
Abstract
Field triage guidelines recommend transport of head-injured patients on anticoagulants or antiplatelets to a higher-level trauma center based on studies suggesting a high incidence of traumatic intracranial hemorrhage (tICH). We compared the incidence of tICH in older adults transported by emergency medical services (EMS) with and without anticoagulation or antiplatelet use and evaluated the accuracies of different sets of field triage criteria to identify tICH. This was a prospective, observational study at five EMS agencies and 11 hospitals. Older adults (≥55 years) with head trauma and transported by EMS from August 2015 to September 2016 were eligible. EMS providers completed standardized data forms and patients were followed through emergency department (ED) or hospital discharge. We enrolled 1304 patients; 1147 (88%) received a cranial computed tomography (CT) scan and were eligible for analysis. Four hundred thirty-four (33%) patients had anticoagulant or antiplatelet use and 112 (10%) had tICH. The incidence of tICH in patients with (11%, 95% confidence interval [CI] 8%–14%) and without (9%, 95% CI 7%–11%) anticoagulant or antiplatelet use was similar. Anticoagulant or antiplatelet use was not predictive of tICH on adjusted analysis. Steps 1–3 criteria alone were not sensitive in identifying tICH (27%), whereas the addition of anticoagulant or antiplatelet criterion improved sensitivity (63%). Other derived sets of triage criteria were highly sensitive (>98%) but poorly specific (<11%). The incidence of tICH was similar between patients with and without anticoagulant or antiplatelet use. Use of anticoagulant or antiplatelet medications was not a risk factor for tICH. We were unable to identify a set of triage criteria that was accurate for trauma center need.
Introduction
T
Many older patients with head injury are transported by Emergency Medical Services (EMS) and it can be challenging for field personnel to reliably recognize those who will ultimately be diagnosed with traumatic intracerebral hemorrhage (tICH). In particular, older adults are at reasonable risk for tICH with minor mechanisms, such as a fall from standing height. 8 This risk is assumed to be amplified if they are taking anticoagulant and/or antiplatelet medications—and such patients are at higher risk for post-traumatic disability and death. 9 –12 These patients require rapid diagnosis of tICH with cranial computed tomography (CT). If a tICH is identified, these patients often require administration of reversal agents and close monitoring for neurological deterioration. 13 –16
In recognition of these concerns with head-injured older adults with anticoagulant and antiplatelet use, the most recent field triage guidelines were revised to recommend taking these patients to trauma centers or hospitals with the capability of rapid and comprehensive treatment. 3 These recommendations, however, were largely based on retrospective, registry-based studies. 17 –19 Such studies are often prone to sampling-related biases and likely overestimate the risk of tICH. 20
Our primary objective of this study was to prospectively compare the incidence of tICH and neurosurgery or death due to trauma in head-injured older adults transported by EMS with and without anticoagulation or antiplatelet use. We also evaluated risk factors, including the use of anticoagulant or antiplatelet medications, to predict the incidence of tICH. Finally, we evaluated the sensitivities and specificities of different sets of triage criteria to identify tICH in this patient population using national benchmarks for sensitivity (≥95%) and specificity (≥65%) as the goal.
Methods
Study design and setting
This was a county-wide, prospective study at five EMS agencies and 11 hospitals in Northern California. Institutional Review Board approval was obtained at all study sites.
The study was conducted primarily in Sacramento County, which encompasses 994 square miles and has a resident population of 1,418,788 of which 158,551 (11%) are 65 years and older (2010 census). Sacramento County is served by 5 EMS agencies that respond to 95% of the 9-1-1 call responses for the county. Over 2700 emergency personnel are certified or accredited by the Sacramento County EMS Agency, including approximately 250 mobile intensive care nurses, 1050 paramedics and 1,400 emergency medical technicians. These five EMS agencies transport patients to 11 general acute care hospitals that have a cumulative capacity of approximately 240 ED beds and 3400 inpatient beds. Nine hospitals are located within Sacramento County and two are located in the adjacent Placer County. We included these two out-of-county acute care hospitals because Sacramento County EMS agencies routinely transport patients to these two hospitals and do so under the guidance of the Sacramento County Trauma Triage Tool (Supplementary Fig. 1; see online supplementary material at
Study participants
We included patients 55 years and older with head trauma who were transported to a hospital by the participating EMS agencies from August 1, 2015 to September 30, 2016. Age 55 years and older was chosen as our study population based on the current field triage definition of older adults. 3 We excluded patients transferred by EMS from another receiving facility (interfacility transport), patients transported to a non-participating hospital, and patients with penetrating head trauma. We also excluded patients for whom we were unable to link hospital data to EMS data.
