
Abstract
Traumatic Brain Injury (TBI) can be associated with partial or total smell loss. Recent studies have suggested that olfactory outcome can be positively modulated after olfactory training (OT). This study's aim was to investigate OT's potential role in smell recovery after TBI-induced olfactory loss. A prospective, randomized, and controlled study was developed. Patients with TBI-induced olfactory dysfunction (n = 42) were randomized into an experimental group with OT and a control group without (nOT). OT was performed twice daily with a six odor training set during 12 weeks. Olfactory loss was assessed using subjective olfactometry (Barcelona Smell Test [BAST] 24), a visual analogue scale (VAS), and n-butanol threshold (n-BTt) at baseline at 4, 12, and 24 weeks. Additionally, patients underwent MRI of the olfactory brain and olfactory bulbs (OB). Based on the MRI results, an overall score (0–16) was developed to associate the structural neurological damage with olfactory outcomes. The primary outcome was the change in olfactory measurements (VAS and BAST-24) between baseline and 12 weeks. The secondary outcome was the association of the MRI score with olfactory outcomes at baseline, and the impact on quality of life (QoL). After 12 weeks of training, OT patients showed a significant improvement in n-BTt (0.6 ± 1.7 OT vs. -0.6 ± 1.8 nOT, p < 0.05), but not in the smell VAS and BAST-24 scores. Olfactory outcomes (VAS, BAST-24, and n-BTt) were significantly associated with MRI structural findings (p < 0.001), but not with the OB volume or olfactory sulcus length. The present study suggests that 12 weeks of OT mildly improves the olfactory threshold in TBI, whereas the overall MRI score may be used as an imaging marker of olfactory dysfunction and disease severity in TBI patients.
Introduction
A
Post-TBI olfactory loss can result in either partial (hyposmia) or total (anosmia) loss of smell. 4,5 The incidence of post-traumatic olfactory disorders ranges widely from 4% to 65% within and between studies. 6 –8 Older studies based on self-assessment of olfactory dysfunction showed a lower incidence of TBI-induced olfactory loss. 9 –11 Because psychophysical tests for olfactory testing are now widely available, a higher incidence of confirmed olfactory loss after TBI has recently been reported. 12 –15 A wide population-based study 4 reported a 5% reporting history of head trauma and observed that those subjects had a higher rate of smell-identification impairment.
Because it is reasonable to assume that a lesion in the olfactory structures engenders smell problems, potential mechanisms for TBI olfactory dysfunction include 16,17 : (1) shearing injury of olfactory nerve fibers crossing the cribriform plate; (2) contusion or hemorrhage in the orbitofrontal and anterior temporal lobes; and (3) mechanical injuries of nasal structures. The latter explains the high prevalence of olfactory loss in patients with frontal lesions, involving the primary and secondary olfactory cortex. 18 Although an association between TBI severity and the degree of olfactory dysfunction has been described, 19,20 other studies have shown that mild TBI may lead to complete olfactory loss 8 and severe TBI may lead to mild olfactory loss. 19
Spontaneous olfactory function recovery occurs over time in a significant number of patients without treatment. The recovery rate of post-traumatic anosmia is currently thought to be between 10% 21 and 36%. 22,23 Welge-Lüssen and coworkers 6 evaluated a cohort of 67 patients who had had post-traumatic olfactory disorder for >5 years, and observed that an anosmia rate of 55.2% at 16 months dropped to 37% at 74 months of follow-up. London and coworkers 24 studied 542 patients with smell dysfunction (106 with head trauma) and observed that 7.2% of anosmic and 22.3% of hyposmic patients reached normal olfactory functioning after 51 months. The latter observations demonstrate that the olfactory system may show a high degree of regeneration and neuroplasticity.
Studies in both healthy rodents and humans have reported that repeated exposure to odorants increases sensitivity to them. 25,26 In intact rodents, exposure to odorants increases neural activity within odor-specific regions of the olfactory bulb (OB). 27 Based on these observations, a number of studies have showed that OT may improve olfactory functioning in healthy volunteers 28 and in patients with post-infectious, 29 post-traumatic, 26 and Parkinson's disease related 30 olfactory loss. 26,31 In a recent study of patients with post-infectious olfactory loss, olfactory training (OT) (16 weeks) has shown a relatively sustained benefit lasting up to 56 weeks. 29
Despite the high frequency and severity of smell dysfunction after TBI, there is, to the best of our knowledge, no randomized controlled study that has assessed the effects of OT in patients with TBI-induced olfactory loss. This study aims to: (1) investigate the impact of OT on the recovery of TBI-induced smell loss; and (2) evaluate the association between TBI-induced structural brain damage and olfactory loss.
Methods
Study population
A prospective, randomized, controlled study on TBI patients was performed between January 2012 and August 2014. TBI patients admitted to a neurorehabilitation hospital or seen through external consultations, with subjective smell loss, were initially recruited at the brain injury rehabilitation program in the Guttmann Institute for Neuro-Rehabilitation and later evaluated at the Hospital Clinic, Barcelona. The inclusion criteria were: (1) age ≥16 to ≤60 years old, (2) interval since TBI ≥1 month to ≤2 years, (3) a Level of Cognitive Functioning Scale (LCFS) Rancho Los Amigos cognitive functioning level score ≥7 points, and (4) being able to answer all required questions and fill out all required questionnaires. The excluded patients had the following conditions, which potentially caused loss of smell: (1) additional neurological disease(s) other than TBI (i.e., dementia, neurodegenerative diseases, Huntintong's disease), (2) major psychiatric problems, and (3) chronic rhinosinusitis or other upper airway infectious or inflammatory diseases. Patients were randomized (Randomizer® v3.2, T.W. VUIJK© Wisse Keizer) into two groups: (1) experimental group with OT for a 3 month period, and (2) control group with no OT (nOT). The sample size calculation was based on a previous study reporting an effect size of at least 30% after OT. 26 An effect size of at least a 30% decrease in smell loss by visual analogue scale (VAS) after 12 weeks after OT was assumed. With an α error of 5% and a power of 80%, a sample size of 41 participants appeared to be sufficient to draw conclusions from.
