSCI
Fore-aft GRFs were significantly reduced in persons with iSCI (n = 15). In particular, we found reduced braking (−219.5 ± 130.8%) and propulsive (214.1 ± 90.0%) impulses in persons with iSCI compared with AB controls (−515.9 ± 83.3% and 481.2 ± 98.1%, respectively) during walking at SS cadence (p < 0.001). The transition point between braking and propulsion impulses occurred earlier in persons with iSCI (42.5 ± 10.8%) compared with AB controls (55.9 ± 2.9%) at SS cadence (p < 0.001). When stratified by AD use, persons with iSCI who walked without an AD exhibited reduced braking (p = 0.006) and propulsive (p = 0.005) impulses and spent a smaller percent of the gait cycle in braking (earlier transition point; p = 0.04) compared with AB controls at matched cadences (Fig. 2, A1–A3).
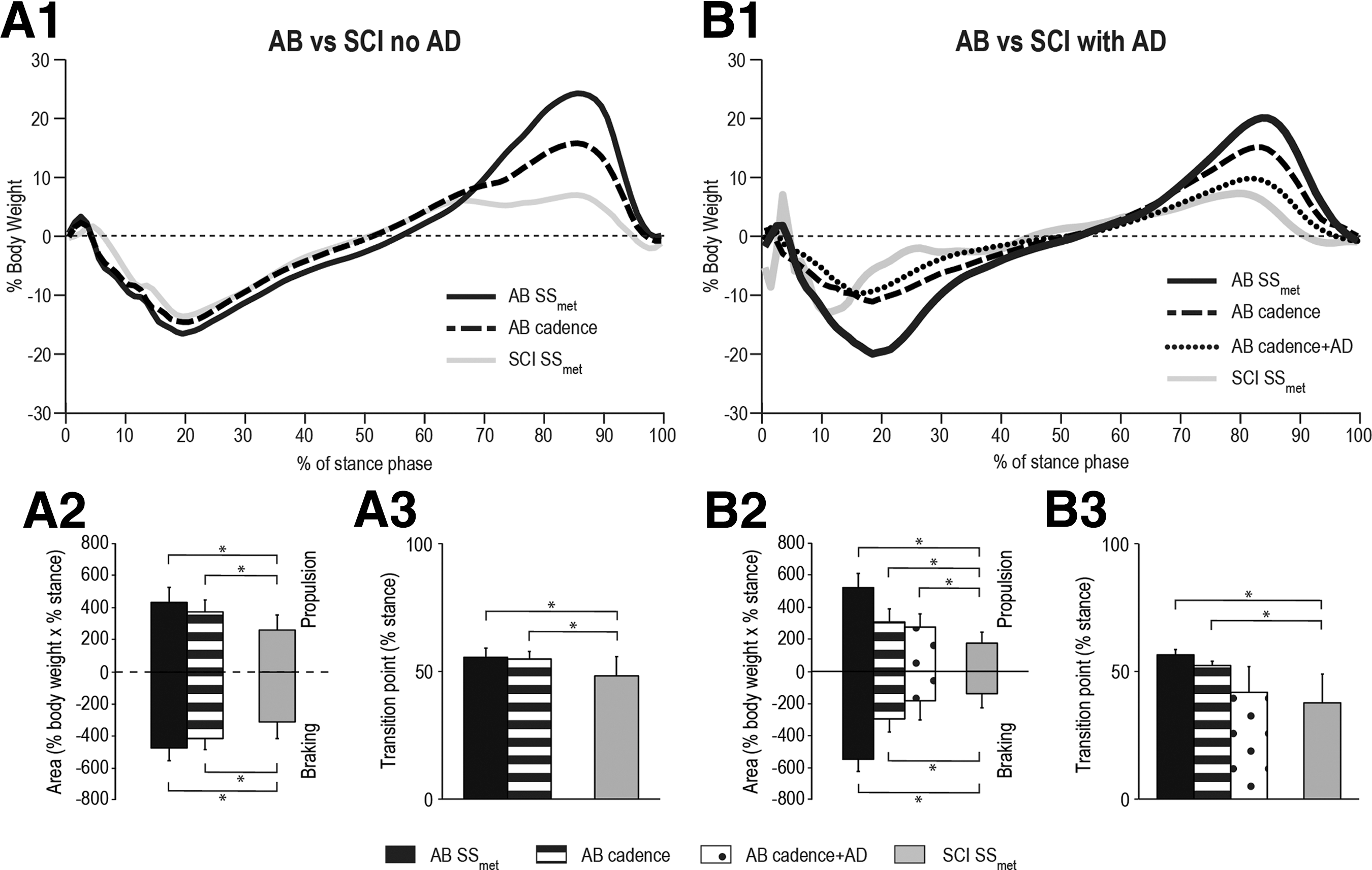
Fore-aft ground reaction forces comparison between persons with incomplete spinal cord injury (iSCI) and able-bodied (AB) controls. Fore-aft ground reaction force data are shown for (
Persons with iSCI who used an AD also exhibited decreased braking (p = 0.003) and propulsive (p = 0.003) impulses and an earlier transition point (p = 0.008) compared with AB controls at matched cadences (Fig. 2, B1–B3). When AB controls walked at matched cadences and AD, there was no difference in fore-aft braking impulse (p = 0.42) or transition point (p = 0.46) between persons with iSCI and AB controls, suggesting that ADs account for some of the observed reduction in fore-aft GRF production, particularly braking. Nevertheless, propulsion was still reduced in persons with iSCI even when controlling for cadence and AD (p = 0.014).