Measurements
EMS providers completed an electronic or paper standardized data collection form that included questions on anticoagulant and/or antiplatelet use, initial Glasgow Coma Scale (GCS) score, and indication for transport to Level 1 or 2 trauma center. Anticoagulant use included warfarin, dabigatran, rivaroxaban, apixaban, and edoxaban. Antiplatelet use included aspirin, clopidogrel, ticlodipine, prasugrel, dipyridamole, cilostazol, and tigagrelor. We designed and modified the data collection form using input from EMS providers, EMS health information managers, emergency medicine physicians, and trauma surgeons. The data collection form was pilot tested with EMS providers and modified prior to the start of the study. EMS providers at all agencies were provided web-based training modules on the objectives of the study and instructions for data collection form completion prior to the start of the study and periodically during the enrollment period.
EMS records were linked to hospital records using name, date of birth, and date of EMS transport. Trained research coordinators abstracted additional data variables from EMS and hospital electronic medical records. EMS variables included mechanism of injury, history of vomiting, headache, loss of consciousness, amnesia, or seizure after head injury, reported dementia, reported intoxication, vital signs during transport (pulse rate, systolic blood pressure, respiratory rate), GCS score, evidence of trauma above the clavicles, transport characteristics (date of transport, EMS agency, level of transport, level of EMS provider, receiving hospital), and the presence of physiological, anatomical, and mechanism of injury field triage criteria (based on the documentation of the presence or absence of explicit criteria). 3 ED and hospital variables included patient demographics, pre-injury anticoagulant or antiplatelet use, serum laboratory results (platelet count, international normalized ratio [INR]), cranial CT results, ED and hospital interventions, Abbreviated Injury Score and Injury Severity Score for hospitalized patients, and ED and hospital disposition. Isolated head injury was defined as an Abbreviated Injury Score <3 in all non-head body regions. 21 Cranial CT imaging and hospital admission were conducted at the discretion of the patients' treating physicians.
A formal coding manual that defined all variables was developed. Study data were collected and managed using REDCap electronic data capture tools hosted at the University of California Davis. 22 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies. Electronic data collection forms were pilot tested prior to data abstraction.
We conducted an enrollment audit on patients who were eligible but not enrolled (failures of the study screening process) during EMS evaluation to assess for enrollment bias. EMS data including age, gender, initial EMS GCS score, and anticoagulant or antiplatelet use were collected on the missed eligible patients.
Outcomes
Our primary outcome measure was the presence of tICH on initial cranial CT imaging in the ED based on radiologist interpretation. Our secondary outcome measure was a composite outcome measure of neurosurgery or death due to trauma during hospitalization. Neurosurgery included craniotomy, craniectomy, or placement of an intracranial pressure monitor. This secondary outcome measure was adapted based on prior consensus-based recommendations for trauma center need. 23
Statistical analysis
We formatted the data and recoded the variables using STATA 13.1 statistical software (STATA Corp., College Station, TX). Descriptive statistics were used to characterize the study population. Non-normal interval data were reported with medians and quartiles 1 (Q1) and 3 (Q3). We compared the incidence of primary and secondary outcome measures in patients with and without anticoagulant or antiplatelet use. We also compared the incidence of outcome measures across specific anticoagulant or antiplatelet medication groups including: warfarin alone, direct oral anticoagulants (dabigatran, rivaroxaban, apixaban, oredoxaban) alone, aspirin alone, other antiplatelet medications (clopidogrel, ticlodipine, prasugrel, dipyridimole, cilostazol, or tigagrelor), concomitant anticoagulant or antiplatelet medications (more than one anticoagulant or antiplatelet medication), and no anticoagulant or antiplatelet medication.