The trial was conducted according to the Declaration of Helsinki (DoH) and was consistent with good clinical practice (GCP) and the applicable regulatory requirements. Our institution's (Hospital Clínic Barcelona) Ethics and Clinical Research Committee approved the trial protocol with the reference number 2011/6592. All patients and controls provided written informed consent to participate in the study.
Study design
At the screening visit (−4 weeks), participants were evaluated with nasal endoscopies to rule out the presence of any sinonasal disease, which could potentially be related to olfactory dysfunction. An MRI of the brain and olfactory system was performed between screening and baseline evaluation. After the screening visit, all participants were evaluated on three occasions: at the baseline visit (V0) patients were randomized into experimental (OT) and control groups (nOT), being assessed for olfaction levels and quality of life (QoL); visit 1 (V1) was scheduled after 4 weeks, mainly to reinforce the training adherence in the OT group; visit 2 (V2) took place at 12 weeks, when patients were evaluated with olfactory tests and QoL (OT was discontinued at V2); and finally, a follow-up visit 3 (V3) took place at 24 weeks, when patients were evaluated to assess the long-term effects of OT on olfaction recovery and QoL compared with the control group (Fig. 1).
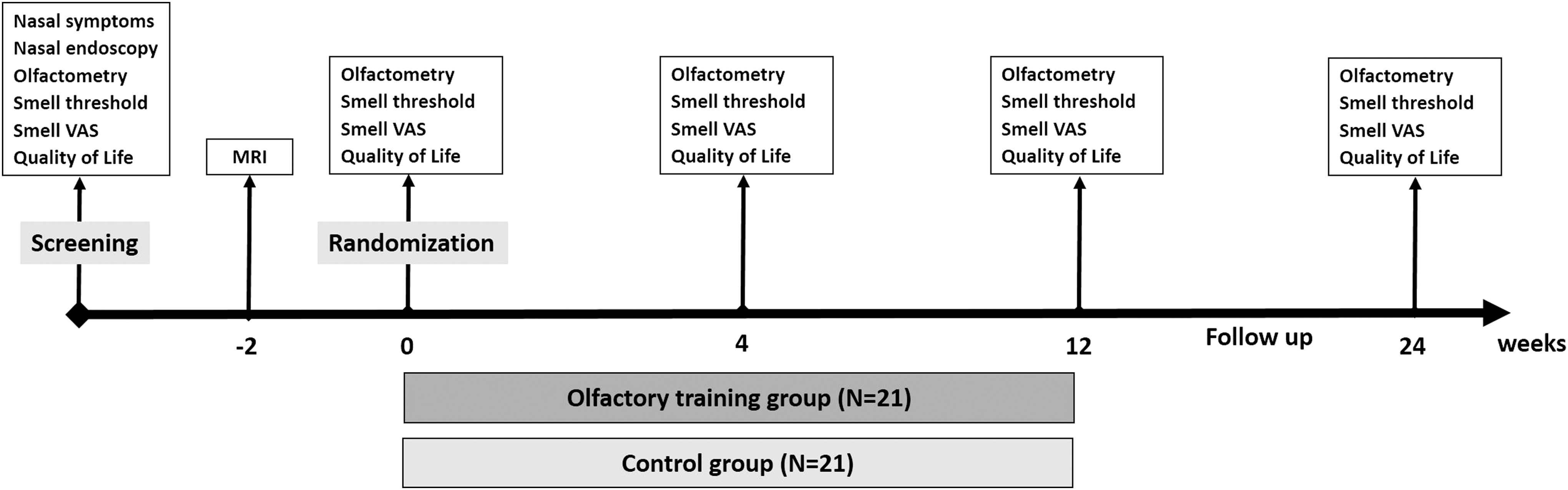
Methodology timeline with interventions for both experimental (olfactory training) and control (no olfactory training) groups. VAS, visual analogue scale.
Intervention
Olfactory training was scheduled to be conducted for 12 weeks using the newly designed training kit of six odorants and the Barcelona Smell Training Test (BASTAT-6), twice a day for 5 min each. BASTAT-6 was designed using those odorants in which the smell detection was >95% in >90% of the healthy Spanish population. 32 Of those, we chose the following odorants: (1) anise (anethole at 30%), (2) lemon (citronellal at 30%), (3) rose (phenyl-ethyl-alcohol [PEA] at 10%), (4) vinegar (acetic acid at 20%), (5) smoked (cade at 1%), and(6) eucalyptus (eucalyptol at 10%). Every session included rotated exposure to each odorant for 10 sec, with 10 sec time intervals between odors. All odorants were placed in hermetic glass jars, which were designed to contain the different odorants according to the Meeting of the German Society for Otorhinolaryngology's recommendations. 33 All patients in the OT group received a BASTAT-6 kit with the odor names labeled on each jar. In order to assure that the patient followed the instructions to perform a correct OT, all patients of the OT group were asked to complete a training diary twice a day with corresponding times and dates. Additionally they had to bring that diary to the subsequent visits so that the research team could monitor that the patient was doing correct OT.
Outcomes
Self-assessment of smell loss
The severity of smell loss was scored using a VAS (0–100 mm), where 0 indicated normal smell perception and 100 indicated total loss of smell perception. Because there are few data assessing the severity of subjective smell loss in TBI patients, we have extrapolated the data from allergic rhinitis, 34 chronic rhinosinusitis, and nasal polyps, 35 to categorize the severity of the symptoms. Further, in a parallel study (not published) of our team assessing olfaction in Parkinson's patients, we were able to show that a severe smell loss assessed by both Barcelona Smell Test (BAST-24) and University of Pennsylvania Smell Identification Test (UPSIT) significantly correlated with a VAS of ≥68mm. Based on these issues, we categorized the smell loss severity as mild (0–30 mm), moderate (> 30 ≤ 70mm) or severe (> 70 mm).