Persons with iSCI did not exhibit task-appropriate modification of fore-aft GRFs with increased cadence
Persons with iSCI exhibited no significant fore-aft GRF modifications with increased cadence in both the no AD and AD groups (p > 0.05) (Fig. 3, A1–A3 and B1–B3). The AB controls, however, exerted greater propulsive impulse when walking at their faster cadence compared with their self-selected cadence (no AD group p = 0.014; AD group p = 0.04). During matched conditions (iSCI cadence + AD), AB controls still exhibited larger propulsive impulse when increasing cadence (no AD group p = 0.03; AD group p = 0.04). In addition, AB controls in the no AD group exerted greater braking impulse when walking at the faster iSCI-matched cadence (p = 0.004).
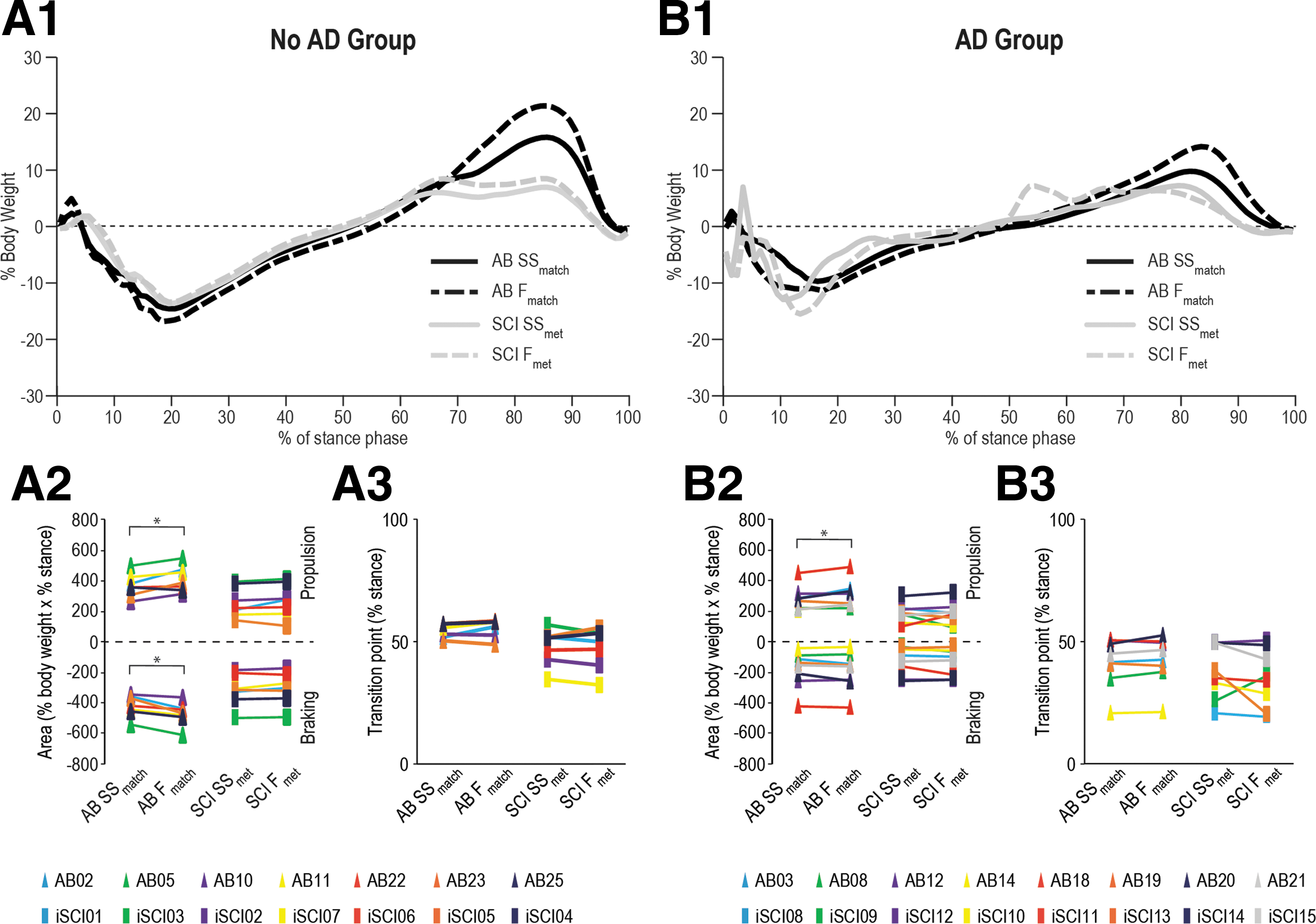
Fore-aft ground reaction force (GRF) modifications to increased cadence. Fore-aft GRF data are shown for persons with incomplete spinal cord injury (iSCI) (and their able-bodied [AB] controls) who ambulate without an assistive device (AD) (
Vertical GRFs are comparable between persons with iSCI and AB controls after controlling for cadence and AD use
Persons walking at slower speeds often produce smaller GRFs. 32,33 In this study, we found that persons with iSCI (n = 15) walked at slower SS (108.4 ± 10.4) and generated smaller vertical GRFs in the more impaired limb (V1Max 100.1 ± 14.5%, V2Max 91.0 ± 9.7%, vertical modulation 21.8 ± 16.3%) compared with AB controls (cadence: 71.0 ± 22.2, p < 0.001; vertical GRFs: V1Max 117.7 ± 7.9%, V2Max 109.5 ± 6.3%, vertical modulation 42.3 ± 14.3, p ≤ 0.001). When stratified by AD use and controlling for cadence, however, there were no differences in vertical GRFs between persons with iSCI, who walked without an AD and AB controls (all p > 0.05, Fig. 4, A1–A4). For persons with iSCI who walked with an AD, smaller V1Max (p = 0.012) and V2Max (p < 0.001) were demonstrated at matched cadences (Fig. 4, B1–B4). We also found that AD use reduced GRF generation, which compliments previous evidence that ADs support partial body weight. 