Ten independent predictor variables (age 80 years or older [ideal cutpoint based on receiver operating curve], male sex, an abnormal initial EMS GCS score [GCS score <15], a mechanism of injury other than a fall from standing height or less, a history of loss of consciousness or amnesia, anticoagulant or antiplatelet use, evidence of trauma above the clavicles, a history of vomiting, a history of headache, and the presence of physiological, anatomical, or mechanism of injury trauma triage criteria [Step 1 to 3 criteria, Fig. 1]) were defined a priori and entered into a random-effects multivariate logistic regression model to account for random variation. Significance was defined as a p value <0.05 and the results of the multi-variate logistic regression model were presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). To identify the ideal cutpoint for age, we explored various age cutpoints using a receiver operating curve for non-parametric data and chose the cutpoint that maximized sensitivity and specificity (Youden Index). 24 We used complete-case analysis to handle missing data due to the infrequency of missing data (<1%) 25 and model fit was evaluated using the c-statistic. 26
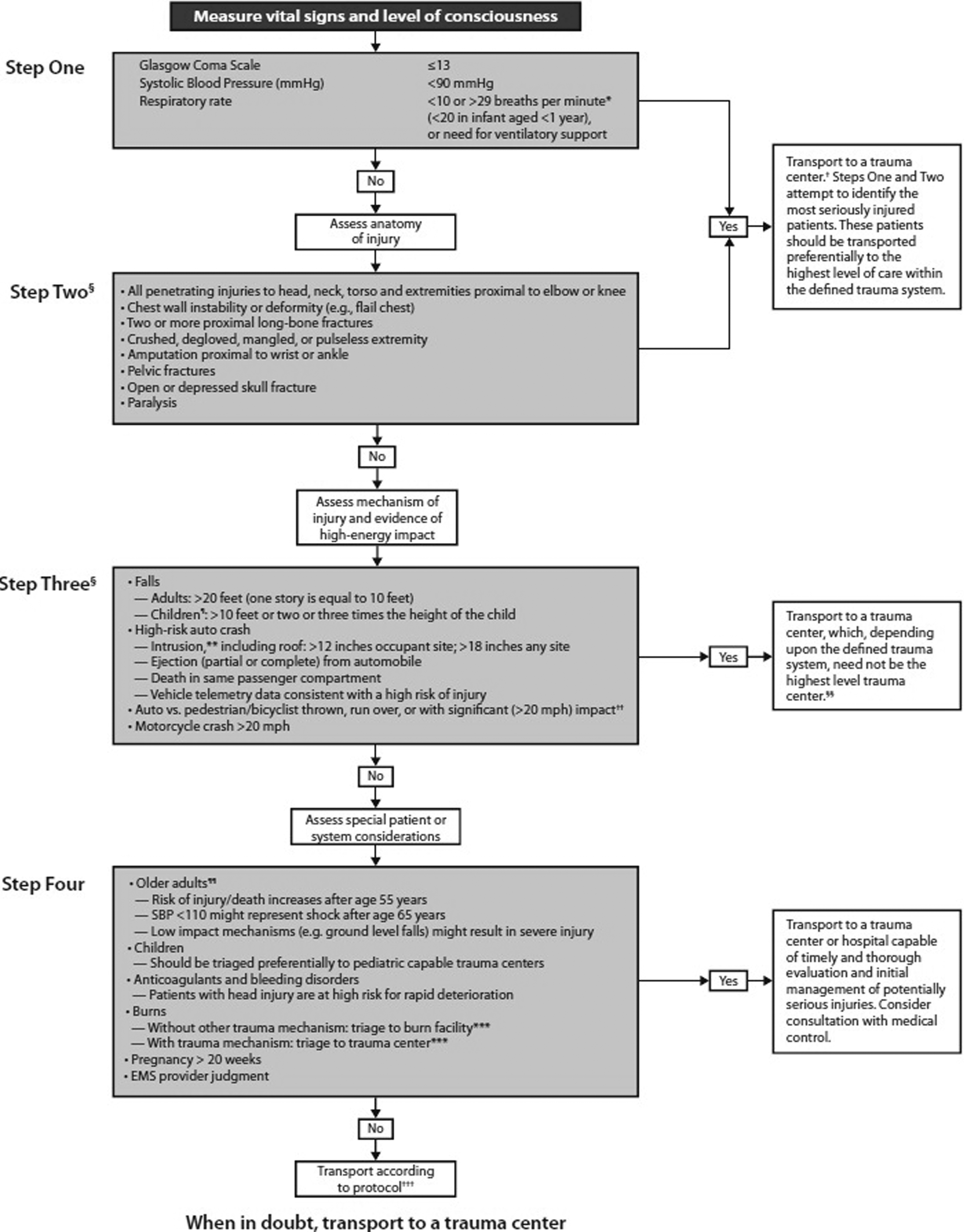
Guidelines for field triage of injured patients—United States, 2011. *The upper limit of respiratory rate in infants is >29 breaths per min to maintain a higher level of overtriage for infants. †Trauma centers are designated Level 1–4. A Level 1 center has the greatest amount of resources and personnel for care of the injured patient and provides regional leadership in education, research, and prevention programs. A Level 2 facility offers similar resources to a Level 1 facility, possibly differing only in continuous availability of certain subspecialties or sufficient prevention, education, and research activities for Level 1 designation; Level 2 facilities are not required to be resident or fellow education centers. A Level 3 center is capable of assessment, resuscitation, and emergency surgery, with severely injured patients being transferred to a Level 1 or 2 facility. A Level 4 trauma center is capable of providing 24-h physician coverage, resuscitation, and stabilization to injured patients before transfer to a facility that provides a higher level of trauma care. §Any injury noted in Step Two or mechanism identified in Step Three triggers a “yes” response. ¶Age <15 years. **Intrusion refers to interior compartment intrusion, as opposed to deformation, which refers to exterior damage. ††Includes pedestrians or bicyclists thrown or run over by a motor vehicle or those with estimated impact >20 mph with a motor vehicle. §§Local or regional protocols should be used to determine the most appropriate level of trauma center within the defined trauma system; need not be the highest-level trauma center. ¶¶Age >55 years. ***Patients with both burns and concomitant trauma for whom the burn injury poses the greatest risk for morbidity and mortality should be transferred to a burn center. If the non-burn trauma presents a greater immediate risk, the patient may be stabilized in a trauma center and then transferred to a burn center. †††Patients who do not meet any of the triage criteria in Steps One through Four should be transported to the most appropriate medical facility as outlined in local EMS protocols.