Subjective olfactometry (BAST-24)
BAST-24, validated for the Catalan and Spanish population and used as previously described, 32 contains 20 odors to assess the first cranial nerve. After the patient was exposed to an odorant for 5 sec, the researcher asked the patient to answer three questions: (1) to test smell detection, “Did you smell anything?”; (2) to test smell memory/recognition, “Did you recognize this odor?”; and (3) to test smell-forced choice, “Which of these four odors did you smell?” For all three smell characteristics—detection, memory/recognition and forced-choice identification—the score for each characteristic was from 0 to 20 (0–100%) for the 20 different odors. Approximately 20 min were needed to test the entire set of odors. In order to demonstrate that the TBI patients had a significant reduction in their smell loss we compared their mean BAST-24 data with the mean BAST-24 data from healthy volunteers. The healthy volunteer data were extracted from the BAST-24 validation study database and were matched for age and gender. Healthy volunteers recruited in our ENT department, and all patients with subjective loss of smell or medical history of known causes of loss of smell such as TBI, neurodegenerative disorders, psychiatric diseases, chronic rhinosinusitis, nasal polyps, allergic rhinitis, and abuse of toxic substances were excluded.
n-Butanol Threshold Test (n-BTt)
The n-BTt employed aqueous dilutions of 1-butanol, where the highest aqueous concentration equaled 4% and successive dilutions differed by a factor of three. The number of dilution steps ranged from 0 (4% of 1-butanol) up to 8 depending on testing circumstances. The test solutions were presented for smelling in 250 mL capacity polyethylene bottles containing 60 mL of solution. The bottle closure had a pop-up spout that fitted to both nostrils. To sample a bottle, the person placed the spout into both nostrils and then sniffed simultaneously. Testing began with the lowest concentration (bottle number 8). The test participant received the bottle with this concentration along with a blank and had to decide which one smelled stronger. If the answer was incorrect, the participant received another blank paired with the next higher concentration. Errors triggered increments in concentration, whereas correct choices led to another presentation of the same concentration (in another bottle) and a blank. Four correct choices in a row led to an end of the testing. The concentration at which this occurred marked the threshold. In order to facilitate the interpretation of the results we used the number of the bottle and not the concentration to analyze the data; patients detecting bottles near bottle 8 had a better smell detection capacity than those recognizing bottles with lower numbers. This test was designed to detect the smell threshold and has been validated in the Spanish population. 36
QoL
Both the Sino-Nasal Outcome Test (SNOT-22) 37 and the EuroQol-5D (EQ-5D) 38 questionnaire were used to assess QoL in TBI patients. Higher scores on the SNOT-22 survey items suggest a worse QoL (total score range: 0–110). The EQ-5D questionnaire is divided into two parts: (1) EQ5D QoL index, ranging from 0 to 1, was calculated as previously described; 39 and (2) a VAS score (0–20 cm), used to assess patients' current health status with 0 representing the “worst health state you can imagine” and 20 the “best health state you can imagine.”
MRI
MRI was performed between the screening and baseline visit to evaluate brain damage, OB and sulcus (OS). Patients were examined on a 3T MRI system (TRI0, Siemens, Erlangen, Germany) using a 32 channel-head coil. The protocol included 5 mm thick standard T1 (repetition time [TR]: 390, echo time [TE]: 2.65, matrix: 768 x 768), fluid-attenuated inversion recovery (FLAIR) (TR: 9000, TE: 79, matrix: 512 x 512) and susceptibility-weighted imaging (SWI) (TR: 26, TE: 20, matrix: 240 x 320) weighted sequences to rule out any organic brain disorder and 3 mm thick T1-weighted three-dimensional (3D) sequence (TR: 421, TE: 3.11, matrix: 192 x 192) and 2 mm thick T2-weighted fast spin echo images (TR: 4920, TE: 76, matrix: 192 x 192) in the coronal, axial, and sagittal planes covering the anterior segment of the base of the skull to study the olfactory bulbs. Reading, analysis, and scoring of MRI were made blindly for participants' data and results by two expert neuroradiologists. OB volumetric and OS length analysis were calculated as previously reported by Rombaux and coworkers. 40 MRI data from a healthy control group (n = 20), matched for age and gender, were compared with data from TBI patients. An imaging score of the brain olfactory centers (Barcelona Olfactory Imaging Score [BOIS]) was developed (0–16 points) to evaluate structural damage's association with olfactory outcomes. Damage, neuromalacia, or scar tissue in primary olfactory areas such as the OB, frontorobital cortex, and temporomedial cortex were scored according to the extension of the brain lesion (Table 1).
Data management and statistical analysis
A clinical significant improvement in olfactory performance was defined by a decrease of at least 30% in the mean change of smell loss by VAS, and/or an increase of 30% BAST-24 scores, and n-BTt at V2 compared with V0. When patients scored 0% (anosmia) in the BAST-24 subjective smell test or in the n-BTt we could not calculate a variation in the percentage; in those cases a significant improvement would be considered if at V2 the patient scored 20% on the BAST-24, and 3 on n-BTt. The total BOIS was correlated with different olfactory outcomes, to provide a mean olfactory function loss based only on structural damage.
Categorical variables were compared between groups, using a χ2 test or a Fisher's exact test as appropriate, and continuous variables were compared using Student's t test. Logistical regression models using Firth's penalized likelihood were estimated to assess associations with smell loss. A multivariable model was estimated by a forward stepwise procedure, using p < 0.05 and p > 0.10 from the Wald test as entering and removing criteria respectively. The variation of the olfactory function quality over time and OT's effect on it was assessed by full two way factorial linear mixed-effects regression models of the mean change of the studied indicators on the intervention group and week, with an unstructured residual error covariance matrix over those repeated measurements taken on the same subject. Models were estimated with no intercept to omit any subject-level effects. Linear regression models were applied to evaluate the performance of the score built using the results of nuclear magnetic resonance. All analyses were performed using Stata/SE 14.0.