34 When controlling for both cadence and AD use, there was no difference in vertical GRF variables between persons with iSCI and AB controls (all p > 0.05). These results show that slower walking and use of an AD in those with iSCI results in smaller vertical GRFs.
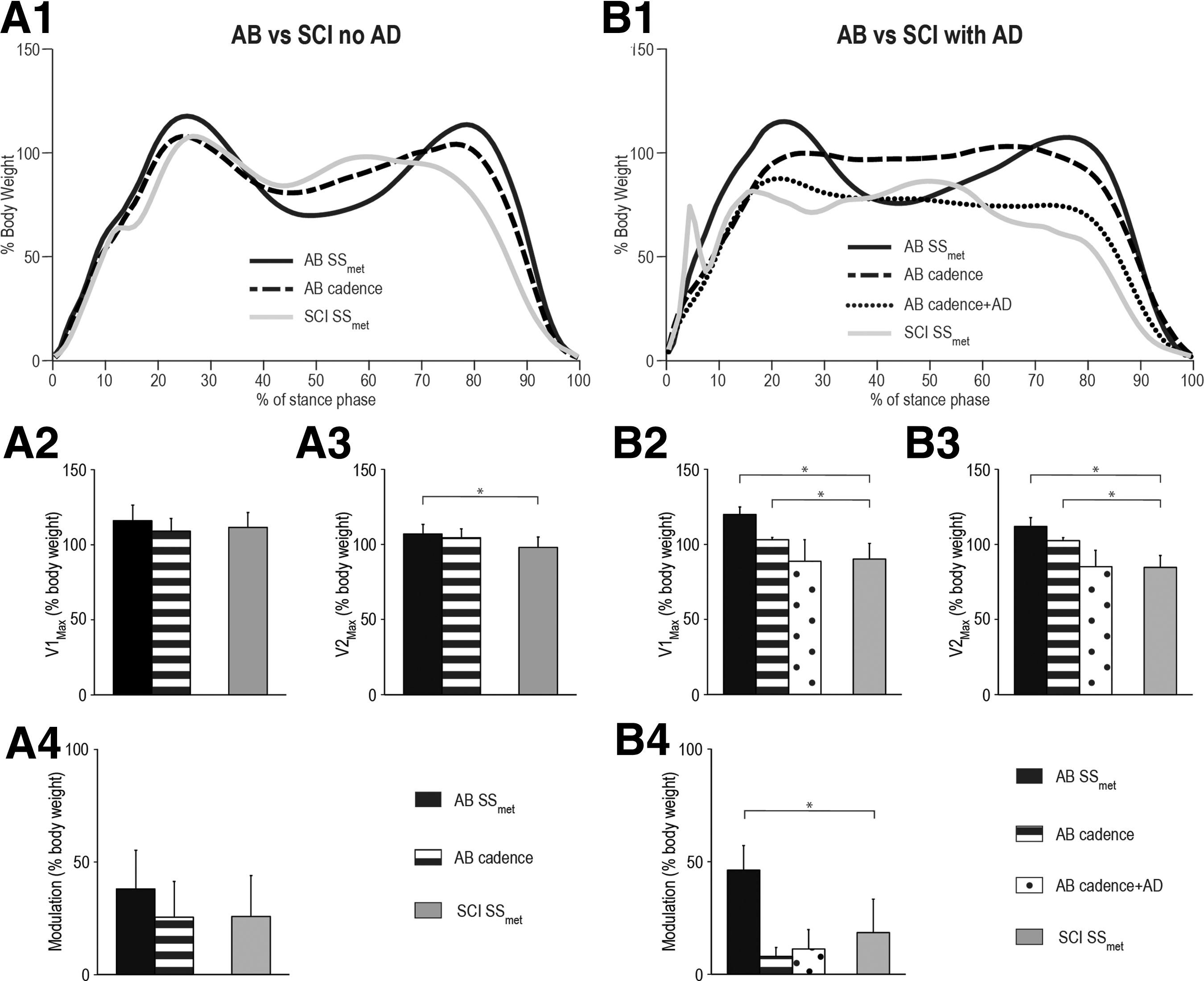
Vertical ground reaction force (GRF) comparison between persons with incomplete spinal cord injury (iSCI) and able-bodied (AB) controls. Vertical GRF data are shown for (
Modification of vertical GRFs for increased cadence was inconsistent across persons with iSCI
Persons with iSCI showed limited or variable modification of vertical GRFs with increased cadence. Similar to AB controls, persons with iSCI who walked without an AD showed greater vertical GRF modulation at F cadence compared with SS cadence (p = 0.005), suggesting task-appropriate modification. In the iSCI AD group, however, no modification of vertical GRFs with increased cadence was observed (Fig. 5, B1–B4), suggesting that use of an AD may compensate for altered lower extremity force production in persons with iSCI. Moreover, AB controls who walked with an AD under iSCI-matched conditions also exhibited reduced vertical GRF modifications with increased cadence.

Vertical ground reaction force (GRF) modifications to increased cadence. Vertical GRF data are shown for persons with incomplete spinal cord injury (iSCI) (and their able-bodied [AB] controls) who ambulate without an assistive device (AD) (