We used binary recursive partitioning to derive a set of triage criteria using Classification and Regression Trees (CART) software (Salford Systems, San Diego, CA). 27 We forced Steps 1 to 3 criteria to be the initial node and used the Ginni splitting function to set the misclassification cost for missing a patient with a tICH at 20:1. This represents the cost of misclassifying 20 patients who did not have a tICH for one patient who did have a tICH.
We evaluated the sensitivity and specificity of different sets of triage criteria including: (a) Steps 1 to 3 criteria only, (b) Steps 1 to 3 criteria and anticoagulant or antiplatelet use, (c) actual transport to a trauma center, (d) actual transport and anticoagulant or antiplatelet use, (e) Steps 1 to 3 criteria and multi-variate logistic regression risk factors, and (f) Steps 1 to 3 criteria and binary recursive partitioning risk factors to identify tICH and the composite outcome measure of in-hospital neurosurgery or death to trauma. Triage criteria (e) and (f) included variables that were significant in the multi-variate logistic regression and binary recursive partitioning analyses respectively.
To evaluate for the possibility that medications were not accurately ascertained or that patients were not compliant with their medications, we conducted a sensitivity analysis evaluating warfarin use and an INR level 2.0 or higher as a risk factor in the adjusted analysis. We also compared the baseline characteristics of patients with and without anticoagulant or antiplatelet use to evaluate for differences between the two groups. Based on prior data that evaluated a similar patient population, we estimated that collecting 12 months of data would generate a sufficiently large sample of patients with anticoagulant or antiplatelet use to ensure adequate precision of analyses. 28
Results
Characteristics of the study subjects
We enrolled 1304 patients after excluding 52 patients (4.0%) because of unmatched hospital data. The median age was 73 years (Q1, Q3: 63, 84 years) and 610 (47%) were male. The most common mechanism of injury was fall from standing height or less (937/1304,72%). Most patients had an initial EMS GCS score of 15 (1003/1296, 77%), were transported by Advanced Life Support (839/1304, 64%), and were treated by a paramedic (1292/1304, 99%). Median transport time (time from scene to arrival at hospital) was 13 min (Q1, Q3: 9, 18 min). Complete patient characteristics are reported in Table 1. Age, male sex, and proportion of patients with an initial EMS GCS score of 15 were similar between patients enrolled and patients eligible but not enrolled (Supplementary Table 1; see online supplementary material at
May have more than one race.
Missing in 22 patients.
Missing in 7 patients.
In patients taking warfarin.
Calculated in admitted patients only.
If Abbreviated Injury Scale score for all non-head body regions is <3.
ED, emergency department; EMS, emergency medical services; Q1, first quartile; Q3, third quartile.
Main results
Of the 1304 patients enrolled, 1147 (88%) received a cranial CT scan and were eligible for outcome analysis. Of these patients receiving a cranial CT scan, there were 112 (9.8%) with a tICH and 22(1.9%) with in-hospital neurosurgery or death due to trauma. Four hundred and thirty-four of 1304 patients (33.3%) had anticoagulant or antiplatelet use. There was no difference in the incidence of tICH in patients with (47/434; 10.8%, 95% CI 8.1%–14.1%) and without (65/713; 9.1%, 95% CI 7.1%–11.5%) anticoagulant or antiplatelet use. There was also no difference in the incidence of in-hospital neurosurgery or death due to trauma in patients with (6/434; 1.4%, 95% CI 0.5%–3.0%) and without (16/713; 2.2%, 95% CI 1.3%–3.6%) anticoagulant or antiplatelet use. The incidence of tICH and in-hospital neurosurgery or death due to trauma also did not differ when compared across specific anticoagulant or antiplatelet medications (Table 2). A comparison of baseline characteristics between patients with and without anticoagulant or antiplatelet use demonstrated several differences between the two groups including age, race and ethnicity, mechanism of injury, reported dementia, reported intoxication, and a history of loss consciousness or amnesia (Supplementary Table 2; see online supplementary material at
Dabigatran, rivaroxaban, apixaban, or edoxaban.