Results
Patient characteristics
Fifty-three (40.1%) out of 132 TBI patients included in the study reported subjective smell loss. Among the 53 patients eligible for randomization, 42 patients participated in and completed the study protocol (Fig. 2). Of the TBI patients who dropped out (n = 11) of the study, six lived >200 km away from the referral center and declined to travel for the study visits, four did not want to participate for personal reasons, and one was diagnosed with nasal polyps during the nasal endoscopy (exclusion criteria). The sample population involved patients of an average age of 34 years with medium-high education as the average qualification level. The mean interval between the time of inclusion and TBI was 11.4 ± 7.7 months. Most of the TBI patients included in the study had a closed head trauma (64.3%) caused by a traffic accident (78.7%). The trauma severity was assessed using the Glasgow Coma Scale (GCS) (7.6 ± 8.8 points) at the time of injury, and post-traumatic amnesia (PTA) (37.8 ± 31 days). Demographic and baseline clinical characteristics did not differ between the OT and nOT groups (Table 2).

Flow chart of the participants in the study.
Mean (standard deviation)
Number (percentage).
Student t test.
Chi-square test.
Fisher's exact test.
Score system according to bottles presented from the more diluted (#8) to the highest stock concentration (#0).
TBI, traumatic brain injury; PTA, post-traumatic amnesia; VAS, visual analogue scale; BAST-24, Barcelona Smell Test 24 odorants; SNOT-22, 22-Item Sino-Nasal Outcome Test; EQ-5D, European Quality of Life-5 Dimensions questionnaire.
Olfactory loss in TBI patients
According to the smell loss VAS, most of the patients (n = 30, 71.4%) reported a severe subjective smell loss (77.6 ± 24.8 mm). Matched for age and gender (Table 3), the olfactory function that was measured with BAST-24 was significantly lower (p < 0.0001) in TBI patients compared with heavy population (HP) for detection (51.8% vs. 99.6%), recognition (22.7% vs. 82.5%), and forced-choice identification (23.2% vs. 76.9%). The smell threshold in TBI patients (1.8 ± 1.9) was severely affected and significantly decreased when compared with the healthy Spanish population (5.8 ± 1.2). 36 No significant differences between the OT and nOT groups were observed at baseline regarding demographic characteristics or smell loss by VAS, BAST-24 (detection, memory/recognition, forced-choice identification), and n-BTt scores. Further, severe TBI had no significant influence on smell loss measured by VAS (p = 0.98), BAST-24 (detection [p = 0.65], memory/recognition [p = 0.63], forced-choice identification [p = 0.84]), or n-BTt (p = 0.56).
Mean (standard deviation).
Number (percentage).
Student t test.
Chi square test.
BAST-24, Barcelona Smell Test 24 odorants; TBI, traumatic brain injury.
QoL in TBI patients
TBI significantly (p < 0.001) impacted the general and specific QoL of TBI patients compared with the healthy population's QoL 41,42 assessed by the EQ-5D index or SNOT-22. Olfactory training did not improve the patients' QoL (Fig. 3)and the severity of smell loss was not associated with SNOT-22 (β = 0.04, t[40] = 0.24, p = 0.81) or EQ-5D (β = 0.06, t[40] = 0.4, p = 0.69). In the subanalysis of the SNOT-22 domains (rhinological symptoms, extranasal rhinological symptoms, ear and facial symptoms, psychological dysfunction, and sleep dysfunction) and the EQ-5D domains (mobility, self care, usual activities, pain/discomfort, anxiety/depression, and the VAS) we did not find any statistical difference between the groups.

Effects of olfactory training on quality of life of traumatic brain injury (TBI) patients. Both EQ-5D index
MRI in TBI patients
Brain and olfactory system MRI was performed in 36 (85.7%) of the 42 patients; however, 6 patients could not undergo MRI because of having metal prostheses. Gender and age were not correlated with changes in OB volume or OS length. Compared with the control HP, both right (54 ± 24.7 mm3 vs. 62.5 ± 15.7 mm3, p = 0.046) and left (51.7 ± 21.3 mm3 vs. 63.4 ± 14.9 mm3, p = 0.002) OBs were significantly smaller. Moreover, right (5.5 ± 4.3 mm vs. 8.6 ± 0.7 mm, p < 0.0001) and left (4.5 ± 4.3 mm vs. 8.4 ± 0.9 mm, p < 0.0001) OS length were significantly shorter in TBI patients. In the control group, OB volume mean values were 62.5 ± 15.7 mm3 (right) and 63.4 ± 14.9 mm3 (left), whereas OS length mean values were 8.6 ± 0.7 mm (right) and 8.4 ± 0.9 mm (left). The overall BOIS scores and a subgroup analysis by severity of smell loss according to baseline VAS is shown in Table 4.
Post-hoc analysis of BOIS according to VAS smell loss severity: severe (>70mm) and mild-moderate (≤70mm).
Student t test for independent groups.
OB, olfactory bulb; OS, olfactory sulcus; OFC, orbitofrontal cortex; TMC, temporo-medial cortex.
Associations between OB volume and OS length with smell loss assessed by VAS, BAST-24 (detection, memory/recognition, forced-choice identification), and n-BTt did not reach statistical significance. BOIS was associated with the olfactory performance in TBI patients (Table 5), and a linear regression analysis showed a positive association with smell loss VAS, increasing by 3.8 mm for every point of BOIS increase. A negative association was observed for BAST-24; BAST-24 decreased by 6.2% (detection), 3.1% (memory/recognition), and 3.8% (forced-choice identification) for each point of BOIS increase. The latter means that for every positive point in the BOIS (more severe damage) the VAS score increases (worse smell) and the BAST-24 results decrease (worse smell). No significant association was observed between BOIS and n-BTt. Trauma severity (mild-moderate vs. severe GCS) was not associated with OB volume, OS length, or total BOIS.
B-NIOS, Barcelona Neuroimaging Olfactory Score; VAS, visual analogue scale; BOIS, Barcelona Olfactory Imaging Score; BAST-24, 24 odorant Barcelona Smell Test; Coef., regression coefficient.
The Bland–Altman plot for total BOIS (Fig. 4) shows the evaluation of the agreement between two observers including 36 samples. The measured bias was 0.11 points and the limits of agreement (LoA) ranged from −2.09 to 2.32 points. Of the 36 samples in 33% (12 subjects) of the cases, both observers had an exact agreement. In 42% (25 subjects) of the cases, observer 1 punctuated with greater frequency and in 25% (9 subjects), it was observer 2. Except for three data points, all the differences fell within the 95% confidence interval (CI) of the agreement limits at different magnitudes of the measured. For the statistical analysis of these three discrepant cases, the mean of the two raters was used as final measure.