In contrast, AB controls exhibited vertical GRF modifications when walking at a faster cadence. Increases in V1Max (no AD group p = 0.003; AD group p = 0.001), V2Max (no AD group p = 0.014; AD group p = 0.03), and vertical GRF modulation (no AD group p < 0.001; AD group p = 0.001) were observed when AB controls walked at 115% of their SS cadence compared with their SS cadence. Similarly, under iSCI-matched conditions, AB controls in the no AD group increased V1Max when increasing cadence from iSCI-matched SS to iSCI-matched F cadence (p = 0.046; Fig. 5, A2). Further, AB controls walking at iSCI-matched cadences with or without an AD showed greater vertical GRF modulation at the faster cadence (p = 0.013 with AD and p = 0.007 without AD). However, The V2Max did not change with cadence (p > 0.05; Fig. 5, A3-A4), however.
Fore-aft braking, but not propulsion, was correlated with clinical measures of walking impairment and leg strength in persons with iSCI
Braking impulse, V1Max, and V2Max were most reduced for persons with iSCI with the greatest walking impairment (Fig. 6). There was a linear relation between walking speed (10MWT) and braking impulse (R 2 = 0.54, p = 0.004), V1Max (R 2 = 0.35, p = 0.03) and V2Max (R 2 = 0.41, p = 0.02); subjects with slower 10MWT times had smaller fore-aft braking as well as smaller V1Max and V2Max GRFs, suggesting that inability to generate these GRFs impairs walking ability. Similarly, there was also a linear relation between clinically observable gait impairments, (as measured by the SCI-FAI) and braking impulse (R 2 = 0.41, p = 0.03) and V2Max (R 2 = 0.70, p = 0.001). A similar, but smaller relationship was observed between strength of the more impaired limb (as quantified by LEMS) and braking (R 2 = 0.31, p = 0.03); subjects with lower LEMS scores had smaller fore-aft braking GRFs. Last, a linear relation was found between spasticity of the more impaired limb (as quantified by SCATS) and fore-aft transition point (R 2 = 0.61, p = 0.003); subjects with greater spasticity had an earlier transition point. No other significant relationships (p > 0.05) were found between clinical measures (10MWT, LEMS, SCATS, SCI-FAI) and fore-aft/vertical GRFs.