Clopidogrel, ticlodipine, prasugrel, dipyridamole, cilostazol, or ticagrelor.
More than one anticoagulant or antiplatelet medication.
CT, computed tomography.
Using the area under the curve c-statistic, the overall logistic regression model was considered a good fit (c-statistic 0.727, cutoff 0.70).
26
On adjusted analysis, a history of vomiting (OR 6.65, 95% CI 2.61–16.96), evidence of trauma above the clavicles (OR 2.55, 95% CI 1.33–4.88), the presence of Steps 1 to 3 criteria (OR 2.49, 95% CI 1.43–4.36), an abnormal initial EMS GCS score (OR 2.06, 95% CI 1.27–3.35), a mechanism of injury other than a fall from standing height or less (OR 1.92, 95% CI 1.17–3.15), and a history of loss of consciousness or amnesia (OR 1.63, 95% CI 1.02–2.61) were independent risk factors for the incidence of tICH on initial cranial CT scan (Table 3). A history of anticoagulant or antiplatelet use was not identified as an independent risk factor for tICH (OR 1.53, 95% CI 0.99–2.38). The sensitivity analysis demonstrated that “warfarin use and INR level 2.0 or higher” was not an independent risk factor for the incidence of tICH (OR 1.18, 95% CI 0.48–2.87) (Supplementary Table 3; see online supplementary material at
CI, confidence interval; CT, computed tomography; EMS, emergency medical services; GCS, Glasgow Coma Scale, OR, odds ratio.
Binary recursive partitioning, including Steps 1 to 3 criteria as a forced initial node, identified trauma above the clavicles, anticoagulant or antiplatelet use, and a history of loss of consciousness or amnesia as predictive criteria to identify tICH (Fig. 2).
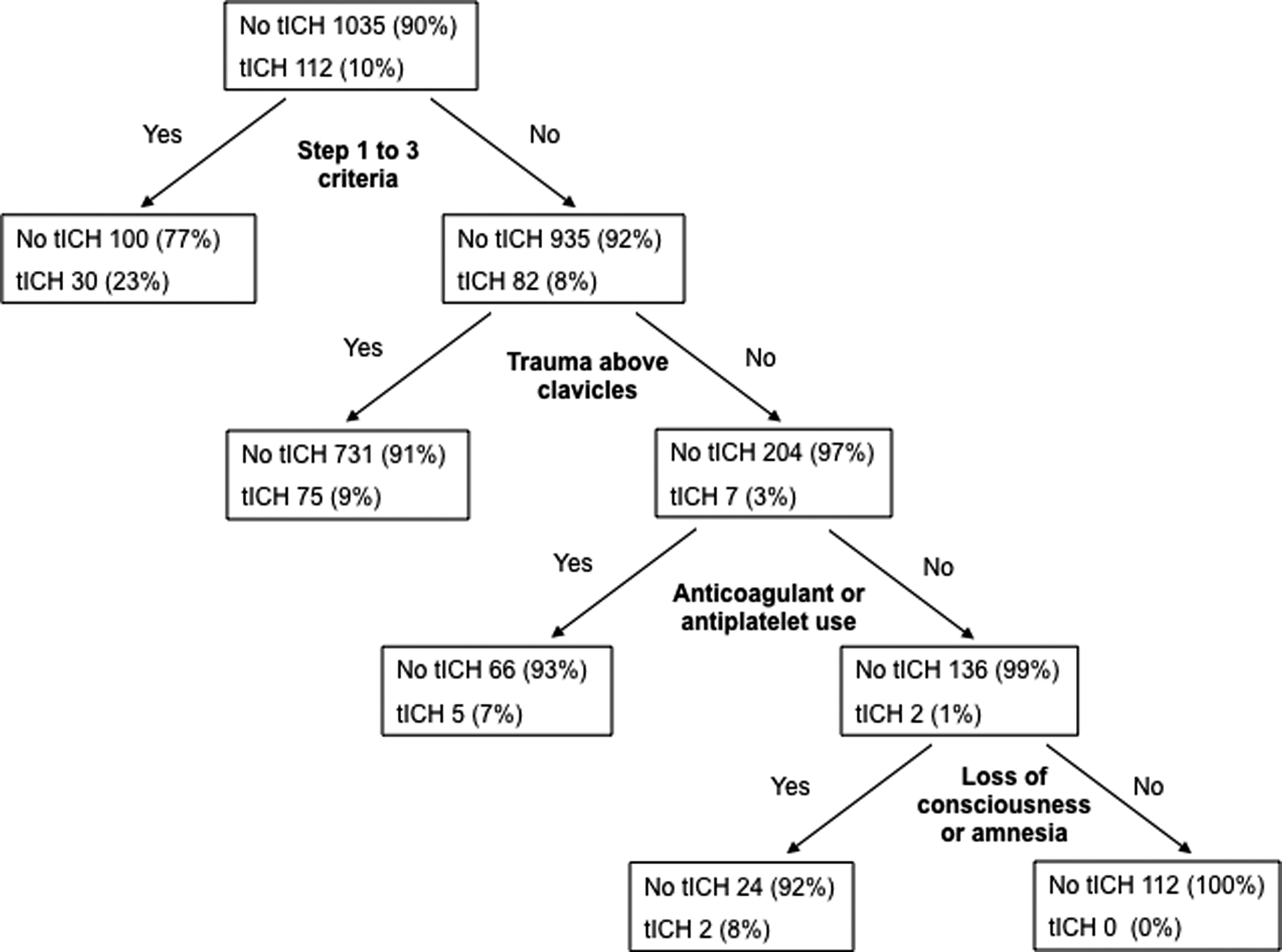
Triage criteria derived from binary recursive partitioning to identify traumatic intracranial hemorrhage (n = 112). tICH, traumatic intracranial hemorrhage.