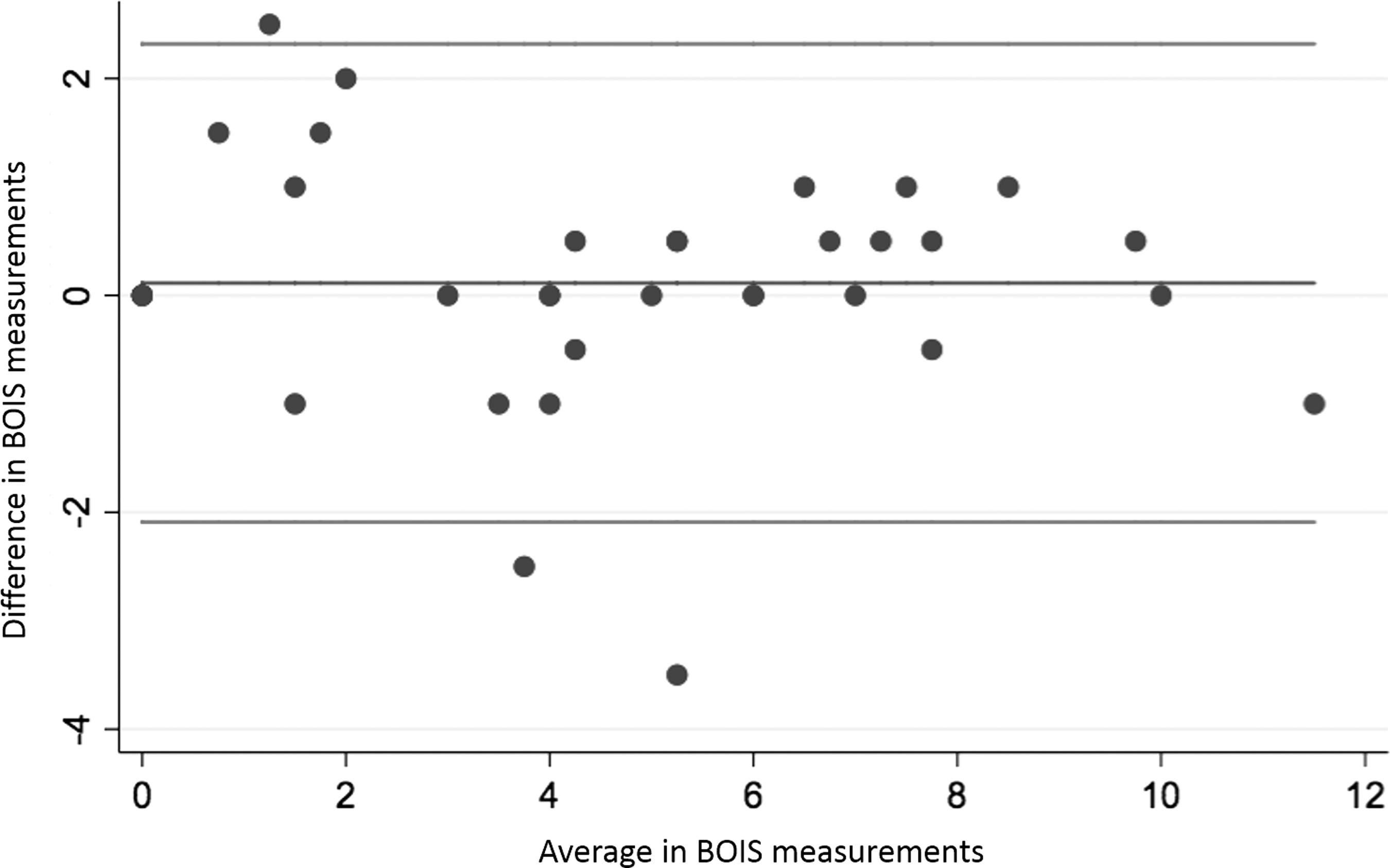
Bland–Altman plots showing the evaluation of the agreement between two observers including 36 samples. Measured bias was 0.11 points and limits of agreement (LoA) ranged from −2.09 to 2.32 points.
OT in TBI patients
After 12 weeks of OT, TBI patients showed a significant improvement in the n-BTt compared with nOT (Fig. 5). However, no significant differences were observed in BAST-24 outcomes and smell loss VAS. Analyzing the patients individually and assuming an increase of at least 30% from baseline in threshold tests (n-BTt), we observed an increase in 26% of the OT group compared with a 5% increase in the control group. An increase of at least 30% in the BAST-24 forced-choice identification at recruitment was observed in 62% of the OT group patients, compared with a 38% increase in the control group. We did not observe any statistically significant improvement with the rest of the variables. Because a strong correlation between smell loss by VAS and BAST-24 detection (r = -0.76, p < 0.001), memory/recognition (r = -0.61, p < 0.001) and forced-choice identification (r = -0.74, p < 0.001) was observed, a post-hoc analysis was performed according to smell loss severity using VAS. TBI patients were divided according to loss of smell severity into mild-moderate (VAS ≤70mm) and severe (VAS >70mm). TBI patients with severe smell loss showed a significant improvement in the n-BTt (Fig. 5B) and a trend of improvement in the BAST-24 forced-choice identification (Fig. 6B), but not when using VAS. The benefit of OT was not sustained after the training period; as such, no difference was observed between the groups (OT vs. nOT) regarding olfactory outcomes after 24 weeks of follow-up (V3). No improvement on loss of smell was observed in patients with mild-moderate loss of smell either using n-BTt, BAST-24, or VAS.