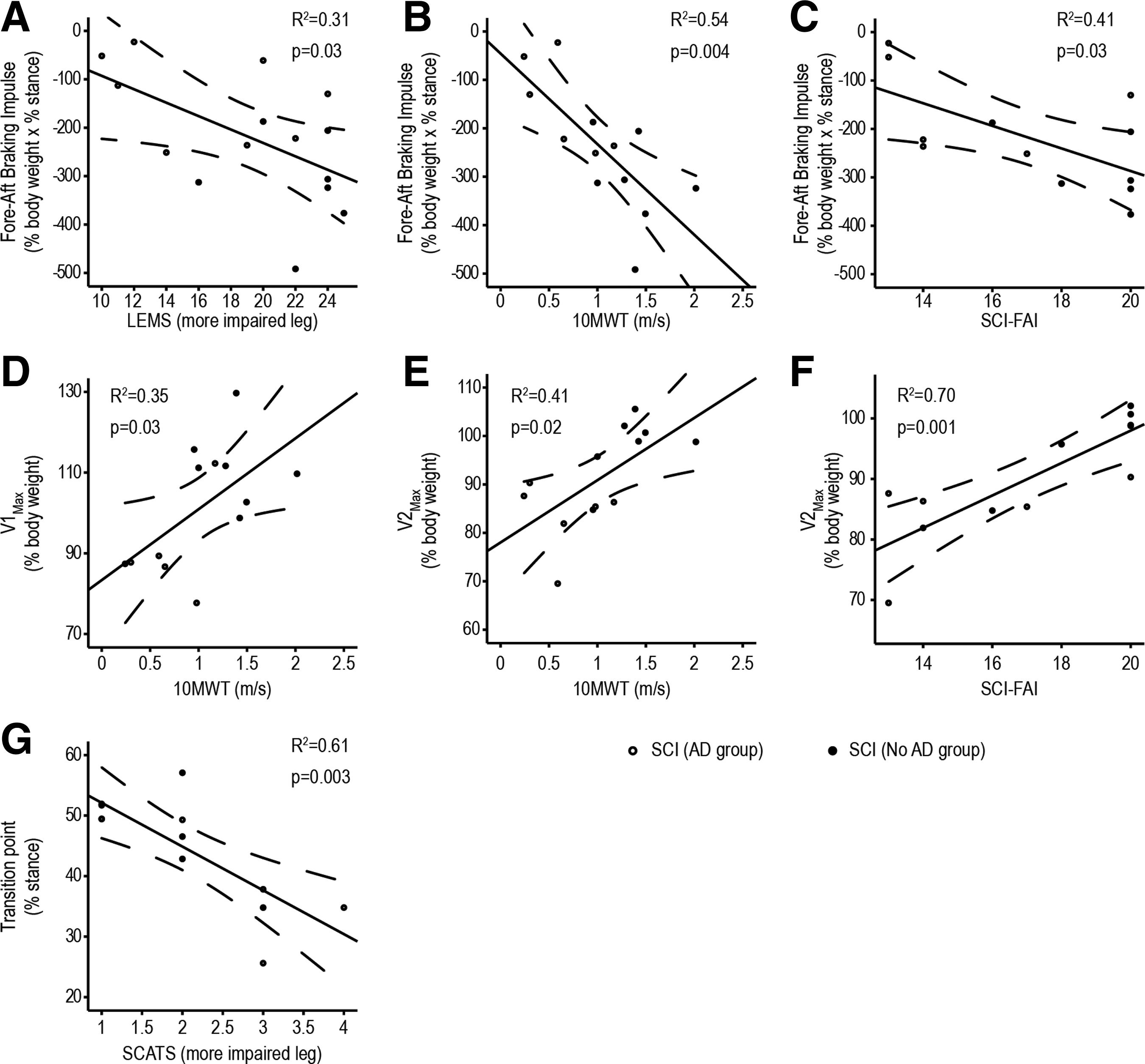
Relationship between fore-aft and vertical ground reaction forces and clinical measures of walking ability, leg strength, and spasticity in persons with incomplete spinal cord injury (iSCI). Only statistically significant (p < 0.05) relationships are shown. Regression line and 95% confidence interval for the group are depicted; open circles represent the assistive device (AD) group, solid circles represent the no AD group. LEMS, Lower Extremity Motor Score; 10MWT, 10 Meter Walk Test; SCI-FAI, Spinal Cord Injury Functional Ambulation Inventory; SCATS, Spinal Cord Assessment Tool for Spastic Reflexes.