When we evaluated the sensitivity and specificity of various triage criteria, the criteria including Steps 1 to 3 criteria and multi-variate logistic regression risk factors and the criteria including Steps 1 to 3 criteria and binary recursive partitioning risk factors were highly sensitive (>98%) but not specific (<11%) in identifying tICH. The use of only Steps 1 to 3 criteria had a very low sensitivity (26.8%) in identifying tICH. The use of Steps 1 to 3 and anticoagulant or antiplatelet criteria, actual transport, and actual transport and anticoagulant or antiplatelet criteria had sensitivities that ranged from 63.4 to 87.5% and specificities that ranged from 24.6 to 55.7%. See Table 4 and Figure 3 for a complete description of the test characteristics of different sets of triage criteria to identifyt ICH and Supplementary Table 4 and Supplementary Figure 2 for a description of the characteristics of different sets of triage criteria to identify patients requiring in-hospital neurosurgery or death due to trauma (see online supplementary material at
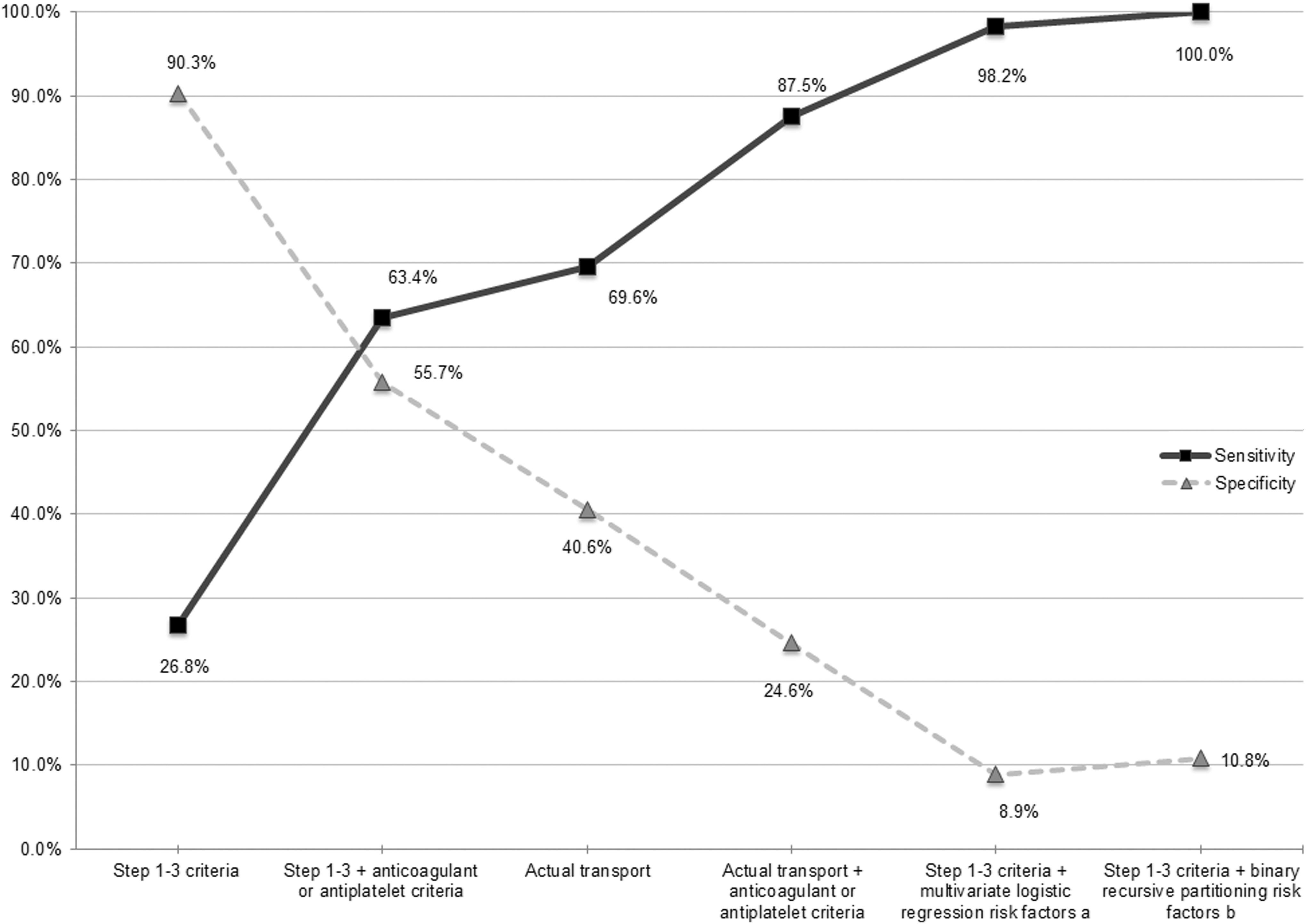
Trade-off of sensitivity and specificity of selected triage criteria to identify traumatic intracranial hemorrhage (n = 112). aLoss of consciousness or amnesia or abnormal initial emergency medical services (EMS) Glasgow Coma Scale (GCS) score or history of vomiting or evidence of trauma above the clavicles or mechanism of injury other than fall from standing height or less. bLoss of consciousness or amnesia or evidence of trauma above the clavicles or anticoagulant or antiplatelet use.
Loss of consciousness or amnesia or abnormal initial EMS GCS score or history of vomiting or evidence of trauma above the clavicles or mechanism of injury other than fall from standing height or less.
Loss of consciousness or amnesia or evidence of trauma above the clavicles or anticoagulant or antiplatelet use.
CI, confidence interval; EMS, emergency medical services; GCS, Glasgow Coma Scale.
Discussion
To our knowledge, this is the first study that prospectively compares the incidence of tICH in head-injured older adults transported by EMS with and without anticoagulation. Prior studies related to this topic have been limited by their retrospective design, 9,10,18,29 lack of patients taking direct oral anticoagulants, 9,10,18,29 and lack of comparator group (i.e., patients not taking anticoagulant or antiplatelet agents). 9,18,28,30 Given the aging population in the United States and the increasing proportion of injured older adults being transported by EMS agencies and evaluated in EDs, this is a high priority area of study for pre-hospital and ED providers. We also anticipate the findings in this study can inform future field triage guideline revisions.