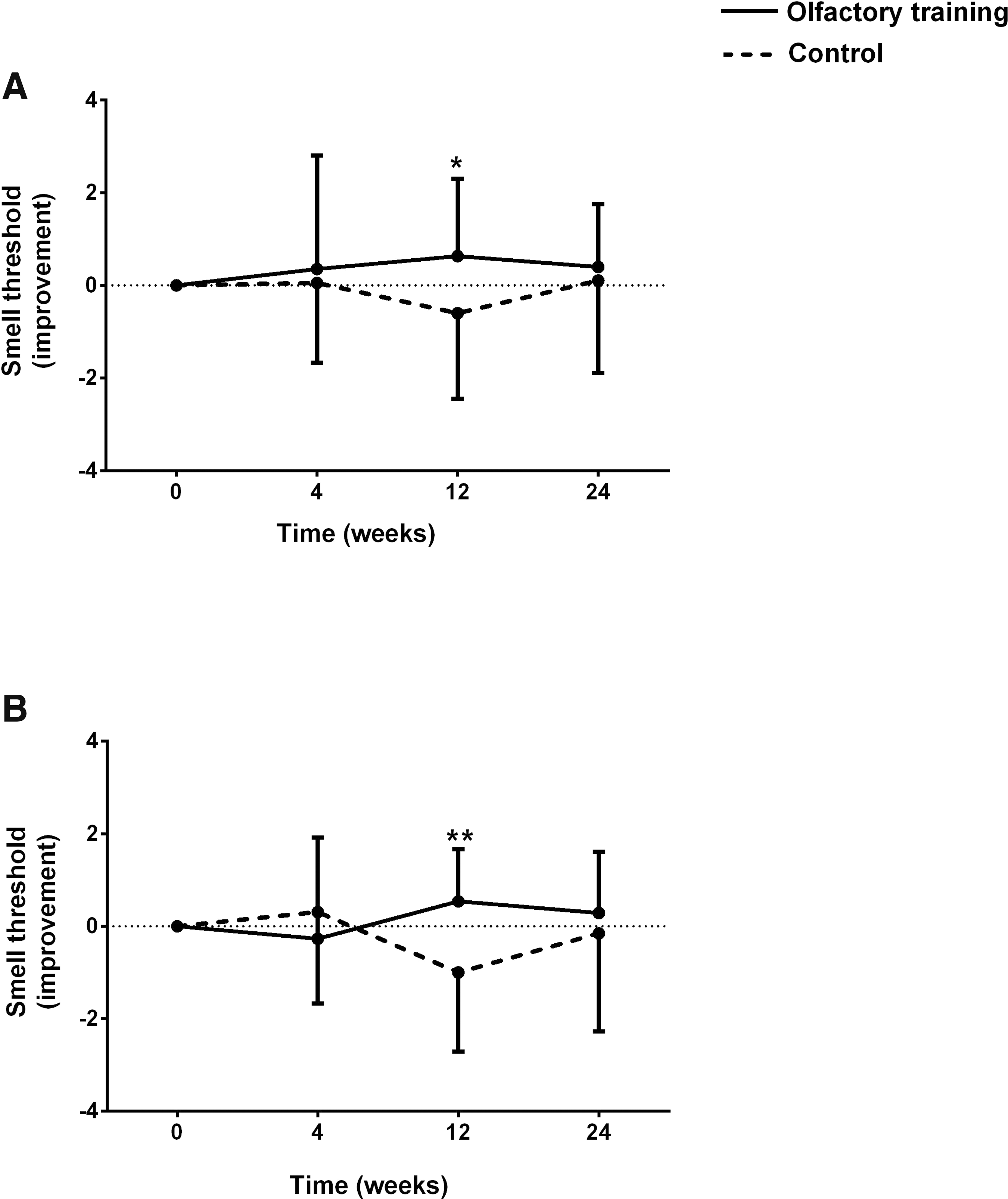
Effect of olfactory training (OT) on n-butanol smell threshold. OT significantly improved smell threshold
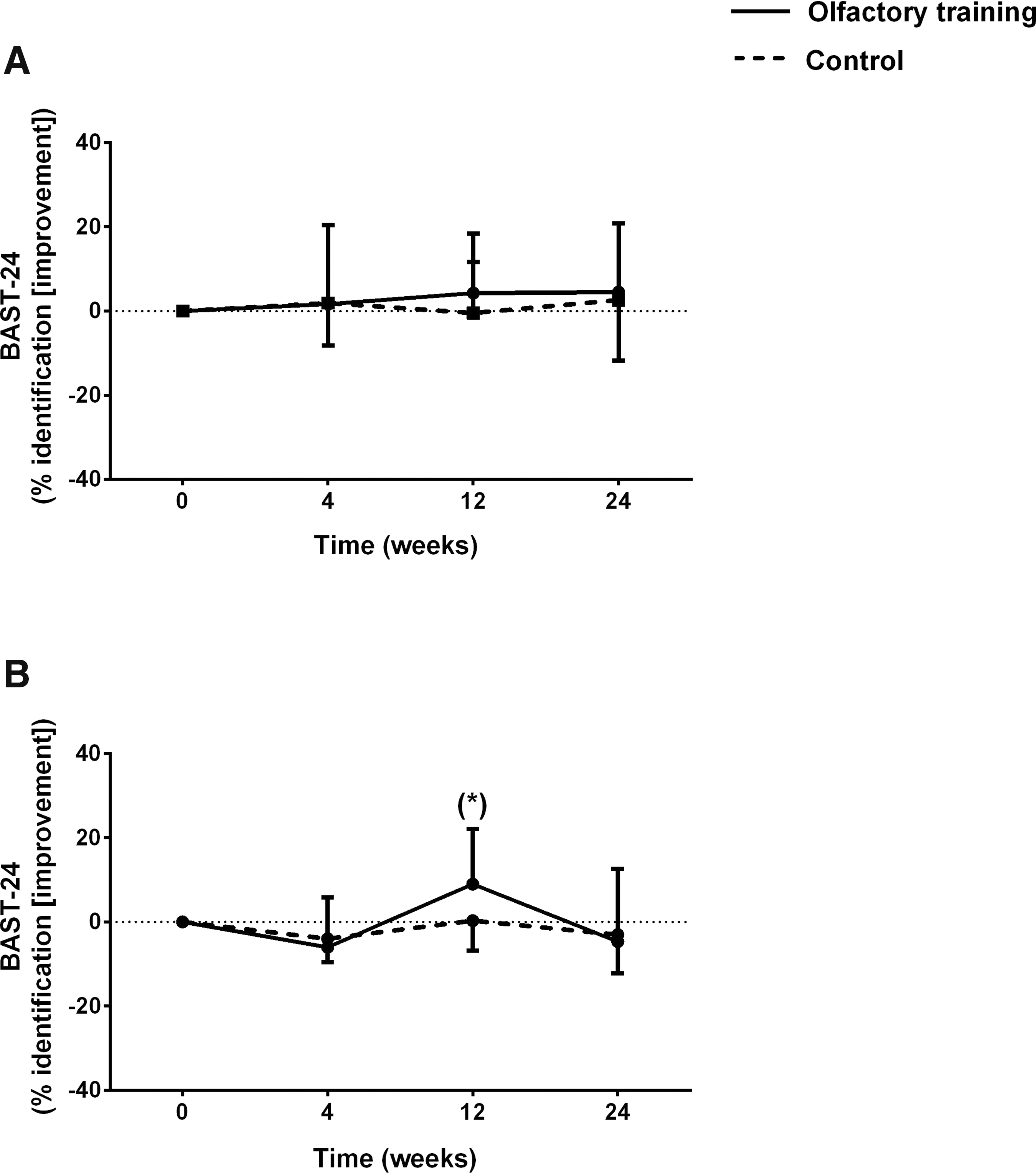
Effect of olfactory training (OT) on BAST-24 subjective olfactometry. OT did not induce improvement of forced-choice smell identification in
Discussion
This study's main findings were: (1) OT induced a mild and transient improvement in smell threshold performance; (2) TBI patients sustained a severe loss of smell irrespective of their gender, age, or TBI severity; (3) TBI-induced loss of smell had a significant negative impact on patients' QoL; and (4) structural brain damage was associated with TBI-induced smell loss.