Discussion
The purpose of this study was to examine the impact of iSCI on task-based production and modification of GRFs and how altered GRFs may constrain overground walking ability after injury. Further, we examined how reduced walking cadence and reliance on ADs may contribute to altered lower extremity GRF production. Our results demonstrate that despite the heterogeneity of our subject cohort, persons with chronic iSCI exhibit reduced GRFs during overground walking compared with AB controls. Slower walking is associated with lower force production, 32,33 and use of an AD also reduces GRFs. 34 Thus, the lower GRFs seen in persons with iSCI may be, in part, because they walk more slowly and use an AD. The AB controls walking at the same cadence and using the same AD as those with iSCI have similarly reduced vertical GRFs. Even with matched cadence and AD use, however, AB controls generate more forward propulsion than those with chronic iSCI.
The reduced propulsive impulse in persons with iSCI may be because of neuromuscular deficits from the SCI, subsequent scarring and neuroplastic changes that have occurred after the injury, muscle atrophy, and/or compensatory strategies that have been learned over time. In those with chronic iSCI, we found that altered GRFs were tightly coupled not only with walking speed, but also with strength and clinically observable gait deficits. Thus, lower extremity force production may be an important target for therapies aimed at improving walking ability after iSCI. Collectively, these findings suggest that links between GRF production, speed, strength, and AD use may contribute to compensatory strategies that evolve after iSCI and possibly reduce the capacity to restore walking ability.
Braking is reduced during overground walking in persons with iSCI, especially with AD use
Both AD use and lower extremity strength may constrain production of fore-aft braking forces after iSCI. Compared with AB controls, braking GRFs were significantly reduced by an average of 75% (AD group) and 34% (no AD group) in persons with chronic iSCI. In addition, a 38% reduction in braking occurred in AB controls who walked with an AD compared with without under iSCI-matched cadence conditions, suggesting that braking is reduced, in part, because of AD use. In an inverted pendulum model of walking, the GRFs in early stance are needed to redirect the body's fall from the previous gait step into movement over the extended leg in the current gait step. 35 Stronger braking is required on the current step if stronger propulsion was generated on the previous step. Therefore, a contributing factor to reduced braking in those with iSCI may be lower levels of propulsion being generated by the contralateral leg. Slow walking, or the use of an AD such as a walker that interferes with the inverted pendulum walking mechanics, would then require less braking.
To the extent that braking can be accomplished with the upper body using an AD, less braking is required by the lower limb. While ADs may improve stability, and thus be helpful for balance control, they encourage slow walking. 36 Walkers promote increased hip flexion during walking in those with iSCI 37 that may interfere with recovery of improved gait mechanics. Over-prescription of ADs should be avoided because of the constraints they impose on gait and thus the potential adverse impact on recovery of GRF production.
In addition, lower extremity muscle weakness may constrain fore-aft braking after iSCI. Braking impulse is largely generated by eccentric muscle activity of the knee extensors, ankle dorsiflexors, and plantar flexors during early stance. 38,39 Impaired eccentric muscle activity and timing during the weight acceptance phase of gait has been found in spinally injured rats 40 and persons with iSCI. 13 Further, lengthening muscle contractions involve greater cortical activity relative to shortening or isometric muscle contractions. 41,42 Thus, braking may be altered because of deficits in eccentric control, leading to reliance on an AD to generate braking forces at initial stance and prevent forward falls. Dependence on an AD may limit subsequent recovery and plasticity by curtailing the need for production of eccentric contractions for braking, however. Without use of residual eccentric muscle control, walking with an AD may fail to drive recovery of eccentric muscle control. Moreover, variable foot contact (e.g., heel strike vs. flat foot) may make it more difficult for persons with iSCI to contact the floor in a controlled, stable manner, subsequently impacting GRFs and further increasing use of an AD for safety.
A moderate correlation between braking impulse and LEMS indicates that muscle weakness may further constrain braking forces in persons with iSCI. Increased spasticity in the more impaired limb (SCATS) was also associated with decreased braking time, which may contribute to an earlier transition to push-off during stance-phase because of increased extensor spasms. 43 Specific training, such as downhill walking focused on eccentric control, may improve braking in persons with iSCI as proposed previously in stroke. 44
Reduced propulsion was not related to AD use, but may limit walking speed in persons with iSCI
Propulsive impulse is vital for acceleration and walking speed. During gait, kinetic energy generated by muscle activation when the COM is low is converted to potential energy as the COM reaches its maximum height. Forward propulsion then occurs as the body falls forward in late stance, until the contralateral heel strike starts to redirect the motion of the COM upward again for the next gait cycle. 45,46 In normal gait, the propulsive impulse quantifies the forward directed propulsive forces along the fore-aft axis. We found propulsive impulse was significantly reduced by an average of 60% (AD group) and 41% (no AD group) in persons with chronic iSCI compared with able-bodied controls. Even when controlling for cadence and AD use by having AB controls walk under matched conditions, propulsion was still reduced by 37% in persons with iSCI. Interestingly, only a 9% reduction in propulsion occurred in AB controls who walked with an AD compared with without under iSCI-matched cadence conditions, suggesting AD use has a minimal impact on propulsive impulse.