Our study demonstrated a number of interesting findings. Identifying no overall difference in the incidence of tICH in head-injured older adults with and without pre-injury anticoagulant or antiplatelet use was surprising. In addition, our adjusted analysis did not demonstrate that anticoagulant or antiplatelet use was an independent predictor for tICH. A sensitivity analysis evaluating warfarin use and an INR 2.0 or higher as a variable in adjusted analysis, also did not find this as an independent predictor. However, given that anticoagulant or antiplatelet use was marginally significant (OR 1.53, 95% CI 0.99–2.38; p = 0.056), it is difficult to emphatically conclude that anticoagulant or antiplatelet use does not independently impart some risk for tICH. Perhaps a larger sample or different sample would have demonstrated anticoagulant or antiplatelet use as an independent predictor. Moreover, it should be emphasized that our study evaluated the risk of tICH after a single incident of head trauma rather than the risk of tICH over time. What our data do strongly suggest however is that other variables, such as a history of vomiting or evidence of trauma above the clavicles or an abnormal EMS GCS score are more predictive of tICH than anticoagulant or antiplatelet use. These findings could inform future versions of the field triage guidelines. One possible explanation why we found no difference in tICH in patients with and without anticoagulant or antiplatelet use, is that the two groups were likely different in terms of both demographic and clinical characteristics (Supplementary Table 2). In general, head-injured older adults with anticoagulant or antiplatelet use were older, more frequently white and non-Hispanic, more frequently had a mechanism of injury due to a fall from standing height or less, more likely to have a history of dementia, less likely to be intoxicated, and less likely to have a history of loss of consciousness or amnesia compared with older adults without anticoagulant or antiplatelet use. These differences suggest that patients with anticoagulant or antiplatelet use were, in general, less severely injured compared with patients without anticoagulant or antiplatelet use. This, in turn, could “balance” the two groups and thus account for the lack of difference in the risk for tICH between the two groups. Although we controlled for numerous demographic and clinical variables in the adjusted analysis, it is possible that unmeasured differences between the two groups exist.