Most of the TBI patients included in our study reported a severe loss of smell. These results align with prior studies, in which patients' olfactory functions were directly assessed using olfactometry tests, reporting an incidence rate between 10% and 50% of TBI-related anosmia. 19,43,44 Admittedly, TBI patients tend to underestimate their smell loss, and olfactometric tests usually do not correlate with self-assessed smell loss. 45 In contrast to previous findings, we observed that smell-loss assessment by VAS was positively correlated with olfactometric outcomes (detection, memory/recognition, and forced-choice identification). Although some studies have found a positive relationship between olfactory function and gender 4,32 and age, 24,32 we did not observe any association between those variables and olfactory outcomes.
The link between olfactory dysfunction and TBI severity has not been deeply investigated. Early studies using brain imaging, number of hospitalization days, and the need for intensive care as qualitative assessment for TBI severity 46 –48 reported a positive correlation between TBI severity and olfactory dysfunction. Only a few studies have used GCS or PTA to measure TBI severity, and only one has observed better smell-identification scores for patients with a high GCS, without differentiating between low and intermediate GCS scores. 47 PTA has been defined as the best predictor of long-term improvement after TBI in a wide range of impairments. 49,50 Frasnelli and coworkers 43 studied the olfactory function in 63 TBI patients within the first 12 days after trauma using the Sniffin’ Sticks identification test and observed that poor olfactory scores were correlated with a longer PTA, but not with GCS scores. Our study's observations support this absence of correlation between TBI severity (GCS and PTA) and olfactory function. Specifically, we observed that TBI severity was not correlated with the long-term olfactory loss severity. In our cohort, the mean time to assess the smell loss after the TBI was 11.4 months (range 2–24 months), but in the studies 43,46 –48 that showed a positive association between TBI severity and smell loss severity, the assessment of the olfactory function was made mostly in the 1st month after the TBI. Therefore, we can say that TBI severity can be associated with short-term olfactory loss severity but not with long-term olfactory loss severity.
Several studies have shown that TBI has a significant long-term impact on all QoL domains. 51,52 To our knowledge, the present study is the first to evaluate QoL outcomes related to olfactory function loss. We observed that TBI-affected patients had a significantly worse QoL, assessed by EQ-5D and SNOT-22 questionnaires, compared with HP; however, no association was observed between severity of olfactory loss and QoL impairment. This lack of association may be because specific olfactory or even generic (SF-36) QoL questionnaires were not used. The Questionnaire of Olfactory Disorders specifically addresses olfactory dysfunction and its impact on a patient's daily life. 53 Although it could be an excellent QoL questionnaire to use, it is not validated in Spanish, and we decided to use validated questionnaires to provide scientifically reliable and reproducible data for further studies.
In our study, the use of imaging (MRI) of the olfactory system in TBI patients allowed the evaluation of different brain structures involved in olfaction. Structural damage such as brain contusions, especially in the OB and orbital frontal pole region, are common causes of post-traumatic olfactory loss. Rombaux and coworkers 54 reported a positive correlation between olfactory testing and the initial measurement of the total OB volume. Additionally, they observed a significant positive correlation between changes in olfactory function and initial total OB volume measurement, with larger OB volumes being related to an improvement of olfactory function. A previous study by the same authors 55 correlated OB volume with olfactory function in a small cohort (n = 25) of TBI patients. Interestingly, this association was largely determined by retronasal olfactory function. In our study, we observed that TBI patients had smaller OB volumes and shorter OS lengths than healthy controls without TBI. However, we could not identify any correlation between OB volume or OS length and olfactory function. This finding might be explained by the fact that OB neuromalacia and/or scar tissue does not change the OB's volume, but rather disrupts the olfactory neuronal pathways causing olfactory function.