The reduction in propulsion in those with iSCI could be the result of reduced plantar flexor strength 12, 47 and/or increased leg flexor activity. 48 Biomechanical modeling of human gait shows that the gastrocnemius, soleus, and gluteus medius generate most of the propulsion during the late-stance phase, 49 suggesting that weakness and/or poor control of these muscles, as might occur in those with iSCI, would be particularly deleterious for generating propulsive impulse. Therapeutic strategies leading to improvement of plantar flexion torque could increase generation of GRFs in persons with iSCI.
Vertical GRFs during overground walking are similar between persons with iSCI and AB controls when matched for cadence and AD use
As might be anticipated from slower walking speeds and AD use, vertical GRFs were smaller in persons with iSCI, particularly for those who use an AD, with significant reductions in V1Max (25%), V2Max (24%), and vertical GRF modulation values (60%) compared with AB controls. In normal gait, the first force peak is a result of the deceleration of the COM and weight bearing during weight acceptance in early stance. This is followed by a decrease in vertical GRF because of vertical acceleration of the person's COM provided by the contralateral limb, partially unloading the limb during midstance. 31,50 Lower vertical acceleration by the contralateral limb would then result in lower vertical GRF modulation values. Last, the second force peak is observed at push-off when the plantar flexors accelerate the COM upward during terminal stance/pre-swing. 51
A reduction of all these values in persons with iSCI may indicate the use of an abnormal gait pattern that does not follow the inverted pendulum model of vertical acceleration and deceleration. Moreover, for those who use an AD, reduced vertical GRFs may indicate reliance on the AD for weight bearing and use of the upper extremities for upward vertical acceleration and swing clearance. These differences are likely explained, however, by slower walking and/or reliance on ADs. When AB controls walked with an AD, they exhibited reduced vertical force production during weight acceptance (14%) and push-off (17%) compared with when walking without an AD at iSCI-matched cadence conditions, further suggesting an impact of AD use on vertical GRFs even in the presence of intact neural control and sufficient lower extremity strength for weight bearing and acceleration. Persons with iSCI may exhibit muscle weakness in knee extensors and/or ankle plantar flexors necessary for weight support and push-off, respectively, that may impair their ability to produce sufficient vertical GRFs for faster speeds and body-weight support, necessitating slower walking speeds and AD reliance in some cases.
AD use and slower walking speed may contribute to reduced GRF production
When walking with an AD, both AB controls and persons with iSCI exhibited reduced fore-aft and vertical GRFs, even at the same cadence. These results suggest that ADs induce force constraints independent of neurologic injury and that it is not a learned constraint, because AB persons had little to no previous experience using ADs. Further, the use of an AD resulted in reduced braking time, reduced braking impulse, and V2Max values below cadence-appropriate levels in AB controls. Likely, these GRF reductions are compensated for by the upper extremities exerting increased forces through the AD. For example, Lofstrand crutches have been shown to provide a restraining (braking) force during walking to prevent users from falling forward 52 and to support vertical forces up to 50% body weight. 37 Thus, while ADs allow users with iSCI to safely increase mobility, they may constrain GRF production by the lower limbs needed for overground walking, potentially curtailing use- and task-dependent plasticity and recovery.
Therapists should be conscious of AD-imposed constraints on force production when prescribing them to patients and when practicing gait training. For example, therapeutic strategies such as overground walking with body-weight support or pre-gait training with decreased upper extremity support may be useful to facilitate increased GRF production during gait. One caveat is that body-weight support training that provides too much support may also impose similar effects, but this possibility remains unclear.
It is well known that persons with iSCI often walk at a slower speed than able-bodied persons, particularly when using an AD. 2,53 Slow walking speeds have been associated with increased gait variability and risk of falls. 54 In our study, we also found a reduction in cadence in persons with iSCI using an AD compared to those who walk without one. Previous studies have shown positive correlations between GRFs and walking speed 55 or cadence. 56 In this regard, the GRF impairments observed in persons with iSCI could be the direct consequence of the lesion, or a combination of the lesion and compensatory strategies including reduced speed/cadence. In our study, the difference in GRFs between persons with iSCI and AB controls walking at matched cadences were often reduced and sometimes completely removed compared with differences when AB controls selected their own cadence. It is difficult to discern whether the inability to produce sufficient forces leads to reduced speed or if slower speed leads to reduced forces. Muscle weakness, dyscoordination, 13 and sensory deficits are all likely important contributing factors. In the future, it appears important to take into consideration speed effects when evaluating locomotor impairments in a pathology such as SCI.