There was a clear trade-off between sensitivity and specificity when evaluating variations of current field triage guidelines, actual transport, and criteria based on derived models (Fig. 3). As sensitivity increases across the different sets of field triage criteria, specificity consequently decreases. It is also evident that use of Steps 1 to 3 criteria was poorly sensitive (26.8%) in identifying patients with tICH. This is consistent with prior studies demonstrating overall poor sensitivity of Steps 1 to 3 criteria in identifying trauma center need in injured older adults. 29,31,32 The addition of anticoagulant or antiplatelet use criterion to Steps 1 to 3 criteria improved sensitivity (63.4%) compared with Steps 1 to 3 criteria alone, with only a moderate reduction in specificity (55.7%), thus validating the decision to include this criteria in the most recent field triage guidelines. 3 This sensitivity however, was not close to meeting the Americal College of Surgeons Committee on Trauma (ACS-COT) benchmark for sensitivity (≥95% sensitivity of field triage criteria). 33 Our derived models using multi-variate logistic regression and binary recursive partitioning were highly sensitive in identifying tICH (>98%) however with very poor specificity (<11%) thus limiting the utility of implementing these criteria. In a prior study, we also were unable to develop a model that identified a subset of head-injured older adults patients who were low risk for tICH. 30 Prior clinical decision rules derived to identify tICH in adult patients with minor head injury included older adults (age >65 years) as a predictor variable. 34 –36 Thus, it is likely that meeting ACS-COT benchmarks for sensitivity and specificity (≥95% sensitivity and ≥65% specificity) is not feasible for head-injured older adults. 37
We chose tICH as the primary outcome measure and the outcome to equate “trauma center need.” Patients with tICH are generally considered severely injured, which is a subgroup of injured patients who have a survival benefit with management at a trauma center compared with management at a non-trauma center. 38 However, because patients with tICH may often be managed non-operatively and thus may do equally well in a non-trauma center compared with a trauma center, we also evaluated in-hospital neurosurgery and traumatic death as a secondary outcome measure. This group represents the most severely injured patients who have the greatest potential benefit of treatment at a trauma center. We found this outcome was very infrequent (22 of 1147 patients, 1.9%). As expected, the sensitivities of Steps 1 to 3 alone (59.1%) and Steps 1 to 3 and anticoagulant or antiplatelet use (72.7%) to identify in-hospital neurosurgery and death due to trauma were higher compared with the identification of tICH, however still fell below ACS-COT benchmarks. For the identification of both outcomes (tICH and in-hospital neurosurgery or death due to trauma), actual transport and actual transport and anticoagulant or antiplatelet use had more moderate sensitivities and specificities, thus suggesting that perhaps the best triage criteria for head-injured older adults may be some combination of EMS clinical impression and explicit criteria.
Our results should be interpreted in the context of some limitations. Despite pre- and in-study training sessions, 49% of eligible patients were not enrolled. Our enrollment audit demonstrated that missed eligible patients were less likely to have anticoagulant or antiplatelet use, thus suggesting the potential for selection bias that could have influenced the results of the study. Our study was conducted in a single county EMS system where the results may not be generalizable to other EMS systems with varied injury severity and trauma care resources. It is possible that specific anticoagulant or antiplatelet medications (e.g., warfarin or clopidogrel) impart an increased risk for tICH compared with patients not taking these medications. However, due to the relatively small numbers of patients taking specific anticoagulant or antiplatelet medications, we were unable to evaluate for small differences in risk associated with these medications.
In conclusion, in older adults with head trauma transported by EMS, the incidence of tICH was similar between patients with and without anticoagulant or antiplatelet use. Use of anticoagulant or antiplatelet medications was not an independent risk factor for tICH. Adding the criterion of anticoagulant or antiplatelet use to Steps 1 to 3 criteria did improve the sensitivity in identifying tICH. However, we were unable to identify a set of triage criteria that met national benchmarks for sensitivity and specificity for trauma center need in this patient population.
Footnotes
Acknowledgments
This work was funded by the Centers for Disease Control and Prevention (CDC), grant number U01CE002177. The findings and conclusion of this research are those of the authors and do not represent the official views of the U.S. Department of Health and Human Services (DHHS) and the CDC. The inclusion of individuals, programs, or organizations in this article does not constitute endorsement by the U.S. federal government, DHHS, or CDC.
Dr. Nishijima was supported through Mentored Clinical Research Training Program Award (Grant Number UL1TR000002 and linked award KL2TR000134) from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research.
Author Disclosure Statement
Dr. Nishijima reports honorarium from Pfizer, outside the submitted work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.