Intraparenchymal hemorrhage, or edemas, are often associated with disorders of smell discrimination. 56 Yousem and coworkers 17 investigated the primary brain injury sites in patients with post-traumatic smell loss. Using an MRI, they found that the highest incidence of post-traumatic encephalomalacia was found in OB and olfactory tracts, subfrontal lobes, and temporal lobes. Based on these findings, we developed a global MRI score (BOIS) accounting for the overall structural damage observed in the OB, OS, fronto-orbital and temporomedial cortex (olfactory function-related areas) to evaluate any potential association with subjective olfactory function. Based on these observations, we clearly demonstrated that a higher BOIS was associated with the loss of olfactory function; BOIS being significantly higher in TBI patients with severe smell loss. Linear regression models of BOIS based on smell loss, VAS, BAST-24, and n-BTt, showed a significant association between the total score and olfactory measurements, except for n-BTt. Only one previous study has tried to associate structural damage with olfactory function based on a MRI brain-morphology algorithm. Lötsch et al. 57 assessed the damage in 11 olfaction-relevant brain areas using MRI from 41 patients with a history of head trauma (20 with hyposmia and 21 with anosmia) and an additional 23 patients without head trauma (16 normosmia, 5 hyposmia, and 2 anosmia). Using classification and the regression tree analysis of the brain lesion pattern, they correctly diagnose anosmia in 81.3% of the cases. Moreover, they observed that anosmia, hyposmia or normosmia were predictable with a 62.3% accuracy rate from the degree of damage in the olfactory bulb and the left temporal lobe pole. Although the study by Lötsch and coworkers 57 provides an elegant algorithm to assess brain olfactory function relating to brain damage, we consider our score (BOIS) easier to perform in daily clinical practice.
Functional and anatomoradiological evidence supports OT-induced neuroplasticity in the olfactory regions of both TBI patients with olfactory dysfunction and healthy controls. 58 Two recent systematic reviews have demonstrated that OT has a positive impact on smell recovery for post-infectious, post-traumatic 59 and neurodegenerative disorders. 60 In contrast to the mild effect in TBI patients, the best results for OT had been shown in post-infectious olfactory loss with recovery rates between 28% and 56%. 26,61,62 These good results may be explained by the fact that post-infectious olfactory loss mainly produces degenerative changes within the olfactory epithelium, 63 in contrast to post-traumatic olfactory loss where the damage is mainly present in olfactory centers and bulbs.
There are only three articles that studied the effect of OT on post-traumatic patients, but none of them are randomized controlled trials. Hummel and coworkers, 26 in a prospective series, included seven patients (OT = 5; nOT = 2) with medical histories of head trauma. They showed that only two patients in the OT group improved their Sniffin’ Stick threshold/discrimination/identification (TDI) score. Konstantinidis and coworkers, 64 in a non-randomized prospective trial, recruited 23 patients with history of smell loss after head trauma for OT and compared them with 15 paired controls with a history of smell loss after head trauma. Patients who underwent OT presented a significantly higher score (33.2% higher) for olfactory function as measured by the Sniffin’ Sticks test. Fleiner and coworkers 65 studied the impact of an 8 month period of OT on patients (46 patients) with olfactory dysfunction. They conducted a nonrandomized, nonblinded, retrospective study; only seven patients had smell loss after head trauma and none of them experienced an improvement in their olfaction after the OT. Our study is the first randomized controlled study of a TBI patient with smell loss. We showed that 12 weeks of olfactory training caused a mild improvement in the smell threshold, although this effect was lost after stopping the OT. After analyzing TBI patients' results regarding different levels of smell loss based on the VAS score, those patients with severe smell loss had a greater improvement in smell threshold (n-BTt) and BAST-24 forced-choice identification after OT compared to nOT. Although OT can be a effective treatment for TBI induce smell loss, our study only showed a mild improvement in the smell threshold test in the OT group, and a tendency toward significance in the BAST-24 forced-choice identification for those patients with severe smell loss (according to VAS) subgroup. This opens the possibility for future research in a larger cohort comparing both TBI patients with and without olfactory disorders.
The duration of the OT effect is scarcely studied. Recently, a prospective study of 111 patients with post-infectious olfactory loss compared a short- (16 weeks) with a long-term (56 weeks) OT. They observed that long-term OT was superior to the short-term scheme. However, even short-term OT (16 weeks) has been reported to give relatively sustainable benefits, lasting for up to 56 weeks. 29 Moreover, a functional MRI study on patients with post-infectious olfactory loss revealed that short-term OT (12 weeks) induced alterations in functional connectivity networks. The latter was based on the observation that a diverse network between the pyriform cortex and mostly non-olfactory regions, shown before the OT, significantly declined after the training. 58 In our TBI cohort, we observed that the effect of training was not sustained over time. The severe structural damage in central olfactory centers showed in our cohort indicates that neuroplasticity changes need a longer period of training to positively affect olfactory function.
The main limitations of this study were as follows. (1) Because no olfactory measurements were performed on the whole cohort (TBI patients), we underestimated the prevalence of smell loss in TBI patients, as well as the impact of loss of smell on QoL of TBI patients. (2) Although OT can be an effective treatment for TBI-induced smell loss, our study only showed a mild improvement in the smell threshold test in the OT group and a tendency toward significance in the BAST-24 forced-choice identification for those patients with severe smell loss (according to VAS) subgroup. This opens the possibility for future research in a larger cohort comparing TBI patients both with and without olfactory disorders. (3) The study was limited to 12 weeks of training. (4) We did not have total certainty that the patients were performing the OT as recommended, especially regarding the duration of exposure for each odorant. It was difficult to truly know if the patient performed the training exercise for exactly 10 sec. In order to prevent this problem we reiterated the duration of odor exposure at each visit. Perhaps in future research, a supervised OT group, by videoconference or in the clinical setting, can be considered. (5) Because of the Ethics Committee's decision, the MRI findings were only assessed at baseline, whereas a potential second MRI post-training could have potentially identified some changes in brain structures, including in the OB and OS. (6) No gold standard test was used to assess sensitivity and specificity for BOIS, although the scoring was done by two neuroradiologists.
Conclusions
TBI patients, independent of the trauma severity, showed a moderate-severe impairment of olfactory function. Structural brain damage strongly correlated with olfactory function; consequently, we propose BOIS as potential scoring system to evaluate structural damage of brain olfactory structures to be correlated with olfactory function. Finally, OT mildly improved olfactory function in TBI patients with olfactory loss, which was predominantly severe.
Footnotes
Acknowledgments
This study was sponsored by a research grant (No. 201106-10) from Fundació La Marató de TV3.
Author Disclosure Statement
No competing financial interests exist.