Persons with iSCI exhibit altered GRF modification with change in cadence
GRFs are important for changing the speed and cadence of walking. In our study, to increase cadence by 15%, AB controls increased both braking and propulsive impulse, as well as vertical loading during weight acceptance and vertical GRF modulation. Similar modifications have been noted in the literature when increasing speed or step length. 56 These strategies allow for walking at faster speeds and/or with longer steps by increasing propulsion while also increasing braking to maintain a controlled, safe heel contact. Persons with iSCI who were not dependent on an AD were able to modify vertical forces with faster cadences, but no other significant GRF modifications were demonstrated, irrespective of AD use. These results suggest that persons with iSCI used different compensatory strategies to increase cadence or speed, such as increased force production through an AD or the less impaired limb. These strategies could be used, in part, because persons with iSCI are not able to increase plantar flexor torque 57 to enable an increase in propulsion, or chose not to increase ankle torque because of inability to brake with the contralateral leg. Alternatively, because of the slower self-selected speeds of those with an AD, increasing cadence by 15% in the AD group may not represent enough of a change in cadence to necessitate measurable GRF modifications in the more impaired limb.
Clinical Implications and Future Directions
Understanding constraints on lower extremity force production after iSCI is important for refining therapeutic strategies to improve overground walking. Retraining of dynamic neuromuscular control strategies, incorporating eccentric quadriceps control, and improved activation/timing of plantar flexors with gait training may improve vertical loading and braking, and propulsive forces, respectively. In addition, gait training that minimizes AD use may contribute to enhanced GRF production. Real-time propulsive feedback during walking is another therapeutic strategy that has been shown to increase propulsive forces and push-off muscle activity. 58 Because GRFs are associated positively with walking speed, improving GRF production may lead to increased speeds necessary for community walking. Further, increased lower extremity strength and GRF production may lessen the compensatory forces transmitted through the shoulder joints to an AD. 59 Such a reduction in upper extremity forces is beneficial toward minimizing overuse injuries, a common secondary complication in persons with iSCI. 60
In the current study, we only measured GRFs on the most impaired leg; thus, clinical implications need to be interpreted within this context. To produce forward motion and increase cadence, it is possible that some force adjustments happened on the less impaired leg. Asymmetrical GRFs have been shown in persons with stroke, with adaptations occurring in the nonparetic leg to compensate for paretic leg deficits. 29,61 Bilateral assessment of GRFs in persons with iSCI could provide more insight into the mechanisms and strategies used to produce forward motion and weight bearing after iSCI. Moreover, it could also be that adaptations are, in part, produced by forces applied through the AD. In the future, it would be beneficial to study the coupling of GRFs and upper extremity forces across different walking speeds by using instrumented mobility devices. 37
Conclusions
This study quantified constraints on GRF production during overground walking in persons with chronic iSCI. Fore-aft and vertical GRF production is altered in persons with iSCI compared with AB controls, especially for those most dependent on an AD. The strong relationship between V2max and SCI-FAI score underscores the importance of altered force generation during late-stance in those with iSCI. While compensatory strategies involving slower cadence and use of an AD can impact fore-aft and vertical GRF production, propulsive forces are still reduced when controlling for these variables compared with AB individuals. Our results suggest that AD use constrains GRF production, even in AB controls, with braking impulse particularly reduced. Moreover, GRF modifications to an increase in cadence are also altered in persons with iSCI. These results highlight the importance of therapeutic strategies that target GRF improvements, incorporating dynamic neuromuscular control strategies, decreased reliance on ADs, and/or biofeedback for force production.
Footnotes
Acknowledgments
The authors would like to thank Robert Havranek and Beth Sasso-Lance, PT, for assistance with subject recruitment and screening; Andrew Tan, PhD, and Wonjoon Sohn, PhD, for their assistance with data collection. We extend special thanks to all study participants.
Author Disclosure Statement
Dr. Randy D. Trumbower has research support from the Wings for Life Foundation, the United States Department of Defense, and the National Institutes of Health. This study was funded by the NIH NICHD (R01 HD081274). The funding sources had no role in study design, collection, patient recruitment, or interpretation of data.
Denise Peters, Yann Thibaudier, Joan Deffeyes, Gila Baer, and Heather Hayes have no competing financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.